Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity—WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017)


 , , ,
, , ,  ,
,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. World Health Organization (WHO) European Childhood Obesity Surveillance Initiative (COSI)
2.2. Sampling of Children
2.3. Measurements
2.3.1. Anthropometry
2.3.2. Energy Balanced-Related Behaviors
Physical Activity
Screen Time
Fruit, Vegetable and Sugared Soft Drinks Intake
2.3.3. Parental Education Level
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
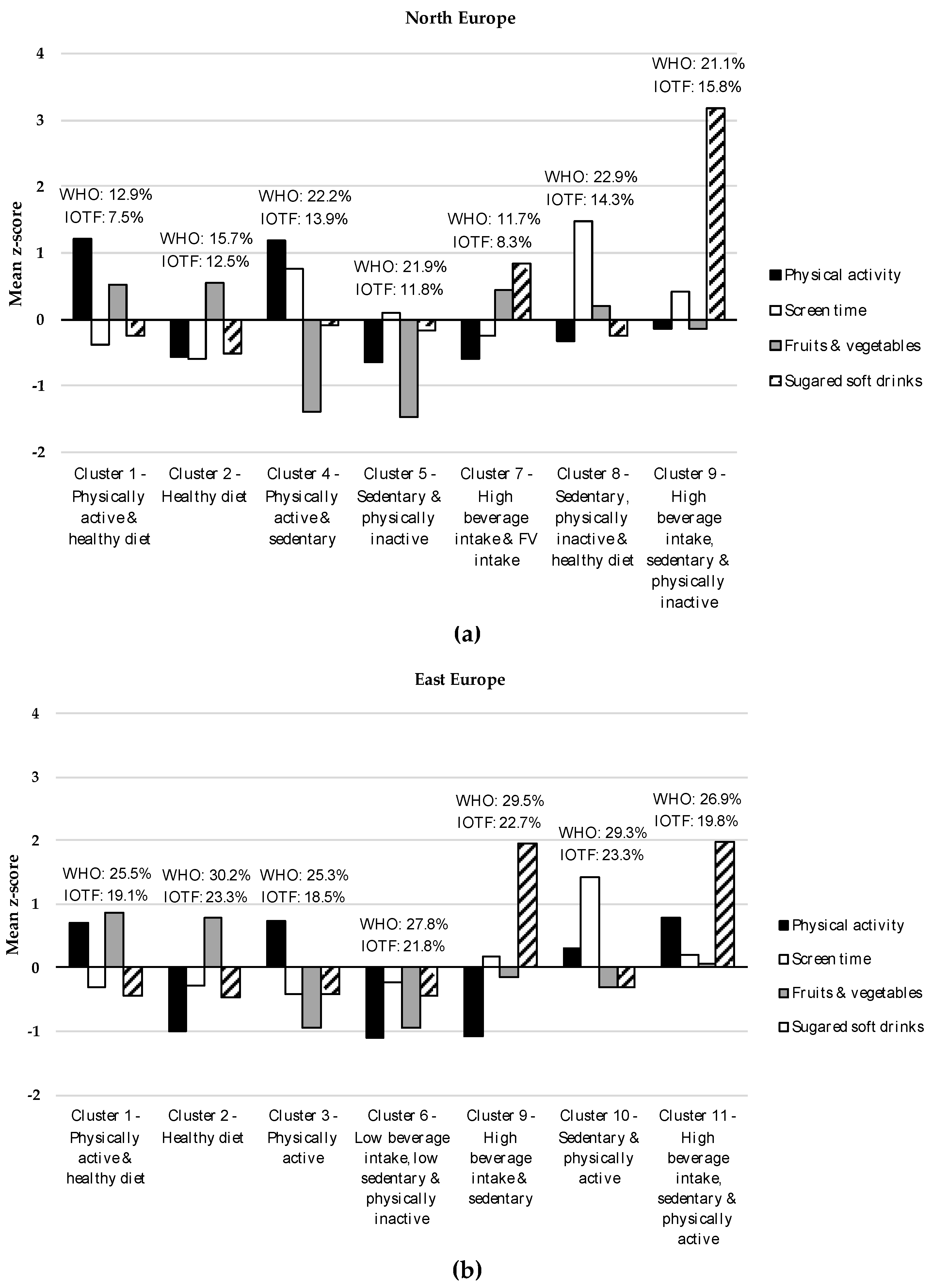
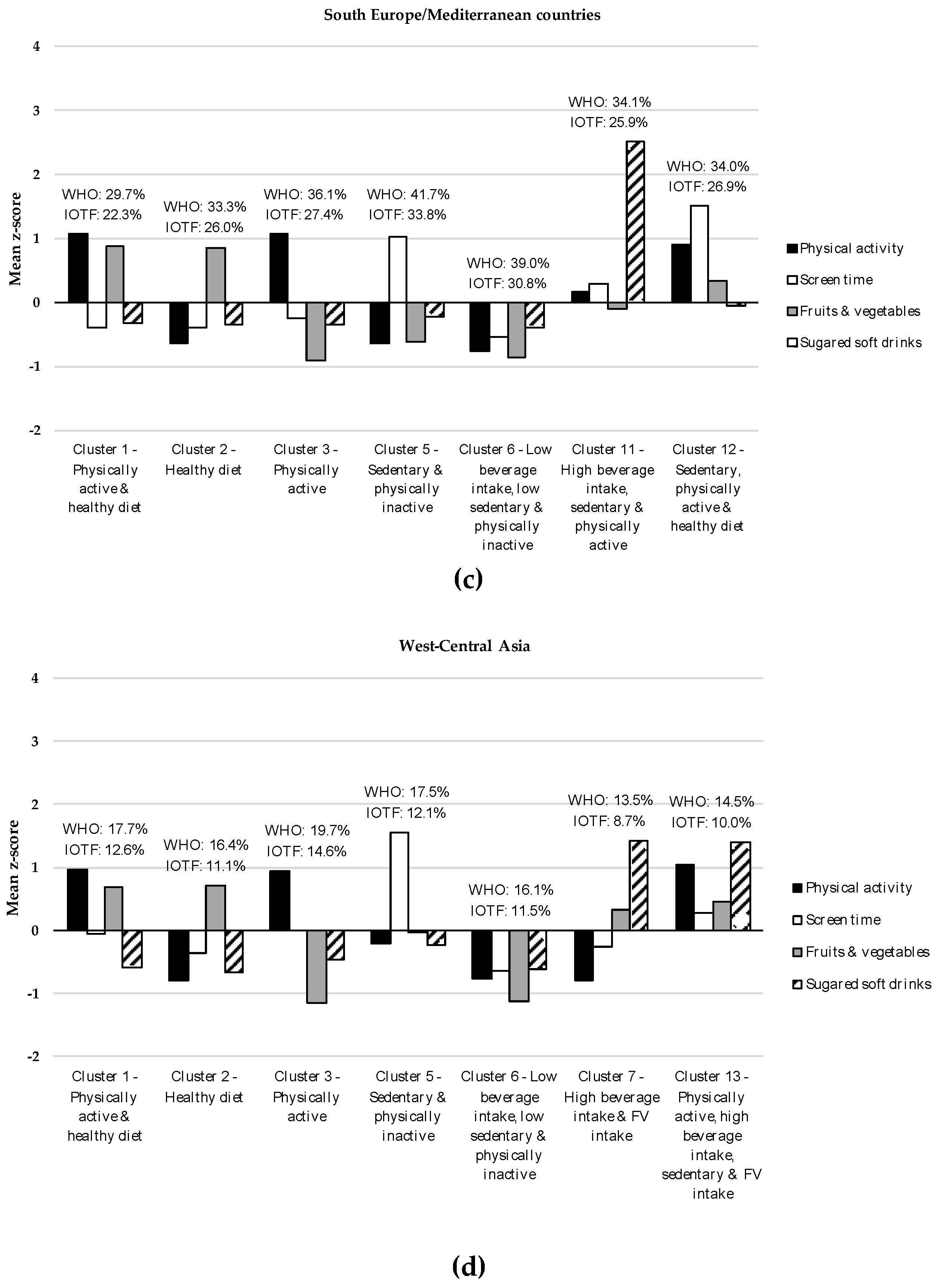
3.2. Clusters Characteristics
3.3. Associations between Cluster Membership and Anthropometric Indicators
4. Discussion
4.1. Clusters Characteristics
4.2. Healthy and Unhealthy Energy Balance-Related Behaviors (EBRB) Clustering
4.3. Co-Occurrence of Healthy and Unhealthy EBRB
4.4. Low EBRB Levels
4.5. Associations between Cluster Membership and Anthropometric Indicators
4.5.1. Differences across Groups of Countries
4.5.2. Synergies among Multiple EBRB and Overweight/Obesity
4.5.3. Measures of EBRB
4.5.4. Role of Sedentary Behaviors
4.5.5. Role of Sedentary Behaviors and Sugared Soft Drinks (SSD) Consumption
4.6. Strengths
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Commision on Ending Childhood Obesity. Facts and Figures on Childhood Obesity. Available online: http://www.who.int/end-childhood-obesity/facts/en/ (accessed on 8 December 2018).
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Boirie, Y.; Cederholm, T.; Chourdakis, M.; Cuerda, C.; Delzenne, N.M.; Deutz, N.E.; Fouque, D.; Genton, L.; Gil, C.; et al. Towards a multidisciplinary approach to understand and manage obesity and related diseases. Clin. Nutr. 2017, 36, 917–938. [Google Scholar] [CrossRef] [PubMed]
- Bradlee, M.L.; Singer, M.R.; Qureshi, M.M.; Moore, L.L. Food group intake and central obesity among children and adolescents in the Third National Health and Nutrition Examination Survey (NHANES III). Public Health Nutr. 2010, 13, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Mellendick, K.; Shanahan, L.; Wideman, L.; Calkins, S.; Keane, S.; Lovelady, C. Diets Rich in Fruits and Vegetables Are Associated with Lower Cardiovascular Disease Risk in Adolescents. Nutrients 2018, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- DeBoer, M.D.; Scharf, R.J.; Demmer, R.T. Sugar-sweetened beverages and weight gain in 2- to 5-year-old children. Pediatrics 2013, 132, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Zang, Y.; Jia, X.; He, X.; Zou, S.; Wang, H.; Shen, M.; Zang, J. Age, period and cohort effects and the predictors of physical activity and sedentary behaviour among Chinese children, from 2004 to 2011. BMC Public Health 2017, 17, 353. [Google Scholar] [CrossRef] [PubMed]
- Falbe, J.; Rosner, B.; Willett, W.C.; Sonneville, K.R.; Hu, F.B.; Field, A.E. Adiposity and different types of screen time. Pediatrics 2013, 132, e1497–e1505. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Bel-Serrat, S.; Mouratidou, T.; Santaliestra-Pasias, A.M.; Iacoviello, L.; Kourides, Y.A.; Marild, S.; Molnar, D.; Reisch, L.; Siani, A.; Stomfai, S.; et al. Clustering of multiple lifestyle behaviours and its association to cardiovascular risk factors in children: The IDEFICS study. Eur. J. Clin. Nutr. 2013, 67, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. Clustering of diet, physical activity and sedentary behaviour among Australian children: Cross-sectional and longitudinal associations with overweight and obesity. Int. J. Obes. 2015, 39, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Santaliestra-Pasias, A.M.; Mouratidou, T.; Reisch, L.; Pigeot, I.; Ahrens, W.; Marild, S.; Molnar, D.; Siani, A.; Sieri, S.; Tornatiris, M.; et al. Clustering of lifestyle behaviours and relation to body composition in European children. The IDEFICS study. Eur. J. Clin. Nutr. 2015, 69, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Oliva, D.; Grao-Cruces, A.; Carbonell-Baeza, A.; Cabanas-Sanchez, V.; Veiga, O.L.; Castro-Pinero, J. Lifestyle Clusters in School-Aged Youth and Longitudinal Associations with Fatness: The UP & DOWN Study. J. Pediatr. 2018, 203, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Seghers, J.; Rutten, C. Clustering of multiple lifestyle behaviours and its relationship with weight status and cardiorespiratory fitness in a sample of Flemish 11- to 12-year-olds. Public Health Nutr. 2010, 13, 1838–1846. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rodrigo, C.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2016, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Alvira, J.M.; De Bourdeaudhuij, I.; Singh, A.S.; Vik, F.N.; Manios, Y.; Kovacs, E.; Jan, N.; Brug, J.; Moreno, L.A. Clustering of energy balance-related behaviors and parental education in European children: The ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Olds, T.; Lewis, L.K.; Martin-Fernandez, J.A.; Barreira, T.; Broyles, S.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. The adiposity of children is associated with their lifestyle behaviours: A cluster analysis of school-aged children from 12 nations. Pediatr. Obes. 2018, 13, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.; Branca, F.; WHO European Childhood Obesity Surveillance Initiative. Protocol, Version January 2008; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- WHO European Childhood Obesity Surveillance Initiative. Protocol, Version October 2012; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- WHO European Childhood Obesity Surveillance Initiative. Protocol, Version October 2016; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2016; Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/333900/COSI-protocol-en.pdf?ua=1 (accessed on 8 December 2018).
- Wijnhoven, T.M.; van Raaij, J.M.; Spinelli, A.; Starc, G.; Hassapidou, M.; Spiroski, I.; Rutter, H.; Martos, E.; Rito, A.I.; Hovengen, R.; et al. WHO European Childhood Obesity Surveillance Initiative: Body mass index and level of overweight among 6–9-year-old children from school year 2007/2008 to school year 2009/2010. BMC Public Health 2014, 14, 806. [Google Scholar] [CrossRef] [PubMed]
- WHO European Childhood Obesity Surveillance Initiative. Overweight and Obesity among 6-to-9-Year-Old Children. Results of the Third Round of Data Collection 2012–2013; World Health Organisation: Copenhagen, Denmark, 2018; Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/378865/COSI-3.pdf?ua=1 (accessed on 8 December 2018).
- Wijnhoven, T.; van Raaij, J.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Implementation of Round 1 (2007/2008) and Round 2 (2009/2010); WHO Regional Office for Europe: Conpenhagen, Denmark, 2014; Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/258781/COSI-report-round-1-and-2_final-for-web.pdf?ua=1 (accessed on 8 December 2018).
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). AnthroPlus for Personal Computers Manual: Software for Assessing Growth of the World’s Children and Adolescents; World Health Organization: Geneva, Switzerland, 2009; Available online: http://www.who.int/entity/growthref/tools/who_anthroplus_manual.pdf (accessed on 8 December 2018).
- Milligan, C.W.; Cooper, M.C. Methodology review: Clustering methods. Appl. Psychol. Meas. 1987, 11, 329–354. [Google Scholar] [CrossRef]
- Gore, P.A. Cluster analysis. In Handbook of Applied Multivariate Statistics and Mathematical Modeling, 1st ed.; Tinsley, H.E.A., Brown, S.D., Eds.; Academic Press: San Diego, CA, USA, 2000; pp. 297–321. [Google Scholar]
- Everitt, B. Cluster Analysis; Heinemann Educational Books: London, UK, 1980. [Google Scholar]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. Clustering of children’s obesity-related behaviours: Associations with sociodemographic indicators. Eur. J. Clin. Nutr. 2014, 68, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.J.; Crawford, D.A.; Salmon, J.; Campbell, K.; McNaughton, S.A.; Mishra, G.D.; Ball, K. Clustering of obesity-related risk behaviors in children and their mothers. Ann. Epidemiol. 2011, 21, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity and Young People. Recommended Levels of Physical Activity for Children Aged 5–17 Years. Available online: https://www.who.int/dietphysicalactivity/factsheet_young_people/en/ (accessed on 8 December 2018).
- Strasburger, V.C.; Hogan, M.J.; Mulligan, D.A.; Ameenuddin, N.; Christakis, D.A.; Cross, C.; Fagbuyi, D.B.; Hill, D.L.; Levine, A.E.; McCarthy, C.; et al. Children, Adolescents, and the Media. Pediatrics 2013, 132, 958–961. [Google Scholar] [CrossRef]
- Pearson, N.; Biddle, S.J. Sedentary behavior and dietary intake in children, adolescents, and adults. A systematic review. Am. J. Prev. Med. 2011, 41, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Vingerhoets, A.M.; Croon, M.; Jeninga, A.; Menges, L. Personality and health habits. Psychol. Health 1990, 4, 333–342. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffussion of Innovations; Free Press of Glencoe: New York, NY, USA. 1962. [Google Scholar]
- Li, L.; Zhang, S.; Huang, Y.; Chen, K. Sleep duration and obesity in children: A systematic review and meta-analysis of prospective cohort studies. J. Pediatr. Child Health 2017, 53, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Chesi, A.; Grant, S.F.A. The Genetics of Pediatric Obesity. Trends Endocrinol. Metab. 2015, 26, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Gorely, T.; Clemes, S.A.; Yates, T.; Edwardson, C.; Brage, S.; Salmon, J.; Marshall, S.J.; Biddle, S.J. Methods of measurement in epidemiology: Sedentary behaviour. Int. J. Epidemiol. 2012, 41, 1460–1471. [Google Scholar] [CrossRef] [PubMed]
- Scharf, R.J.; DeBoer, M.D. Sugar-Sweetened Beverages and Children’s Health. Annu. Rev. Public Health 2016, 37, 273–293. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Watson, J.; Burrows, T. Measuring dietary intake in children and adolescents in the context of overweight and obesity. Int. J. Obes. 2010, 34, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.S.; Landau, S.; Leese, M.; Stahl, D. Cluster Analysis, 5th ed.; John Wiley & Sons Ltd.: West Sussex, UK, 2011. [Google Scholar]



{kind=link}
{kind=link}
| North Europe | East Europe | South Europe/ Mediterranean Countries | West-Central Asia | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age (years) | 7.2 | 0.4 | 8.1 | 0.8 | 7.9 | 0.9 | 8.0 | 0.9 |
| Weight (kg) | 24.9 | 4.3 | 28.7 | 6.7 | 28.9 | 7.2 | 25.5 | 5.6 |
| Height (cm) | 125.1 | 5.8 | 130.7 | 7.4 | 128.6 | 8.1 | 125.4 | 7.8 |
| BMI (kg/m2) | 15.9 | 1.8 | 16.7 | 2.7 | 17.3 | 2.8 | 16.1 | 2.4 |
| BMI/A | 0.10 | 1.0 | 0.29 | 1.3 | 0.62 | 1.3 | −0.01 | 1.16 |
| Physical activity (hours/day) | 1.5 | 0.7 | 2.0 | 0.7 | 1.6 | 0.8 | 1.6 | 0.8 |
| Screen time (hours/day) | 1.9 | 0.9 | 1.7 | 1.0 | 1.4 | 0.8 | 1.6 | 1.1 |
| Fruit and vegetable intake (times/week) | 11.0 | 3.5 | 8.5 | 3.8 | 8.3 | 3.8 | 9.2 | 4.0 |
| Soft drinks (times/week) | 0.9 | 1.1 | 1.7 | 2.1 | 1.3 | 1.9 | 2.6 | 2.6 |
| n | % | n | % | n | % | n | % | |
| Sex | ||||||||
| Boys | 908 | 51.7 | 13,975 | 49.9 | 10,807 | 50.1 | 5966 | 50.3 |
| Girls | 850 | 48.3 | 14,018 | 50.1 | 10,785 | 49.9 | 5906 | 49.7 |
| Parental education level | ||||||||
| Primary school | 11 | 0.6 | 1937 | 7.2 | 1126 | 5.4 | 87 | 0.8 |
| Secondary and vocational school | 517 | 29.7 | 11,294 | 42.1 | 10,361 | 49.3 | 7098 | 62.4 |
| Undergraduate/Bachelor degree | 693 | 39.9 | 6223 | 23.2 | 7122 | 33.8 | 2603 | 22.9 |
| Master degree or higher | 519 | 29.8 | 7357 | 27.5 | 2419 | 11.5 | 1586 | 13.9 |
| Season questionnaire completion | ||||||||
| Winter | 605 | 34.4 | 915 | 3.3 | 8017 | 37.1 | 2681 | 22.6 |
| Spring | 180 | 10.2 | 16,596 | 59.3 | 7955 | 36.8 | 3047 | 25.7 |
| Summer | 252 | 14.4 | 1688 | 6.0 | 1232 | 5.7 | 1 | 0.01 |
| Autumn | 721 | 41.0 | 8794 | 31.4 | 4388 | 20.3 | 6143 | 51.7 |
| Overweight/obese (WHO 2007) | 291 | 16.6 | 7644 | 27.5 | 7611 | 35.3 | 1927 | 16.4 |
| Overweight/obese (IOTF) | 198 | 11.3 | 5824 | 20.9 | 5929 | 27.5 | 1346 | 11.5 |
| n | % | Sex | Physical Activity (Hours/Day) | Screen Time (Hours/Day) | Fruit and Vegetables (Times/Week) | Soft Drinks (Times/Week) | Overweight/Obesity (WHO 2007) | Overweight/Obesity (IOTF) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | |||||||||||||||||
| n | % | n | % | Mean | SD | Mean | SD | Mean | SD | Mean | SD | n | % | n | % | |||
| North Europe (n = 1758) | ||||||||||||||||||
| C1 | 374 | 21.3 | 195 | 52.1 | 179 | 47.9 | 2.3 | 0.3 | 1.6 | 0.6 | 12.8 | 1.7 | 0.6 | 0.7 | 48 | 12.9 | 28 | 7.5 |
| C2 | 522 | 29.7 | 230 | 44.1 | 292 | 55.9 | 1.1 | 0.4 | 1.4 | 0.5 | 12.9 | 1.6 | 0.3 | 0.2 | 82 | 15.7 | 65 | 12.5 |
| C4 | 158 | 9.0 | 86 | 54.4 | 72 | 45.6 | 2.3 | 0.4 | 2.6 | 0.9 | 6.0 | 3.0 | 0.9 | 0.8 | 35 | 22.2 | 22 | 13.9 |
| C5 | 246 | 14.0 | 125 | 50.8 | 121 | 49.2 | 1.1 | 0.4 | 2.0 | 0.7 | 5.7 | 2.5 | 0.7 | 0.8 | 43 | 21.9 | 29 | 11.8 |
| C7 | 205 | 11.7 | 112 | 54.6 | 93 | 45.4 | 1.1 | 0.4 | 1.7 | 0.6 | 12.5 | 1.7 | 2.0 | 0.0 | 24 | 11.7 | 17 | 8.3 |
| C8 | 196 | 11.1 | 125 | 63.8 | 71 | 36.2 | 1.3 | 0.6 | 3.2 | 0.6 | 11.7 | 2.2 | 0.6 | 0.7 | 43 | 22.9 | 28 | 14.3 |
| C9 | 57 | 3.2 | 35 | 61.4 | 22 | 38.6 | 1.4 | 0.7 | 2.3 | 0.8 | 10.5 | 3.1 | 5.0 | 0.0 | 12 | 21.1 | 9 | 15.8 |
| East Europe (n = 27,993) | ||||||||||||||||||
| C1 | 6555 | 23.4 | 3174 | 48.4 | 3381 | 51.6 | 2.5 | 0.4 | 1.4 | 0.7 | 11.8 | 1.9 | 0.8 | 0.8 | 1662 | 25.5 | 1248 | 19.1 |
| C2 | 4798 | 17.1 | 2170 | 45.2 | 2628 | 57.8 | 1.2 | 0.3 | 1.4 | 0.7 | 11.5 | 1.9 | 0.8 | 0.8 | 1443 | 30.2 | 1113 | 23.3 |
| C3 | 4548 | 16.3 | 2357 | 51.8 | 2191 | 48.2 | 2.5 | 0.4 | 1.3 | 0.7 | 4.9 | 2.1 | 0.9 | 0.8 | 1146 | 25.3 | 837 | 18.5 |
| C6 | 4028 | 14.4 | 1957 | 48.6 | 2071 | 51.4 | 1.2 | 0.4 | 1.5 | 0.8 | 4.9 | 2.1 | 0.8 | 0.8 | 1117 | 27.8 | 876 | 21.8 |
| C9 | 1795 | 6.4 | 911 | 50.8 | 884 | 49.2 | 1.2 | 0.4 | 1.9 | 1.0 | 8.0 | 3.9 | 5.9 | 1.0 | 527 | 29.5 | 406 | 22.7 |
| C10 | 3205 | 11.5 | 1726 | 53.9 | 1479 | 46.1 | 2.2 | 0.6 | 3.3 | 0.8 | 7.4 | 3.1 | 1.1 | 1.0 | 932 | 29.3 | 742 | 23.3 |
| C11 | 3064 | 11.0 | 1680 | 54.8 | 1384 | 45.2 | 2.6 | 0.4 | 2.0 | 1.0 | 8.8 | 3.8 | 5.9 | 1.0 | 817 | 26.9 | 602 | 19.8 |
| South Europe/Mediterranean countries (n = 21,592) | ||||||||||||||||||
| C1 | 2946 | 13.6 | 1556 | 52.8 | 1390 | 47.2 | 2.4 | 0.3 | 1.1 | 0.5 | 11.6 | 1.9 | 0.7 | 0.8 | 874 | 29.7 | 657 | 22.3 |
| C2 | 5366 | 24.9 | 2488 | 46.4 | 2878 | 53.6 | 1.1 | 0.4 | 1.1 | 0.5 | 11.5 | 1.9 | 0.6 | 0.8 | 1789 | 33.3 | 1396 | 26.0 |
| C3 | 2754 | 12.8 | 1501 | 54.5 | 1253 | 45.5 | 2.4 | 0.4 | 1.2 | 0.6 | 4.8 | 2.1 | 0.6 | 0.8 | 993 | 36.1 | 754 | 27.4 |
| C5 | 2121 | 9.8 | 1059 | 49.9 | 1032 | 50.1 | 1.1 | 0.4 | 2.4 | 0.5 | 5.9 | 2.8 | 0.9 | 0.9 | 885 | 41.7 | 716 | 33.8 |
| C6 | 4244 | 19.7 | 2018 | 47.6 | 2226 | 52.4 | 1.0 | 0.4 | 1.0 | 0.4 | 5.0 | 2.1 | 0.6 | 0.8 | 1654 | 39.0 | 1306 | 30.8 |
| C12 | 1821 | 8.4 | 947 | 52.0 | 874 | 48.0 | 2.3 | 0.5 | 2.8 | 0.6 | 9.5 | 3.2 | 1.2 | 1.0 | 621 | 34.1 | 472 | 25.9 |
| C11 | 2340 | 10.8 | 1238 | 52.9 | 1102 | 47.1 | 1.7 | 0.8 | 1.7 | 0.8 | 7.8 | 3.9 | 6.0 | 1.0 | 795 | 34.0 | 628 | 26.9 |
| West-Central Asia (n = 11,872) | ||||||||||||||||||
| C1 | 1787 | 15.0 | 875 | 49.0 | 912 | 51.0 | 2.4 | 0.4 | 1.6 | 0.8 | 11.9 | 1.9 | 1.1 | 0.8 | 314 | 17.7 | 223 | 12.6 |
| C2 | 2086 | 17.6 | 993 | 47.6 | 1093 | 52.4 | 1.0 | 0.4 | 1.2 | 0.7 | 12.1 | 1.9 | 0.9 | 0.8 | 339 | 16.4 | 230 | 11.1 |
| C3 | 1511 | 12.7 | 794 | 52.6 | 717 | 47.4 | 2.4 | 0.4 | 1.6 | 0.9 | 4.6 | 2.2 | 1.4 | 1.6 | 296 | 19.7 | 220 | 14.6 |
| C5 | 1270 | 10.7 | 697 | 54.9 | 573 | 45.1 | 1.5 | 0.6 | 3.4 | 0.8 | 9.1 | 3.5 | 2.0 | 2.0 | 220 | 17.5 | 152 | 12.1 |
| C6 | 1911 | 16.1 | 917 | 48.0 | 994 | 52.0 | 1.0 | 0.4 | 0.9 | 0.7 | 4.6 | 2.2 | 1.0 | 1.3 | 303 | 16.1 | 217 | 11.5 |
| C7 | 1728 | 14.6 | 839 | 48.6 | 889 | 51.4 | 1.0 | 0.4 | 1.4 | 0.9 | 10.6 | 3.6 | 6.3 | 1.0 | 230 | 13.5 | 149 | 8.7 |
| C13 | 1579 | 13.3 | 851 | 53.9 | 728 | 46.1 | 2.5 | 0.4 | 2.0 | 1.0 | 11.0 | 3.1 | 6.2 | 1.0 | 225 | 14.5 | 155 | 10.0 |
| BMI/A | Overweight/Obesity (WHO 2007) | Overweight/Obesity (IOTF) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model a | Crude Model | Adjusted Model a | Crude Model | Adjusted Model a | |||||||
| β | 95% CI | β | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| North Europe (n = 1758) | ||||||||||||
| C1 | ref. | ref. | ref. | ref. | ref. | ref. | ||||||
| C2 | 0.07 | −0.06–0.21 | 0.08 | −0.05–0.22 | 1.32 | 0.89–1.94 | 1.35 | 0.91–2.00 | 1.83 | 1.15–2.92 * | 1.85 | 1.15–2.97 * |
| C4 | 0.12 | −0.07–0.31 | 0.07 | −0.12–0.26 | 1.85 | 1.14–3.01 * | 1.68 | 1.02–2.76 * | 1.92 | 1.06–3.47 * | 1.60 | 0.86–2.96 |
| C5 | 0.12 | −0.04–0.28 | 0.11 | −0.05–0.27 | 1.67 | 1.07–2.60 * | 1.63 | 1.04–2.54 * | 1.71 | 0.99–2.97 | 1.63 | 0.94–2.83 |
| C7 | 0.03 | −0.15–0.21 | 0.04 | −0.14–0.21 | 1.13 | 0.65–1.95 | 1.09 | 0.63–1.87 | 1.39 | 0.72–2.69 | 1.37 | 0.72–2.63 |
| C8 | 0.22 | 0.05–0.40 * | 0.25 | 0.07–0.42 ** | 1.93 | 1.22–3.05 ** | 1.92 | 1.21–3.05 ** | 2.08 | 1.19–3.63 * | 2.15 | 1.22–3.77 ** |
| C9 | 0.24 | −0.05–0.52 | 0.18 | −0.11–0.46 | 2.18 | 1.06–4.48 * | 1.78 | 0.85–3.73 | 2.78 | 1.22–6.36 * | 2.22 | 0.94–5.26 |
| East Europe (n = 27,993) | ||||||||||||
| C1 | ref. | ref. | ref. | ref. | ref. | ref. | ||||||
| C2 | 0.16 | 0.11–0.21 *** | 0.17 | 0.12–0.22 *** | 1.30 | 1.20–1.42 *** | 1.32 | 1.21–1.44 *** | 1.34 | 1.22–1.47 *** | 1.35 | 1.23–1.49 *** |
| C3 | 0.02 | −0.04–0.07 | 0.03 | −0.03–0.07 | 1.01 | 0.93–1.11 | 1.03 | 0.94–1.12 | 1.00 | 0.90–1.10 | 1.01 | 0.92–1.12 |
| C6 | 0.12 | 0.07–0.17 *** | 0.13 | 0.07–0.18 *** | 1.17 | 1.07–1.28 ** | 1.18 | 1.08–1.30 *** | 1.26 | 1.14–1.39 *** | 1.28 | 1.15–1.41 *** |
| C9 | 0.06 | −0.01–0.13 | 0.08 | 0.01–0.15 * | 1.19 | 1.06–1.34 ** | 1.22 | 1.08–1.38 ** | 1.23 | 1.08–1.40 ** | 1.26 | 1.11–1.44 ** |
| C10 | 0.16 | 0.10–0.21*** | 0.16 | 0.10–0.22 *** | 1.22 | 1.11–1.34 *** | 1.22 | 1.11–1.35 *** | 1.30 | 1.17–1.45 *** | 1.33 | 1.20–1.49 *** |
| C11 | 0.01 | −0.05–0.07 | 0.03 | −0.03–0.09 | 1.03 | 0.93–1.14 | 1.05 | 0.95–1.16 | 1.00 | 0.90–1.11 | 1.04 | 0.93–1.17 |
| South Europe/Mediterranean countries (n = 21,592) | ||||||||||||
| C1 | ref. | ref. | ref. | ref. | ref. | ref. | ||||||
| C2 | 0.08 | 0.03–0.14 ** | 0.10 | 0.04–0.16 ** | 1.15 | 1.04–1.26 ** | 1.14 | 1.06–1.30 ** | 1.18 | 1.06–1.31 ** | 1.18 | 1.06–1.32 ** |
| C3 | 0.11 | 0.05–0.18 ** | 0.08 | 0.01–0.14 * | 1.21 | 1.08–1.35 ** | 1.17 | 1.04–1.31 ** | 1.19 | 1.05–1.34 ** | 1.12 | 0.99–1.27 |
| C5 | 0.32 | 0.25–0.39 *** | 0.30 | 0.23–0.37 *** | 1.61 | 1.43–1.81 *** | 1.59 | 1.40–1.79 *** | 1.67 | 1.47–1.90 *** | 1.61 | 1.42–1.84 *** |
| C6 | 0.17 | 0.11–0.23 *** | 0.15 | 0.09–0.21 *** | 1.35 | 1.21–1.49 *** | 1.31 | 1.18–1.46 *** | 1.37 | 1.23–1.54 *** | 1.29 | 1.15–1.45 *** |
| C11 | 0.16 | 0.09–0.23 *** | 0.11 | 0.04–0.18 ** | 1.29 | 1.15–1.46 *** | 1.21 | 1.07–1.37 ** | 1.34 | 1.18–1.53 *** | 1.23 | 1.08–1.40 ** |
| C12 | 0.13 | 0.06–0.21 *** | 0.10 | 0.03–0.18 ** | 1.26 | 1.11–1.44 *** | 1.22 | 1.07–1.39 ** | 1.24 | 1.08–1.43 ** | 1.19 | 1.03–1.37 * |
| West-Central Asia (n = 11,872) | ||||||||||||
| C1 | ref. | ref. | ref. | ref. | ref. | ref. | ||||||
| C2 | 0.04 | −0.03–0.12 | 0.05 | −0.02–0.13 | 0.97 | 0.81–1.15 | 0.99 | 0.73–1.18 | 0.92 | 0.76–1.13 | 0.93 | 0.76–1.14 |
| C3 | −0.01 | −0.09–0.07 | 0.01 | −0.08–0.09 | 0.89 | 0.75–1.07 | 0.95 | 0.79–1.14 | 0.92 | 0.75–1.13 | 0.98 | 0.79–1.20 |
| C5 | 0.06 | −0.03–0.14 | 0.06 | −0.02–0.15 | 1.03 | 0.85–1.25 | 1.04 | 0.85–1.26 | 1.00 | 0.80–1.25 | 1.02 | 0.81–1.28 |
| C6 | −0.03 | −0.10–0.05 | 0.01 | −0.07–0.08 | 0.87 | 0.73–1.04 | 0.92 | 0.76–1.10 | 0.88 | 0.71–1.08 | 0.93 | 0.76–1.15 |
| C7 | −0.03 | −0.11–0.05 | -0.02 | −0.10–0.06 | 0.95 | 0.78–1.14 | 0.98 | 0.81–1.20 | 0.90 | 0.72–1.12 | 0.93 | 0.74–1.17 |
| C13 | 0.01 | −0.07–0.08 | 0.02 | −0.06–0.10 | 0.90 | 0.74–1.08 | 0.94 | 0.78–1.14 | 0.89 | 0.72–1.11 | 0.95 | 0.76–1.19 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bel-Serrat, S.; Ojeda-Rodríguez, A.; Heinen, M.M.; Buoncristiano, M.; Abdrakhmanova, S.; Duleva, V.; Farrugia Sant’Angelo, V.; Fijałkowska, A.; Hejgaard, T.; Huidumac, C.; et al. Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity—WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017). Nutrients 2019, 11, 511. https://doi.org/10.3390/nu11030511
Bel-Serrat S, Ojeda-Rodríguez A, Heinen MM, Buoncristiano M, Abdrakhmanova S, Duleva V, Farrugia Sant’Angelo V, Fijałkowska A, Hejgaard T, Huidumac C, et al. Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity—WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017). Nutrients. 2019; 11(3):511. https://doi.org/10.3390/nu11030511
Chicago/Turabian StyleBel-Serrat, Silvia, Ana Ojeda-Rodríguez, Mirjam M. Heinen, Marta Buoncristiano, Shynar Abdrakhmanova, Vesselka Duleva, Victoria Farrugia Sant’Angelo, Anna Fijałkowska, Tatjana Hejgaard, Constanta Huidumac, and et al. 2019. "Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity—WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017)" Nutrients 11, no. 3: 511. https://doi.org/10.3390/nu11030511
APA StyleBel-Serrat, S., Ojeda-Rodríguez, A., Heinen, M. M., Buoncristiano, M., Abdrakhmanova, S., Duleva, V., Farrugia Sant’Angelo, V., Fijałkowska, A., Hejgaard, T., Huidumac, C., Hyska, J., Kujundzic, E., Musić Milanović, S., Ovezmyradova, G., Pérez-Farinós, N., Petrauskiene, A., Rito, A. I., Shengelia, L., Taxová Braunerová, R., ... Breda, J. (2019). Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity—WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017). Nutrients, 11(3), 511. https://doi.org/10.3390/nu11030511