Flavonoids and the Risk of Gastric Cancer: An Exploratory Case-Control Study in the MCC-Spain Study


 ,
,  ,
,  , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
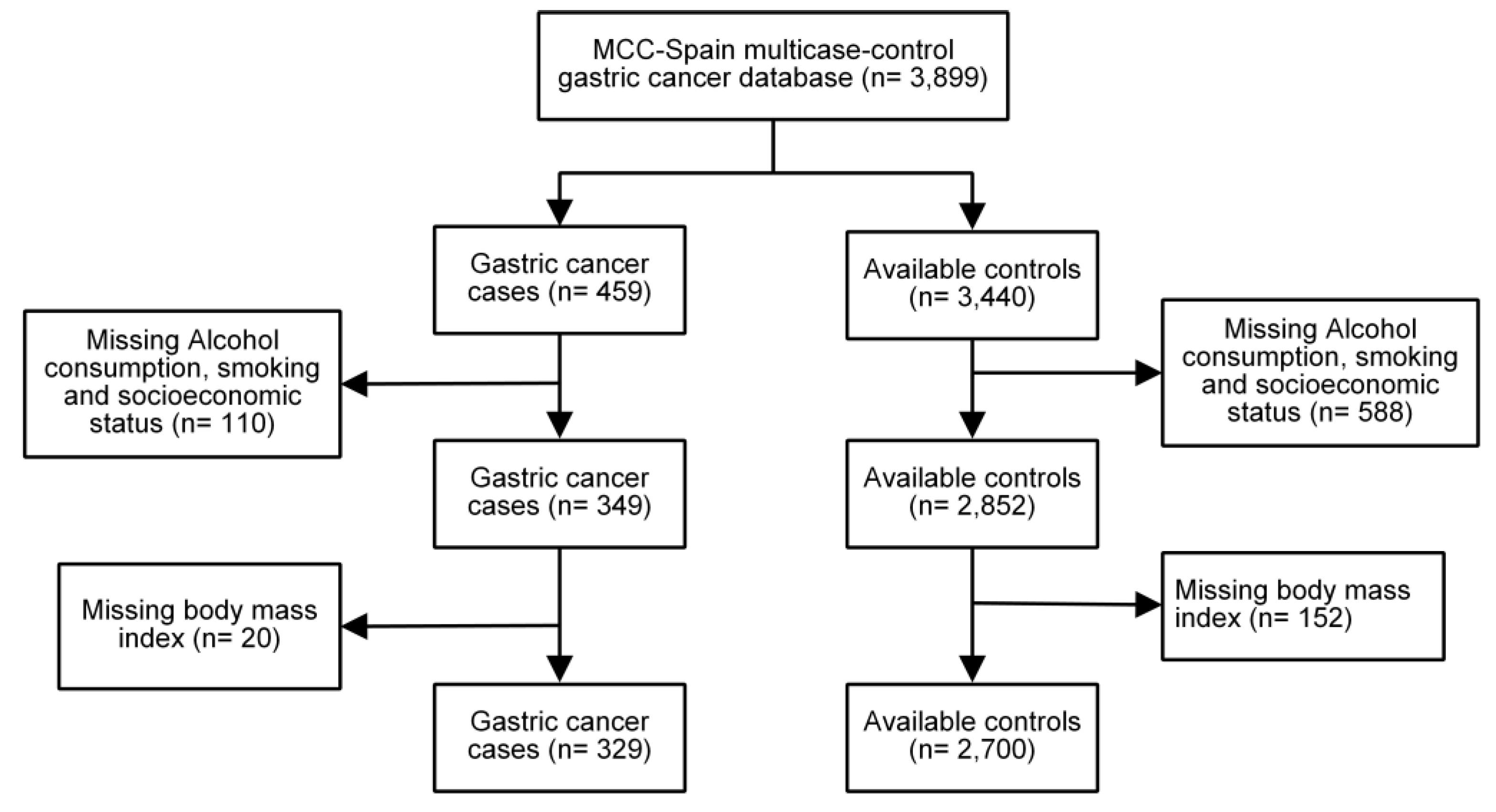
2.1. Study Population
2.2. Variables and Data Collection
2.3. Ethics Approval and Consent to Participate
2.4. Assessment of Flavonoid Intake
2.5. Analysis of Flavonoid Intake
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Available online: https://www.wcrf.org/sites/default/files/Summary-third-expert-report.pdf (accessed on 24 December 2018).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Niksic, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Esteve, J.; et al. Global surveillance of trends in cancer survival 2000-14 (concord-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef]
- Turati, F.; Rossi, M.; Pelucchi, C.; Levi, F.; La Vecchia, C. Fruit and vegetables and cancer risk: A review of southern european studies. Br. J. Nutr. 2015, 113, S102–S110. [Google Scholar] [CrossRef] [PubMed]
- van Duijnhoven, F.J.; Bueno-De-Mesquita, H.B.; Ferrari, P.; Jenab, M.; Boshuizen, H.C.; Ros, M.M.; Casagrande, C.; Tjonneland, A.; Olsen, A.; Overvad, K.; et al. Fruit, vegetables, and colorectal cancer risk: The european prospective investigation into cancer and nutrition. Am. J. Clin. Nutr. 2009, 89, 1441–1452. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J. Fruit and vegetables and cancer risk. Br. J. Cancer 2011, 104, 6–11. [Google Scholar] [CrossRef]
- Norat, T.; Aune, D.; Chan, D.; Romaguera, D. Fruits and vegetables: Updating the epidemiologic evidence for the wcrf/aicr lifestyle recommendations for cancer prevention. Cancer Treat. Res. 2014, 159, 35–50. [Google Scholar]
- Petrick, J.L.; Steck, S.E.; Bradshaw, P.T.; Trivers, K.F.; Abrahamson, P.E.; Engel, L.S.; He, K.; Chow, W.H.; Mayne, S.T.; Risch, H.A.; et al. Dietary intake of flavonoids and oesophageal and gastric cancer: Incidence and survival in the united states of america (USA). Br. J. Cancer 2015, 112, 1291–1300. [Google Scholar] [CrossRef]
- Terao, J. Factors modulating bioavailability of quercetin-related flavonoids and the consequences of their vascular function. Biochem. Pharmacol. 2017, 139, 15–23. [Google Scholar] [CrossRef]
- Cheng, J.; Zhou, L.; Liu, Q.; Tickner, J.; Tan, Z.; Li, X.; Liu, M.; Lin, X.; Wang, T.; Pavlos, N.J.; et al. Cyanidin chloride inhibits ovariectomy-induced osteoporosis by suppressing rankl-mediated osteoclastogenesis and associated signaling pathways. J. Cell. Physiol. 2018, 233, 2502–2512. [Google Scholar] [CrossRef]
- Niedzwiecki, A.; Roomi, M.W.; Kalinovsky, T.; Rath, M. Anticancer efficacy of polyphenols and their combinations. Nutrients 2016, 8, 552. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.H. Potential synergy of phytochemicals in cancer prevention: Mechanism of action. J. Nutr. 2004, 134, S3479–S3485. [Google Scholar] [CrossRef]
- Martinez-Perez, C.; Ward, C.; Cook, G.; Mullen, P.; McPhail, D.; Harrison, D.J.; Langdon, S.P. Novel flavonoids as anti-cancer agents: Mechanisms of action and promise for their potential application in breast cancer. Biochem. Soc. Trans. 2014, 42, 1017–1023. [Google Scholar] [CrossRef]
- Azqueta, A.; Collins, A. Polyphenols and DNA damage: A mixed blessing. Nutrients 2016, 8, 785. [Google Scholar] [CrossRef] [PubMed]
- Ramos, S. Effects of dietary flavonoids on apoptotic pathways related to cancer chemoprevention. J. Nutr. Biochem. 2007, 18, 427–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.; Hlatky, L.; Jeong, Y.S.; Kim, D. Therapeutic effectiveness of anticancer phytochemicals on cancer stem cells. Toxins 2016, 8, 199. [Google Scholar] [CrossRef] [PubMed]
- Sznarkowska, A.; Kostecka, A.; Meller, K.; Bielawski, K.P. Inhibition of cancer antioxidant defense by natural compounds. Oncotarget 2017, 8, 15996–16016. [Google Scholar] [CrossRef]
- Khalid, E.B.; Ayman, E.E.; Rahman, H.; Abdelkarim, G.; Najda, A. Natural products against cancer angiogenesis. Tumour Boil. 2016, 37, 14513–14536. [Google Scholar] [CrossRef]
- Kandaswami, C.; Lee, L.T.; Lee, P.P.; Hwang, J.J.; Ke, F.C.; Huang, Y.T.; Lee, M.T. The antitumor activities of flavonoids. In Vivo 2005, 19, 895–909. [Google Scholar]
- Baltas, N.; Karaoglu, S.A.; Tarakci, C.; Kolayli, S. Effect of propolis in gastric disorders: Inhibition studies on the growth of helicobacter pylori and production of its urease. J. Enzyme Inhib. Med. Chem. 2016, 31, 46–50. [Google Scholar] [CrossRef]
- Harsha, C.; Banik, K.; Bordoloi, D.; Kunnumakkara, A.B. Antiulcer properties of fruits and vegetables: A mechanism based perspective. Food Chem. Toxicol. 2017, 108, 104–119. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Agudo, A.; Lujan-Barroso, L.; Romieu, I.; Ferrari, P.; Knaze, V.; Bueno-de-Mesquita, H.B.; Leenders, M.; Travis, R.C.; Navarro, C.; et al. Dietary flavonoid and lignan intake and gastric adenocarcinoma risk in the european prospective investigation into cancer and nutrition (epic) study. Am. J. Clin. Nutr. 2012, 96, 1398–1408. [Google Scholar] [CrossRef] [PubMed]
- Bo, Y.; Sun, J.; Wang, M.; Ding, J.; Lu, Q.; Yuan, L. Dietary flavonoid intake and the risk of digestive tract cancers: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 24836. [Google Scholar] [CrossRef]
- Xie, Y.; Huang, S.; Su, Y. Dietary flavonols intake and risk of esophageal and gastric cancer: A meta-analysis of epidemiological studies. Nutrients 2016, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Rosato, V.; Bosetti, C.; Lagiou, P.; Parpinel, M.; Bertuccio, P.; Negri, E.; La Vecchia, C. Flavonoids, proanthocyanidins, and the risk of stomach cancer. Cancer Causes Control 2010, 21, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, A.; Arnold, M.; Ferlay, J.; Goodman, K.J.; Forman, D.; Soerjomataram, I. Global patterns of cardia and non-cardia gastric cancer incidence in 2012. Gut 2015, 64, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Lunet, N.; Valbuena, C.; Vieira, A.L.; Lopes, C.; Lopes, C.; David, L.; Carneiro, F.; Barros, H. Fruit and vegetable consumption and gastric cancer by location and histological type: Case-control and meta-analysis. Eur. J. Cancer Prev. 2007, 16, 312–327. [Google Scholar] [CrossRef] [PubMed]
- Metere, A.; Giacomelli, L. Absorption, metabolism and protective role of fruits and vegetables polyphenols against gastric cancer. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5850–5858. [Google Scholar]
- Castano-Vinyals, G.; Aragones, N.; Perez-Gomez, B.; Martin, V.; Llorca, J.; Moreno, V.; Altzibar, J.M.; Ardanaz, E.; de Sanjose, S.; Jimenez-Moleon, J.J.; et al. Population-based multicase-control study in common tumors in spain (mcc-spain): Rationale and study design. Gac. Sanit. 2015, 29, 308–315. [Google Scholar] [CrossRef]
- Ley orgánica 15/1999 de protección de datos de carácter personal. Available online: http://noticias.juridicas.com/base_datos/Admin/lo15-1999.html (accessed on 19 December 2018).
- Garcia-Closas, R.; Garcia-Closas, M.; Kogevinas, M.; Malats, N.; Silverman, D.; Serra, C.; Tardon, A.; Carrato, A.; Castano-Vinyals, G.; Dosemeci, M.; et al. Food, nutrient and heterocyclic amine intake and the risk of bladder cancer. Eur. J. Cancer 2007, 43, 1731–1740. [Google Scholar] [CrossRef]
- Mcc-spain Questuionaries. Available online: http://www.mccspain.org/wp-content/uploads/2016/07/Quest_MCCSpain.pdf (accessed on 9 December 2018).
- Zamora-Ros, R.; Knaze, V.; Luján-Barroso, L.; Romieu, I.; Scalbert, A.; Slimani, N.; Hjartåker, A.; Engeset, D.; Skeie, G.; Overvad, K. Differences in dietary intakes, food sources and determinants of total flavonoids between mediterranean and non-mediterranean countries participating in the european prospective investigation into cancer and nutrition (epic) study. Br. J. Nutr. 2013, 109, 1498–1507. [Google Scholar] [CrossRef]
- Calvert, C.; Cade, J.; Barrett, J.H.; Woodhouse, A. Using cross-check questions to address the problem of mis-reporting of specific food groups on food frequency questionnaires. Ukwcs steering group. United Kingdom women’s cohort study steering group. Eur. J. Clin. Nutr. 1997, 51, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Neveu, V.; Perez-Jimenez, J.; Vos, F.; Crespy, V.; du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D. Phenol-explorer: An online comprehensive database on polyphenol contents in foods. Database 2010. [Google Scholar] [CrossRef] [PubMed]
- Usda Database for the Proanthocyanidin Content of Selected Foods-2004. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/nutrient-data-laboratory/docs/usda-database-for-the-proanthocyanidin-content-of-selected-foods-2004/ (accessed on 10 December 2018).
- Balentine, D.A.; Dwyer, J.T.; Erdman, J.W., Jr.; Ferruzzi, M.G.; Gaine, P.C.; Harnly, J.M.; Kwik-Uribe, C.L. Recommendations on reporting requirements for flavonoids in research. Am. J. Clin. Nutr. 2015, 101, 1113–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Methods Used to Create Phenol-Explorer. Available online: http://phenol-explorer.eu/methods_used (accessed on 23 September 2018).
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, S1220–S1228. [Google Scholar] [CrossRef]
- Zumel, N.M. Practical Data Science with R; Manning Publications Co.: Shelter Island, NY, USA, 2014. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- The Python Language Reference. Available online: https://docs.python.org/3/reference/ (accessed on 28 September 2018).
- R: A Language and Environment for Statistical Computing. Available online: http://softlibre.unizar.es/manuales/Aplicaciones/r/fullrefman.pdf (accessed on 3 September 2018).
- Bertuccio, P.; Rosato, V.; Andreano, A.; Ferraroni, M.; Decarli, A.; Edefonti, V.; La Vecchia, C. Dietary patterns and gastric cancer risk: A systematic review and meta-analysis. Ann. Oncol. 2013, 24, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Godos, J.; Lamuela-Raventos, R.; Ray, S.; Micek, A.; Pajak, A.; Sciacca, S.; D’Orazio, N.; Del Rio, D.; Galvano, F. A comprehensive meta-analysis on dietary flavonoid and lignan intake and cancer risk: Level of evidence and limitations. Mol. Nutr. Food Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Scalbert, A.; Williamson, G. Dietary intake and bioavailability of polyphenols. J. Nutr. 2000, 130, S2073–S2085. [Google Scholar] [CrossRef]
- Zhuang, C.; Zhang, W.; Sheng, C.; Zhang, W.; Xing, C.; Miao, Z. Chalcone: A privileged structure in medicinal chemistry. Chem. Rev. 2017, 117, 7762–7810. [Google Scholar] [CrossRef]
- Woo, H.D.; Lee, J.; Choi, I.J.; Kim, C.G.; Lee, J.Y.; Kwon, O.; Kim, J. Dietary flavonoids and gastric cancer risk in a korean population. Nutrients 2014, 6, 4961–4973. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.K.; Abd Malek, S.N. Xanthohumol induces growth inhibition and apoptosis in ca ski human cervical cancer cells. Evid. Based Complement. Alternat. Med. 2015, 2015, 921306. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.K.; Ho, Y.F.; Malek, S.N. Xanthohumol induces apoptosis and s phase cell cycle arrest in a549 non-small cell lung cancer cells. Pharmacog. Mag. 2015, 11, S275–S283. [Google Scholar]
- Yu, R.J.; Liu, H.B.; Yu, Y.; Liang, L.; Xu, R.; Liang, C.; Tang, J.S.; Yao, X.S. Anticancer activities of proanthocyanidins from the plant urceola huaitingii and their synergistic effects in combination with chemotherapeutics. Fitoterapia 2016, 112, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.M.; Afaq, F.; Khan, N.; Mukhtar, H. Delphinidin, an anthocyanidin in pigmented fruits and vegetables, induces apoptosis and cell cycle arrest in human colon cancer hct116 cells. Mol. Carcinog. 2009, 48, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Bin Hafeez, B.; Asim, M.; Siddiqui, I.A.; Adhami, V.M.; Murtaza, I.; Mukhtar, H. Delphinidin, a dietary anthocyanidin in pigmented fruits and vegetables: A new weapon to blunt prostate cancer growth. Cell Cycle 2008, 7, 3320–3326. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.L.; Chen, P.N.; Chu, S.C.; Kuo, D.Y.; Kuo, W.H.; Chen, J.Y.; Hsieh, Y.S. Peonidin 3-glucoside inhibits lung cancer metastasis by downregulation of proteinases activities and mapk pathway. Nutr. Cancer 2010, 62, 505–516. [Google Scholar] [CrossRef]
- Onoda, C.; Kuribayashi, K.; Nirasawa, S.; Tsuji, N.; Tanaka, M.; Kobayashi, D.; Watanabe, N. (-)-epigallocatechin-3-gallate induces apoptosis in gastric cancer cell lines by down-regulating survivin expression. Int. J. Oncol. 2011, 38, 1403–1408. [Google Scholar] [PubMed]
- Tanaka, T.; Ishii, T.; Mizuno, D.; Mori, T.; Yamaji, R.; Nakamura, Y.; Kumazawa, S.; Nakayama, T.; Akagawa, M. (-)-epigallocatechin-3-gallate suppresses growth of az521 human gastric cancer cells by targeting the dead-box rna helicase p68. Free Radic. Biol. Med. 2011, 50, 1324–1335. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Liu, F.; Guo, H.B.; Li, Y.; Tan, B.B.; Zhang, W.X.; Peng, Y.H. Naringenin inhibits proliferation, migration, and invasion as well as induces apoptosis of gastric cancer sgc7901 cell line by downregulation of akt pathway. Tumour Biol. 2016, 37, 11365–11374. [Google Scholar] [CrossRef]
- Song, H.; Bao, J.; Wei, Y.; Chen, Y.; Mao, X.; Li, J.; Yang, Z.; Xue, Y. Kaempferol inhibits gastric cancer tumor growth: An in vitro and in vivo study. Oncol. Rep. 2015, 33, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wu, D.; Vikash; Song, J.; Wang, J.; Yi, J.; Dong, W. Hesperetin induces the apoptosis of gastric cancer cells via activating mitochondrial pathway by increasing reactive oxygen species. Dig. Dis. Sci. 2015, 60, 2985–2995. [Google Scholar] [CrossRef]
- Chen, J.; Chen, J.; Li, Z.; Liu, C.; Yin, L. The apoptotic effect of apigenin on human gastric carcinoma cells through mitochondrial signal pathway. Tumour Biol. 2014, 35, 7719–7726. [Google Scholar] [CrossRef]
- Hara, A.; Sasazuki, S.; Inoue, M.; Iwasaki, M.; Shimazu, T.; Sawada, N.; Yamaji, T.; Tsugane, S.; Japan Public Health Center–based Prospective Study Group. Isoflavone intake and risk of gastric cancer: A population-based prospective cohort study in japan. Am. J. Clin. Nutr. 2012, 95, 147–154. [Google Scholar] [CrossRef]
- Wada, K.; Tsuji, M.; Tamura, T.; Konishi, K.; Kawachi, T.; Hori, A.; Tanabashi, S.; Matsushita, S.; Tokimitsu, N.; Nagata, C. Soy isoflavone intake and stomach cancer risk in japan: From the takayama study. Int. J. Cancer 2015, 137, 885–892. [Google Scholar] [CrossRef]
- Ekstrom, A.M.; Serafini, M.; Nyren, O.; Wolk, A.; Bosetti, C.; Bellocco, R. Dietary quercetin intake and risk of gastric cancer: Results from a population-based study in Sweden. Ann. Oncol. 2011, 22, 438–443. [Google Scholar] [CrossRef]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Lampe, J.W. Interindividual differences in response to plant-based diets: Implications for cancer risk. Am. J. Clin. Nutr. 2009, 89, S1553–S1557. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Paxton, J.W. The effects of flavonoids on the abc transporters: Consequences for the pharmacokinetics of substrate drugs. Expert Opin. Drug Metab. Toxicol. 2013, 9, 267–285. [Google Scholar] [CrossRef]
- D’Archivio, M.; Filesi, C.; Vari, R.; Scazzocchio, B.; Masella, R. Bioavailability of the polyphenols: Status and controversies. Int. J. Mol. Sci. 2010, 11, 1321–1342. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Alcohol consumption and ethyl carbamate. IARC Monogr. Eval. Carcinog. Risks Hum. 2010, 96, 3–1383. [Google Scholar]
- Knott, C.S.; Coombs, N.; Stamatakis, E.; Biddulph, J.P. All cause mortality and the case for age specific alcohol consumption guidelines: Pooled analyses of up to 10 population based cohorts. BMJ 2015, 350, h384. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Knaze, V.; Rothwell, J.A.; Hemon, B.; Moskal, A.; Overvad, K.; Tjonneland, A.; Kyro, C.; Fagherazzi, G.; Boutron-Ruault, M.C.; et al. Dietary polyphenol intake in europe: The european prospective investigation into cancer and nutrition (epic) study. Eur. J. Nutr. 2016, 55, 1359–1375. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Controls (%) | Cases (%) | |||||
|---|---|---|---|---|---|---|---|
| Total | By Anatomical Subtypes | By Histological Subtypes | |||||
| (n = 2 700) | (n = 329) | Cardia (n = 84) | Non-Cardia (n = 238) | Intestinal (n = 122) | Diffuse (n = 75) | ||
| Age mean ± SD | 63.53 ± 0.21 | 65.40 ± 0.68 | 63.37 ± 1.26 | 66.06 ± 0.82 | 69.49 ± 0.96 | 61.79 (1.56) | |
| Gender (men, %) | 56.2 | 72.6 | 91.6 | 65.5 | 70.4 | 60.0 | |
| Socioeconomic status | High (%) | 448 (16.59) | 27 (8.21) | 9 (10.71) | 18 (7.56) | 8 (6.56) | 8 (10,67) |
| Medium (%) | 1 361 (50.41) | 146 (44.38) | 38 (45.24) | 103 (43.28) | 49 (40.16) | 34 (45.33) | |
| Low (%) | 891 (33.00) | 156 (47.42) | 37 (44.05) | 117(49.16) | 65 (53.28) | 33 (44.00) | |
| Smoking status (%) | yes | 1 531 (56.70) | 201 (61.09) | 65 (77.38) | 130 (54.62) | 60 (49.18) | 45 (60.00) |
| no | 1 169 (43.30) | 128 (38.91) | 19 (22.62) | 108 (45.38) | 62 (50.82) | 30 (40.00) | |
| GC family history (%) | yes | 170 (6.30) | 53 (16.11) | 11 (13.0) | 40 (16.81) | 27 (22.13) | 13 (17.33) |
| no | 2 530 (93.70) | 276 (83.89) | 73 (86.90) | 198 (83.19) | 95 (77.87) | 62 (82.67) | |
| Physical activity (METS*h/week) | <8 | 1 374 (50.89) | 201 (61.09) | 50 (59.52) | 147 (61.76) | 66 (54.10) | 48 (64.00) |
| ≥8 | 1 326 (49.11) | 128 (38.91) | 34 (40.48) | 91 (38.24) | 56 (45.90) | 27 (36.00) | |
| Body mass index (kg/m2) | ≤25 | 1 026 (38.00) | 103 (31.31) | 21 (25) | 80 (33.61) | 41 (33.61) | 32 (42.67) |
| >25–30 | 1 129 (41.81) | 150 (45.59) | 37 (44.05) | 110 (46.22) | 59 (48.36) | 31 (41.33) | |
| ≥30 | 545 (20.19) | 76 (23.10) | 26 (30.95) | 48 (20.17) | 22 (18.03) | 12 (16.00) | |
| Alcohol consumption (g/day) | 0 | 418 (15.48) | 47 (14.29) | 8 (9.52) | 39 (16.39) | 22 (18.03) | 13 (17.33) |
| <12 | 1 179 (43.67) | 103 (31.31) | 16 (19.05) | 84 (35.29) | 40 (32.79) | 27 (36.00) | |
| 12–47 | 787 (29.15) | 101 (30.70) | 34 (40.48) | 66 (27.73) | 30 (24.59) | 22 (29.33) | |
| >47 | 316 (11.70) | 78 (23.71) | 26 (30.95) | 49 (20.59) | 30 (24.59) | 13 (17.33) | |
| Vegetables total intake (g/day), mean ± SD | 191.32 ± 2.42 | 180.80 ± 6.95 | 184.76 ± 18.32 | 177.88 ± 7.04 | 189.25 ± 9.7 | 185.63 ± 13.87 | |
| Red meat intake (g/day), mean ± SD | 64.02 (0.76) | 84.35 (2.94) | 97.50 (6.54) | 80.10 (3.28) | 84.63 (4.58) | 73.12 (5.19) | |
| Sodium intake (mg/day), mean ± SD | 3 008.64 (24.04) | 3 529.30 (86.26) | 3 758.56 (200.71) | 3443.85 (94.85) | 3 403.23 (144.63) | 3 821.43 (187.65) | |
| Total flavonoid intake (mg/day), mean ± SD | 371.25 (3.72) | 358.48 (9.88) | 371.15 (18.63) | 351.18 (11.69) | 367.16 (14.72) | 362.48 (24.51) | |
| Flavonoids Subclass | Flavonoid Intake mg/day ± SD | Most Consumed Foods by Flavonoid Subclass Content-Gastric Cancer-All Controls | |||||
|---|---|---|---|---|---|---|---|
| First (%) | Second (%) | Third (%) | |||||
| Anthocyanins | 22.3 ± 0.35 | Wine [Red] | 31.3 | Sweet cherry | 24.7 | Strawberry | 15.9 |
| Chalcones | 0.004 ± 0.0001 | Beer [Regular] | 98.2 | Beer [Alcohol free] | 1.8 | - | - |
| Dihydrochalcones | 1.15 ± 0.023 | Apple | 95.3 | Non-orange pure juice | 5.5 | - | - |
| Dihydroflavonols | 1.87 ± 0.06 | Wine [Red] | 97.8 | Wine [Rosé/White] | 2.2 | - | - |
| Flavan-3-ols | 26.94 ± 0.33 | Apple | 33.4 | Wine [Red] | 20.55 | Broad bean seed | 13.64 |
| Flavanones | 43.81 ± 0.69 | Orange/Tangerine | 75.1 | Orange pure juice | 21.1 | Tomato | 1.48 |
| Flavones | 3.88 ± 0.08 | Globe artichoke | 24.7 | Orange pure juice | 18.0 | Olives | 16.16 |
| Flavonols | 23.75 ± 0.28 | Swiss chard | 34.2 | Lentils/Chickpea/Common bean | 15.9 | Wine [Red] | 10.7 |
| Isoflavonoids | 1.35 ± 0.11 | Soy milk | 95.3 | Lentils | 4.3 | Nuts | 0.27 |
| Proanthocyanidins | 200.99 ± 2.16 | Beans | 32.5 | Apple | 23.3 | Wine [Red] | 11.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitelli Storelli, F.; Molina, A.J.; Zamora-Ros, R.; Fernández-Villa, T.; Roussou, V.; Romaguera, D.; Aragonés, N.; Obón-Santacana, M.; Guevara, M.; Gómez-Acebo, I.; et al. Flavonoids and the Risk of Gastric Cancer: An Exploratory Case-Control Study in the MCC-Spain Study. Nutrients 2019, 11, 967. https://doi.org/10.3390/nu11050967
Vitelli Storelli F, Molina AJ, Zamora-Ros R, Fernández-Villa T, Roussou V, Romaguera D, Aragonés N, Obón-Santacana M, Guevara M, Gómez-Acebo I, et al. Flavonoids and the Risk of Gastric Cancer: An Exploratory Case-Control Study in the MCC-Spain Study. Nutrients. 2019; 11(5):967. https://doi.org/10.3390/nu11050967
Chicago/Turabian StyleVitelli Storelli, Facundo, Antonio José Molina, Raul Zamora-Ros, Tania Fernández-Villa, Vasiliki Roussou, Dora Romaguera, Nuria Aragonés, Mireia Obón-Santacana, Marcela Guevara, Inés Gómez-Acebo, and et al. 2019. "Flavonoids and the Risk of Gastric Cancer: An Exploratory Case-Control Study in the MCC-Spain Study" Nutrients 11, no. 5: 967. https://doi.org/10.3390/nu11050967
APA StyleVitelli Storelli, F., Molina, A. J., Zamora-Ros, R., Fernández-Villa, T., Roussou, V., Romaguera, D., Aragonés, N., Obón-Santacana, M., Guevara, M., Gómez-Acebo, I., Fernández-Tardón, G., Molina-Barceló, A., Olmedo-Requena, R., Capelo, R., Chirlaque, M. D., Pérez-Gómez, B., Moreno, V., Castilla, J., Rubín-García, M., ... Martín, V. (2019). Flavonoids and the Risk of Gastric Cancer: An Exploratory Case-Control Study in the MCC-Spain Study. Nutrients, 11(5), 967. https://doi.org/10.3390/nu11050967