The Impact of Intermittent Fasting (Ramadan Fasting) on Psoriatic Arthritis Disease Activity, Enthesitis, and Dactylitis: A Multicentre Study


 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Patients’ Selection and Inclusion
2.3. Measures and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Impact of Intermittent Fasting on Patient Weight
3.3. Impact of Intermittent Fasting on Biochemical Parameters
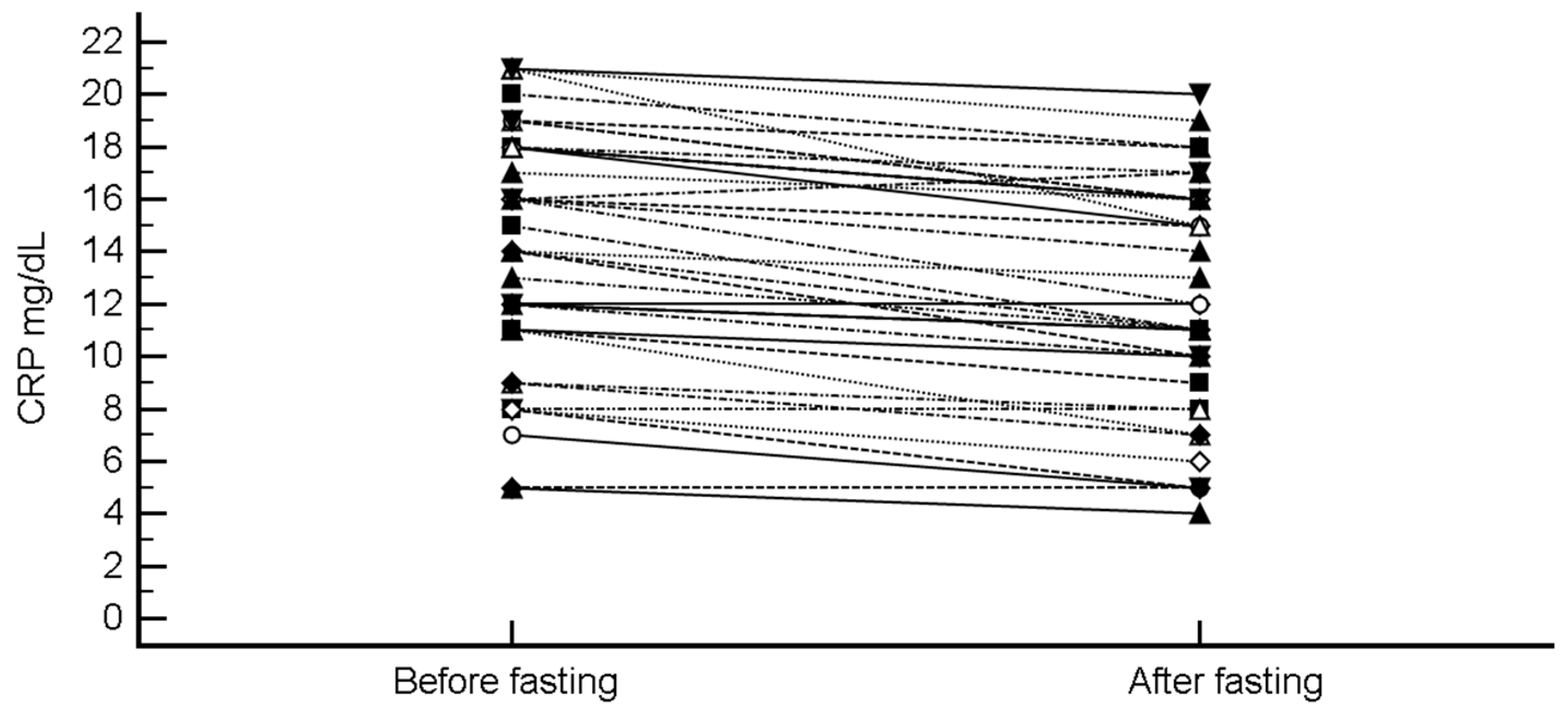
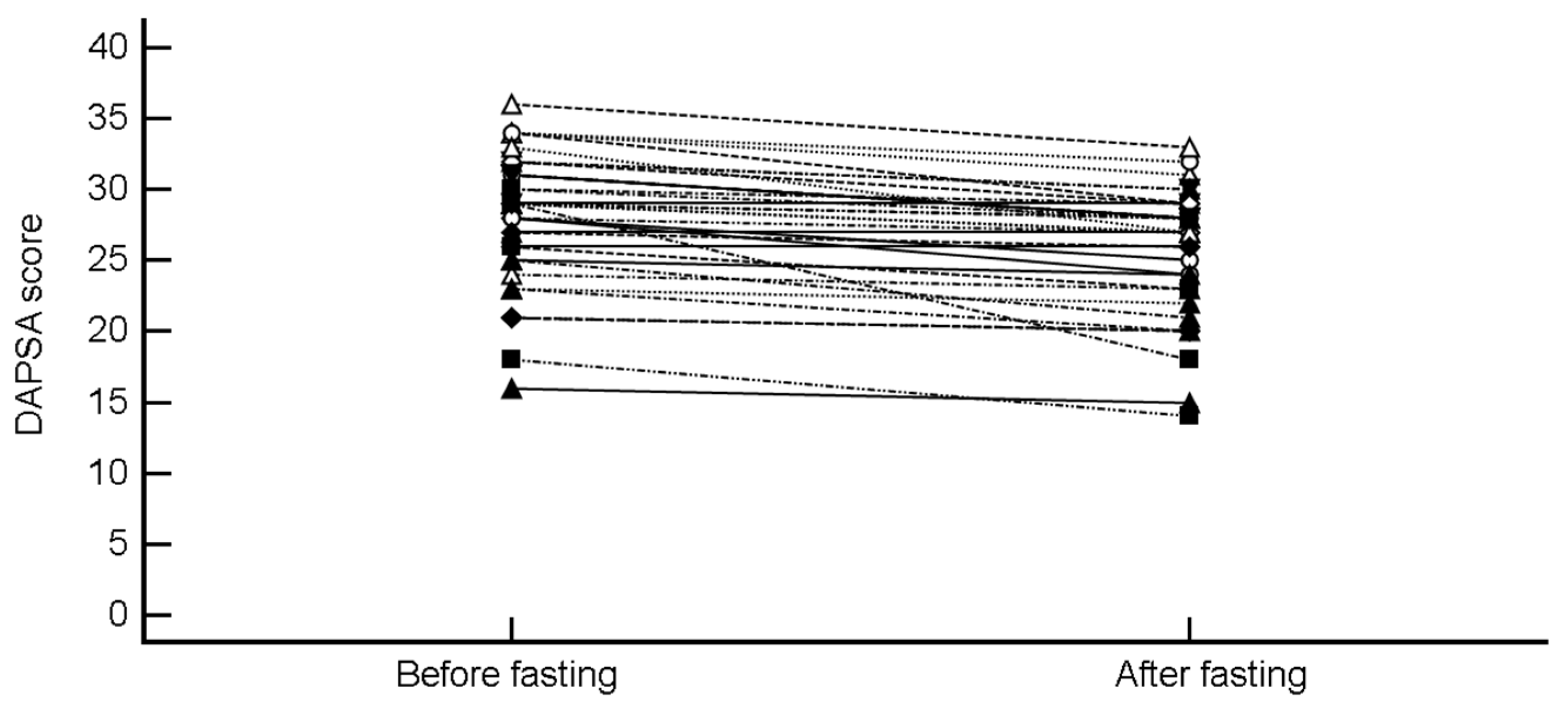
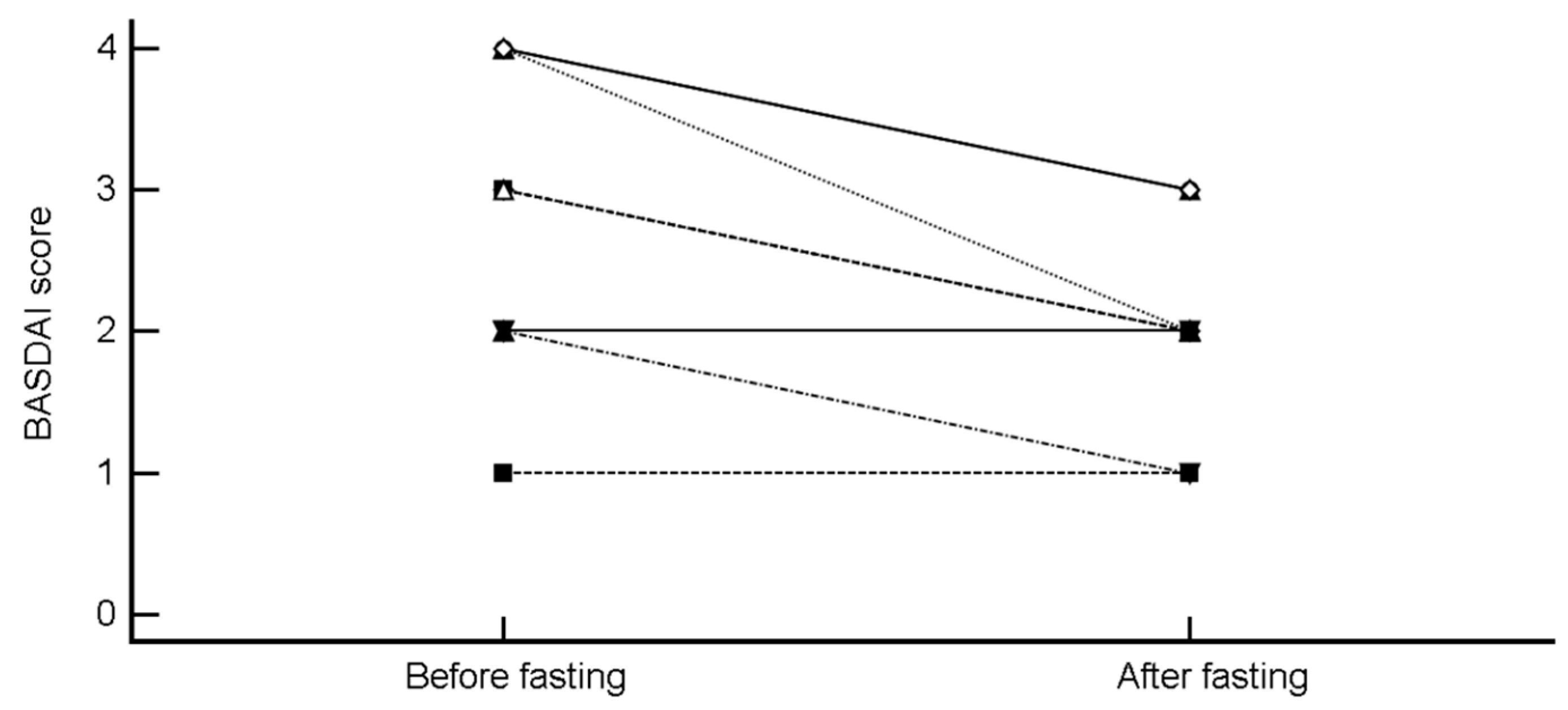
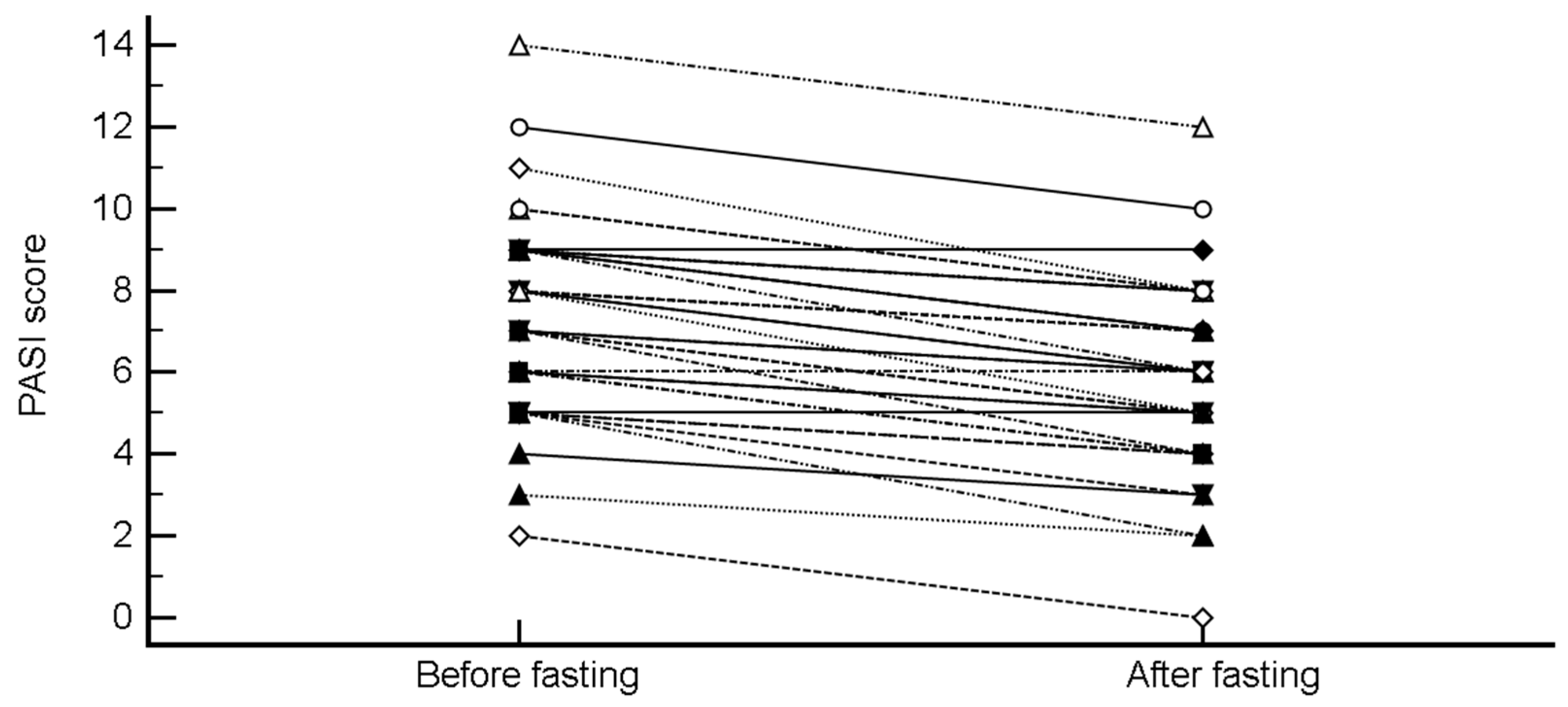
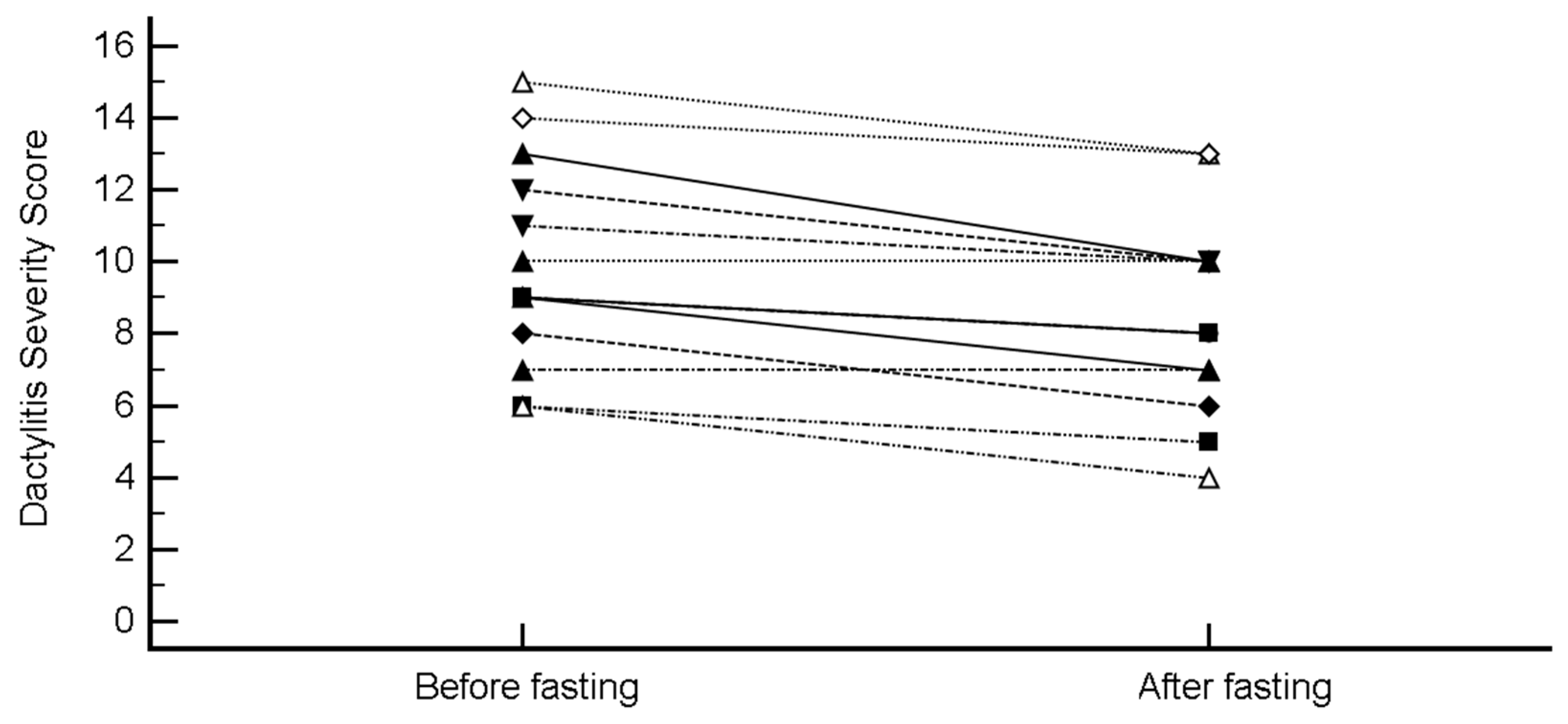
3.4. Impact of Intermittent Fasting on PsA Disease Activity Scores, Enthesitis and Dactylitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ritchlin, C.T.; Colbert, R.A.; Gladman, D.D. Psoriatic arthritis. N. Engl. J. Med. 2017, 376, 957–970. [Google Scholar] [CrossRef] [PubMed]
- Bridgewood, C.; Watad, A.; Cuthbert, R.J.; McGonagle, D. Spondyloarthritis: New insights into clinical aspects, translational immunology and therapeutics. Curr. Opin. Rheumatol. 2018, 30, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Bridgewood, C.; Russell, T.; Marzo-Ortega, H.; Cuthbert, R.; McGonagle, D. The early phases of ankylosing spondylitis: Emerging insights from clinical and basic science. Front. Immunol. 2018, 9, 2668. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Mendelsohn, A.; Sarnes, E. The burden of psoriatic arthritis: A literature review from a global health systems perspective. Pharm. Ther. 2010, 35, 680–689. [Google Scholar]
- Zhu, T.Y.; Li, E.K.; Tam, L.-S. Cardiovascular risk in patients with psoriatic arthritis. Int. J. Rheumatol. 2012, 2012, 714321. [Google Scholar] [CrossRef]
- Watad, A.; Cuthbert, R.J.; Amital, H.; McGonagle, D. Enthesitis: Much more than focal insertion point inflammation. Curr. Rheumatol. Rep. 2018, 20, 41. [Google Scholar] [CrossRef] [PubMed]
- Savage, L.; Goodfield, M.; Horton, L.; Watad, A.; Hensor, E.; Emery, P.; Wakefield, R.; Wittmann, M.; McGonagle, D. Regression of Peripheral Subclinical Enthesopathy in Therapy-Naive Patients Treated with Ustekinumab for Moderate-to-Severe Chronic Plaque Psoriasis: A Fifty-Two-Week, Prospective, Open-Label Feasibility Study. Arthritis. Rheumatol. 2018. [Google Scholar] [CrossRef]
- McGonagle, D.; Tan, A.L.; Watad, A.; Helliwell, P. Pathophysiology, assessment and treatment of psoriatic dactylitis. Nat. Rev. Rheumatol. 2019, 15, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Adawi, M.; Watad, A.; Brown, S.; Aazza, K.; Aazza, H.; Zouhir, M.; Sharif, K.; Ghanayem, K.; Farah, R.; Mahagna, H.; et al. Ramadan fasting exerts immunomodulatory effects: Insights from a systematic review. Front. Immunol. 2017, 8, 1144. [Google Scholar] [CrossRef]
- Hafstrom, I.; Ringertz, B.; Gyllenhammar, H.; Palmblad, J.; Harms-Ringdahl, M. Effects of fasting on disease activity, neutrophil function, fatty acid composition, and leukotriene biosynthesis in patients with rheumatoid arthritis. Arthritis Rheum. 1988, 31, 585–592. [Google Scholar] [CrossRef] [Green Version]
- Damiani, G.; Watad, A.; Bridgewood, C.; Pigatto, D.P.; Pacifico, A.; Malagoli, P.; Bragazzi, L.N.; Adawi, M. The impact of ramadan fasting on the reduction of PASI score, in moderate-to-severe psoriatic patients: A real-life multicenter study. Nutrients 2019, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Association of changes in diet quality with total and cause-specific mortality. N. Engl. J. Med. 2017, 377, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Dahan, S.; Segal, Y.; Shoenfeld, Y. Dietary factors in rheumatic autoimmune diseases: A recipe for therapy? Nat. Rev. Rheumatol. 2017, 13, 348. [Google Scholar] [CrossRef]
- Manzel, A.; Muller, D.N.; Hafler, D.A.; Erdman, S.E.; Linker, R.A.; Kleinewietfeld, M. Role of “Western diet” in inflammatory autoimmune diseases. Curr. Allergy Asthma Rep. 2014, 14, 404. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Balato, N.; Di Somma, C.; Macchia, P.E.; Napolitano, M.; Savanelli, M.C.; Esposito, K.; Colao, A.; Savastano, S. Nutrition and psoriasis: Is there any association between the severity of the disease and adherence to the Mediterranean diet? J. Transl. Med. 2015, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Tridon, A.; Beaufrère, B.; Caldefie, F.; Portefaix, G.; Chassagne, J.; Moreau, K.; Cynober, L.; Vasson, M.-P.; Boirie, Y.; Walrand, S. Specific and nonspecific immune responses to fasting and refeeding differ in healthy young adult and elderly persons. Am. J. Clin. Nutr. 2001, 74, 670–678. [Google Scholar] [CrossRef]
- Husted, J.A.; Thavaneswaran, A.; Chandran, V.; Eder, L.; Rosen, C.F.; Cook, R.J.; Gladman, D.D. Cardiovascular and other comorbidities in patients with psoriatic arthritis: A comparison with patients with psoriasis. Arthritis Care Res. 2011, 63, 1729–1735. [Google Scholar] [CrossRef] [Green Version]
- Jon Love, T.; Zhu, Y.; Zhang, Y.; Wall-Burns, L.; Ogdie, A.; Gelfand, J.M.; Choi, H.K. Obesity and the risk of psoriatic arthritis: A population-based study. Ann. Rheum. Dis. 2012, 71, 1273. [Google Scholar] [CrossRef]
- Soltani-Arabshahi, R.; Wong, B.; Feng, B.-J.; Goldgar, D.E.; Duffin, K.C.; Krueger, G.G. Obesity in early adulthood as a risk factor for psoriatic arthritisearly adult obesity and psoriatic arthritis. Arch. Dermatol. 2010, 146, 721–726. [Google Scholar] [CrossRef]
- Cañete, J.D.; Mease, P. The link between obesity and psoriatic arthritis. Ann. Rheum. Dis. 2012, 71, 1265. [Google Scholar] [CrossRef]
- Torres-Ruiz, J.; Sulli, A.; Cutolo, M.; Shoenfeld, Y. Air travel, circadian rhythms/hormones, and autoimmunity. Clin. Rev. Allergy Immunol. 2017, 53, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Haus, E.; Smolensky, M. Biological clocks and shift work: Circadian dysregulation and potential long-term effects. Cancer Causes Control 2006, 17, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Merrow, M. The circadian clock and human health. Curr. Biol. 2016, 26, R432–R443. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, A.B.; Vitaterna, O.; Haugh, I.M.; Bavishi, A.A.; Zee, P.C.; Turek, F.W.; Sheldon, S.H.; Silverberg, J.I.; Paller, A.S. Nocturnal eczema: Review of sleep and circadian rhythms in children with atopic dermatitis and future research directions. Clin. Rev. Allergy Immunol. 2015, 136, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Scheiermann, C.; Kunisaki, Y.; Frenette, P.S. Circadian control of the immune system. Nat. Rev. Immunol. 2013, 13, 190. [Google Scholar] [CrossRef]
- Bahammam, A.S.; Alaseem, A.M.; Alzakri, A.A.; Sharif, M.M. The effects of Ramadan fasting on sleep patterns and daytime sleepiness: An objective assessment. J. Res. Med. Sci. 2013, 18, 127–131. [Google Scholar]
- Qasrawi, S.O.; Pandi-Perumal, S.R.; BaHammam, A.S. The effect of intermittent fasting during Ramadan on sleep, sleepiness, cognitive function, and circadian rhythm. Sleep Breath 2017, 21, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Venneri, M.A.; Hasenmajer, V.; Fiore, D.; Sbardella, E.; Pofi, R.; Graziadio, C.; Gianfrilli, D.; Pivonello, C.; Negri, M.; Naro, F. Circadian rhythm of glucocorticoid administration entrains clock genes in immune cells: A DREAM trial ancillary study. J. Clin. Endocrinol. Metab. 2018, 103, 2998–3009. [Google Scholar] [CrossRef]
- Logan, R.W.; Zhang, C.; Murugan, S.; O’Connell, S.; Levitt, D.; Rosenwasser, A.M.; Sarkar, D.K. Chronic shift-lag alters the circadian clock of NK cells and promotes lung cancer growth in rats. J. Immunol. 2012, 188, 2583–2591. [Google Scholar] [CrossRef]
- Castanon-Cervantes, O.; Wu, M.; Ehlen, J.C.; Paul, K.; Gamble, K.L.; Johnson, R.L.; Besing, R.C.; Menaker, M.; Gewirtz, A.T.; Davidson, A.J. Dysregulation of inflammatory responses by chronic circadian disruption. J. Immunol. 2010, 185, 5796–5805. [Google Scholar] [CrossRef]
- Gupta, M.A.; Simpson, F.C.; Gupta, A.K. Psoriasis and sleep disorders: A systematic review. Sleep Med. Rev. 2016, 29, 63–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, N.; Nakamura, Y.; Aoki, R.; Ishimaru, K.; Ogawa, H.; Okumura, K.; Shibata, S.; Shimada, S.; Nakao, A. Circadian gene clock regulates psoriasis-like skin inflammation in mice. J. Investig. Dermatol. 2015, 135, 3001–3008. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M. Circadian rhythms and rheumatoid arthritis. Joint Bone Spine 2018. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Sellami, M.; Salem, I.; Conic, R.; Kimak, M.; Pigatto, P.D.M.; Damiani, G. Fasting and Its Impact on Skin Anatomy, Physiology, and Physiopathology: A Comprehensive Review of the Literature. Nutrients 2019, 11, 249. [Google Scholar] [CrossRef] [PubMed]
- Spies, C.M.; Straub, R.H.; Cutolo, M.; Buttgereit, F. Circadian rhythms in rheumatology—A glucocorticoid perspective. Arthritis Res. Ther. 2014, 16, S3. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | |
|---|---|---|
| Age (years) | 43.32 ± 7.81 (median 43) | |
| Gender (%) | Male | 14 (37.8%) |
| Female | 23 (62.2%) | |
| BMI (kg/m2) | 26.16 ± 1.59 | |
| Disease duration (years) | 7.59 ± 3.78 (median 8) | |
| Family history positive for PsA | 15 (40.5%) | |
| Country of origin | Egypt | 10 (27.0%) |
| Morocco | 6 (16.2%) | |
| Algeria | 5 (13.5%) | |
| Turkey | 5 (13.5%) | |
| Israel | 3 (8.1%) | |
| Kurdistan | 3 (8.1%) | |
| Afghanistan | 2 (5.4%) | |
| Cyprus | 2 (5.4%) | |
| Jordan | 1 (2.7%) | |
| Enthesitis | 24 (64.9%) | |
| Dactylitis | 13 (35.1%) | |
| Axial involvement | 13 (35.1%) | |
| Peripheral arthritis | 12 (32.4%) | |
| Treatment | Methotrexate | 3 (8.1%) |
| TNF-α blockers | 28 (75.7%) | |
| IL-17 blockers | 6 (16.2%) | |
| Parameter | Before Fasting | After Fasting |
|---|---|---|
| WBC (N/μL) | 7850 ± 430 | 7750 ± 510 |
| Neutrophils (109/L) | 5.4 ± 0.8 | 5.4 ± 0.6 |
| Lymphocytes (109/L) | 2.7 ± 0.4 | 2.8 ± 0.4 |
| RBC (106/μL) | 5.6 ± 1.2 | 5.7 ± 1.1 |
| MCV (fL) | 89.8 ± 2.3 | 90 ± 2.1 |
| Hb (g/dL) | 14.8 ± 1.3 | 14.7 ± 1.4 |
| PLT (1,000/μL) | 215 ± 32 | 216 ± 28 |
| Creatinine (mg/dL) | 0.7 ± 0.1 | 0.7 ± 0.1 |
| Urea (mg/dL) | 7.3 ± 0.9 | 6.9 ± 1.2 |
| AST (IU/L) | 37 ± 5.2 | 38 ± 4 |
| ALT (IU/L) | 35 ± 8.3 | 36 ± 6.7 |
| GGT (IU/L) | 26 ± 5.6 | 26 ± 4 |
| ALK (IU/L) | 48 ± 8 | 47 ± 6.4 |
| CRP (mg/dL) | 14.1 ± 4.7 | 12.2 ± 4.5 |
| Independent Variables | Coefficient | Standard Error (SE) | t | p-Value | rpartial | rsemipartial |
|---|---|---|---|---|---|---|
| Delta BASDAI | ||||||
| (Constant) | 5.04 | |||||
| Age | −0.05 | 0.03 | −1.63 | 0.1480 | −0.52 | 0.48 |
| Therapy | 0.58 | 0.50 | 1.15 | 0.2883 | 0.40 | 0.34 |
| Gender | 0.33 | 0.51 | 0.65 | 0.5397 | 0.24 | 0.19 |
| BMI | −0.14 | 0.15 | −0.95 | 0.3732 | −0.34 | 0.28 |
| Delta CRP | ||||||
| (Constant) | 3.98 | |||||
| Age | −0.03 | 0.03 | −0.83 | 0.4132 | −0.15 | 0.14 |
| Therapy | −0.46 | 0.53 | −0.86 | 0.3942 | −0.15 | 0.15 |
| Gender | 0.48 | 0.57 | 0.85 | 0.3997 | 0.15 | 0.15 |
| BMI | −0.01 | 0.18 | −0.043 | 0.9658 | −0.01 | 0.01 |
| Delta DAPSA | ||||||
| (Constant) | 12.06 | |||||
| Age | −0.05 | 0.05 | −1.10 | 0.2785 | −0.19 | 0.19 |
| Therapy | −0.66 | 0.78 | −0.86 | 0.3991 | −0.15 | 0.14 |
| Gender | 0.94 | 0.83 | 1.14 | 0.2627 | 0.20 | 0.19 |
| BMI | −0.25 | 0.27 | −0.93 | 0.3601 | −0.16 | 0.16 |
| Delta Dactylitis Severity Score | ||||||
| (Constant) | −4.13 | |||||
| Age | 0.01 | 0.02 | 0.41 | 0.6845 | 0.07 | 0.07 |
| Therapy | −0.32 | 0.30 | −1.04 | 0.3063 | −0.18 | 0.17 |
| Gender | −0.52 | 0.32 | −1.60 | 0.1186 | −0.27 | 0.26 |
| BMI | 0.24 | 0.11 | 2.28 | 0.0293 | 0.37 | 0.37 |
| Delta Leeds Enthesitis Index | ||||||
| (Constant) | −1.71 | |||||
| Age | 0.02 | 0.01 | 1.08 | 0.2939 | 0.24 | 0.21 |
| Therapy | 0.57 | 0.26 | 2.22 | 0.0390* | 0.45 | 0.44 |
| Gender | −0.19 | 0.27 | −0.72 | 0.4833 | −0.16 | 0.14 |
| BMI | 0.02 | 0.08 | 0.23 | 0.8212 | 0.05 | 0.04 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adawi, M.; Damiani, G.; Bragazzi, N.L.; Bridgewood, C.; Pacifico, A.; Conic, R.R.Z.; Morrone, A.; Malagoli, P.; Pigatto, P.D.M.; Amital, H.; et al. The Impact of Intermittent Fasting (Ramadan Fasting) on Psoriatic Arthritis Disease Activity, Enthesitis, and Dactylitis: A Multicentre Study. Nutrients 2019, 11, 601. https://doi.org/10.3390/nu11030601
Adawi M, Damiani G, Bragazzi NL, Bridgewood C, Pacifico A, Conic RRZ, Morrone A, Malagoli P, Pigatto PDM, Amital H, et al. The Impact of Intermittent Fasting (Ramadan Fasting) on Psoriatic Arthritis Disease Activity, Enthesitis, and Dactylitis: A Multicentre Study. Nutrients. 2019; 11(3):601. https://doi.org/10.3390/nu11030601
Chicago/Turabian StyleAdawi, Mohammad, Giovanni Damiani, Nicola Luigi Bragazzi, Charlie Bridgewood, Alessia Pacifico, Rosalynn R. Z. Conic, Aldo Morrone, Piergiorgio Malagoli, Paolo Daniele Maria Pigatto, Howard Amital, and et al. 2019. "The Impact of Intermittent Fasting (Ramadan Fasting) on Psoriatic Arthritis Disease Activity, Enthesitis, and Dactylitis: A Multicentre Study" Nutrients 11, no. 3: 601. https://doi.org/10.3390/nu11030601
APA StyleAdawi, M., Damiani, G., Bragazzi, N. L., Bridgewood, C., Pacifico, A., Conic, R. R. Z., Morrone, A., Malagoli, P., Pigatto, P. D. M., Amital, H., McGonagle, D., & Watad, A. (2019). The Impact of Intermittent Fasting (Ramadan Fasting) on Psoriatic Arthritis Disease Activity, Enthesitis, and Dactylitis: A Multicentre Study. Nutrients, 11(3), 601. https://doi.org/10.3390/nu11030601