Association of Infant Feeding Patterns with Taste Preferences in European Children and Adolescents: A Retrospective Latent Profile Analysis

 ,
,  ,
,  , ,
, ,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Core Questionnaire
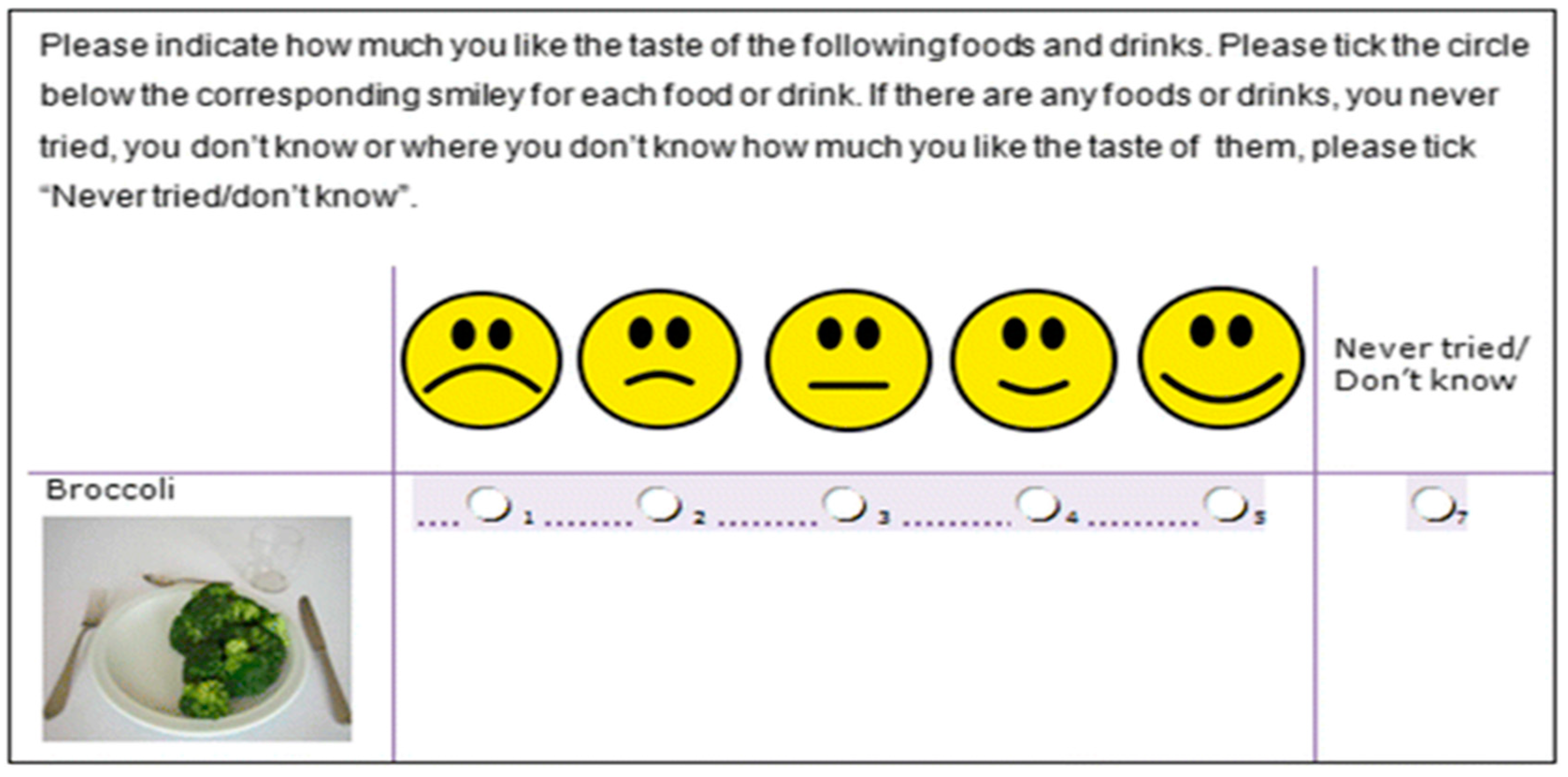
2.3. Food and Beverage Preference Questionnaire
2.4. Taste Preference Scores
2.5. Pregnancy and Early Childhood Questionnaire
- Exclusive breastfeeding (EBF): calculated as the difference in months between age at start of other forms of feeding (formula or other complementary foods) and the age at the start of EBF (at birth); EBF was then classified in categories “None”, “Up to 4 months” and “More than 4 months”,
- Combined breastfeeding (BF&FMF): calculated as the total duration of breastfeeding after birth (breastfeeding combined with any other type of feeding, formula or complementary foods) and classified as “None“, ”Up to 6 months” and “More than 6 months”.
- Exclusive formula milk feeding (EFMF): calculated as the difference of total duration of formula milk feeding in combination with other types of feeding and the duration of either EBF or BF&FMF. It was then categorized as “None”, “Up to 6 months”, “More than 6 months”.
2.6. Statistical Analyses
3. Results
3.1. Study Characteristics
3.2. Association between Exclusive Breastfeeding and Taste Preference
3.3. Association between Combined Breastfeeding and Taste Preference
3.4. Association between Exclusive Formula Feeding and Taste Preference
3.5. Association between Latent Profiles of Feeding Practices and Taste Preferences
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Drewnowski, A. Taste preferences and food intake. Annu. Rev. Nutr. 1997, 17, 237–253. [Google Scholar] [CrossRef] [PubMed]
- IQWiG (Institute for Quality and Efficiency in Health Care). How Does Our Sense of Taste Work? IQWiG (Institute for Quality and Efficiency in Health Care): Cologne, Germany, 2011. [Google Scholar]
- Mennella, J.A. Ontogeny of taste preferences: Basic biology and implications for health. Am. J. Clin. Nutr. 2014, 99, 704s–711s. [Google Scholar] [CrossRef]
- Ikeda, K. New seasonings. Chem. Senses 2002, 27, 847–849. [Google Scholar] [CrossRef] [PubMed]
- Running, C.A.; Craig, B.A.; Mattes, R.D. Oleogustus: The unique taste of fat. Chem. Senses 2015, 40, 507–516. [Google Scholar] [CrossRef]
- Besnard, P.; Passilly-Degrace, P.; Khan, N.A. Taste of fat: A sixth taste modality? Physiol. Rev. 2016, 96, 151–176. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Cowart, B.J.; Mennella, J.A.; Marsh, R.R. Infant salt taste: Developmental, methodological, and contextual factors. Dev. Psychobiol. 1994, 27, 353–365. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Cowart, B.J.; Moran, M. Developmental changes in salt acceptability in human infants. Dev. Psychobiol. 1986, 19, 17–25. [Google Scholar] [CrossRef]
- Fisher, J.O.; Birch, L.L.; Smiciklas-Wright, H.; Picciano, M.F. Breast-feeding through the first year predicts maternal control in feeding and subsequent toddler energy intakes. J. Am. Diet. Assoc. 2000, 100, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Scanlon, K.S.; May, A.; Rose, C.; Birch, L. Bottle-feeding practices during early infancy and eating behaviors at 6 years of age. Pediatrics 2014, 134 (Suppl. 1), S70–S77. [Google Scholar] [CrossRef]
- Sullivan, S.A.; Birch, L.L. Infant dietary experience and acceptance of solid foods. Pediatrics 1994, 93, 271–277. [Google Scholar]
- Michaelsen, K.F.; Europe, W.R.O.f.; Europe, W.H.O.R.O.f. Feeding and Nutrition of Infants and Young Children: Guidelines for the Who European Region, with Emphasis on the Former Soviet Countries; WHO Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Carling, S.J.; Demment, M.M.; Kjolhede, C.L.; Olson, C.M. Breastfeeding duration and weight gain trajectory in infancy. Pediatrics 2015, 135, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Imai, C.M.; Gunnarsdottir, I.; Thorisdottir, B.; Halldorsson, T.I.; Thorsdottir, I. Associations between infant feeding practice prior to six months and body mass index at six years of age. Nutrients 2014, 6, 1608–1617. [Google Scholar] [CrossRef]
- De Kroon, M.L.; Renders, C.M.; Buskermolen, M.P.; Van Wouwe, J.P.; van Buuren, S.; Hirasing, R.A. The terneuzen birth cohort. Longer exclusive breastfeeding duration is associated with leaner body mass and a healthier diet in young adulthood. BMC Pediatr. 2011, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Hirota, Y. Feeding practices in early life and later intake of fruit and vegetables among Japanese toddlers: The Osaka maternal and child health study. Public Health Nutr. 2016, 19, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Chih, T.; Oddy, W. Food variety at 2 years of age is related to duration of breastfeeding. Nutrients 2012, 4, 1464–1474. [Google Scholar] [CrossRef] [PubMed]
- De Lauzon-Guillain, B.; Jones, L.; Oliveira, A.; Moschonis, G.; Betoko, A.; Lopes, C.; Moreira, P.; Manios, Y.; Papadopoulos, N.G.; Emmett, P.; et al. The influence of early feeding practices on fruit and vegetable intake among preschool children in 4 European birth cohorts. Am. J. Clin. Nutr. 2013, 98, 804–812. [Google Scholar] [CrossRef] [Green Version]
- Grieger, J.A.; Scott, J.; Cobiac, L. Dietary patterns and breast-feeding in Australian children. Public Health Nutr. 2011, 14, 1939–1947. [Google Scholar] [CrossRef] [Green Version]
- Skinner, J.D.; Carruth, B.R.; Bounds, W.; Ziegler, P.; Reidy, K. Do food-related experiences in the first 2 years of life predict dietary variety in school-aged children? J. Nutr. Educ. Behav. 2002, 34, 310–315. [Google Scholar] [CrossRef]
- Schwartz, C.; Chabanet, C.; Laval, C.; Issanchou, S.; Nicklaus, S. Breast-feeding duration: Influence on taste acceptance over the first year of life. Br. J. Nutr. 2013, 109, 1154–1161. [Google Scholar] [CrossRef]
- Andreas, N.J.; Kampmann, B.; Le-Doare, K.M. Human breast milk: A review on its composition and bioactivity. Early Hum. Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef]
- De Cosmi, V.; Scaglioni, S.; Agostoni, C. Early taste experiences and later food choices. Nutrients 2017, 9, 107. [Google Scholar] [CrossRef]
- Mennella, J.A.; Beauchamp, G.K. Flavor experiences during formula feeding are related to preferences during childhood. Early Hum. Dev. 2002, 68, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Trabulsi, J.C.; Mennella, J.A. Diet, sensitive periods in flavour learning, and growth. Int. Rev. Psychiatry (Abingdon Engl.) 2012, 24, 219–230. [Google Scholar] [CrossRef] [Green Version]
- North, K.; Emmett, P. Multivariate analysis of diet among three-year-old children and associations with socio-demographic characteristics. The Avon longitudinal study of pregnancy and childhood (alspac) study team. Eur. J. Clin. Nutr. 2000, 54, 73–80. [Google Scholar] [CrossRef]
- Robinson, S.; Marriott, L.; Poole, J.; Crozier, S.; Borland, S.; Lawrence, W.; Law, C.; Godfrey, K.; Cooper, C.; Inskip, H. Dietary patterns in infancy: The importance of maternal and family influences on feeding practice. Br. J. Nutr. 2007, 98, 1029–1037. [Google Scholar] [CrossRef]
- Burnier, D.; Dubois, L.; Girard, M. Exclusive breastfeeding duration and later intake of vegetables in preschool children. Eur. J. Clin. Nutr. 2011, 65, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. The role of food experiences during early childhood in food pleasure learning. Appetite 2016, 104, 3–9. [Google Scholar] [CrossRef]
- Galef, B.G.; Henderson, P.W. Mother’s milk: A determinant of the feeding preferences of weaning rat pups. J. Comp. Physiol. Psychol. 1972, 78, 213–219. [Google Scholar] [CrossRef]
- Galef, B.G.; Sherry, D.F. Mother’s milk: A medium for transmission of cues reflecting the flavor of mother’s diet. J. Comp. Physiol. Psychol. 1973, 83, 374–378. [Google Scholar] [CrossRef]
- Mennella, J.A.; Forestell, C.A.; Morgan, L.K.; Beauchamp, G.K. Early milk feeding influences taste acceptance and liking during infancy. Am. J. Clin. Nutr. 2009, 90, 780s–788s. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Beauchamp, G.K. Mothers’ milk enhances the acceptance of cereal during weaning. Pediatr. Res. 1997, 41, 188–192. [Google Scholar] [CrossRef]
- Galloway, A.T.; Lee, Y.; Birch, L.L. Predictors and consequences of food neophobia and pickiness in young girls. J. Am. Diet. Assoc. 2003, 103, 692–698. [Google Scholar] [CrossRef] [Green Version]
- Cooke, L.J.; Wardle, J.; Gibson, E.L.; Sapochnik, M.; Sheiham, A.; Lawson, M. Demographic, familial and trait predictors of fruit and vegetable consumption by pre-school children. Public Health Nutr. 2004, 7, 295–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennella, J.A.; Daniels, L.M.; Reiter, A.R. Learning to like vegetables during breastfeeding: A randomized clinical trial of lactating mothers and infants. Am. J. Clin. Nutr. 2017, 106, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Hausner, H.; Nicklaus, S.; Issanchou, S.; Molgaard, C.; Moller, P. Breastfeeding facilitates acceptance of a novel dietary flavour compound. Clin. Nutr. (Edinb. Scotl.) 2010, 29, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Forestell, C.A.; Mennella, J.A. Early determinants of fruit and vegetable acceptance. Pediatrics 2007, 120, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, W.; Bammann, K.; Siani, A.; Buchecker, K.; De Henauw, S.; Iacoviello, L.; Hebestreit, A.; Krogh, V.; Lissner, L.; Mårild, S.; et al. The idefics cohort: Design, characteristics and participation in the baseline survey. Int. J. Obes. 2011, 35 (Suppl. 1), S3–S15. [Google Scholar] [CrossRef]
- Hebestreit, A.; Intemann, T.; Siani, A.; De Henauw, S.; Eiben, G.; Kourides, Y.A.; Kovacs, E.; Moreno, L.A.; Veidebaum, T.; Krogh, V.; et al. Dietary patterns of european children and their parents in association with family food environment: Results from the i.Family study. Nutrients 2017, 9, 126. [Google Scholar] [CrossRef]
- Ahrens, W.; Siani, A.; Adan, R.; De Henauw, S.; Eiben, G.; Gwozdz, W.; Hebestreit, A.; Hunsberger, M.; Kaprio, J.; Krogh, V.; et al. Cohort profile: The transition from childhood to adolescence in European children-how i.Family extends the idefics cohort. Int. J. Epidemiol. 2017, 46, 1394–1395j. [Google Scholar] [CrossRef]
- Bel-Serrat, S.; Mouratidou, T.; Pala, V.; Huybrechts, I.; Börnhorst, C.; Fernández-Alvira, J.; Moreno, L. Relative validity of the children’s eating habits questionnaire–food frequency section among young european children: The idefics study. Public Health Nutr. 2014, 17, 266–276. [Google Scholar] [CrossRef]
- Huybrechts, I.; Börnhorst, C.; Pala, V.; Moreno, L.A.; Barba, G.; Lissner, L.; Fraterman, A.; Veidebaum, T.; Hebestreit, A.; Sieri, S.; et al. Evaluation of the children’s eating habits questionnaire used in the idefics study by relating urinary calcium and potassium to milk consumption frequencies among european children. Int. J. Obes. 2011, 35 (Suppl. 1), S69–S78. [Google Scholar] [CrossRef]
- Lanfer, A.; Hebestreit, A.; Ahrens, W.; Krogh, V.; Sieri, S.; Lissner, L.; Eiben, G.; Siani, A.; Huybrechts, I.; Loit, H.M.; et al. Reproducibility of food consumption frequencies derived from the children’s eating habits questionnaire used in the idefics study. Int. J. Obes. 2011, 35 (Suppl. 1), S61–S68. [Google Scholar] [CrossRef]
- Arvidsson, L.; Eiben, G.; Hunsberger, M.; De Bourdeaudhuij, I.; Molnar, D.; Jilani, H.; Thumann, B.; Veidebaum, T.; Russo, P.; Tornatitis, M.; et al. Bidirectional associations between psychosocial well-being and adherence to healthy dietary guidelines in european children: Prospective findings from the idefics study. BMC Public Health 2017, 17, 926. [Google Scholar] [CrossRef]
- Jilani, H.S.; Pohlabeln, H.; Buchecker, K.; Gwozdz, W.; De Henauw, S.; Eiben, G.; Molnar, D.; Moreno, L.A.; Pala, V.; Reisch, L.; et al. Association between parental consumer attitudes with their children’s sensory taste preferences as well as their food choice. PLoS ONE 2018, 13, e0200413. [Google Scholar] [CrossRef]
- UNESCO. International Standard Classification of Education 2012. Available online: http://uis.Unesco.Org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.Pdf (accessed on 27 October 2016).
- Livingstone, M.B.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jilani, H.P.H.; De Henauw, S.; Eiben, G.; Hunsberger, M.; Molnar, D.; Moreno, L.; Pala, V.; Russo, P.; Solea, A.; Veidebaum, T.; et al. Relative validity of a food and beverage preference questionnaire to characterise taste phenotypes in children, adolescents and adult. Nutrient 2019. under revision. [Google Scholar]
- Ricketts, C.D. Fat preferences, dietary fat intake and body composition in children. Eur. J. Clin. Nutr. 1997, 51, 778–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, A.K.; Mennella, J.A. Innate and learned preferences for sweet taste during childhood. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 379–384. [Google Scholar] [CrossRef]
- Paes, V.M.; Ong, K.K.; Lakshman, R. Factors influencing obesogenic dietary intake in young children (0–6 years): Systematic review of qualitative evidence. BMJ Open 2015, 5, e007396. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Jilani, H.S.; Intemann, T.; Bogl, L.H.; Eiben, G.; Molnar, D.; Moreno, L.A.; Pala, V.; Russo, P.; Siani, A.; Solea, A.; et al. Familial aggregation and socio-demographic correlates of taste preferences in european children. BMC Nutr. 2017, 3, 87. [Google Scholar] [CrossRef]
- Parent, A.-S.; Teilmann, G.; Juul, A.; Skakkebaek, N.E.; Toppari, J.; Bourguignon, J.-P. The timing of normal puberty and the age limits of sexual precocity: Variations around the world, secular trends, and changes after migration. Endocr. Rev. 2003, 24, 668–693. [Google Scholar] [CrossRef] [PubMed]
- Lanza, S.T.; Flaherty, B.P.; Collins, L.M. Latent class and latent transition analysis. In Handbook of Psychology; Weiner, I.B., Ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2003. [Google Scholar]
- Lanza, S.T.; Dziak, J.J.; Huang, L.; Xu, S.; Collins, L.M. PROC LCA & PROC LTA Users’ Guide (Version 1.3.2); The Methodology Center; Penn State: University Park, PA, USA, 2011. [Google Scholar]
- Desor, J.A.; Beauchamp, G.K. Longitudinal changes in sweet preferences in humans. Physiol. Behav. 1987, 39, 639–641. [Google Scholar] [CrossRef]
- Johnson, S.L.; McPhee, L.; Birch, L.L. Conditioned preferences: Young children prefer flavors associated with high dietary fat. Physiol. Behav. 1991, 50, 1245–1251. [Google Scholar] [CrossRef]
- Kern, D.L.; McPhee, L.; Fisher, J.; Johnson, S.; Birch, L.L. The postingestive consequences of fat condition preferences for flavors associated with high dietary fat. Physiol. Behav. 1993, 54, 71–76. [Google Scholar] [CrossRef]
- Fernandez-Alvira, J.M. Parental education and frequency of food consumption in European children: The idefics study. Public Health Nutr. 2013, 16, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Van Ansem, W.J.; Schrijvers, C.T.; Rodenburg, G.; van de Mheen, D. Maternal educational level and children’s healthy eating behaviour: Role of the home food environment (cross-sectional results from the inpact study). Int. J. Behav. Nutr. Phys. Act. 2014, 11, 113. [Google Scholar] [CrossRef] [PubMed]
- Cribb, V.L.; Jones, L.R.; Rogers, I.S.; Ness, A.R.; Emmett, P.M. Is maternal education level associated with diet in 10-year-old children? Public Health Nutr. 2011, 14, 2037–2048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sausenthaler, S.; Standl, M.; Buyken, A.; Rzehak, P.; Koletzko, S.; Bauer, C.P.; Schaaf, B.; von Berg, A.; Berdel, D.; Borte, M.; et al. Regional and socio-economic differences in food, nutrient and supplement intake in school-age children in germany: Results from the giniplus and the lisaplus studies. Public Health Nutr. 2011, 14, 1724–1735. [Google Scholar] [CrossRef]
- Sausenthaler, S.; Kompauer, I.; Mielck, A.; Borte, M.; Herbarth, O.; Schaaf, B.; von Berg, A.; Heinrich, J. Impact of parental education and income inequality on children’s food intake. Public Health Nutr. 2007, 10, 24–33. [Google Scholar] [CrossRef]
- Lehto, E.; Ray, C.; Te Velde, S.; Petrova, S.; Duleva, V.; Krawinkel, M.; Behrendt, I.; Papadaki, A.; Kristjansdottir, A.; Thorsdottir, I.; et al. Mediation of parental educational level on fruit and vegetable intake among schoolchildren in ten european countries. Public Health Nutr. 2015, 18, 89–99. [Google Scholar] [CrossRef]
- Mallan, K.M.; Fildes, A.; Magarey, A.M.; Daniels, L.A. The relationship between number of fruits, vegetables, and noncore foods tried at age 14 months and food preferences, dietary intake patterns, fussy eating behavior, and weight status at age 3.7 years. J. Acad. Nutr. Diet. 2016, 116, 630–637. [Google Scholar] [CrossRef]
- Perl, M.A.; Mandic, M.L.; Primorac, L.; Klapec, T.; Perl, A. Adolescent acceptance of different foods by obesity status and by sex. Physiol. Behav. 1998, 65, 241–245. [Google Scholar] [CrossRef]
- Tilgner, L.; Wertheim, E.H.; Paxton, S.J. Effect of social desirability on adolescent girls’ responses to an eating disorders prevention program. Int. J. Eat. Disord. 2004, 35, 211–216. [Google Scholar] [CrossRef]
- Herrmann, D.; Suling, M.; Reisch, L.; Siani, A.; De Bourdeaudhuij, I.; Maes, L.; Santaliestra-Pasias, A.M.; Veidebaum, T.; Molnar, D.; Pala, V.; et al. Repeatability of maternal report on prenatal, perinatal and early postnatal factors: Findings from the idefics parental questionnaire. Int. J. Obes. (Lond.) 2011, 35 (Suppl. 1), S52–S60. [Google Scholar] [CrossRef]
- Natland, S.T.; Andersen, L.F.; Nilsen, T.I.L.; Forsmo, S.; Jacobsen, G.W. Maternal recall of breastfeeding duration twenty years after delivery. BMC Med. Res. Methodol. 2012, 12, 179. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Scanlon, K.S.; Serdula, M.K. The validity and reliability of maternal recall of breastfeeding practice. Nutr. Rev. 2005, 63, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L. The relationship between children’s food preferences and those of their parents. J. Nutr. Educ. 1980, 12, 14–18. [Google Scholar] [CrossRef]


{kind=link}
| Types of Feeding Practices (N = 5526) Duration in Months | Mean/SD | Median | Min/Max |
|---|---|---|---|
| Exclusive Breastfeeding (EBF) | 3.3/2.7 | 4.0 | 0.0/36.0 |
| Combined Breastfeeding (BF&FMF) | 7.2/6.3 | 6.0 | 0.0/36.0 |
| Exclusive Formula Milk Feeding (EFMF) | 4.1/8.1 | 0 | 0.0/48.0 |
| Combined Breastfeeding (BF&FMF) | All | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | None | Up to 6 Months | More Than 6 Months | |||||
| N | % | N | % | N | % | N | % | |
| All | 798 | 100.0 | 2318 | 100.0 | 2410 | 100.0 | 5526 | 100.0 |
| Age Groups | ||||||||
| <12 years | 404 | 50.6 | 1184 | 51.1 | 1359 | 56.4 | 2947 | 53.3 |
| ≥12 years | 394 | 49.4 | 1134 | 48.9 | 1051 | 43.6 | 2579 | 46.7 |
| Sex | ||||||||
| Boys | 410 | 51.4 | 1147 | 49.5 | 1203 | 49.9 | 2760 | 49.9 |
| Girls | 388 | 48.6 | 1171 | 50.5 | 1207 | 50.1 | 2766 | 50.1 |
| SES | ||||||||
| Low –Medium | 511 | 64.0 | 1306 | 56.3 | 921 | 38.2 | 2738 | 49.5 |
| High | 287 | 36.0 | 1012 | 43.7 | 1489 | 61.8 | 2788 | 50.5 |
| Migrant Status | ||||||||
| Both Parents | 69 | 8.6 | 107 | 4.6 | 122 | 5.1 | 298 | 5.4 |
| One parent | 94 | 11.8 | 276 | 11.9 | 170 | 7.1 | 540 | 9.8 |
| Neitherparent | 635 | 79.6 | 1935 | 83.5 | 2118 | 87.9 | 4688 | 84.8 |
| Complementary Food Introduction | ||||||||
| Missing | 76 | 9.5 | 153 | 6.6 | 86 | 3.6 | 315 | 5.7 |
| ≤6 months | 592 | 74.2 | 1892 | 81.6 | 1833 | 76.1 | 4317 | 78.1 |
| >6 months | 130 | 16.3 | 273 | 11.8 | 491 | 20.4 | 894 | 16.2 |
| Sweet Taste Preference | ||||||||
| Low | 350 | 43.9 | 950 | 41.0 | 918 | 38.1 | 2218 | 40.1 |
| High | 448 | 56.1 | 1368 | 59.0 | 1485 | 61.6 | 3301 | 59.7 |
| Missing 1 | 0 | 0 | 0 | 0 | 7 | 0.3 | 7 | 0.1 |
| Fatty Taste Preference | ||||||||
| Low | 317 | 39.7 | 855 | 36.9 | 948 | 39.3 | 2120 | 38.4 |
| High | 481 | 60.3 | 1463 | 63.1 | 1460 | 60.6 | 3404 | 61.6 |
| Missing 1 | 0 | 0 | 0 | 0 | 2 | 0.1 | 2 | 0.0 |
| Bitter Taste Preference | ||||||||
| Low | 546 | 68.4 | 1583 | 68.3 | 1624 | 67.4 | 3753 | 67.9 |
| High | 223 | 27.9 | 666 | 28.7 | 707 | 29.3 | 1596 | 28.9 |
| Missing 1 | 29 | 3.6 | 69 | 3.0 | 79 | 3.3 | 177 | 3.2 |
| Country | ||||||||
| Italy | 170 | 21.3 | 652 | 28.1 | 224 | 9.3 | 1046 | 18.9 |
| Estonia | 57 | 7.1 | 265 | 11.4 | 554 | 23.0 | 876 | 15.9 |
| Cyprus | 228 | 28.6 | 508 | 21.9 | 169 | 7.0 | 905 | 16.4 |
| Sweden | 41 | 5.1 | 208 | 9.0 | 433 | 18.0 | 682 | 12.3 |
| Germany | 181 | 22.7 | 310 | 13.4 | 315 | 13.1 | 806 | 14.6 |
| Hungary | 60 | 7.5 | 242 | 10.4 | 509 | 21.1 | 811 | 14.7 |
| Spain | 61 | 7.6 | 133 | 5.7 | 206 | 8.5 | 400 | 7.2 |
| Sweet Taste (N = 5191) | Fatty Taste (N = 5196) | Bitter Taste (N = 5029) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||||
| EBF | |||||||||
| (ref: None) | 1.00 | 1.00 | 1.00 | ||||||
| ≤4 months | 1.12 | 0.97 | 1.29 | 1.04 | 0.90 | 1.21 | 0.98 | 0.84 | 1.15 |
| >4 months | 1.10 | 0.95 | 1.29 | 1.02 | 0.87 | 1.19 | 0.95 | 0.80 | 1.12 |
| Healthy Diet Adherence Score (HDAS) $ | 0.88 | 0.82 | 0.96 | 0.88 | 0.81 | 0.95 | 1.31 | 1.20 | 1.43 |
| Complementary Food Introduction | |||||||||
| (ref. ≤6 months) | |||||||||
| >6 months | 0.91 | 0.77 | 1.07 | 0.81 | 0.68 | 0.95 | 1.02 | 0.86 | 1.22 |
| Missing | 0.88 | 0.67 | 1.14 | 0.82 | 0.62 | 1.07 | 1.02 | 0.75 | 1.38 |
| SES | |||||||||
| (ref. high) | |||||||||
| Low- medium | 1.11 | 0.98 | 1.26 | 1.14 | 1.009 | 1.30 | 0.88 | 0.77 | 1.017 |
| Sweet Taste (N = 5191) | Fatty Taste (N = 5196) | Bitter Taste (N = 5029) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||||
| BF&FMF | |||||||||
| (ref. None) | 1.00 | 1.00 | 1.00 | ||||||
| ≤6 months | 1.11 | 0.93 | 1.32 | 1.15 | 0.96 | 1.37 | 0.98 | 0.81 | 1.19 |
| >6 months | 1.10 | 0.92 | 1.32 | 1.03 | 0.85 | 1.24 | 1.09 | 0.89 | 1.33 |
| HDAS $ | 0.88 | 0.81 | 0.96 | 0.88 | 0.81 | 0.95 | 1.31 | 1.20 | 1.43 |
| Complementary Food Introduction | |||||||||
| (ref. ≤6 months) | |||||||||
| >6 months | 0.91 | 0.78 | 1.07 | 0.82 | 0.70 | 0.97 | 0.99 | 0.83 | 1.18 |
| Missing | 0.88 | 0.67 | 1.15 | 0.82 | 0.63 | 1.08 | 1.01 | 0.74 | 1.37 |
| SES | |||||||||
| (ref. High) | |||||||||
| Low- medium | 1.11 | 0.98 | 1.26 | 1.14 | 1.004 | 1.29 | 0.90 | 0.78 | 1.03 |
| Sweet Taste (N = 5191) | Fatty Taste (N = 5196) | Bitter Taste (N = 5029) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||||
| EFMF | |||||||||
| (ref. None) | |||||||||
| ≤6 months | 1.001 | 0.84 | 1.18 | 1.09 | 0.92 | 1.29 | 0.85 | 0.71 | 1.02 |
| >6 months | 1.009 | 0.85 | 1.18 | 1.008 | 0.85 | 1.18 | 0.95 | 0.80 | 1.13 |
| HDAS $ | 0.88 | 0.82 | 0.96 | 0.88 | 0.81 | 0.96 | 1.31 | 1.20 | 1.43 |
| Complementary Food Introduction | |||||||||
| (ref. ≤6 months) | |||||||||
| >6 months | 0.91 | 0.78 | 1.07 | 0.81 | 0.69 | 0.95 | 1.004 | 0.84 | 1.19 |
| Missing | 0.87 | 0.67 | 1.14 | 0.82 | 0.62 | 1.07 | 1.01 | 0.75 | 1.37 |
| SES | |||||||||
| (ref. High) | |||||||||
| Low- medium | 1.10 | 0.97 | 1.25 | 1.14 | 1.004 | 1.29 | 0.90 | 0.78 | 1.03 |
| Latent Profiles of Feeding Practices | Frequency | % | ||
| 1. Long period of EBF and mixed breastfeeding, no exclusive use of formula milk, late introduction of complementary foods | 1334 | 24.14 | ||
| Variable | Category | ρ-estimate | ||
| Mixed feeding | more than 6 months | 0.869 | ||
| Exclusive breastfeeding | more than 4 months | 0.853 | ||
| Exclusive formula milk feeding | None | 0.952 | ||
| Introduction of vegetables | after month 6 | 0.674 | ||
| Introduction of fruit | after month 6 | 0.562 | ||
| Introduction of meat | after month 6 | 0.981 | ||
| Introduction of cow milk | after month 6 | 0.988 | ||
| 2. Predominantly formula milk feeding (mixed and exclusive) and late introduction of complementary foods | 774 | 14.01 | ||
| Variable | Category | ρ-estimate | ||
| Mixed feeding | 0–6 months | 0.702 | ||
| Exclusive breastfeeding | 0–4 months | 0.464 | ||
| Exclusive formula milk feeding | more than 6 months | 0.619 | ||
| Introduction of vegetables | after month 6 | 0.832 | ||
| Introduction of fruit | after month 6 | 0.657 | ||
| Introduction of meat | after month 6 | 0.997 | ||
| Introduction of cow milk | after month 6 | 0.973 | ||
| 3. Short duration of EBF and mixed BF without exclusive formula milk use, early introduction of main complementary foods | 2700 | 48.86 | ||
| Variable | Category | ρ-estimate | ||
| Mixed feeding | 0–6 months | 0.541 | ||
| Exclusive breastfeeding | 0–4 months | 0.627 | ||
| Exclusive formula milk feeding | None | 0.764 | ||
| Introduction of vegetables | before month 6 | 0.964 | ||
| Introduction of fruit | before month 6 | 0.988 | ||
| Introduction of meat | before month 6 | 0.681 | ||
| Introduction of cow milk | after month 6 | 0.824 | ||
| 4. No breastfeeding, but exclusive formula milk use, early introduction of main complementary foods. | 718 | 12.99 | ||
| Variable | Category | ρ-estimate | ||
| Mixed feeding | None | 0.841 | ||
| Exclusive breastfeeding | None | 0.994 | ||
| Exclusive formula milk feeding | more than 6 months | 0.583 | ||
| Introduction of vegetables | before month 6 | 0.911 | ||
| Introduction of fruit | before month 6 | 0.983 | ||
| Introduction of meat | before month 6 | 0.645 | ||
| Introduction of cow milk | after month 6 | 0.806 | ||
| Sweet Taste (N = 5191) | Fatty Taste (N = 5196) | Bitter Taste (N = 5029) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | OR | 95% CI | OR | 95%CI | |||
| Profile of FP | |||||||||
| (ref: profile 4) | 1.00 | 1.00 | 1.00 | ||||||
| Profile 1 | 0.99 | 0.81 | 1.20 | 0.97 | 0.79 | 1.19 | 1.09 | 0.88 | 1.36 |
| Profile 2 | 0.90 | 0.72 | 1.13 | 1.13 | 0.90 | 1.43 | 1.05 | 0.82 | 1.35 |
| Profile 3 | 1.09 | 0.91 | 1.30 | 1.11 | 0.92 | 1.33 | 1.06 | 0.87 | 1.29 |
| HDAS $ | 0.88 | 0.82 | 0.96 | 0.88 | 0.81 | 0.95 | 1.31 | 1.20 | 1.43 |
| SES (ref: high) | |||||||||
| Low/medium | 1.11 | 0.97 | 1.25 | 1.14 | 1.004 | 1.29 | 0.89 | 0.78 | 1.02 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sina, E.; Buck, C.; Jilani, H.; Tornaritis, M.; Veidebaum, T.; Russo, P.; Moreno, L.A.; Molnar, D.; Eiben, G.; Marild, S.; et al. Association of Infant Feeding Patterns with Taste Preferences in European Children and Adolescents: A Retrospective Latent Profile Analysis. Nutrients 2019, 11, 1040. https://doi.org/10.3390/nu11051040
Sina E, Buck C, Jilani H, Tornaritis M, Veidebaum T, Russo P, Moreno LA, Molnar D, Eiben G, Marild S, et al. Association of Infant Feeding Patterns with Taste Preferences in European Children and Adolescents: A Retrospective Latent Profile Analysis. Nutrients. 2019; 11(5):1040. https://doi.org/10.3390/nu11051040
Chicago/Turabian StyleSina, Elida, Christoph Buck, Hannah Jilani, Michael Tornaritis, Toomas Veidebaum, Paola Russo, Luis A. Moreno, Denes Molnar, Gabriele Eiben, Staffan Marild, and et al. 2019. "Association of Infant Feeding Patterns with Taste Preferences in European Children and Adolescents: A Retrospective Latent Profile Analysis" Nutrients 11, no. 5: 1040. https://doi.org/10.3390/nu11051040
APA StyleSina, E., Buck, C., Jilani, H., Tornaritis, M., Veidebaum, T., Russo, P., Moreno, L. A., Molnar, D., Eiben, G., Marild, S., Pala, V., Ahrens, W., & Hebestreit, A. (2019). Association of Infant Feeding Patterns with Taste Preferences in European Children and Adolescents: A Retrospective Latent Profile Analysis. Nutrients, 11(5), 1040. https://doi.org/10.3390/nu11051040