Vitamin D Supplementation and Post-Stroke Rehabilitation: A Randomized, Double-Blind, Placebo-Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population, Eligibility, and Consent
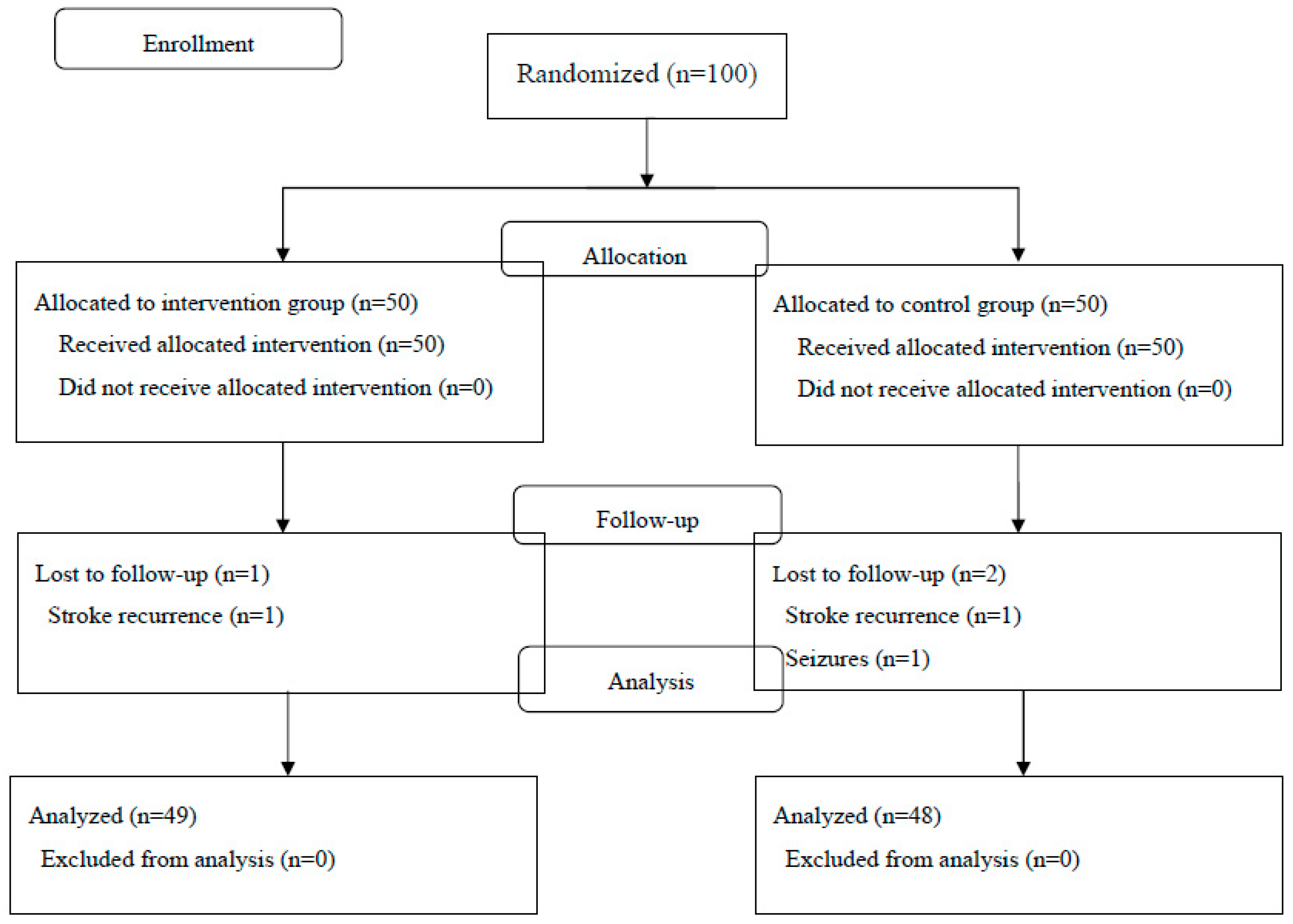
2.3. Randomization, Blinding, and Intervention
2.4. Follow-Up Procedures
2.5. Assessment of Outcomes
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [PubMed]
- Strong, K.; Mathers, C.; Bonita, R. Preventing stroke: Saving lives around the world. Lancet Neurol. 2007, 6, 182–187. [Google Scholar] [CrossRef]
- McArthur, K.S.; Quinn, T.J.; Higgins, P.; Langhorne, P. Postacute care and secondary prevention after ischaemic stroke. BMJ 2011, 3429, d2083. [Google Scholar] [CrossRef] [PubMed]
- Neo, J.J.; Kong, K.H. Prevalence of Vitamin D Deficiency in Elderly Patients Admitted to an Inpatient Rehabilitation Unit in Tropical Singapore. Rehabil. Res. Pract. 2016, 2016, 9689760. [Google Scholar] [CrossRef] [PubMed]
- Schilling, S. Epidemic vitamin D deficiency among patients in an elderly care rehabilitation facility. Dtsch. Arztebl. Int. 2012, 109, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Zhou, H.; Wang, S.; Cheng, L.; Fang, Y. Low Serum Levels of 25-Hydroxyvitamin D Are Associated with Stroke Recurrence and Poor Functional Outcomes in Patients with Ischemic Stroke. J. Nutr. Health Aging 2017, 21, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Zhong, C.; Peng, Y.; Chen, C.S.; Wang, J.; Ju, Z.; Li, Q.; Geng, D.; Sun, Y.; Zhang, D.; et al. Serum 25-hydroxyvitamin D deficiency predicts poor outcome amongst acute ischaemic stroke patients with low high density lipoprotein cholesterol. Eur. J. Neurol. 2016, 23, 1763–1768. [Google Scholar] [CrossRef]
- Alfieri, D.F.; Lehmann, M.F.; Oliveira, S.R.; Flauzino, T.; Delongui, F.; de Araújo, M.C.; Dichi, I.; Delfino, V.D.; Mezzaroba, L.; Simão, A.N.; et al. Vitamin D deficiency is associated with acute ischemic stroke, C-reactive protein, and short-term outcome. Metab. Brain Dis. 2017, 32, 493–502. [Google Scholar] [CrossRef]
- Park, K.Y.; Chung, P.W.; Kim, Y.B.; Moon, H.-S.; Suh, B.-C.; Won, Y.S.; Kim, O.-S.; Youn, Y.C.; Kwon, O.-S. Serum vitamin D status as a predictor of prognosis in patients with acute ischemic stroke. Cerebrovasc. Dis. 2015, 40, 73–80. [Google Scholar] [CrossRef]
- Tu, W.J.; Zhao, S.J.; Xu, D.J.; Chen, H. Serum 25-hydroxyvitamin D predicts the short-term outcomes of Chinese patients with acute ischaemic stroke. Clin. Sci. 2014, 126, 339–346. [Google Scholar] [CrossRef]
- Daubail, B.; Jacquin, A.; Guilland, J.C.; Hervieu, M.; Osseby, G.V.; Rouaud, O.; Giroud, M.; Béjot, Y. Serum 25-hydroxyvitamin D predicts severity and prognosis in stroke patients. Eur. J. Neurol. 2013, 20, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Yalbuzdag, S.A.; Sarifakioglu, B.; Afsar, S.I.; Celik, C.; Can, A.; Yegin, T.; Senturk, B.; Guzelant, A.Y. Is 25(OH)D associated with cognitive impairment and functional improvement in stroke? A retrospective clinical study. J. Stroke Cerebrovasc. Dis. 2015, 24, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ji, H.; Tong, Y.; Zhang, Z.B. Prognostic value of serum 25-hydroxyvitamin D in patients with stroke. Neurochem. Res. 2014, 39, 1332–1337. [Google Scholar] [CrossRef] [PubMed]
- Makariou, S.E.; Michel, P.; Tzoufi, M.S.; Challa, A.; Milionis, H.J. Vitamin D and stroke: Promise for prevention and better outcome. Curr. Vasc. Pharmacol. 2014, 12, 117–124. [Google Scholar] [CrossRef]
- Kalueff, A.V.; Tuohimaa, P. Neurosteroid hormone vitamin D and its utility in clinical nutrition. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Burgos, R.; Bretón, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jésus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. 2018, 37, 354–396. [Google Scholar] [CrossRef] [Green Version]
- Antoniak, A.E.; Greig, C.A. The effect of combined resistance exercise training and vitamin D(3) supplementation on musculoskeletal health and function in older adults: A systematic review and meta-analysis. BMJ Open 2017, 7, e014619. [Google Scholar] [CrossRef]
- Bunout, D.; Barrera, G.; Leiva, L.; Gattas, V.; de la Maza, M.P.; Avendaño, M.; Hirsch, S. Effects of vitamin D supplementation and exercise training on physical performance in Chilean vitamin D deficient elderly subjects. Exp. Gerontol. 2006, 41, 746–752. [Google Scholar] [CrossRef]
- Hornikx, M.; Van, R.H.; Lehouck, A.; Mathieu, C.; Maes, K.; Gayan-Ramirez, G.; Decramer, M.; Troosters, T.; Janssens, W. Vitamin D supplementation during rehabilitation in COPD: A secondary analysis of a randomized trial. Respir. Res. 2012, 13, 84. [Google Scholar] [CrossRef]
- Narasimhan, S.; Balasubramanian, P. Role of vitamin D in the outcome of ischemic stroke—A randomized controlled trial. J. Clin. Diagn. Res. 2017, 11, CC06–CC10. [Google Scholar] [CrossRef]
- Gupta, A.; Prabhakar, S.; Modi, M.; Bhadada, S.K.; Kalaivani, M.; Lal, V.; Khurana, D. Effect of Vitamin D and calcium supplementation on ischaemic stroke outcome: A randomised controlled open-label trial. Int. J. Clin. Pract. 2016, 70, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Sai, A.; Templin, T.; Smith, L. Dose response to vitamin D supplementation in postmenopausal women: A randomized trial. Ann. Intern. Med. 2012, 156, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Mahone, F.; Barthel, D. Functional evaluation: The Barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Brunnstrom, S. Motor testing procedures in hemiplegia: Based on sequential recovery stages. Phys. Ther. 1966, 46, 357–375. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Test-Retest Reliability of Measurements of Hand-Grip Strength Obtained by Dynamometry from Older Adults: A Systematic Review of Research in the PubMed Database. J. Frailty Aging 2017, 6, 83–87. [Google Scholar] [PubMed]
- Tresignie, J.; Scafoglieri, A.; Pieter, C.J.; Cattrysse, E. Reliability of standard circumferences in domain-related constitutional applications. Am. J. Hum. Biol. 2013, 25, 637–642. [Google Scholar] [PubMed]
- Koh, G.C.; Chen, C.H.; Petrella, R.; Thind, A. Rehabilitation impact indices and their independent predictors: A systematic review. BMJ Open 2013, 3, e003483. [Google Scholar] [CrossRef]
- Hsieh, Y.W.; Wang, C.H.; Wu, S.C.; Chen, P.C.; Sheu, C.F.; Hsieh, C.L. Establishing the minimal clinically important difference of the Barthel Index in stroke patients. Neurorehabil. Neural Repair 2007, 21, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Tellioglu, A.; Basaran, S.; Guzel, R.; Seydaoglu, G. Efficacy and safety of high dose intramuscular or oral cholecalciferol in vitamin D deficient/insufficient elderly. Maturitas 2012, 72, 332–338. [Google Scholar] [CrossRef]
- Smith, H.; Anderson, F.; Raphae, H.; Maslin, P.; Crozier, S.; Cooper, C. Effect of annual intramuscular vitamin D on fracture risk in elderly men and women—A population-based, randomized, double-blind, placebo-controlled trial. Rheumatology 2007, 46, 1852–1857. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA 2010, 303, 1815–1822. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.H.; Corbett, D. Plasticity during stroke recovery: From synapse to behaviour. Nat. Rev. Neurosci. 2009, 10, 861–872. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Vitamin D3 (n = 49) | Placebo (n = 48) | |
|---|---|---|
| Age, years (SD) | 67.6 (11.7) | 65.5 (11.7) |
| Male sex, n (%) | 34 (69.4) | 34 (70.8) |
| Type of stroke, n (%) | ||
| Cerebral infarction | 29 (58.3) | 28 (59.2) |
| Cerebral hemorrhage | 17 (35.4) | 17 (34.7) |
| Subarachnoid hemorrhage | 3 (6.3) | 3 (6.3) |
| Common comorbidities, n (%) | ||
| Hypertension | 20 (40.8) | 17 (35.4) |
| Dyslipidemia | 10 (20.4) | 3 (6.3) |
| Diabetes mellitus | 7 (14.3) | 4 (8.3) |
| Atrial fibrillation | 2 (4.1) | 2 (4.2) |
| Paretic side, n (%) | ||
| Right | 25 (51.0) | 27 (56.3) |
| Left | 24 (49.0) | 21 (43.8) |
| Days since stroke, mean (SD) | 34.2 (16.6) | 33.6 (15.6) |
| Barthel Index, mean (SD) | 50.7 (25.9) | 53.8 (23.0) |
| Brunnstrom stage, median (IQR) | ||
| Arm | 4 (2–5) | 4 (2–5) |
| Hand | 4 (2–5) | 4 (2–5) |
| Leg | 3 (2–5) | 3 (2–5) |
| Hand grip strength, kg, mean (SD) | ||
| Right | 16.2 (12.9) | 17.1 (13.0) |
| Left | 13.8 (14.3) | 15.8 (12.1) |
| Calf circumference, cm, mean (SD) | ||
| Right | 32.0 (2.9) | 32.3 (3.8) |
| Left | 31.8 (2.8) | 32.1 (4.0) |
| Vitamin D3 (n = 49) | Placebo (n = 48) | p-Value | |
|---|---|---|---|
| Barthel Index gain, mean (SD) | 19.0 (14.8) | 19.5 (13.1) | 0.48 |
| Patient age, years | |||
| ≥65 | 16.7 (11.8) | 20.2 (12.2) | 0.26 |
| <65 | 24.3 (19.5) | 18.8 (14.2) | 0.41 |
| Type of stroke | |||
| Ischemic | 21.2 (15.7) | 17.7 (12.1) | 0.75 |
| Non-ischemic | 15.9 (13.1) | 22.0 (14.3) | 0.83 |
| Vitamin D3 (n = 49) | Placebo (n = 48) | p-Value | |
|---|---|---|---|
| Barthel Index efficiency, mean (SD) | 0.32 (0.31) | 0.27 (0.21) | 0.46 |
| Brunnstrom stage improved, n (%) | |||
| Arm | 21 (42.9) | 18 (37.5) | 0.59 |
| Hand | 17 (34.7) | 18 (37.5) | 0.77 |
| Leg | 20 (40.8) | 18 (37.5) | 0.74 |
| Hand grip strength | |||
| Right | |||
| Change, kg, mean (SD) | 1.4 (3.4) | 1.1 (2.8) | 0.87 |
| Improved, n (%) | 27 (55.1) | 25 (52.1) | 0.77 |
| Left | |||
| Change, kg, mean (SD) | 1.2 (3.3) | 0.5 (4.1) | 0.36 |
| Improved, n (%) | 20 (40.8) | 18 (37.5) | 0.74 |
| Calf circumference | |||
| Right | |||
| Change, cm, mean (SD) | −0.1 (1.8) | −0.3 (1.6) | 0.99 |
| Improved, n (%) | 19 (38.8) | 20 (41.7) | 0.77 |
| Left | |||
| Change, cm, mean (SD) | 0.4 (1.6) | −0.2 (2.0) | 0.51 |
| Improved, n (%) | 23 (46.9) | 20 (41.7) | 0.60 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Momosaki, R.; Abo, M.; Urashima, M. Vitamin D Supplementation and Post-Stroke Rehabilitation: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2019, 11, 1295. https://doi.org/10.3390/nu11061295
Momosaki R, Abo M, Urashima M. Vitamin D Supplementation and Post-Stroke Rehabilitation: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2019; 11(6):1295. https://doi.org/10.3390/nu11061295
Chicago/Turabian StyleMomosaki, Ryo, Masahiro Abo, and Mitsuyoshi Urashima. 2019. "Vitamin D Supplementation and Post-Stroke Rehabilitation: A Randomized, Double-Blind, Placebo-Controlled Trial" Nutrients 11, no. 6: 1295. https://doi.org/10.3390/nu11061295
APA StyleMomosaki, R., Abo, M., & Urashima, M. (2019). Vitamin D Supplementation and Post-Stroke Rehabilitation: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients, 11(6), 1295. https://doi.org/10.3390/nu11061295