Multidisciplinary Integrated Metabolic Rehabilitation in Elderly Obese Patients: Effects on Cardiovascular Risk Factors, Fatigue and Muscle Performance

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
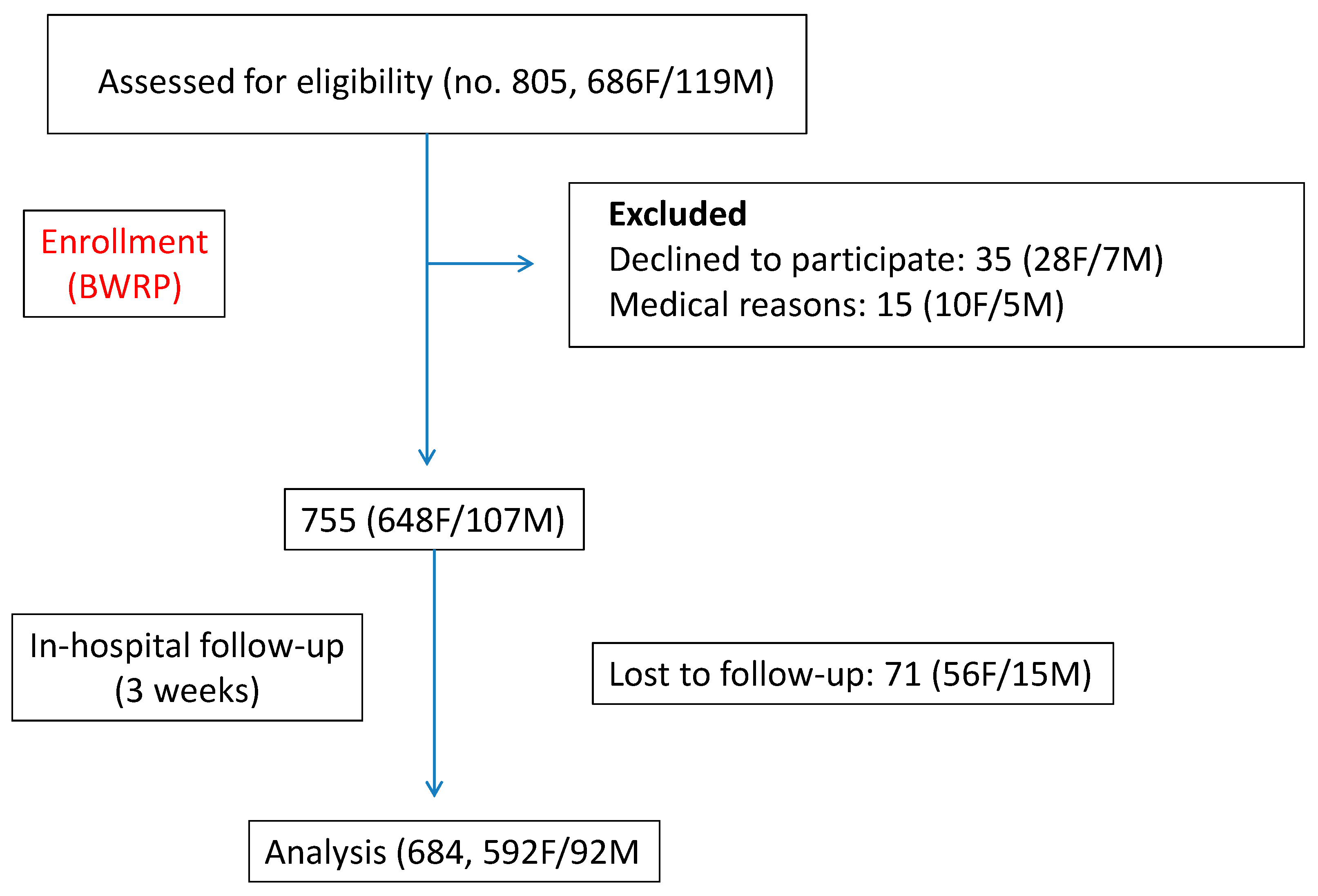
2.1. Patients and Body Weight Reduction Program
2.2. Stair Climbing Test
2.3. Fatigue Severity Scale
2.4. Evaluation of Coronary Heart Disease Risk
2.5. Hematochemical Testing
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
References
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in obesity among adults in theUnited States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Amarya, S.; Singh, K.; Sabharwal, M. Health consequences of obesity in the elderly. J. Clin. Gerontol. Geriatr. 2014, 5, 63–67. [Google Scholar] [CrossRef] [Green Version]
- Bales, C.W.; Porter Starr, K.N. Obesity interventions for older adults: Diet as a determinant of physical function. Adv. Nutr. 2018, 9, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J. Health benefits of weight reduction in postmenopausal women: A systematic review. J. Br. Menopause Soc. 2006, 12, 164–171. [Google Scholar] [CrossRef]
- Locher, J.L.; Goldsby, T.U.; Goss, A.M.; Kilgore, M.L.; Gower, B.; Ard, J.D. Calorie restriction in overweight older adults: Do benefits exceed potential risks? Exp. Gerontol. 2016, 86, 4–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzankoff, S.P.; Norris, A.H. Effect of muscle mass decrease on age-related BMR changes. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1977, 43, 1001–1006. [Google Scholar] [CrossRef]
- Elia, M.; Ritz, P.; Stubbs, R.J. Total energy expenditure in the elderly. Eur. J. Clin. Nutr. 2000, 54 (Suppl. 3), S92–S103. [Google Scholar] [CrossRef] [PubMed]
- Villareal, D.T.; Apovian, C.M.; Kushner, R.F.; Klein, S. Obesity in older adults: Technical review and position statement of the American Society for Nutrition and NAASO, The Obesity Society. Am. J. Clin. Nutr. 2005, 82, 923–934. [Google Scholar] [CrossRef]
- Ten Haaf, T.; Verreijen, A.M.; Memelink, R.G.; Tieland, M.; Weijs, P.J. Reduction in energy expenditure during weight loss is higher than predicted based on fat free mass and fat mass in older adults. Clin. Nutr. 2018, 37, 250–253. [Google Scholar] [CrossRef]
- Porter Starr, K.N.; McDonald, S.R.; Bales, C.W. Obesity and physical frailty in older adults: A scoping review of lifestyle intervention trials. J. Am. Med. Dir. Assoc. 2014, 15, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Costamagna, D.; Costelli, P.; Sampaolesi, M.; Penna, F. Role of inflammation in muscle homeostasis and myogenesis. Mediat. Inflamm. 2015, 2015, 805172. [Google Scholar] [CrossRef] [PubMed]
- Weinheimer, E.M.; Sands, L.P.; Campbell, W.W. A systematic review of the separate and combined effects of energy restriction and exercise on fat-free mass in middle-aged and older adults: Implications for sarcopenic obesity. Nutr. Rev. 2010, 68, 375–388. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Metter, E.J.; Ramachandran, R.; Chia, C.W.; Saudek, C.D. Glucose and insulin measurements from the oral glucose tolerance test and relationship to muscle mass. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Giunta, M.; Rigamonti, A.E.; Agosti, F.; Patrizi, A.; Compri, E.; Cardinale, M.; Sartorio, A. Combination of external load and whole body vibration potentiates the GH-releasing effect of squatting in healthy females. Horm. Metab. Res. 2013, 45, 611–666. [Google Scholar] [CrossRef] [PubMed]
- Sartorio, A.; Lafortuna, C.L.; Maffiuletti, N.A.; Agosti, F.; Marazzi, N.; Rastelli, F.; Rigamonti, A.E.; Muller, E.E. GH responses to two consecutive bouts of whole body vibration, maximal voluntary contractions or vibration alternated with maximal voluntary contractions administered at 2-h intervals in healthy adults. Growth Horm. IGF Res. 2010, 20, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Rigamonti, A.E.; Locatelli, L.; Cella, S.G.; Bonomo, S.M.; Giunta, M.; Molinari, F.; Sartorio, A.; Müller, E.E. Muscle expressions of MGF, IGF-IEa, and myostatin in intact and hypophysectomized rats: Effects of rhGH and testosterone alone or combined. Horm. Metab. Res. 2009, 41, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Soltani, S.; Hunter, G.R.; Kazemi, A.; Shab-Bidar, S. The effects of weight loss approaches on bone mineral density in adults: A systematic review and meta-analysis of randomized controlled trials. Osteoporos. Int. 2016, 27, 2655–2671. [Google Scholar] [CrossRef]
- Wang, S.; Ren, J. Obesity paradox in aging: From prevalence to pathophysiology. Prog. Cardiovasc. Dis. 2018, 61, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.J.; Morley, J.E.; Argiles, J.; Bales, C.; Baracos, V.; Guttridge, D.; Jatoi, A.; Kalantar-Zadeh, K.; Lochs, H.; Mantovani, G.; et al. Cachexia: A new definition. Clin. Nutr. 2008, 27, 793–799. [Google Scholar] [CrossRef]
- Sartorio, A.; Lafortuna, C.L.; Marinone, P.G.; Tavani, A.; La Vecchia, C.; Bosetti, C. Short-term effects of two integrated, non-pharmacological body weight reduction programs on coronary heart disease risk factors in young obese patients. Diab. Nutr. Metab. 2003, 16, 262–265. [Google Scholar]
- Sartorio, A.; Lafortuna, C.L.; Conte, G.; Faglia, G.; Narici, M.V. Changes in motor control and muscle performance after a short-term body mass reduction program in obese subjects. J. Endocrinol. Investig. 2001, 24, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Sartorio, A.; Narici, M.V.; Fumagalli, E.; Faglia, G.; Lafortuna, C.L. Aerobic and anaerobic performance before and after a short-term body mass reduction program in obese subjects. Diab. Nutr. Metab. 2001, 14, 51–57. [Google Scholar]
- Impellizzeri, F.M.; Agosti, F.; De Col, A.; Sartorio, A. Psychometric properties of the Fatigue Severity Scale in obese patients. Health Qual. Life Outcomes 2013, 11, 32. [Google Scholar] [CrossRef]
- Sartorio, A.; Proietti, M.; Marinone, P.G.; Agosti, F.; Adorni, F.; Lafortuna, C.L. Influence of gender, age and BMI on lower limb muscular power output in a large population of obese men and women. Int. J. Obes. 2004, 28, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Margaria, R.; Aghemo, P.; Rovelli, E. Measurement of muscular power (anaerobic) in man. J. Appl. Physiol. 1966, 21, 1662–1664. [Google Scholar] [CrossRef]
- Sartorio, A.; Fontana, P.; Trecate, L.; Lafortuna, C.L. Short-term changes of fatigue and muscle performance in severe obese patients after an integrated body mass reduction program. Diab. Nutr. Metab. 2003, 16, 88–93. [Google Scholar]
- Hjollund, N.H.; Andersen, J.H.; Bech, P. Assessment of fatigue in chronic disease: A bibliographic study of fatigue measurement scales. Health Qual. Life Outcomes 2007, 5, 12. [Google Scholar] [CrossRef]
- Elbers, R.G.; Rietberg, M.B.; van Wegen, E.E.; Verhoef, J.; Kramer, S.F.; Terwee, C.B.; Kwakkel, G. Self-report fatigue questionnaires in multiple sclerosis, Parkinson’s disease and stroke: A systematic review of measurement properties. Qual. Life Res. 2012, 21, 925–944. [Google Scholar] [CrossRef]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershats, H.; Kannel, W.B. Prediction of coronary hearth disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef]
- Rigamonti, A.E.; Piscitelli, F.; Aveta, T.; Agosti, F.; De Col, A.; Bini, S.; Cella, S.G.; Di Marzo, V.; Sartorio, A. Anticipatory and consummatory effects of (hedonic) chocolate intake are associated with increased circulating levels of the orexigenic peptide ghrelin and endocannabinoids in obese adults. Food Nutr. Res. 2015, 59, 29678. [Google Scholar] [CrossRef] [PubMed]
- Rigamonti, A.E.; Resnik, M.; Compri, E.; Agosti, F.; De Col, A.; Monteleone, P.; Marazzi, N.; Bonomo, S.M.; Müller, E.E.; Sartorio, A. The cholestyramine-induced decrease of PYY postprandial response is negatively correlated with fat mass in obese women. Horm. Metab. Res. 2011, 43, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L. Obesity and functional decline: Epidemiology and geriatric consequences. Clin. Geriatr. Med. 2005, 21, 677–687. [Google Scholar] [CrossRef]
- Moreh, E.; Jacobs, J.M.; Stessman, J. Fatigue, function, and mortality in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Fritschi, C.; Quinn, L. Fatigue in patients with diabetes: A review. J. Psychosom. Res. 2010, 69, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Teel, C.; Sabus, C.; McGinnis, P.; Kluding, P. Fatigue in Type 2 Diabetes: Impact on Quality of Life and Predictors. PLoS ONE 2016, 11, e0165652. [Google Scholar] [CrossRef]
- Ten Hoor, G.A.; Kok, G.; Peters, G.Y.; Frissen, T.; Schols, A.M.; Plasqui, G. The psychological effects of strength exercises in people who are overweight or obese: A systematic review. Sports Med. 2017, 47, 2069–2081. [Google Scholar] [CrossRef]
- Lin, T.W.; Kuo, Y.M. Exercise benefits brain function: The monoamine connection. Brain Sci. 2013, 3, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Lee, P.H.; Hsiao, D.J.; Huang, S.W.; Tsauo, J.Y.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with exercise intervention on frailty indices, body composition, and physical function in frail older adults. Nutrients 2018, 10, 1916. [Google Scholar] [CrossRef] [PubMed]
- Cottell, K.E.; Dorfman, L.R.; Straight, C.R.; Delmonico, M.J.; Lofgren, I.E. The effects of diet education plus light resistance training on coronary heart disease risk factors in community-dwelling older adults. J. Nutr. Health Aging 2011, 15, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Butryn, M.L.; Byrne, K.J. Efficacy of lifestyle modification for long-term weight control. Obes. Res. 2004, 12 (Suppl. 12), 151S–162S. [Google Scholar] [CrossRef]
- Braun, N.; Gomes, F.; Schütz, P. “The obesity paradox” in disease—Is the protective effect of obesity true? Swiss Med. Wkly. 2015, 145, w14265. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.L. Cardiovascular risk factors: Does sex matter? Curr. Vasc. Pharmacol. 2016, 14, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Kallen, A.N.; Pal, L. Cardiovascular disease and ovarian function. Curr. Opin. Obstet. Gynecol. 2011, 23, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Barford, A.; Dorling, D.; Davey Smith, G.; Shaw, M. Life expectancy: Women now on top everywhere. BMJ 2006, 332, 808. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | >60 Year | 60–69 Year | >70 Year | >60 Year | 60–69 Year | >70 Year | >60 Year | 60–69 Year | >70 Year |
| No. | 684 | 500 | 184 | 92 | 69 | 23 | 592 | 432 | 160 |
| Age (year) | 67.7 ± 4.7 | 64.7 ± 2.6 | 73.4 ± 3.1 | 67.0 ± 4.8 | 64.7 ± 2.5 | 74.1 ± 2.6 | 67.1 ± 4.7 | 64.7 ± 2.6 | 73.4 ± 3.1 |
| WHR | 1.0 ± 0.1 | 0.9 ± 0.1 | 1.0 ± 0.1 | 1.0 ± 0.1 a | 1.0 ± 0.1 a | 1.0 ± 0.1 a | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.1 |
| Height (m) | 1.6 ± 0.1 | 1.6 ± 0.1 | 1.6 ± 0.1 | 1.7 ± 0.1 a | 1.7 ± 0.1 a | 1.6 ± 0.1 a | 1.5 ± 0.1 | 1.5 ± 0.1 | 1.5 ± 0.1 |
| PRE-BW (kg) | 104.3 ± 15.7 | 106.0 ± 16.4 | 99.6 ± 12.3 | 114.8 ± 16.8 a | 118.1 ± 16.7 a | 104.9 ± 12.6 a,b | 102.6 ± 14.9 | 104.0 ± 15.5 | 98.8 ± 12.1 b |
| POST-BW (kg) | 100.3 ± 15.2 c | 101.8 ± 15.9 c | 96.4 ± 12.2 c | 110.1 ± 16.3 c | 113.3 ± 16.3 c | 98.8 ± 14.4 c | 98.8 ± 14.4 c | 99.9 ± 15.0 c | 95.7 ± 12.0 c |
| ΔBW (%) | 4.7 ± 9.2 | 4.8 ± 8.7 | 4.4 ± 10.3 | 5.3 ± 10.1 | 5.7 ± 11.6 | 4.0 ± 1.5 | 4.6 ± 9.0 | 4.6 ± 8.1 | 4.4 ± 11.1 |
| PRE-BMI (kg/m2) | 42.6 ± 5.6 | 43.0 ± 5.9 | 41.4 ± 4.8 d | 40.6 ± 4.8 e | 41.1 ± 4.6 e | 38.9 ± 5.0 e | 42.9 ± 5.7 | 43.3 ± 6.0 | 41.8 ± 4.7 f |
| POST-BMI (kg/m2) | 41.0 ± 5.5 c | 41.3 ± 5.7 c | 40.0 ± 4.8 c | 38.9 ± 4.7 c | 39.4 ± 4.6 c | 37.4 ± 4.8 c | 41.3 ± 5.6 c | 41.6 ± 5.8 c | 40.5 ± 4.7 c |
| ΔBMI (%) | 4.0 ± 2.1 | 4.2 ± 1.8 | 3.5 ± 2.8 | 4.2 ± 1.7 | 4.3 ± 1.7 | 4.0 ± 1.6 | 3.9 ± 2.2 | 4.1 ± 1.8 | 3.4 ± 3.0 |
| Total | Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | >60 Year | 60–69 Year | >70 Year | >60 Year | 60–69 Year | >70 Year | >60 Year | 60–69 Year | >70 Year |
| PRE-GLU (mg/dL) | 107.3 ± 33.9 | 108.3 ± 35.4 | 104.5 ± 29.0 | 105.4 ± 28.0 | 108.4 ± 30.3 | 96.1 ± 16.7 | 107.6 ± 34.7 | 108.2 ± 36.2 | 105.8 ± 30.3 |
| POST-GLU (mg/dL) | 88.0 ± 14.4 a | 87.8 ± 14.9 a | 88.5 ± 12.8 a | 86.1 ± 12.8 a | 86.2 ± 13.0 a | 85.8 ± 12.6 a | 88.5 ± 14.8 a | 88.2 ± 15.4 a | 89.3 ± 13.0 a |
| ΔGLU (%) | 10.6 ± 14.5 | 10.9 ± 14.7 | 9.6 ± 13.9 | 11.7 ± 13.8 | 11.2 ± 15.6 | 12.9 ± 8.0 | 10.2 ± 14.8 | 10.8 ± 14.5 | 8.5 ± 15.6 |
| PRE-T-C (mg/dL) | 199.0 ± 38.8 | 199.2 ± 39.8 | 198.4 ± 36.1 | 193.7 ± 36.1 | 193.6 ± 36.0 | 194.0 ± 37.3 | 199.8 ± 39.2 | 200.1 ± 40.3 | 199.0 ± 36.1 |
| POST-T-C (mg/dL) | 169.7 ± 35.9 a | 170.0 ± 36.2 a | 168.8 ± 34.8 a | 155.9 ± 36.8 a | 156.4 ± 39.4 a | 154.6 ± 28.0 a | 171.8 ± 35.3 a | 172.2 ± 35.3 a | 170.6 ± 35.3 a |
| ΔT-C (%) | 13.7 ± 14.3 | 13.5 ± 14.0 | 14.3 ± 15.1 | 17.9 ± 16.7 | 17.8 ± 17.9 | 18.2 ± 12.6 | 13.1 ± 13.8 | 12.8 ± 13.2 | 13.8 ± 15.4 |
| PRE-HDL-C (mg/dL) | 50.9 ± 13.5 | 50.5 ± 13.9 | 51.7 ± 12.1 b | 40.9 ± 9.2 c | 40.0 ± 9.0 c | 43.8 ± 9.6 c | 52.4 ± 13.4 | 52.2 ± 13.9 | 52.9 ± 12.1 |
| POST-HDL-C (mg/dL) | 42.7 ± 10.3 a | 42.6 ± 10.6 a | 43.0 ± 9.3 a | 35.6 ± 7.9 a | 34.8 ± 7.8 a | 38.1 ± 7.8 a | 43.8 ± 10.2 a | 43.8 ± 10.5 a | 43.8 ± 9.3 a |
| ΔHDL-C (%) | 14.8 ± 13.7 | 14.3 ± 13.2 | 16.0 ± 15.0 | 11.0 ± 13.3 | 10.9 ± 13.8 | 11.1 ± 11.8 | 15.4 ± 13.7 | 14.9 ± 13.0 | 16.7 ± 15.3 |
| PRE-DBP (mmHg) | 77.6 ± 8.2 | 77.8 ± 7.9 | 76.9 ± 8.8 | 76.8 ± 9.5 | 78.0 ± 9.0 | 73.3 ± 10.5 | 77.7 ± 7.9 | 77.8 ± 7.7 | 77.4 ± 8.4 |
| POST-DBP (mmHg) | 74.6 ± 6.7 a | 74.6 ± 7.0 a | 74.4 ± 5.9 a | 74.7 ± 7.5 a | 74.9 ± 7.9 a | 74.3 ± 6.2 | 74.5 ± 6.6 a | 74.5 ± 6.8 a | 74.5 ± 5.9 a |
| ΔDBP (%) | 3.2 ± 11.7 | 3.5 ± 10.8 | 2.6 ± 13.8 | 2.7 ± 16.8 | 3.3 ± 10.7 | 1.0 ± 28.7 | 3.3 ± 10.7 | 3.5 ± 10.8 | 2.9 ± 10.5 |
| PRE-SBP (mmHg) | 132.6 ± 14.6 | 132.3 ± 14.4 | 133.4 ± 15.4 | 131.5 ± 14.5 | 32.4 ± 14.0 | 128.6 ± 16.0 | 132.8 ± 14.7 | 132.2 ± 14.5 | 134.2 ± 15.1 |
| POST-SBP (mmHg) | 123.8 ± 10.2 a | 123.7 ± 10.3 a | 124.0 ± 9.9 a | 123.9 ± 11.1 a | 124.0 ± 11.4 a | 123.6 ± 10.4 a | 123.8 ± 10.0 a | 123.7 ± 10.1 a | 124.1 ± 9.9 a |
| ΔSBP (%) | 5.9 ± 9.9 | 5.7 ± 10.2 | 6.4 ± 9.1 | 5.0 ± 9.7 | 5.4 ± 10.0 | 3.7 ± 8.6 | 6.0 ± 9.9 | 5.7 ± 10.2 | 6.0 ± 9.1 |
| Total | Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcome | >60 Year | 60–69 Year | >70 Year | >60 Year | 60–69 Year | >70 Year | >60 Year | 60–69 Year | >70 Year |
| PRE-CHD-R (points) | 10.2 ± 3.5 | 10.2 ± 3.4 | 10.1 ± 3.6 a | 8.6 ± 2.9 b | 8.4 ± 3.1 b | 9.0 ± 2.3 | 10.4 ± 3.5 | 10.5 ± 3.4 | 10.3 ± 3.8 c |
| POST-CHD-R (points) | 9.9 ± 3.5 d | 9.9 ± 3.5 d | 9.7 ± 3.5 d | 7.3 ± 2.5 d | 7.1 ± 2.7 d | 7.9 ± 1.5 d | 10.3 ± 3.5 | 10.4 ± 3.5 | 10.0 ± 3.6 |
| ΔCHD-R (points) | 0.4 ± 2.7 | 0.4 ± 2.7 | 0.6 ± 2.6 | 1.4 ± 2.9 b | 1.4 ± 2.9 b | 1.3 ± 2.7 c | 0.3 ± 2.7 | 0.2 ± 2.7 | 0.5 ± 2.6 |
| PRE-FSS score (points) | 40.9 ± 13.5 | 40.1 ± 13.7 | 43.3 ± 12.4 | 36.2 ± 13.1 b | 35.2 ± 13.2 b | 39.7 ± 12.6 | 41.7 ± 13.4 | 40.8 ± 13.7 | 43.9 ± 12.3 |
| POST-FSS score (points) | 34.1 ± 13.1 d | 33.3 ± 13.2 d | 36.2 ± 12.4 d | 30.1 ± 11.2 d | 29.9 ± 11.5 d | 31.1 ± 10.3 d | 34.7 ± 13.2 d | 33.8 ± 13.4 d | 36.9 ± 12.5 d |
| ΔFSS score (%) | 16.4 ± 18.5 | 16.6 ± 18.3 | 15.8 ± 18.9 | 15.0 ± 17.4 | 13.8 ± 16.0 | 19.3 ± 21.9 | 16.6 ± 18.6 | 17.1 ± 18.6 | 15.4 ± 18.7 |
| PRE-SCT time (sec) | 7.7 ± 1.9 | 7.6 ± 1.8 | 8.2 ± 2.2 | 6.8 ± 1.5 b | 6.6 ± 1.3 b | 7.4 ± 2.0 | 7.9 ± 2.0 | 7.8 ± 1.9 | 8.4 ± 2.2 |
| POST-SCT time (sec) | 7.4 ± 1.9 d | 7.2 ± 1.8 d | 7.9 ± 2.1 d | 6.5 ± 1.5 d | 6.3 ± 1.3 d | 7.2 ± 2.0 d | 7.5 ± 1.9 d | 7.4 ± 1.8 d | 8.0 ± 2.1 d |
| ΔSCT time (%) | 4.3 ± 4.7 | 4.5 ± 4.9 | 4.0 ± 4.2 | 3.7 ± 3.3 | 3.8 ± 3.5 | 3.3 ± 2.9 | 4.5 ± 4.9 | 4.6 ± 5.1 | 4.1 ± 4.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigamonti, A.E.; De Col, A.; Tamini, S.; Cicolini, S.; Caroli, D.; De Micheli, R.; Tringali, G.; Abbruzzese, L.; Marazzi, N.; Cella, S.G.; et al. Multidisciplinary Integrated Metabolic Rehabilitation in Elderly Obese Patients: Effects on Cardiovascular Risk Factors, Fatigue and Muscle Performance. Nutrients 2019, 11, 1240. https://doi.org/10.3390/nu11061240
Rigamonti AE, De Col A, Tamini S, Cicolini S, Caroli D, De Micheli R, Tringali G, Abbruzzese L, Marazzi N, Cella SG, et al. Multidisciplinary Integrated Metabolic Rehabilitation in Elderly Obese Patients: Effects on Cardiovascular Risk Factors, Fatigue and Muscle Performance. Nutrients. 2019; 11(6):1240. https://doi.org/10.3390/nu11061240
Chicago/Turabian StyleRigamonti, Antonello E., Alessandra De Col, Sofia Tamini, Sabrina Cicolini, Diana Caroli, Roberta De Micheli, Gabriella Tringali, Laura Abbruzzese, Nicoletta Marazzi, Silvano G. Cella, and et al. 2019. "Multidisciplinary Integrated Metabolic Rehabilitation in Elderly Obese Patients: Effects on Cardiovascular Risk Factors, Fatigue and Muscle Performance" Nutrients 11, no. 6: 1240. https://doi.org/10.3390/nu11061240
APA StyleRigamonti, A. E., De Col, A., Tamini, S., Cicolini, S., Caroli, D., De Micheli, R., Tringali, G., Abbruzzese, L., Marazzi, N., Cella, S. G., & Sartorio, A. (2019). Multidisciplinary Integrated Metabolic Rehabilitation in Elderly Obese Patients: Effects on Cardiovascular Risk Factors, Fatigue and Muscle Performance. Nutrients, 11(6), 1240. https://doi.org/10.3390/nu11061240