Setting Policy Priorities for Front-of-Pack Health Claims and Symbols in the European Union: Expert Consensus Built by Using a Delphi Method



Abstract
:1. Introduction
2. Materials and Methods
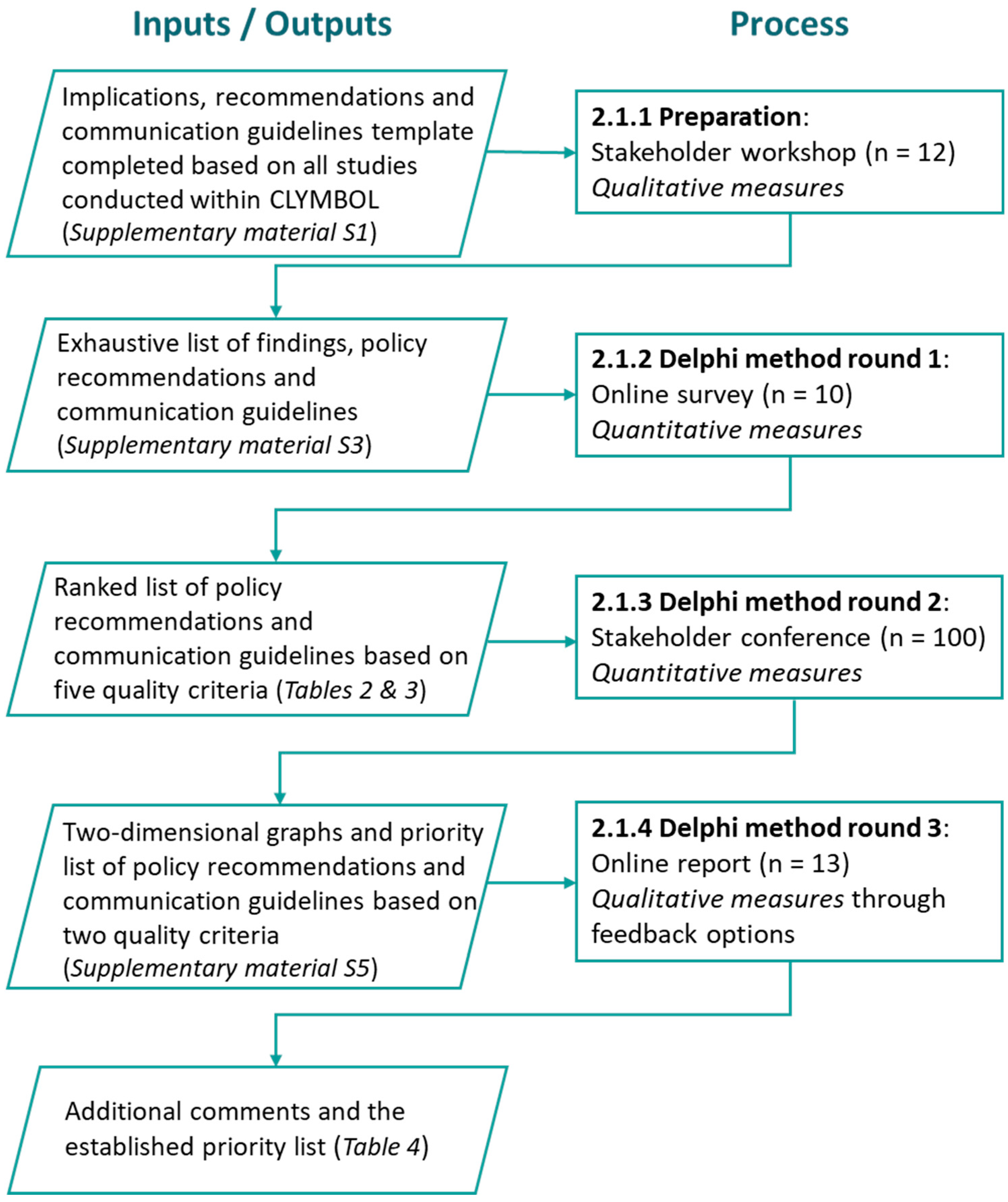
2.1. Procedure
2.1.1. Preparation
2.1.2. Delphi Round 1
2.1.3. Delphi Round 2
2.1.4. Delphi Round 3
2.2. Expert Panel
2.3. Data Analysis
3. Results
3.1. Compilation of Evidence to Formulate Strategies
3.2. Evaluation and Priority Setting
3.2.1. Delphi Round 1
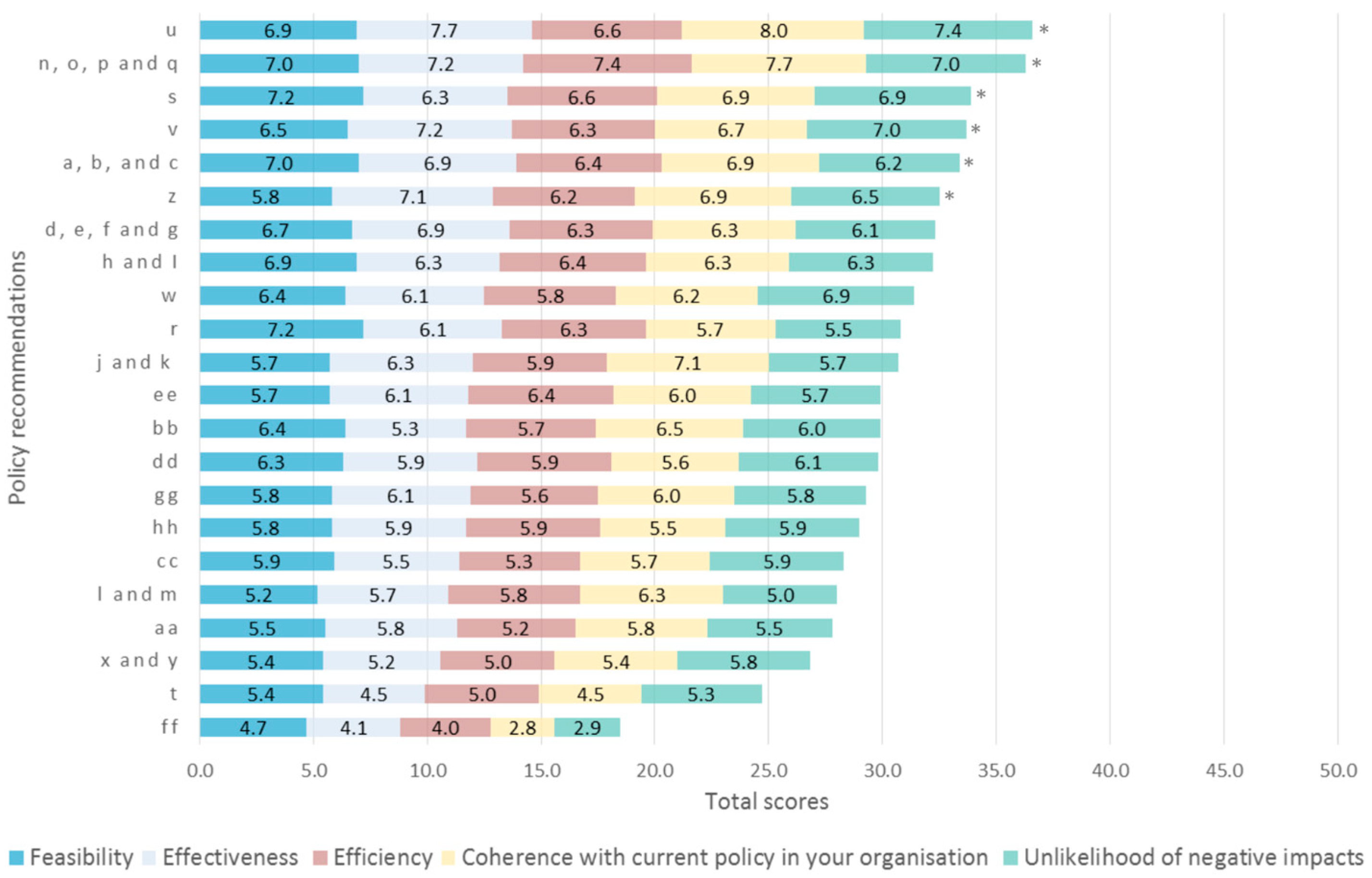
3.2.2. Delphi Round 2
3.2.3. Delphi Round 3
4. Policy Implications and Conclusion
Supplementary Materials
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
References
- Hieke, S.; Kuljanic, N.; Pravst, I.; Miklavec, K.; Kaur, A.; Brown, K.A.; Egan, B.M.; Pfeifer, K.; Gracia, A.; Rayner, M. Prevalence of nutrition and health-related claims on pre-packaged foods: A five-country study in Europe. Nutrients 2016, 8, 137. [Google Scholar] [CrossRef]
- Van Kleef, E.; Van Trijp, H.; Paeps, F.; Fernandez-Celemin, L. Consumer preferences for front-of-pack calories labelling. Public Health Nutr. 2008, 11, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Fernqvist, F.; Ekelund, L. Credence and the effect on consumer liking of food—A review. Food Qual. Prefer. 2014, 32, 340–353. [Google Scholar] [CrossRef]
- Kaur, N.; Singh, D.P. Deciphering the consumer behavior facets of functional foods: A literature review. Appetite 2017, 112, 167–187. [Google Scholar] [CrossRef] [PubMed]
- Aschemann-Witzel, J. The EU health claim regulation in international comparison: Review of the possible impact on food marketing and consumer protection. CAB Rev. Perspect. Agric. Vet. Sci. Nutr. Nat. Resour. 2011, 6, 1–7. [Google Scholar] [CrossRef]
- Hieke, S.; Kuljanic, N.; Wills, J.M.; Pravst, I.; Kaur, A.; Raats, M.M.; van Trijp, H.C.M.; Verbeke, W.; Grunert, K.G. The role of health-related claims and health-related symbols in consumer behavior: Design and conceptual framework of the CLYMBOL project and initial results. Nutr. Bull. 2015, 40, 66–72. [Google Scholar] [CrossRef]
- Hieke, S.; Kuljanic, N.; Fernandez, L.; Lähteenmäki, L.; Stancu, V.; Raats, M.; Egan, B.; Brown, K.; Van Trijp, H.; Van Kleef, E.; et al. Country differences in the history of use of health claims and symbols. Eur. J. Nutr. Food Saf. 2016, 6, 148–168. [Google Scholar] [CrossRef]
- Kaur, A.; Scarborough, P.; Hieke, S.; Kusar, A.; Pravst, I.; Raats, M.; Rayner, M. The nutritional quality of foods carrying health-related claims in Germany, The Netherlands, Spain, Slovenia and the United Kingdom. Eur. J. Clin. Nutr. 2016, 70, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Hodgkins, C.; Barnett, J.; Wasowicz-Kirylo, G.; Stysko-Kunkowska, M.; Gulcan, Y.; Kustepeli, Y.; Akgungor, S.; Chryssochoidis, G.; Fernández-Celemin, L.; Genannt Bonsmann, S.S.; et al. Understanding how consumers categorise nutritional labels: a consumer derived typology for front-of-pack nutrition labelling. Appetite 2012, 59, 806–817. [Google Scholar] [CrossRef]
- Klepacz, N.A.; Nash, R.A.; Egan, M.B.; Hodgkins, C.E.; Raats, M.M. When is an image a health claim? A false-recollection method to detect implicit inferences about products’ health benefits. Health Psychol. 2016, 35, 898. [Google Scholar] [CrossRef]
- Gröppel-Klein, A.; Freichel, M.; Kliebenstein, S. Awareness and Relevance of Health Claims at the Point of Sale. Adv. Consum. Res. 2017, 45, 640. [Google Scholar]
- Hung, Y.; Grunert, K.G.; Hoefkens, C.; Hieke, S.; Verbeke, W. Motivation outweighs ability in explaining European consumers’ use of health claims. Food Qual. Prefer. 2017, 58, 34–44. [Google Scholar] [CrossRef]
- Hung, Y.; Verbeke, W. Consumer Evaluation, Use and Health Relevance of Health Claims in the European Union. Food Qual. Prefer. 2019, 74, 88–99. [Google Scholar] [CrossRef]
- Kaur, A.; Hieke, S.; Rayner, M. Do health and nutrition claims meet consumers’ health needs? Agro Food Ind. Hi-Tech 2016, 27, 3. [Google Scholar]
- Brown, K.A.; Hart, K.H.; Sommers-Jones, G.; Egan, B.; Fiates, G.M.R.; Raats, M.M.; Hieke, S. Do health claims affect consumption, as measured in the laboratory or in the field? Proc. Nutr. Soc. 2016, 75. [Google Scholar] [CrossRef] [Green Version]
- Grunert, K.G. Recommendations for the Use of Methodologies. The Role of Health-Related Claims and Symbols in Consumer Behavior: Outcomes. 2015. Available online: http://www.clymbol.eu/images/CLYMBOL%20report%20on%20the%20recommendation%20of%20methodologies%20Oct%202015.pdf (accessed on 27 December 2018).
- Stancu, V.; Grunert, K.G.; Lähteenmäki, L. Consumer inferences from different versions of a β-glucans health claim. Food Qual. Prefer. 2017, 60, 81–95. [Google Scholar] [CrossRef]
- Edenbrandt, A.K.; Smed, S.; Jansen, L. A hedonic analysis of nutrition labels across product types and countries. Eur. Rev. Agric. Econ. 2017, 45, 101–120. [Google Scholar] [CrossRef]
- Edenbrandt, A.K.; Smed, S. Exploring the correlation between self-reported preferences and actual purchases of nutrition labeled products. Food Policy 2018, 77, 71–80. [Google Scholar] [CrossRef]
- Smed, S.; Edenbrandt, A.K.; Koch-Hansen, P.; Jansen, L. Who is the purchaser of nutrition-labelled products? Br. Food J. 2017, 119, 1934–1952. [Google Scholar] [CrossRef]
- Simon, J.; Kemeny I Varga A van Herpen, E.; Palasha, A. The impact of health claims and health symbols on the attention processes of consumers. NeuroPsychoEconomics Conf. Proc. 2017, in press. [Google Scholar]
- Hieke, S.; Cascanette, T.; Pravst, I.; Kaur, A.; Van Trijp, H.; Verbeke, W.; Grunert, K.G. The role of health-related claims and symbols in consumer behavior. Agro Food Ind. Hi-Tech 2016, 27, 26–29. [Google Scholar]
- Linstone, H.A.; Turoff, M. The Delphi Method. In Techniques and Applications; Addison-Wesley: Reading, MA, USA, 2002. [Google Scholar]
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Aichholzer, G. Das ExpertInnen-Delphi: Methodische Grundlagen und Anwendungsfeld Technology Foresight. In Das Experteninterview; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2002; pp. 133–153. [Google Scholar]
- Turoff, M. The design of a policy Delphi. Technol. Forecast. Soc. Chang. 1970, 2, 149–171. [Google Scholar] [CrossRef]
- Aschemann-Witzel, J.; Perez-Cueto, F.J.; Niedzwiedzka, B.; Verbeke, W.; Bech-Larsen, T. Transferability of private food marketing success factors to public food and health policy: An expert Delphi survey. Food Policy 2012, 37, 650–660. [Google Scholar] [CrossRef]
- Nelson, T.F.; Xuan, Z.; Babor, T.F.; Brewer, R.D.; Chaloupka, F.J.; Gruenewald, P.J.; Holder, H.; Klitzner, M.; Mosher, J.F.; Ramirez, R.L.; et al. Efficacy and the strength of evidence of US alcohol control policies. Am. J. Prev. Med. 2013, 45, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Bisson, J.I.; Tavakoly, B.; Witteveen, A.B.; Ajdukovic, D.; Jehel, L.; Johansen, V.J.; Nordanger, D.; Garcia, F.O.; Punamaki, R.L.; Schnyder, U.; et al. TENTS guidelines: Development of post-disaster psychosocial care guidelines through a Delphi process. Br. J. Psychiatry 2010, 196, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Skulmoski, G.J.; Hartman, F.T.; Krahn, J. The Delphi method for graduate research. J. Inf. Technol. Educ. 2007, 6, 1–21. [Google Scholar] [CrossRef]
- Diefenbach, M.A.; Weinstein, N.D.; O’Reilly, J. Scales for assessing perceptions of health hazard susceptibility. Health Educ. Res. 1993, 8, 181–192. [Google Scholar] [CrossRef]
- Lewis, J.R. Multipoint scales: Mean and median differences and observed significance levels. Int. J. Hum.-Comput. Interact. 1993, 5, 383–392. [Google Scholar] [CrossRef]
- Baguley, I.J.; Perkes, I.E.; Ferndandez-Ortega, J.F.; Rabinstein, A.A. Establishing consensus on Paroxysmal Sympathetic Hyperactivity after acquired brain injury. In BRAIN INJURY; Informa Healthcare Telephone House: London, UK, 2014; pp. 69–77. [Google Scholar]
- Madani, A.; Watanabe, Y.; Vassiliou, M.; Feldman, L.S.; Duh, Q.Y.; Singer, M.C.; Ruan, D.T.; Tabah, R.; Mitmaker, E. Defining competencies for safe thyroidectomy: An international Delphi consensus. Surgery 2016, 159, 86–101. [Google Scholar] [CrossRef]
- Szasz, P.; Louridas, M.; de Montbrun, S.; Harris, K.A.; Grantcharov, T.P. Consensus-based training and assessment model for general surgery. Br. J. Surg. 2016, 103, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Gevers, D.W.M.; Kremers, S.P.J.; de Vries, N.K.; van Assema, P. Clarifying concepts of food parenting practices. A Delphi study with an application to snacking behavior. Appetite 2014, 79, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Sereda, M.; Hoare, D.J.; Nicholson, R.; Smith, S.; Hall, D.A. Consensus on hearing aid candidature and fitting for mild hearing loss, with and without tinnitus: Delphi review. Ear Hearing 2015, 36, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Van der Maaden, T.; van der Steen, J.T.; de Vet, H.C.; Achterberg, W.P.; Boersma, F.; Schols, J.M.; van Berkel, J.F.; Mehr, D.R.; Arcand, M.; Hoepelman, A.I.; et al. Development of a practice guideline for optimal symptom relief for patients with pneumonia and dementia in nursing homes using a Delphi study. Int. J. Geriatr. Psychiatry 2015, 30, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Ems, L.; Gonzales, A.L. Subculture-centered public health communication: A social media strategy. New Media Soc. 2016, 18, 1750–1767. [Google Scholar] [CrossRef]
- Capacci, S.; Mazzocchi, M.; Brambilla Macias, J.; Shankar, B.; Verbeke, W.; Perez-Cueto, A.; Niedzwiedzka, B.; Koziol-Kozakowska, A.; Kijowska, V.; Piorecka, B.; et al. Policies to promote healthy eating in Europe: A structured review of policies and their effectiveness. Nutr. Rev. 2012, 70, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Mørk, T.; Grunert, K.G.; Fenger, M.; Juhl, H.J.; Tsalis, G. An analysis of the effects of a campaign supporting use of a health symbol on food sales and shopping behavior of consumers. BMC Public Health 2017, 17, 239. [Google Scholar] [CrossRef]
- Miklavec, K.; Pravst, I.; Raats, M.M.; Pohar, J. Front of package symbols as a tool to promote healthier food choices in Slovenia: Accompanying explanatory claim can considerably influence the consumer’s preferences. Food Res. Int. 2016, 90, 235–243. [Google Scholar] [CrossRef]
- Vandenbroele, J.; Slabbinck, H.; Van Kerckhove, A.; Vermeir, I. Curbing portion size effects by adding smaller portions at the point of purchase. Food Qual. Prefer. 2018, 64, 82–87. [Google Scholar] [CrossRef]
- Van Ooijen, I.; Fransen, M.L.; Verlegh, P.W.; Smit, E.G. Signalling product healthiness through symbolic package cues: Effects of package shape and goal congruence on consumer behavior. Appetite 2017, 109, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Bialkova, S.; Sasse, L.; Fenko, A. The role of nutrition labels and advertising claims in altering consumers’ evaluation and choice. Appetite 2016, 96, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.S.; Timotijevic, L.; Newton, R.; Coutinho, D.; Llerena, J.L.; Ortega, S.; Benighaus, L.; Hofmaier, C.; Xhaferri, Z.; de Boer, A.; et al. The framing of innovation among European research funding actors: Assessing the potential for ‘responsible research and innovation’in the food and health domain. Food Policy 2016, 62, 78–87. [Google Scholar] [CrossRef]
- Masson, E.; Debucquet, G.; Fischler, C.; Merdji, M. French consumers’ perceptions of nutrition and health claims: A psychosocial-anthropological approach. Appetite 2016, 105, 618–629. [Google Scholar] [CrossRef]
- Sandvik, P.; Nydahl, M.; Kihlberg, I.; Marklinder, I. Consumers’ health-related perceptions of bread—Implications for labeling and health communication. Appetite 2018, 121, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Brooks, K.; Lusk, J.L. Stated and revealed preferences for organic and cloned milk: Combining choice experiment and scanner data. Am. J. Agric. Econ. 2010, 92, 1229–1241. [Google Scholar] [CrossRef]
- Larceneux, F. Segmentation des signes de qualité: Labels expérientiels et labels techniques. Décis. Mark. 2003, 29, 35–46. [Google Scholar]
- Heiko, A. Consensus measurement in Delphi studies: Review and implications for future quality assurance. Technol. Forecast. Soc. Chang. 2012, 79, 1525–1536. [Google Scholar]
- Yoshida, S. Approaches, tools and methods used for setting priorities in health research in the 21st century. J. Glob. Health 2016, 6, 1–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Stakeholder Types | Frequency |
|---|---|
| Stakeholder workshop for preparation (n = 12) | |
| Consumer/Patient Organizations | 3 |
| Industry Representation | 5 |
| National Authorities | 4 |
| Online survey for Delphi method round 1 (n = 10) | |
| Association of Food Industry | 2 |
| Consumer Organization | 1 |
| Food Industry (Producer/Retailer) | 4 |
| Government | 2 |
| Health Professional | 1 |
| Stakeholder conference for Delphi method round 2 (n = 100) | |
| Academia/Research Institute a | 25 |
| Association of Food Industry b | 10 |
| Consumer Organization c | 3 |
| Food Industry (Producer/Retailer) b | 28 |
| Government c | 8 |
| Health Professional c | 5 |
| Legal Advisor c | 7 |
| Non-Governmental Organization (NGO) c | 11 |
| Others/No response c | 3 |
| Online report for Delphi method round 3 (n = 13) | |
| Academia/Research Institute | 2 |
| Association of Food Industry | 4 |
| Food Industry (Producer/Retailer) | 3 |
| Government | 2 |
| Health Professional | 1 |
| Non-Governmental Organization (NGO) | 1 |
| Policy Recommendations | Mean ± S.D. |
|---|---|
| 7.32 ± 2.18 |
| 7.26 ± 2.35 |
| 6.78 ± 1.94 |
| 6.74 ± 2.77 |
| 6.68 ± 1.64 |
| 6.50 ± 2.27 |
| 6.46 ± 2.07 |
| 6.44 ± 2.12 |
| 6.28 ± 2.65 |
| 6.16 ± 2.74 |
| 6.14 ± 2.99 |
| 5.98 ± 1.69 |
| 5.98 ± 1.82 |
| 5.96 ± 2.14 |
| 5.86 ± 2.06 |
| 5.80 ± 2.57 |
| 5.66 ± 2.15 |
| 5.60 ± 3.00 |
| 5.56 ± 2.82 |
| 5.36 ± 2.55 |
| 4.94 ± 2.51 |
| 3.70 ± 2.57 |
| Communication Guidelines | Mean ± S.D. |
|---|---|
| 7.56 ± 2.22 |
| 6.96 ± 1.53 |
| 6.86 ±1.71 |
| 6.74 ± 1.71 |
| 6.68 ± 1.75 |
| 6.56 ± 2.70 |
| 6.44 ± 2.05 |
| 6.36 ± 2.63 |
| 6.32 ± 2.13 |
| 6.28 ± 2.31 |
| 6.26 ± 2.10 |
| 6.18 ± 1.39 |
| 6.16 ± 1.80 |
| 6.06 ± 1.93 |
| 6.00 ± 2.51 |
| 4.96 ± 2.72 |
| 4.90 ± 2.42 |
| Round 2 (n = 100) | Round 1 (n = 10) | ||||||
|---|---|---|---|---|---|---|---|
| Ranking | Mean Scores # | S.D. | IQR | Stakeholder Groups ‡ | Ranking | Changes | |
| Policy recommendations * | |||||||
| #1 | u. Focus on ways to improve motivation | 5.19 b,c | 1.15 | 1.00 | - | #1 | = |
| #2 | p. Provide accurate information about less familiar nutrients | 5.07 a,b,c | 1.51 | 2.00 | - | #2 | = |
| #3 | z. Promote the use of tested method toolbox | 5.07 b,c | 1.58 | 2.00 | Relevance: Academia > Others | #6 | ↑ |
| #4 | n. Increase awareness about existing health claims and symbols | 5.02 c | 1.36 | 1.00 | Relevance: Industry and Academia > Others Feasibility: Academia > Others | #2 | ↓ |
| #5 | a. Profile consumer segments to support well-targeted actions | 4.93 a,b,c | 1.40 | 2.00 | Feasibility: Academia > Industry | #5 | = |
| #6 | s. Call for research on how individual interprets information | 4.85 a,b,c | 1.45 | 2.00 | - | #3 | ↓ |
| #7 | o. Appoint a national authority for informing consumers | 4.83 a,b,c | 1.45 | 2.50 | - | #2 | ↓ |
| #8 | v. Focus not only on education but also need for information | 4.71 a,b,c | 1.42 | 1.50 | Feasibility: Academia > Industry | #4 | ↓ |
| #9 | c. Encourage collaboration between stakeholders and empowerment for monitoring | 4.64 a,b,c | 1.40 | 2.00 | Feasibility: Industry and Academia > Others | #5 | ↓ |
| #10 | b. Appoint a national authority for impact assessment | 4.17 a,b | 1.85 | 3.00 | - | #5 | ↓ |
| #11 | q. Include consumer understanding data in EFSA approval process | 4.15 a | 1.73 | 3.00 | - | #2 | ↓ |
| Communication guidelines * | |||||||
| #1/#2 | xiii. Use innovative ways to communicate healthy eating | 5.20 e,f | 1.21 | 1.50 | - | #3 | ↑ |
| #1/#2 | x. Keep communication simple and clear and avoid jargons | 5.19 f | 1.22 | 1.50 | - | #1 | = |
| #3 | xi. Consider that consumers interpret health claims and symbols differently as experts do | 4.88 e,f | 1.36 | 1.50 | - | #5 | ↑ |
| #4 | ii. Provide additional information in the context of a balanced diet | 4.78 e,f | 1.37 | 2.00 | - | #8 | ↑ |
| #5 | xiv. Inform consumers about the EC Regulation 1924/2006, avoid using low trusted information sources | 4.70 d,e,f | 1.57 | 2.00 | Feasibility: Others > Industry | #2 | ↓ |
| #6 | xix. Communicate health goals at the point-of-sale | 4.69 e,f | 1.64 | 1.50 | - | #9 | ↑ |
| #7 | i. Take into account the needs of different consumer segments | 4.59 d,e | 1.65 | 2.50 | - | #7 | = |
| #8 | xxii. Communicate possible benefits of correct health symbol use | 4.27 d,e | 1.48 | 1.50 | - | #4 | ↓ |
| #9 | xii. Inform consumers that the prevalence of health claims does not necessarily reflect health priorities | 4.04 d | 1.33 | 1.50 | - | #6 | ↓ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, Y.; Hieke, S.; Grunert, K.G.; Verbeke, W. Setting Policy Priorities for Front-of-Pack Health Claims and Symbols in the European Union: Expert Consensus Built by Using a Delphi Method. Nutrients 2019, 11, 403. https://doi.org/10.3390/nu11020403
Hung Y, Hieke S, Grunert KG, Verbeke W. Setting Policy Priorities for Front-of-Pack Health Claims and Symbols in the European Union: Expert Consensus Built by Using a Delphi Method. Nutrients. 2019; 11(2):403. https://doi.org/10.3390/nu11020403
Chicago/Turabian StyleHung, Yung, Sophie Hieke, Klaus G Grunert, and Wim Verbeke. 2019. "Setting Policy Priorities for Front-of-Pack Health Claims and Symbols in the European Union: Expert Consensus Built by Using a Delphi Method" Nutrients 11, no. 2: 403. https://doi.org/10.3390/nu11020403
APA StyleHung, Y., Hieke, S., Grunert, K. G., & Verbeke, W. (2019). Setting Policy Priorities for Front-of-Pack Health Claims and Symbols in the European Union: Expert Consensus Built by Using a Delphi Method. Nutrients, 11(2), 403. https://doi.org/10.3390/nu11020403