Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review


 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Selection
2.2. Study Quality Assessment
3. Results
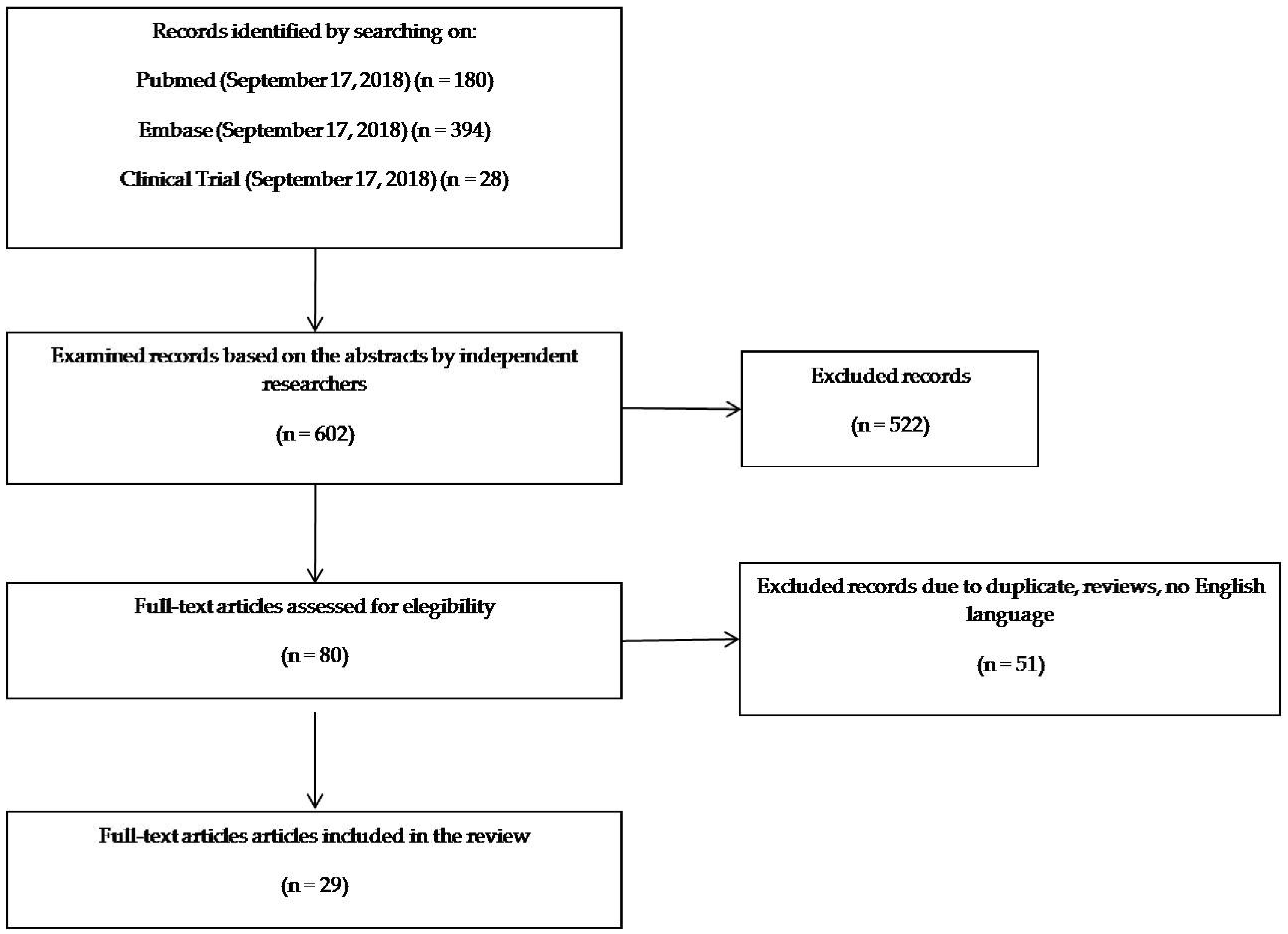
3.1. Search Findings
3.2. Studies Characteristics
3.3. Risk of bias and Quality of Reporting
3.4. Evidence Synthesis
3.4.1. Foetal Growth Restriction and Small for Gestational Age
3.4.2. Prematurity
3.4.3. Neural Tube Defects
3.4.4. Congenital Heart Defects and Gastroschisis
3.4.5. Asthma and Allergy
3.4.6. Body Weight and Metabolic Markers
4. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hambidge, K.M.; Krebs, N.F. Strategies for optimizing maternal nutrition to promote infant development. Reprod Health 2018, 15, 87. [Google Scholar] [CrossRef]
- Simeoni, U.; Armengaud, J.B.; Siddeek, B.; Tolsa, J.F. Perinatal origins of adult disease. Neonatology 2018, 113, 393–399. [Google Scholar] [CrossRef]
- Rodriguez-Rodriguez, P.; Ramiro-Cortijo, D.; Reyes-Hernandez, C.G.; Lopez de Pablo, A.L.; Gonzalez, M.C.; Arribas, S.M. Implication of oxidative stress in fetal programming of cardiovascular disease. Front. Physiol. 2018, 9, 602. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.M.; Vickers, M.H. Utility of small animal models of developmental programming. Methods Mol. Biol. 2018, 1735, 145–163. [Google Scholar] [PubMed]
- Trivedi, M.K.; Sharma, S.; Rifas-Shiman, S.L.; Camargo, C.A., Jr.; Weiss, S.T.; Oken, E.; Gillman, M.W.; Gold, D.R.; DeMeo, D.L.; Litonjua, A.A. Folic acid in pregnancy and childhood asthma: A US cohort. Clin. Pediatr. (Phila) 2018, 57, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Vinding, R.K.; Stokholm, J.; Sevelsted, A.; Chawes, B.L.; Bonnelykke, K.; Barman, M.; Jacobsson, B.; Bisgaard, H. Fish oil supplementation in pregnancy increases gestational age, size for gestational age, and birth weight in infants: A randomized controlled trial. J. Nutr. 2019, 149, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Nardozza, L.M.; Caetano, A.C.; Zamarian, A.C.; Mazzola, J.B.; Silva, C.P.; Marcal, V.M.; Lobo, T.F.; Peixoto, A.B.; Araujo Junior, E. Fetal growth restriction: Current knowledge. Arch. Gynecol. Obstet. 2017, 295, 1061–1077. [Google Scholar] [CrossRef] [PubMed]
- Baschat, A.A. Neurodevelopment after fetal growth restriction. Fetal. Diagn. Ther. 2014, 36, 136–142. [Google Scholar] [CrossRef]
- Pallotto, E.K.; Kilbride, H.W. Perinatal outcome and later implications of intrauterine growth restriction. Clin. Obstet. Gynecol. 2006, 49, 257–269. [Google Scholar] [CrossRef]
- Calkins, K.; Devaskar, S.U. Fetal origins of adult disease. Curr. Probl. Pediatr. Adolesc. Health Care 2011, 41, 158–176. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [PubMed]
- McCowan, L.M.; Harding, J.E.; Stewart, A.W. Customized birthweight centiles predict SGA pregnancies with perinatal morbidity. BJOG 2005, 112, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice bulletin no. 134: Fetal growth restriction. Obstet. Gynecol. 2013, 121, 1122–1133.
- Brantsaeter, A.L.; Haugen, M.; Samuelsen, S.O.; Torjusen, H.; Trogstad, L.; Alexander, J.; Magnus, P.; Meltzer, H.M. A dietary pattern characterized by high intake of vegetables, fruits, and vegetable oils is associated with reduced risk of preeclampsia in nulliparous pregnant Norwegian women. J. Nutr. 2009, 139, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Olafsdottir, A.S.; Forsum, E.; Olsen, S.F.; Thorsdottir, I. Does milk and dairy consumption during pregnancy influence fetal growth and infant birthweight? A systematic literature review. Food Nutr. Res. 2012, 56, 20050. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.F. Consumption of marine n-3 fatty acids during pregnancy as a possible determinant of birth weight. A review of the current epidemiologic evidence. Epidemiol. Rev. 1993, 15, 399–413. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O.; Hediger, M.L.; Schall, J.I.; Khoo, C.S.; Fischer, R.L. Dietary and serum folate: Their influence on the outcome of pregnancy. Am. J. Clin. Nutr. 1996, 63, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Haugen, M.; Myhre, R.; Sengpiel, V.; Englund-Ögge, L.; Nilsen, R.M.; Borgen, I.; Duarte-Salles, T.; Papadopoulou, E.; Vejrup, K.; et al. Diet matters, particularly in pregnancy—Results from MoBa studies of maternal diet and pregnancy outcomes. Norsk. Epidemiologi. 2014, 24, 63–77. [Google Scholar] [CrossRef]
- Salih, M.A.; Murshid, W.R.; Seidahmed, M.Z. Classification, clinical features, and genetics of neural tube defects. Saudi. Med. J. 2014, 35, S5–S14. [Google Scholar]
- Bhide, P.; Gund, P.; Kar, A. Prevalence of congenital anomalies in an Indian maternal cohort: Healthcare, prevention, and surveillance implications. PLoS ONE 2016, 11, e0166408. [Google Scholar] [CrossRef]
- Carpenter, J.L.; Wiebe, T.L.; Cass, D.L.; Olutoye, O.O.; Lee, T.C. Assessing quality of life in pediatric gastroschisis patients using the Pediatric Quality of Life Inventory survey: An institutional study. J. Pediatr. Surg. 2016, 51, 726–729. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W., Jr.; Garcia, F.A.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; Landefeld, C.S.; et al. Folic acid supplementation for the prevention of neural tube defects: US preventive services task force recommendation statement. JAMA 2017, 317, 183–189. [Google Scholar] [PubMed]
- Goodman, J.R.; Peck, J.D.; Landmann, A.; Williams, M.; Elimian, A. An evaluation of nutritional and vasoactive stimulants as risk factors for gastroschisis: A pilot study. J. Matern. Fetal. Neonatal. Med. 2019, 32, 2346–2353. [Google Scholar] [CrossRef] [PubMed]
- Pearce, N.; Ait-Khaled, N.; Beasley, R.; Mallol, J.; Keil, U.; Mitchell, E.; Robertson, C. Worldwide trends in the prevalence of asthma symptoms: Phase III of the international study of asthma and allergies in childhood (ISAAC). Thorax 2007, 62, 758–766. [Google Scholar] [CrossRef]
- Devereux, G.; Seaton, A. Diet as a risk factor for atopy and asthma. J. Allergy Clin. Immunol. 2005, 115, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Seaton, A.; Godden, D.J.; Brown, K. Increase in asthma: A more toxic environment or a more susceptible population? Thorax 1994, 49, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Corella, D.; Coltell, O.; Macian, F.; Ordovas, J.M. Advances in understanding the molecular basis of the mediterranean diet effect. Annu. Rev. Food Sci. Technol. 2018, 9, 227–249. [Google Scholar] [CrossRef] [PubMed]
- Agnoli, C.; Sieri, S.; Ricceri, F.; Giraudo, M.T.; Masala, G.; Assedi, M.; Panico, S.; Mattiello, A.; Tumino, R.; Giurdanella, M.C.; et al. Adherence to a Mediterranean diet and long-term changes in weight and waist circumference in the EPIC-Italy cohort. Nutr. Diabetes 2018, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campa, A.; Martinez-Gonzalez, M.A.; Ruiz-Canela, M. Mediterranean diet and health outcomes in the SUN cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef]
- Bacopoulou, F.; Landis, G.; Rentoumis, A.; Tsitsika, A.; Efthymiou, V. Mediterranean diet decreases adolescent waist circumference. Eur. J. Clin. Invest. 2017, 47, 447–455. [Google Scholar] [CrossRef]
- Mistretta, A.; Marventano, S.; Antoci, M.; Cagnetti, A.; Giogianni, G.; Nolfo, F.; Rametta, S.; Pecora, G.; Marranzano, M. Mediterranean diet adherence and body composition among Southern Italian adolescents. Obes. Res. Clin. Pract. 2017, 11, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Tognon, G.; Hebestreit, A.; Lanfer, A.; Moreno, L.A.; Pala, V.; Siani, A.; Tornaritis, M.; De Henauw, S.; Veidebaum, T.; Molnar, D.; et al. Mediterranean diet, overweight and body composition in children from eight European countries: Cross-sectional and prospective results from the IDEFICS study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, S.; Steegers-Theunissen, R.P.; Vujkovic, M.; den Breeijen, H.; Russcher, H.; Lindemans, J.; Mackenbach, J.; Hofman, A.; Lesaffre, E.E.; Jaddoe, V.V.; et al. The Mediterranean diet and fetal size parameters: The Generation R Study. Br. J. Nutr. 2012, 108, 1399–1409. [Google Scholar] [CrossRef]
- Chatzi, L.; Mendez, M.; Garcia, R.; Roumeliotaki, T.; Ibarluzea, J.; Tardon, A.; Amiano, P.; Lertxundi, A.; Iniguez, C.; Vioque, J.; et al. Mediterranean diet adherence during pregnancy and fetal growth: INMA (Spain) and RHEA (Greece) mother-child cohort studies. Br. J. Nutr. 2012, 107, 135–145. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Saunders, L.; Guldner, L.; Costet, N.; Kadhel, P.; Rouget, F.; Monfort, C.; Thome, J.P.; Multigner, L.; Cordier, S. Effect of a Mediterranean diet during pregnancy on fetal growth and preterm delivery: Results from a French Caribbean Mother-Child Cohort Study (TIMOUN). Paediatr. Perinat. Epidemiol. 2014, 28, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Gomez Roig, M.D.; Mazarico, E.; Ferrero, S.; Montejo, R.; Ibanez, L.; Grima, F.; Vela, A. Differences in dietary and lifestyle habits between pregnant women with small fetuses and appropriate-for-gestational-age fetuses. J. Obstet. Gynaecol. Res. 2017, 43, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Peraita-Costa, I.; Llopis-Gonzalez, A.; Perales-Marin, A.; Sanz, F.; Llopis-Morales, A.; Morales-Suarez-Varela, M. A retrospective cross-sectional population-based study on prenatal levels of adherence to the Mediterranean diet: Maternal profile and effects on the newborn. Int. J. Environ. Res. Public Health 2018, 15, 1530. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; Garcia, A.; Perez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Parlapani, E.; Agakidis, C.; Karagiozoglou-Lampoudi, T.; Sarafidis, K.; Agakidou, E.; Athanasiadis, A.; Diamanti, E. The Mediterranean diet adherence by pregnant women delivering prematurely: Association with size at birth and complications of prematurity. J. Matern. Fetal. Neonatal Med. 2017, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Galiano, J.M.; Olmedo-Requena, R.; Barrios-Rodriguez, R.; Amezcua-Prieto, C.; Bueno-Cavanillas, A.; Salcedo-Bellido, I.; Jimenez-Moleon, J.J.; Delgado-Rodriguez, M. Effect of adherence to a Mediterranean diet and olive oil intake during pregnancy on risk of small for gestational age infants. Nutrients 2018, 10, 1234. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Fernandez-Jarne, E.; Serrano-Martinez, M.; Wright, M.; Gomez-Gracia, E. Development of a short dietary intake questionnaire for the quantitative estimation of adherence to a cardioprotective Mediterranean diet. Eur. J. Clin. Nutr. 2004, 58, 1550–1552. [Google Scholar] [CrossRef] [PubMed]
- Assaf-Balut, C.; Garcia de la Torre, N.; Duran, A.; Fuentes, M.; Bordiu, E.; Del Valle, L.; Familiar, C.; Ortola, A.; Jimenez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef]
- Schroder, H.; Fito, M.; Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Lamuela-Raventos, R.; Ros, E.; Salaverria, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Carmichael, S.L.; Yang, W.; Shaw, G.M. Maternal dietary nutrient intake and risk of preterm delivery. Am. J. Perinatol. 2013, 30, 579–588. [Google Scholar] [PubMed]
- Bodnar, L.M.; Siega-Riz, A.M. A Diet Quality Index for Pregnancy detects variation in diet and differences by sociodemographic factors. Public Health Nutr. 2002, 5, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, T.B.; Osterdal, M.L.; Knudsen, V.K.; Haugen, M.; Meltzer, H.M.; Bakketeig, L.; Olsen, S.F. Association between a Mediterranean-type diet and risk of preterm birth among Danish women: A prospective cohort study. Acta Obstet. Gynecol. Scand. 2008, 87, 325–330. [Google Scholar] [CrossRef]
- Khoury, J.; Henriksen, T.; Christophersen, B.; Tonstad, S. Effect of a cholesterol-lowering diet on maternal, cord, and neonatal lipids, and pregnancy outcome: A randomized clinical trial. Am. J. Obstet. Gynecol. 2005, 193, 1292–1301. [Google Scholar] [CrossRef]
- Haugen, M.; Meltzer, H.M.; Brantsaeter, A.L.; Mikkelsen, T.; Osterdal, M.L.; Alexander, J.; Olsen, S.F.; Bakketeig, L. Mediterranean-type diet and risk of preterm birth among women in the Norwegian Mother and Child Cohort Study (MoBa): A prospective cohort study. Acta Obstet. Gynecol. Scand. 2008, 87, 319–324. [Google Scholar] [CrossRef]
- Smith, L.K.; Draper, E.S.; Evans, T.A.; Field, D.J.; Johnson, S.J.; Manktelow, B.N.; Seaton, S.E.; Marlow, N.; Petrou, S.; Boyle, E.M. Associations between late and moderately preterm birth and smoking, alcohol, drug use and diet: A population-based case-cohort study. Arch Dis. Child. Fetal. Neonatal Ed. 2015, 100, F486–F491. [Google Scholar] [CrossRef] [PubMed]
- Vujkovic, M.; Steegers, E.A.; Looman, C.W.; Ocke, M.C.; van der Spek, P.J.; Steegers-Theunissen, R.P. The maternal Mediterranean dietary pattern is associated with a reduced risk of spina bifida in the offspring. BJOG 2009, 116, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, S.L.; Yang, W.; Feldkamp, M.L.; Munger, R.G.; Siega-Riz, A.M.; Botto, L.D.; Shaw, G. Reduced risks of neural tube defects and orofacial clefts with higher diet quality. Arch. Pediatr. Adolesc. Med. 2012, 166, 121–126. [Google Scholar] [CrossRef]
- Botto, L.D.; Krikov, S.; Carmichael, S.L.; Munger, R.G.; Shaw, G.M.; Feldkamp, M.L. Lower rate of selected congenital heart defects with better maternal diet quality: A population-based study. Arch. Dis. Child. Fetal. Neonatal Ed. 2016, 101, F43–F49. [Google Scholar] [CrossRef]
- Feldkamp, M.L.; Krikov, S.; Botto, L.D.; Shaw, G.M.; Carmichael, S.L. Better diet quality before pregnancy is associated with reduced risk of gastroschisis in Hispanic women. J. Nutr. 2014, 144, 1781–1786. [Google Scholar]
- Chatzi, L.; Torrent, M.; Romieu, I.; Garcia-Esteban, R.; Ferrer, C.; Vioque, J.; Kogevinas, M.; Sunyer, J. Mediterranean diet in pregnancy is protective for wheeze and atopy in childhood. Thorax 2008, 63, 507–513. [Google Scholar] [CrossRef]
- de Batlle, J.; Garcia-Aymerich, J.; Barraza-Villarreal, A.; Anto, J.M.; Romieu, I. Mediterranean diet is associated with reduced asthma and rhinitis in Mexican children. Allergy 2008, 63, 1310–1316. [Google Scholar] [CrossRef]
- Castro-Rodriguez, J.A.; Garcia-Marcos, L.; Sanchez-Solis, M.; Perez-Fernandez, V.; Martinez-Torres, A.; Mallol, J. Olive oil during pregnancy is associated with reduced wheezing during the first year of life of the offspring. Pediatr. Pulmonol. 2010, 45, 395–402. [Google Scholar]
- Psaltopoulou, T.; Naska, A.; Orfanos, P.; Trichopoulos, D.; Mountokalakis, T.; Trichopoulou, A. Olive oil, the Mediterranean diet, and arterial blood pressure: The Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2004, 80, 1012–1018. [Google Scholar] [CrossRef]
- Chatzi, L.; Garcia, R.; Roumeliotaki, T.; Basterrechea, M.; Begiristain, H.; Iniguez, C.; Vioque, J.; Kogevinas, M.; Sunyer, J. Mediterranean diet adherence during pregnancy and risk of wheeze and eczema in the first year of life: INMA (Spain) and RHEA (Greece) mother-child cohort studies. Br. J. Nutr. 2013, 110, 2058–2068. [Google Scholar] [CrossRef]
- Alvarez Zallo, N.; Aguinaga-Ontoso, I.; Alvarez-Alvarez, I.; Marin-Fernandez, B.; Guillen-Grima, F.; Azcona-San Julian, C. Influence of the Mediterranean diet during pregnancy in the development of wheezing and eczema in infants in Pamplona, Spain. Allergol. Immunopathol. (Madr) 2018, 46, 9–14. [Google Scholar] [CrossRef]
- Lange, N.E.; Rifas-Shiman, S.L.; Camargo, C.A., Jr.; Gold, D.R.; Gillman, M.W.; Litonjua, A.A. Maternal dietary pattern during pregnancy is not associated with recurrent wheeze in children. J. Allergy Clin. Immunol. 2010, 126, 250–255. [Google Scholar] [CrossRef]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in Project Viva: A US cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Castro-Rodriguez, J.A.; Ramirez-Hernandez, M.; Padilla, O.; Pacheco-Gonzalez, R.M.; Perez-Fernandez, V.; Garcia-Marcos, L. Effect of foods and Mediterranean diet during pregnancy and first years of life on wheezing, rhinitis and dermatitis in preschoolers. Allergol. Immunopathol. (Madr) 2016, 44, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Gesteiro, E.; Rodriguez Bernal, B.; Bastida, S.; Sanchez-Muniz, F.J. Maternal diets with low healthy eating index or Mediterranean diet adherence scores are associated with high cord-blood insulin levels and insulin resistance markers at birth. Eur. J. Clin. Nutr. 2012, 66, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ruiz-Gutierrez, V.; Covas, M.I.; Fiol, M.; Gomez-Gracia, E.; Lopez-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chatzi, L.; Rifas-Shiman, S.L.; Georgiou, V.; Joung, K.E.; Koinaki, S.; Chalkiadaki, G.; Margioris, A.; Sarri, K.; Vassilaki, M.; Vafeiadi, M.; et al. Adherence to the Mediterranean diet during pregnancy and offspring adiposity and cardiometabolic traits in childhood. Pediatr. Obes. 2017, 12, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Barres, S.; Romaguera, D.; Valvi, D.; Martinez, D.; Vioque, J.; Navarrete-Munoz, E.M.; Amiano, P.; Gonzalez-Palacios, S.; Guxens, M.; Pereda, E.; et al. Mediterranean dietary pattern in pregnant women and offspring risk of overweight and abdominal obesity in early childhood: The INMA birth cohort study. Pediatr. Obes. 2016, 11, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Norat, T.; Vergnaud, A.C.; Mouw, T.; May, A.M.; Agudo, A.; Buckland, G.; Slimani, N.; Rinaldi, S.; Couto, E.; et al. Mediterranean dietary patterns and prospective weight change in participants of the EPIC-PANACEA project. Am. J. Clin. Nutr. 2010, 92, 912–921. [Google Scholar] [CrossRef]
- Gesteiro, E.; Bastida, S.; Rodriguez Bernal, B.; Sanchez-Muniz, F.J. Adherence to Mediterranean diet during pregnancy and serum lipid, lipoprotein and homocysteine concentrations at birth. Eur. J. Nutr. 2015, 54, 1191–1199. [Google Scholar] [CrossRef]
- Mantzoros, C.S.; Sweeney, L.; Williams, C.J.; Oken, E.; Kelesidis, T.; Rifas-Shiman, S.L.; Gillman, M.W. Maternal diet and cord blood leptin and adiponectin concentrations at birth. Clin. Nutr. 2010, 29, 622–626. [Google Scholar] [CrossRef]
- Gonzalez-Nahm, S.; Mendez, M.; Robinson, W.; Murphy, S.K.; Hoyo, C.; Hogan, V.; Rowley, D. Low maternal adherence to a Mediterranean diet is associated with increase in methylation at the MEG3-IG differentially methylated region in female infants. Environ. Epigenet. 2017, 3, dvx007. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Avila, M.; Romieu, I.; Parra, S.; Hernandez-Avila, J.; Madrigal, H.; Willett, W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud. Publica. Mex. 1998, 40, 133–140. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. BMJ 2018, 361, k2234. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trials.gov. Improving Mothers for a Better Prenatal Care Trial Barcelona (IMPACTBCN). Available online: https://clinicaltrials.gov/ct2/show/NCT03166332 (accessed on 17 September 2018).
- Yang, X.; Hsu-Hage, B.; Zhang, H.; Zhang, C.; Zhang, Y. Women with impaired glucose tolerance during pregnancy have significantly poor pregnancy outcomes. Diabetes Care 2002, 25, 1619–1624. [Google Scholar] [CrossRef] [PubMed]
- Czeizel, A.E.; Dudas, I.; Paput, L.; Banhidy, F. Prevention of neural-tube defects with periconceptional folic acid, methylfolate, or multivitamins? Ann. Nutr. Metab. 2011, 58, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Guillemette, L.; Hay, J.L.; Kehler, D.S.; Hamm, N.C.; Oldfield, C.; McGavock, J.M.; Duhamel, T.A. Exercise in pregnancy and children’s cardiometabolic risk factors: A systematic review and meta-analysis. Sports Med. Open 2018, 4, 35. [Google Scholar] [CrossRef] [PubMed]
- Plagemann, A. Perinatal programming and functional teratogenesis: Impact on body weight regulation and obesity. Physiol. Behav. 2005, 86, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Sampson, L. Food frequency questionnaires as a research instrument. Clin. Nutr. 1985, 4, 171–178. [Google Scholar]
- Kazman, J.B.; Scott, J.M.; Deuster, P.A. Using item response theory to address vulnerabilities in FFQ. Br. J. Nutr. 2017, 118, 383–391. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Geographic Area | Study Design | Included Participants | Assessment of Dietary Habits | Assessment of Adherence to MD | Outcomes | Results |
|---|---|---|---|---|---|---|---|
| Timmermans et al. (2012) [38] | Netherlands | Prospective population-based cohort study | 3207 mothers with a spontaneously conceived live-born singleton pregnancy | Semi-quantitative FFQ (293 items) self-administered during early pregnancy (GA < 18 weeks) | Logistic regression analysis was used to identify a comparable dietary pattern, which was labeled MD as it was characterized by higher intakes of pasta, rice, vegetable oils, fish, vegetables and alcohol, and lower intakes of meat, potatoes and fatty sauces. All women were categorized into equal tertiles based on their probability score for the diet, namely: low MDA, medium MDA and high MDA. | Fetal growth | Low MDA resulted associated with lower birth weight (difference in grams at birth −72 [95% CI: −110.8 to 33.3]) |
| Chatzi et al. (2012) [39] | Spain (INMA cohort) and Greece (RHEA cohort) | Prospective population-based cohort study | Spain: 2461 mother-newborn pairs. Greece: 889 mother-newborn pairs | Semi-quantitative FFQ (100 items in IMNA cohort and 250 items in RHEA cohort) administered by trained interviewers during first (IMNA cohort) or mid trimester (RHEA cohort) of pregnancy | Trichopoulou’s score [40] modified for pregnancy | Fetal growth | High MDA was associated with lower risk of delivering a FGR infant (OR 0.5 [95% CI: 0.3–0.9]) in the INMA-Mediterranean cohort. In all cohort high MD adherence increased birth weight in smoking mothers |
| Sauders et al. (2014) [41] | Guadeloupe (French Caribbean Island) | Prospective mother-child cohort study | 728 pregnant women with a live-born singleton pregnancy without major congenital malformations | Semi-quantitative FFQ (214 items) administered by trained interviewers in the days after delivery | Trichopoulou’s score [40] | Fetal growth and prematurity | No overall associations with FGR. No overall association with prematurity. Decreased risk in overweight and obese woman (adjOR 0.7 [95% CI: 0.6–0.9]) |
| Gomez-Roig et al. (2017) [42] | Spain | Cross-sectional study | 46 mothers with SGA fetuses 81 mothers with appropriate for gestational age (AGA) fetuses | Semi-quantitative FFQ (127 items) administered by trained interviewers during the third trimester of pregnancy | Trichopoulou’s score [40] | SGA infants | High MD score was associated with a lower risk of SGA (OR 0.18 [95% CI: 0.74–0.501]) for the third consumer quartile |
| Peraita-Costa et al. (2018) [43] | Spain | Cross-sectional population-based study | 492 mothers | Semi-quantitative FFQ (16 items) self-administered after delivery | Modified KidMed score [44] | SGA infants | The newborns born to women with low MDA presented a higher risk of being SGA (adjOR 1.68 [95% CI: 1.02–5.46]) when adjusting for parental BMI and multiple gestation, but not when adjusting for all significant possible confounders. |
| Parlapani et al. (2017) [45] | Greece | Single-center, prospective, observational cohort study | 82 women who delivered preterm singletons at post conceptional age < 34 weeks | Semi-quantitative FFQ (156 items) self-administered immediately before or after delivery | Panagiotakos dietary score [46] | Fetal growth and prematurity-associated complications | Low MD adherence increased the risk of IUGR, low birth weight, bronchopulmonary dysplasia and necrotizing enterocolitis in preterm infants (<34 weeks) |
| Martinez-Galiano et al. (2018) [47] | Spain | Prospective multicenter matched case-control study (matching criterion: maternal age at delivery) | 518 mothers of singleton SGA infants 518 mothers of singleton infants with normal weight for GA | Semi-quantitative FFQ (137 items) administered by trained interviewers within 2 days after delivery | PREDIMED score [48], Trichopoulou’s score [40], Panagiotakos’ score [46] | SGA infants | MDA and daily consumption of 5 gr of olive oil was associated to a reduced risk of SGA in newborns (adjOR 0.59 [95% CI: 0.38–0.98]) |
| Assaf-Balut et al. (2017) [49] | Spain | Prospective randomized controlled intervention trial | 500 mothers allocated to intervention (MD diet supplemented with extra virgin olive oil and pistachios) and 500 allocated to control (standard diet with limited fat intake) | Semi-quantitative FFQ (14 items) administered by trained interviewed during 4 study visits (at first ultrasound visit at 24–28 GA, at 36–38 GA, and at delivery) to evaluate the adherence to the intervention | MDA screener score [50] | SGA infants and prematurity | MD supplemented with extravergin olive oil and pistachios significantly reduced prematurity rate (p 0.023) and SGA (p 0.001) in the intervention group |
| Carmichael et al. (2013) [51] | United States | Cross-sectional study | 5738 mothers with a singleton pregnancy who delivered non-malformed infants | Semi-quantitative FFQ (58 items) administered by telephone interview 6 weeks—24 months after delivery | Trichopoulou’s score [40] and DQI incorporating pregnancy-specific nutritional recommendations [52] | Prematurity | No association |
| Mikkelse et al. (2008) [53] | Denmark | Prospective cohort study | 35657 pregnant women with a live-born singleton pregnancy | Semi-quantitative FFQ (360 items) self-administered at mid-pregnancy (week 25) by mail | Khoury’s score [54] | Prematurity | High MDA reduced the risk of early preterm birth (adjOR 0.28 [95% CI: 0.11–0.76]). No associations with late preterm delivery. |
| Haugen et al. (2008) [55] | Norway | Prospective cohort study | 26563 pregnant women with a live-born singleton pregnancy | Semi-quantitative FFQ (255 items) self-administered at week 18–22 of pregnancy | Khoury’s score [54] | Prematurity | No association |
| Smith et al. (2015) [56] | United Kingdom | Population-based cohort study | 922 mothers with singleton late and moderate preterm (LMPT) births 965 mothers with singleton term births | Maternal interview shortly after delivery | MDA on the basis of the presence of at least 1 of the following major criteria: five portions of fruit and vegetables every day; fish more than twice a week; meat no more than twice a week; max two cups of coffee/d. | Late and moderately preterm (LMPT) birth | Higher risk of delivering LMPT in not adherent women (RR 1.81 [95% CI: 1.04–3.14]) |
| Vujkovic et al. (2009) [57] | Netherlands | Retrospective multicenter case-control study | 50 mothers of children with spina bifida 81 control mothers | Semi-quantitative FFQ (200 items) administered 14 months after delivery and individually checked for consistency at the hospital or by telephone by the researcher. | Principal component factor analysis (PCA) and reduce rank regression (RRR) were used to identify a comparable dietary pattern, which was labeled MD as it was characterized by high intake of vegetables, fruits, vegetable oils, legumes, fish, alcohol and cereal products and low intakes of potatoes and sweets. | NTDs | Low MDA according to both PCA and RRR, was associated with an increased risk of spina bifida (OR 2.7 [95% CI: 1.2–6.1] and OR 3.5 [95% CI: 1.5–7.9], respectively) |
| Carmicheal et al. (2012) [58] | United States | Retrospective multicenter case-control study | 936 mothers of children with NTDs 2475 mothers of children with orofacial clefts 6147 control mothers | Semi-quantitative FFQ (58 items) administered by telephone interviews 6 weeks–24 months after delivery | Trichopoulou’s score [40] and DQI [52] incorporating pregnancy-specific nutritional recommendations | NTDs and orofacial clefts | High Trichopoulou score and DQI score were protective for NTDs, with a stronger association observed for anencephaly (adjOR 0.64 [95% CI: 0.45–0.92] and 0.49 [95% CI: 0.31–0.75], respectively) |
| Botto et al. (2016) [59] | USA | Population based, multicenter case-control study | 9885 case mothers 9468 control mothers | Semi-quantitative FFQ (58 items) administered by telephone interviews 6 weeks–24 months after delivery | Trichopoulou’s score [40] and the DQI [52] incorporating pregnancy-specific nutritional recommendations | Congenital Heart Defects | High Trichopoulou’s score was protective only for perimembranous ventricular septal defects (14%, OR 0.86 [95% CI: 0.69–1.07]). High DQI was protective for tetralogy of Fallot (OR 0.63 [95% CI: 0.49–0.80]), conotruncal defects (OR 0.76 [95% CI: 0.64–0.91]), atrial septal defects (OR 0.77 [95% CI: 0.63–0.94]) and for all septal defects (OR 0.86 [95% CI: 0.75–1.00]). |
| Feldkamp et al. (2014) [60] | USA | Population based, multicenter case-control study | 1125 gastroschisis cases 9483 controls | 58-item FFQ (58 items) administered by a computerized-assisted telephone interview (CATI) to case and control mothers 6wk to 24 months delivery | Trichopoulou’s score [40] and the DQI [52] incorporating pregnancy-specific nutritional recommendations | Gastroschisis | High Trichopoulou’s score (quartile 2, adjOR0.62 [95% CI: 0.33–1.16]; quartile 3, adjOR0.51 [95% CI: 0.28–0.94]; quartile 4, adjOR0.50 [95% CI: 0.28, 0.90]) and DQI score (quartile 2, adjOR 0.58 [95% CI: 0.40–0.86]; quartile 3, adjOR 0.52 [95% CI: 0.36–0.79]; quartile 4, adjOR 0.48 [95% CI: 0.32–0.76]) were protective for gastroschisis. |
| Chatzi et al. (2008) [61] | Spain | Cohort study | 460 children | Semi-quantitative FFQ (42 items) referred to the pregnancy and administered to mothers 3 months after delivery by a face-to-face interview. Semi-quantitative FFQ (96 items) administered to the parents of the children at 6.5 year of age by an interviewer | Trichopoulou’s score [40] | Wheeze, atopic wheeze and atopy at 6.5 years | High MDS in mothers was protective for persistent wheeze (adjOR 0.22 [95% CI:0.08–0.58]), atopic wheeze (adjOR0.30 [95% CI:0.10–0.90]), and atopy (adjOR 0.55 [95% CI: 0.31–0.97]) in children at 6,5 years |
| De Batlle et al. (2008) [62] | Mexico | Cross-sectional study | 1476 children | Semi-quantitative FFQ (70 items) referred to the pregnancy and self-administered at the children age of 6–7 years | Trichopoulou’s score [40] | Asthma, Wheezing, rhinitis, sneezing, itchy-watery eyes at 6-7 years | High MDS was protective for current sneezing (OR 0.71 [95% CI: 0.53–0.97]). |
| Castro-Rodriguez et al. (2010) [63] | Spain | Cohort study | 1409 infants | Semi-quantitative FFQ (11 items) referred to the pregnancy and self-administered at the children’s aged of 15–18 months | MDS modified from Psaltopoulou [64] | Wheeze at 12 months | MD (p 0.036) and olive oil (p 0.002) were associated with less wheezing. Only olive oil intake remained inversely associated with wheezing (adjOR 0.57 [95% CI: 0.4–0.9]) |
| Chatzi et al. (2013) [65] | Spain (INMA cohort) and Greece (RHEA cohort) | Cohort study | Spain: 1771 mother-newborn pairs. Greece: 745 mother-newborn pairs | Semi-quantitative FFQ (100 items in IMNA cohort and 250 items in RHEA cohort) administered by trained interviewers at mean 13.8 weeks of GA (IMNA cohort) or 14.6 weeks of GA (RHEA cohort) | Trichopoulou’s score [40] modified for pregnancy considering dairy food protective and not including in the score alcohol consumption. | Wheeze and eczema at 12 months | No associations between MD score and wheeze and eczema |
| Alvarez-Zallo et al. (2018) [66] | Spain | Cohort study | 1087 mother-infant pairs | Semi-quantitative FFQ (11-items) referred to the pregnancy and self-administered at the children aged 12–15 months | MDS modified from Psaltopoulou [64] | Wheeze and eczema at 12–15 months | No associations between MD score and wheezing, recurrent wheezing and eczema |
| Lange et al. (2010) [67] | United States | Cohort study | 1376 mother-infant pairs | Semi-quantitative FFQ (166 items) self-administered at the first and second trimesters visits | MD score modified from Trichopoulou [40], Alternate Healthy Eating Index modified for pregnancy [68] and PCA to look at Western and Prudent diets | Wheeze, asthma and atopy at 3 years | No associations between dietary patterns and asthma, atopy or wheezing |
| Castro-Rodriguez et al. (2016) [69] | Spain | Cohort study | 1000 mother-newborn pairs | Semi-quantitative FFQ (11 items) regarding the consumption of foods during pregnancy self-administered at the time point of 1.5 years of children’s life. Semi-quantitative FFQ (11 items) regarding the consumption of food by the child self-administered at the time point of 4 years of life | MDS modified from Psaltopoulou [64] | Wheeze, dermatitis and allergic rhinitis at 4 years | No associations between MD score and wheezing, rhinitis and dermatitis |
| Gesteiro et al. (2012) [70] | Spain | Cross sectional study | 35 women | 169 items FFQ conducted by a trained dietician 3–5 after delivery | Healthy eating index (HEI) adapted for the Spanish population [71] and by a modified MDA scores used in the PREDIMED study [72] | Various insulin sensitivity/resistance biomarkers at birth | Low HEI- or low MDA-score diet delivered infants with high insulinaemia (p 0.048 or p 0.017, respectively), HOMA-IR (p 0.031 or p 0.049, respectively) and glycaemia (p 0.018 or p 0.048, respectively). The relative risk (RR) of high-neonatal glycaemia and insulinaemia were 7.6 (p 0.008) and 6.7 (p 0.017) for low vs. high HEI-score groups. High HOMA-IR and high glucose RR were, respectively, 3.4 (p 0.043) and 3.9 (p 0.016) in neonates from the <7 MDA- vs. >7 MDA-score group. |
| Chatzi et al. (2017) [73] | USA (Project Viva cohort) and Greece (RHEA cohort) | Prospective mother–child cohort study | 997 mother–child pairs from Project Viva and 569 pairs from the RHEA study | In Project Viva, mothers reported their diet since the time of their last menstrual period at study enrolment (median 9.9 weeks gestation) using a validated semi-quantitative FFQ. RHEA participants completed a validated FFQ at mean 14.6 weeks gestation. | Trichopoulou’s score [40] | BMI z-score, waist circumference, skin-fold thickness, systolic and diastolic blood pressure | In the pooled analysis, for each 3-point increment in the MDS, offspring BMI z-score was lower by 0.14 units (95% CI: −0.15 to −0.13), waist circumference by 0.39cm (95% CI: −0.64 to −0.14), the sum of skin-fold thicknesses by 0.63mm (95% CI: 0.98 to −0.28), systolic blood pressure by −1.03 mmHg (95% CI: −1.65 to −0.42) and diastolic blood pressure by −0.57 mmHg (95% CI: −0.98 to −0.16). |
| Fernández-Barrés et al. (2016) [74] | Spain | Population based cohort study | 1827 pairs of mother and children | Validated 101 items FFQ conducted from first to third trimester | RelativeMediterranean diet score (rMED) [75] | BMI and waist circumference | A significant association between higher adherence to MD and lower waist circumference (−0.62 cm [95% CI: −1.1 to −0.14]). |
| Gesteiro et al. (2015) [76] | Spain | Cross sectional study | 35 women | Complete 169 items FFQ guided by a trained dietician conducted at first trimester | Modified MDA scores used in the PREDIMED study [72] | Cord blood lipoprotein and homocysteine concentrations | Mothers at the low MDA-score delivered neonates with high cord blood LDL-c (p 0.049), Apo B (p 0.040), homocysteine (p 0.026) and Apo A1/Apo B ratio (p 0.024). |
| Mantzoros et al. (2010) [77] | USA | Prospective cohort study | 780 women | Slightly modified semi-quantitative FFQ at both the first and second trimester | Trichopoulou’s score [40] | Cord blood leptin and adiponectin concentrations | Closer adherence to a Mediterranean pattern diet during pregnancy was not associated with cord blood leptin (p 0.38) or adiponectin (p 0.93) |
| Gonzalez-Nahm et al. (2017) [78] | USA | Cohort study | 390 women whose infants had DNA methylation data available from cord blood leukocytes | 150 items FFQ at preconception or at first trimester | Modified Trichopoulou’s score [40] | Methylation at the MEG3-IG region | Infants of mothers with a low adherence to a Mediterranean diet had a greater odd of hypo-methylation at the MEG3-IG differentially methylated region (OR 2.80 [95% CI: 1.35−5.82]) |
| Author | Study Type | Tool for Assessment | Quality |
|---|---|---|---|
| Timmermans et al. (2012) [38] | Cohort | STROBE | 24/33—Intermediate |
| Chatzi et al. (2012) [39] | Cohort | STROBE | 27/33—Good |
| Sauders et al. (2014) [41] | Cohort | STROBE | 24/33—Intermediate |
| Gomez-Roig et al. (2017) [42] | Cross Sectional | STROBE | 12/33—Poor |
| Peraita-Costa et al. (2018) [43] | Cross Sectional | STROBE | 16/33—Intermediate |
| Parlapani et al. (2017) [45] | Cohort | STROBE | 21/33—Intermediate |
| Martinez-Galiano et al. (2018) [47] | Case-Control | STROBE | 22/33—Intermediate |
| Assaf-Balut et al. (2017) [49] | RCT | Cochrane ROB Tool | Poor quality due to blindness and allocation concealment |
| Carmichael et al. (2013) [51] | Cross Sectional | STROBE | 11/33—Poor |
| Mikkelsen et al. (2008) [53] | Cohort | STROBE | 19/33—Intermediate |
| Haugen et al. (2008) [55] | Cohort | STROBE | 22/33—Intermediate |
| Smith et al. (2015) [56] | Cohort | STROBE | 26/33—Good |
| Vujkovic et al. (2009) [57] | Case-Control | STROBE | 21/33—Intermediate |
| Carmicheal et al. (2012) [58] | Case-Control | STROBE | 17/33—Intermediate |
| Botto et al. (2016) [59] | Case-Control | STROBE | 18/33—Intermediate |
| Feldkamp et al. (2014) [60] | Case-Control | STROBE | 23/33—Intermediate |
| Chatzi et al. (2008) [61] | Cohort | STROBE | 25/33—Intermediate |
| De Batlle et al. (2008) [62] | Cross Sectional | STROBE | 12/33—Poor |
| Castro-Rodriguez et al. (2010) [63] | Cohort | STROBE | 26/33—Good |
| Chatzi et al. (2013) [65] | Cohort | STROBE | 28/33—Good |
| Alvarez-Zallo et al. (2018) [66] | Cohort | STROBE | 14/33—Poor |
| Lange et al. (2010) [67] | Cohort | STROBE | 31/33—Good |
| Castro-Rodriguez et al. (2016) [69] | Cross Sectional | STROBE | 18/33—Intermediate |
| Gesteiro et al. (2012) [70] | Cross Sectional | STROBE | 16/33—Intermediate |
| Chatzi et al. (2017) [73] | Cohort | STROBE | 26/33—Good |
| Fernández-Barrés et al. (2016) [74] | Cohort | STROBE | 27/33—Good |
| Gesteiro et al. (2015) [76] | Cross Sectional | STROBE | 22/33—Intermediate |
| Mantzoros et al. (2010) [77] | Cohort | STROBE | 25/33—Intermediate |
| Gonzalez-Nahm et al. (2017) [78] | Cohort | STROBE | 13/33—Poor |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biagi, C.; Di Nunzio, M.; Bordoni, A.; Gori, D.; Lanari, M. Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients 2019, 11, 997. https://doi.org/10.3390/nu11050997
Biagi C, Di Nunzio M, Bordoni A, Gori D, Lanari M. Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients. 2019; 11(5):997. https://doi.org/10.3390/nu11050997
Chicago/Turabian StyleBiagi, Carlotta, Mattia Di Nunzio, Alessandra Bordoni, Davide Gori, and Marcello Lanari. 2019. "Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review" Nutrients 11, no. 5: 997. https://doi.org/10.3390/nu11050997
APA StyleBiagi, C., Di Nunzio, M., Bordoni, A., Gori, D., & Lanari, M. (2019). Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients, 11(5), 997. https://doi.org/10.3390/nu11050997