Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet




Abstract
:1. Introduction: Mediterranean Diet, When Evidence Speaks
2. Obesity as a Global Disease
3. The Choice: Mediterranean Diet Versus Western Diets
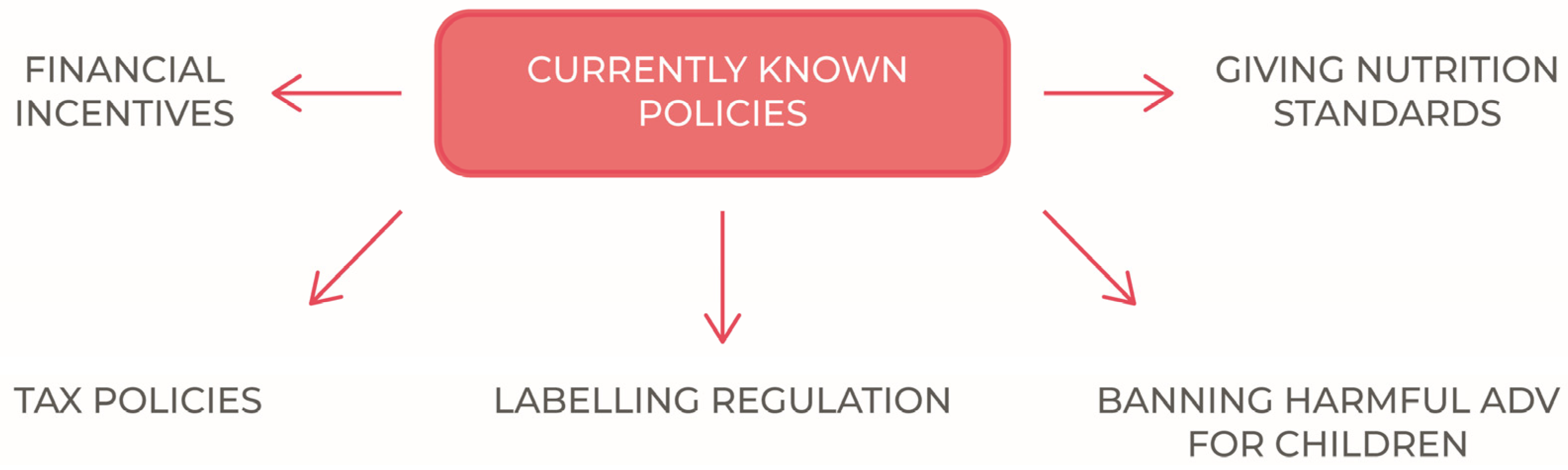
4. Public Policy Measures to Tackle the Phaenomenon
5. The Three Pillars and the Public Health Choices
6. Facts and Patterns of the Onset of the Epidemic: the Relevance of Environmental Factors
7. Fiscal Strategies for A Healthier Lifestyle: Do They Work?
8. The Role of the Food and Drink Industry
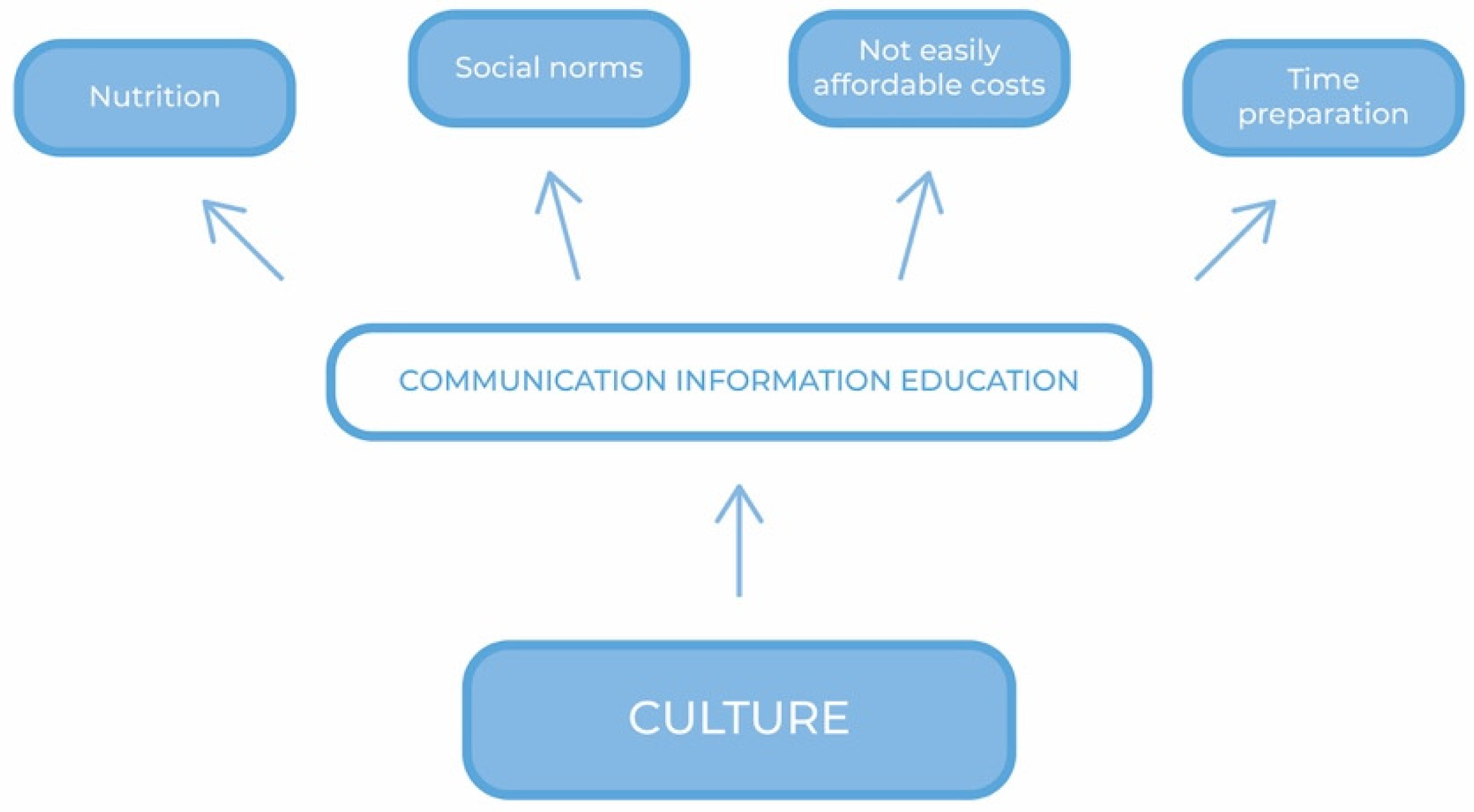
9. The Nature of the Obstacles to the Adoption of the MD: Addressing Research
10. Individual Choices and Actions to be Implemented
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Romagnolo, D.F.; Selmin, O.I. Mediterranean Diet and Prevention of Chronic Diseases. Nutr. Today 2017, 52, 208–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Foundation Expert Group. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases. Exp. Biol. Med. 2008, 233, 674–688. [Google Scholar] [CrossRef]
- Marventano, S.; Kolacz, P.; Castellano, S.; Galvano, F.; Buscemi, S.; Mistretta, A.; Grosso, G. A review of recent evidence in human studies of n-3 and n-6 PUFA intake on cardiovascular diseases, cancer, and depressive disorders: Does the ratio really matter? Int. J. Food Sci. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Hartley, L.; Clarke, A.; Thorogood, M.; Stranges, S. Mediterranean’ dietary pattern for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2012, 2012. [Google Scholar] [CrossRef]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Dontas, A.S.; Zerefos, N.S.; Panagiotakos, D.B.; Valis, D.A. Mediterranean diet and prevention of coronary heart disease in the elderly. Clin. Interv. Aging 2007, 2, 109–115. [Google Scholar] [CrossRef]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.; Stronati, M.; Lanari, M. Mediterranean diet, folic acid, and neural tube defects. Ital. J. Pediatr. 2017, 43, 74. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, T.B.; Osterdal, M.L.; Knudsen, V.K.; Haugen, M.; Meltzer, H.M.; Bakketeig, L.; Olsen, S.F. Association between a Mediterranean-type diet and risk of preterm birth among Danish women: A prospective cohort study. Acta Obs. Gynecol. Scand. 2008, 87, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.K.; Draper, E.S.; Evans, T.A.; Field, D.J.; Johnson, S.J.; Manktelow, B.N.; Seaton, S.E.; Marlow, N.; Petrou, S.; Boyle, E.M. Associations between late and moderately preterm birth and smoking, alcohol, drug use and diet: A population-based case-cohort study. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F486–F491. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Galiano, J.M.; Olmedo-Requena, R.; Barrios-Rodríguez, R.; Amezcua-Prieto, C.; Bueno-Cavanillas, A.; Salcedo-Bellido, I.; Jimenez-Moleon, J.J.; Delgado-Rodríguez, M. Effect of Adherence to a Mediterranean Diet and Olive Oil Intake during Pregnancy on Risk of Small for Gestational Age Infants. Nutrients 2018, 10, 1234. [Google Scholar] [CrossRef]
- Fernandez-Barres, S.; Romaguera, D.; Valvi, D.; Martinez, D.; Vioque, J.; Navarrete-Munoz, E.M.; Amiano, P.; Gonzalez-Palacios, S.; Guxens, M.; Pereda, E.; et al. Mediterranean dietary pattern in pregnant women and offspring risk of overweight and abdominal obesity in early childhood: The INMA birth cohort study. Pediatr. Obes. 2016, 11, 491–499. [Google Scholar] [CrossRef]
- Chatzi, L.; Rifas-Shiman, S.L.; Georgiou, V.; Joung, K.E.; Koinaki, S.; Chalkiadaki, G.; Margioris, A.; Sarri, K.; Vassilaki, M.; Vafeiadi, M.; et al. Adherence to the Mediterranean diet during pregnancy and offspring adiposity and cardiometabolic traits in childhood. Pediatr. Obes. 2017, 12 (Suppl. 1), 47–56. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Nahm, S.; Mendez, M.; Robinson, W.; Murphy, S.K.; Hoyo, C.; Hogan, V.; Rowley, D. Low maternal adherence to a Mediterranean diet is associated with increase in methylation at the MEG3-IG differentially methylated region in female infants. Environ. Epigenetics 2017, 3, dvx007. [Google Scholar] [CrossRef]
- D’Alessandro, A.; De Pergola, G. The Mediterranean Diet: Its definition and evaluation of a priori dietary indexes in primary cardiovascular prevention. Int. J. Food Sci. Nutr. 2018. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a literature review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Altomare, R.; Cacciabaudo, F.; Damiano, G.; Palumbo, V.D.; Gioviale, M.C.; Bellavia, M.; Tomasello, G.; Monte, A.I. The Mediterranean Diet: A History of Health. Iran. J. Public Health 2013, 42, 449–457. [Google Scholar] [PubMed]
- Mocciaro, G.; Ziauddeen, N.; Godos, J.; Marranzano, M.; Chan, M.Y.; Ray, S. Does a Mediterranean-type dietary pattern exert a cardio-protective effect outside the Mediterranean region? A review of current evidence. Int. J. Food Sci. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.; Hershey, M.; Zazpe, I.; Trichopoulou, A. Transferability of the Mediterranean Diet to Non-Mediterranean Countries. What Is and What Is Not the Mediterranean Diet. Nutrients 2017, 9, 1226. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Norat, T.; Vergnaud, A.C.; Mouw, T.; May, A.M.; Agudo, A.; Buckland, G.; Slimani, N.; Rinaldi, S.; Couto, E.; et al. Mediterranean dietary patterns and prospective weight change in participants of the EPIC-PANACEA project. Am. J. Clin. Nutr. 2010, 92, 912–921. [Google Scholar] [CrossRef]
- Bonaccio, M.; Iacoviello, L.; De Gaetano, G. The Mediterranean diet: The reasons for a success. Thromb. Res. 2012, 129, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Tognon, G.; Hebestreit, A.; Lanfer, A.; Moreno, L.A.; Pala, V.; Siani, A.; Tornaritis, M.; De Henauw, S.; Veidebaum, T.; Molnar, D.; et al. Mediterranean diet, overweight and body composition in children from eight European countries: Cross-sectional and prospective results from the IDEFICS study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 205–213. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Available online: www.thelancet.com (accessed on 10 May 2019).
- Braet, C.; Mervielde, I.; Vandereycken, W. Psychological aspects of childhood obesity: A controlled study in a clinical and nonclinical sample. J. Pediatr. Psychol. 1997, 22, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-related consequences of childhood obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Hartlev, M. Stigmatisation as a public health tool against obesity—A health and human rights perspective. Eur. J. Health Law 2014, 21, 365–386. [Google Scholar] [CrossRef] [PubMed]
- Karnik, S.; Kanekar, A. Childhood obesity: A global public health crisis. Int. J. Prev. Med. 2012, 3, 1–7. [Google Scholar] [PubMed]
- Tsakiraki, M.; Grammatikopoulou, M.G. Nutrition transition and health status of Cretan women: Evidence from two generations. Public Health Nutr. 2011, 14, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 2012, 307, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.G.; Kim, S.U.; Wong, V.W. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborty, C.; Das, S. Dynamics of diabetes and obesity: An alarming situation in the developing countries in Asia. Mini Rev. Med. Chem. 2016, 16, 1258–1268. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Larsen, P.; Wang, H.; Popkin, B.M. Overweight Dynamics in Chinese Children and Adults. Obes. Rev. 2014, 15, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wu, W.; Mao, Z.; Huo, W.; Tu, R.; Qian, X.; Zhang, X.; Tian, Z.; Zhang, H.; Jiang, J.; et al. Prevalence and influencing factors of overweight and obesity in a Chinese rural population: The Henan Rural Cohort Study. Sci Rep. 2018, 8, 13101. [Google Scholar] [CrossRef]
- Zhai, F.; Du, S.; Wang, Z.; Zhang, J.; Du, W.; Popki, B. Dynamics of the Chinese Diet and the Role of Urbanicity, 1991–2011. Obes. Rev. 2014, 15. [Google Scholar] [CrossRef]
- Popkin, B.M.; Reardon, T. Obesity and the food system transformation in Latin America. Obes. Rev. 2018, 19, 1028–1064. [Google Scholar] [CrossRef]
- UNICEF-WHO-The World Bank Group. Joint Child Malnutrition Estimates—Levels and Trends, 2018 ed.; World Health Organization: Geneva, Switzerland, 2018; Available online: Http://www.who.int/nutgrowthdb/ estimates2017/en/ (accessed on 17 May 2018).
- Klingberg, S.; Draper, C.E.; Micklesfield, L.K.; Benjamin-Neelon, S.E.; Van Sluijs, E.M.F. Childhood Obesity Prevention in Africa: A Systematic Review of Intervention Effectiveness and Implementation. Int. J. Environ. Res. Public Health 2019, 16, 1212. [Google Scholar] [CrossRef]
- Australian Government, Australian Institute of Health and Welfare. A Picture of Overweight and Obesity in Australia. Available online: https://www.aihw.gov.au/getmedia/172fba28-785e-4a08-ab37-2da3bbae40b8/aihw-phe-216.pdf.aspx?inline=true (accessed on 12 May 2019).
- Finkelstein, E.A.; Trogdon, J.G.; Cohen, J.W.; Dietz, W. Annual Medical Spending Attributable to Obesity: Payer-and Service-Specific Estimates. Health Aff. 2009, 28, w822–w831. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and weight loss: Meta-analysis of randomized controlled trials. Metab. Syndr. Relat. Disord. 2011, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Laccetti, R.; Pota, A.; Stranges, S.; Falconi, C.; Memoli, B.; Bardaro, L.; Guida, B. Evidence on the prevalence and geographic distribution of major cardiovascular risk factors in Italy. Public Health Nutr. 2012, 30, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Childhood Obesity Surveillance Initiative (COSI) Factsheet. Highlights 2015–2017. 2018. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/activities/who-european-childhood-obesity-surveillance-initiative-cosi/cosi-publications/childhood-obesity-surveillance-initiative-cosi-factsheet.-highlights-2015-17-2018 (accessed on 20 March 2019).
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Schmidhuber, J.; Traill, W.B. The changing structure of diets in the European Union in relation to healthy eating guidelines. Public Health Nutr. 2006, 9, 584–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, L.A.; Sarria, A.; Popkin, B.M. The nutrition transition in Spain: A European Mediterranean country. Eur. J. Clin. Nutr. 2002, 56, 992–1003. [Google Scholar] [CrossRef]
- Grosso, G.; Galvano, F. Mediterranean diet adherence in children and adolescents in southern European countries. NFS J. 2016, 3, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Caballero, B. The Nutrition Transition: Global Trends in Diet and Disease; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; pp. 1717–1722. [Google Scholar]
- Kearneys, J. Food Consumptions trends and drivers. Philos. Trans. R. Soc. B Biol. Sci. 2010, 365, 2793–2807. [Google Scholar] [CrossRef]
- Oggioni, C.; Lara, J.; Wells, J.C.; Soroka, K.; Siervo, M. Shifts in population dietary patterns and physical inactivity as determinants of global trends in the prevalence of diabetes: An ecological analysis. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1105–1111. [Google Scholar] [CrossRef]
- Thow, A.M. Trade liberalization and the nutrition transition: Mapping the pathways for public health nutritionists. Public Health Nutr. 2009, 12, 2150–2158. [Google Scholar] [CrossRef]
- Ogden, C.L.; Kuczmarski, R.J.; Flegal, K.M.; Mei, Z.; Guo, S.; Wei, R.; Grummer-Strawn, L.M.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. Centers for Disease Control and Prevention 2000 growth charts for the United States: Improvements to the 1977 National Center for Health Statistics version. Pediatrics 2002, 109, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5 (Suppl. 1), 4–104. [Google Scholar] [CrossRef]
- Magarey, A.M.; Daniels, L.A.; Boulton, T.J. Prevalence of overweight and obesity in Australian children and adolescents: Reassessment of 1985 and 1995 data against new standard international definitions. Med. J. Aust. 2001, 174, 561–564. [Google Scholar] [PubMed]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Finucane, M.M.; Stevens, G.A.; Cowan, M.J.; Danaei, G.; Lin, J.K.; Paciorek, C.J.; Singh, G.M.; Gutierrez, H.R.; Lu, Y.; Bahalim, A.N.; et al. National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 2011, 377, 557–567. [Google Scholar] [CrossRef]
- Bleich, S.N.; Cutler, D.; Murray, C.; Adams, A. Why Is the Developed World Obese? Annu. Rev. Public Health 2008, 29, 273–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagarani, M.; Forleo, M.; Zampino, S. Household Food Expenditure Behaviours and Socioeconomic Welfare in Italy: A Microeconometric Analysis. In Proceedings of the European Association of Agricultural Economists (EAAE) > 113th Seminar, Chania, Crete, Greece, 3–6 September 2009; Available online: https://tind-customer-agecon.s3.amazonaws.com/1f27feaf-1359-44e9-afee-e9b4da06f434?response-content-disposition=inline%3B%20filename%2A%3DUTF-8%27%27Bagarani.pdf&response-content-type=application%2Fpdf&AWSAccessKeyId=AKIAXL7W7Q3XHXDVDQYS&Expires=1559637196&Signature=Y9Kt8nHvnsmR0HPkafRGIzBQNuY%3D (accessed on 4 May 2019).
- Baourakis, G.; Mattas, K.; Zopounidis, C.; Van Dijk, G. A Resilient European Food Industry in a Challenging World; Nova Science Publishers: Hauppauge, NY, USA, 2010; ISBN1 978-1611220322. ISBN2 1611220327. [Google Scholar]
- Conforti, P. Looking Ahead in World Food and Agriculture. Perspectives to 2050; Food and Agriculture Organization of the United Nations, Economic and Social Development Department, Agricultural Development Economics Division: Rome, Italy, 2011. [Google Scholar]
- Behlasen, R. Nutrition transition and food sustainability. Proc. Nutr. Soc. 2014, 73, 385–388. [Google Scholar] [CrossRef] [Green Version]
- Archero, F.; Ricotti, R.; Solito, A.; Carrera, D.; Civello, F.; Di Bella, R.; Bellone, S.; Prodam, F. Adherence to the Mediterranean Diet among School Children and Adolescents Living in Northern Italy and Unhealthy Food Behaviors Associated to Overweight. Nutrients 2018, 10, 1322. [Google Scholar] [CrossRef]
- Ritchie, L.D.; Ivey, S.L.; Woodward-Lopez, G.; Crawford, P.B. Alarming trends in pediatric overweight in the United States. Soc. Prev. Med. 2003, 48, 168–177. [Google Scholar]
- McPherson, K.; Marsh, T.; Brown, M. Foresight, Tackling Obesities: Future Choices—Modelling Future Trends in Obesity and the Impact on Health. 2007. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.629.2896&rep=rep1&type=pdf (accessed on 10 May 2019).
- Rappange, D.R.; Brouver, W.B.F.; Hoogenveen, R.T.; Van Baal, P.H.M. Healthcare Costs and Obesity Prevention, Drug Costs and Other Sector-Specific Consequences. Pharmacoeconomics 2009, 27. [Google Scholar] [CrossRef]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Key Facts. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 March 2019).
- Swinburn, B.A. Obesity prevention: The role of policies, laws and regulations. Aust. New Zealand Health Policy 2008, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Gortmaker, S.L.; Swinburn, B.A.; Levy, D.; Carter, R.; Mabry, P.L.; Finegood, D.T.; Moodie, M.L. Changing the future of obesity: Science, policy, and action. Lancet 2011, 378, 838–847. [Google Scholar] [CrossRef]
- Trust for America’s Health. R.W. Johnson Foundation. Available online: https://stateofobesity.org/wp-content/uploads/2018/09/stateofobesity2018.pdf (accessed on 30 September 2018).
- Dietz, W.H.; Benken, D.E.; Hunter, A.S. Public health law and the prevention and control of obesity. Milbank Q. 2009, 87, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Mensah, G.A.; Goodman, R.A.; Zaza, S.; Moulton, A.D.; Kocher, P.L.; Dietz, W.H.; Pechacek, T.F.; Marks, J.S. Law as a tool for preventing chronic diseases: Expanding the range of effective public health strategies. Prev. Chronic Dis. 2004, 1, A13. [Google Scholar] [PubMed]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo Serra-Majem, L.; Lairon, D.; Estruch, R.; Trichopoulou, A. Mediterranean food pattern and the primary prevention of chronic disease: Recent development. Nutr. Rev. 2009, 67, S111–S116. [Google Scholar] [CrossRef]
- Saulle, R.; Semyonov, L.; La Torre, G. Cost and Cost-Effectiveness of the Mediterranean Diet: Results of a Systematic Review. Nutrients 2013, 5, 4566–4586. [Google Scholar] [CrossRef] [PubMed]
- Traill, W.B.; University of Reading. Poor Diets in Europe: Causes and Implications for Policy. Available online: http://ilo.unimol.it/sidea/images/upload/convegno_2009/plenarie/relazione%20plenaria_traill.pdf (accessed on 3 March 2019).
- Lopez, C.N.; Martinez-Gonzalez, M.A.; Sanchez-Villegas, A.; Alonso, A.; Pimenta, A.M.; Bes-Rastrollo, M. Costs of Mediterranean and western dietary patterns in a Spanish cohort and their relationship with prospective weight change. J. Epidemiol. Community Health 2009, 63, 920–927. [Google Scholar] [CrossRef]
- Bonaccio, M.; Bonanni, A.E.; Di Castelnuovo, A.; De Lucia, F.; Donati, M.B.; De Gaetano, G.; Iacoviello, L.; Moli-sani Project Investigators. Low income is associated with poor adherence to a Mediterranean diet and a higher prevalence of obesity: Cross-sectional results from the Molisani study. BMJ. Open 2012, 2. [Google Scholar] [CrossRef]
- Tiffin, R.; Salois, M. Inequalities in diet and nutrition. Proc. Nutr. Soc. 2012, 71, 105–111. [Google Scholar] [CrossRef]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- Shareck, M.; Frolich, K.L.; Poland, B. Reducing social inequalities in health through settings-related interventions—A conceptual framework. Glob. Health Promot. 2013, 20, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Brownell, K.D. Weight Bias: Nature, Consequences, and Remedies. In Eating Disorders and Obesity, 3rd ed.; A Comprehensive Handbook; Guilford Publications: New York, NY, USA, 2005. [Google Scholar]
- Choquet, H.; Meyre, D. Genomic insights into early-onset obesity. Genome Med. 2010, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Kass, D.; Haslam, D. Is bariatric Surgery the Right Approach to Obesity? 2015. Available online: https://www.pharmaceutical-journal.com/opinion/comment/is-bariatric-surgery-the-right-approach-to-obesity/20067632.article?firstPass=false (accessed on 17 December 2018).
- Hofmann, B. Bariatric surgery for obese children and adolescents: A review of the moral challenges. BMC Med Ethics 2013. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.M.; Butcher, K.F.; Whitmore Schanzenbach, D. Childhood Disadvantage and Obesity: Is Nurture Trumping Nature? NBER Working Paper No. 13479, Issued in October 2007, NBER Program(s): Children, Labor Studies; National Bureau of Economic Research 1050 Massachusetts Avenue: Cambridge, MA, USA, 2007. [Google Scholar]
- Allebeck, P. The prevention paradox or the inequality paradox? Eur. J. Public Health 2008, 18, 215. [Google Scholar] [CrossRef] [PubMed]
- Chiolero, A. Why causality, and not prediction, should guide obesity prevention policy. Lancet Public Health 2018. [Google Scholar] [CrossRef]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy Progress in Obesity Prevention, Emerging Examples, Entrenched Barriers and New Thinking. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61744-X/fulltext (accessed on 19 January 2019).
- EU Working Group on Socio-Economic Inequalities in Health. Monitoring Socio-Economic Inequalities in Health in the European Union: Guidelines and Illustrations. 2001. Available online: http://ec.europa.eu/health/ph_projects/1998/monitoring/fp_monitoring_1998_frep_06_a_en.pdf (accessed on 22 January 2019).
- McAllister, E.J.; Dhurandhar, N.V.; Keith, S.W.; Aronne, L.J.; Barger, J.; Baskin, M.; Benca, R.M.; Biggio, J.; Boggiano, M.M.; Eisenmann, J.C.; et al. Ten putative contributors to the obesity epidemic. Crit. Rev. Food Sci. Nutr. 2009, 49, 868–913. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Willett, W.C.; Hu, F.B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef]
- Samouda, H.; Ruiz-Castell, M.; Bocquet, V.; Kuemmerle, A.; Chioti, A.; Dadoun, F.; Kandala, N.; Stranges, S. Geografical variation of overweight, obesity and related risk factors, Findings from the European Health Examination Survey in Luxembourg 2013–2015. PLoS ONE 2018. [Google Scholar] [CrossRef]
- Brownell, K.D. Behavioral, psychological, and environmental predictors of obesity and success at weight reduction. Int. J. Obes. 1984, 8, 543–550. [Google Scholar]
- WHO. Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/258781/COSI-report-round-1-and-2_final-for-web.pdf?ua=1 (accessed on 2 March 2019).
- Haber, B. The Mediterranean diet: A view from history. Ame. J. Clin. Nutr. 1997, 66, 1053S–1057S. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.D.; Christoffel, K.K.; Necheles, J.W.; Becker, A.B. Social Marketing as a Childhood Obesity Prevention Strategy. Obesity 2010. [Google Scholar] [CrossRef] [PubMed]
- Lycett, K.; Miller, A.; Knox, A.; Dunn, S.; Kerr, J.A.; Sung, V.; Wake, M. ‘Nudge’ interventions for improving children’s dietary behaviours in the home: A systematic review. Obes. Med. 2017. [Google Scholar] [CrossRef]
- Oliver, A. Is nudge an effective public health strategy to tackle obesity? Yes. BMJ 2011, 342, d2168. [Google Scholar] [CrossRef] [PubMed]
- Rayner, G.; Lang, T. Is nudge an effective public health strategy to tackle obesity? No. BMJ 2011, 342, d2177. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, F.; Garnett, E.; Dorsell, C.; Aveyard, P.; Jebb, S.A. Restructuring physical micro-environments to reduce the demand for meat: a systematic review and qualitative comparative analysis. Lancet Planet. Health 2018, 2, e384–e397. [Google Scholar] [CrossRef]
- Arno, A.; Thomas, S. Restructuring physical micro environmentsto reduce the demand for meat:a systematic review and qualitative and comparative analysis The efficacy of nudge theories strategies in influencing adult dietary behaviours, a systematic review and meta analysis. BMC Public Health 2016, 16, 676–697. [Google Scholar] [CrossRef]
- Smith, M.; Topprakkiran, N. Behavioural Insight, Nudge and the Choice in Obesity Policy. Available online: https://rsa.tandfonline.com/doi/full/10.1080/01442872.2018.1554806?scroll=top&needAccess=true#.XBPuja2h3q3 (accessed on 9 March 2019).
- WHO. Key Considerations for the Use of Law to Prevent Noncommunicable Diseases in the WHO European Region Report of an Intensive Legal Training and Capacity-Building Workshop on Law and Noncommunicable Diseases. 2016. Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/333954/Moscow-report.pdf?ua=1 (accessed on 28 January 2019).
- Holcombe, R.G. Selective Excise Taxation from an Interest-Group Perspective. In Taxing Choice: The Predatory Politics of Fiscal Discrimination; William, F., Shughart, I.I., Eds.; Rutgers—The State University of New Jersey: New Brunswick, NJ, USA, 1998; pp. 81–100. [Google Scholar]
- Fletcher, J.M.; Frisvold, D.; Tefft, N. Can Soft Drink Taxes Reduce Population Weight? Available online: http://www.economics.emory.edu/Working_Papers/wp/2008wp/Frisvold_08_08_paper.pdf (accessed on 28 January 2019).
- Kerry. Global Map of the Sugar Tax, 2018. Available online: https://kerrydotcomcdn.azureedge.net/cdprod/Media/infographics/kerry-sugar-tax-infographic (accessed on 28 January 2019).
- Bødker, M.; Pisinger, C.; Toft, U.; Jørgensen, T. The Danish fat tax—Effects on consumption patterns and risk of ischaemic heart disease. Prev. Med. 2015, 77, 200–203. [Google Scholar] [CrossRef]
- Silver, L.D.; Ng, S.W.; Ryan-Ibarra, S.; Taillie, L.S.; Induni, M.; Miles, D.R.; Poti, J.M.; Popkin, B.M. Changes in prices, sales, consumer spending, and beverage consumption one yearafter a tax on sugar-sweetened beverages in Berkeley, California, US: A before-and-after study. PLoS Med. 2017. [Google Scholar] [CrossRef]
- Thelancet.com/diabetes-endocrinology Vol 5 April. Available online: https://www.thelancet.com/pdfs/journals/landia/PIIS2213-8587(17)30070-0.pdf (accessed on 26 January 2019).
- Mytton, O.; Gray, A.; Rayner, M.; Rutter, H. Could targeted food taxes improve health? J. Epidemiol. Community Health 2007, 61, 689–694. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.M.; Dulloo, A.G.; Montani, J.P. Sugar drinks in the pathogenesis of obesity and cardiovascular diseases. Int. J. Obes. (Lond.) 2008, 32 (Suppl. 6), S28–S34. [Google Scholar] [CrossRef]
- Choi, H.K.; Willett, W.; Curhan, G. Fructose-rich beverages and risk of gout in women. JAMA 2010, 304, 2270–2278. [Google Scholar] [CrossRef] [PubMed]
- Adamowicz, J.; DrewaIs, T. Is there a link between soft drinks and erectile dysfunction? Cent. Eur. J. Urol. 2011, 64, 140–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satterthwaite, D.; McGranahan, G.; Tacoli, C. Urbanization and its implications for food and farming, review. R. Soc. Philos. Trans. B 2010, 365, 2809–2820. [Google Scholar] [CrossRef] [PubMed]
- Franck, C.; Grandi, S.M.; Eisenberg, M.J. Taxing junk food to counter obesity. Am. J. Public Health 2013, 103, 1949–1953. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.M.; Frisvold, D.E.; Tefft, N. The effects of soft drink taxes on child andadolescent consumption and weight outcomes. J. Public Econ. 2010, 94, 967–974. [Google Scholar] [CrossRef]
- Chen, L.; Appel, L.J.; Loria, C.; Lin, P.H.; Champagne, C.M.; Elmer, P.J.; Ard, J.D.; Mitchell, D.; Batch, B.C.; Svetkey, L.P.; et al. Reduction in consumption of sugar-sweetened beverages is associated with weight loss: The PREMIER trial. Am. J. Clinnutr. 2009, 89, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Ludwig, D.S.; Sonneville, K.; Gortmaker, S.L. Impact of change in sweetened caloric beverage consumption on energy intake among children and adolescents. Arch. Pediatr. Adolesc. Med. 2009, 163, 336–343. [Google Scholar] [CrossRef]
- Williams, R.; Christ, K. Mercatus on Policy, Taxing Sin: Are Excise Taxes Efficient? N°52. Available online: https://www.mercatus.org/system/files/RSP_MOP52_Taxing_Sins_web.pdf (accessed on 2 January 2019).
- Studio Censis Coldiretti. Primo Rapporto Sulle Abitudini Alimentari Degli Italiani Sintesi dei Principali Risultati. Available online: https://www.coldiretti.it/archivio/censis-il-primo-rapporto-sulle-abitudini-alimentari-degli-italiani-alcuni-flash-19-05-2010 (accessed on 24 January 2019).
- WHO. Fiscal Policies for Diet and the Prevention of NCD. 2016. Available online: http://apps.who.int/iris/bitstream/handle/10665/250131/9789241511247-eng.pdf;jsessionid=3A372C03CFB2A8FC33E4A03A37CFF073?sequence=1, pag.23 (accessed on 24 January 2019).
- Garde, A.; Bartlett, O.; Ward, K. Fizzy Drinks Tax Alone Won’t Solve Childhood Obesity Nightmare. Available online: https://theconversation.com/fizzy-drinks-tax-alone-wont-solve-childhood-obesity-nightmare-56523 (accessed on 24 January 2019 ).
- Di Nicolantonio, J.J.; O’Keefe, J.H.; Wilson, W.L. Sugar addiction: Is it real? A narrative review. Br. J. Sports Med. 2018, 52, 910–913. [Google Scholar] [CrossRef]
- Lien, L.; Lien, N.; Heyerdahl, S.; Thoresen, M.; Bjertness, E. Consumption of Soft Drinks and Hyperactivity, Mental Distress, and Conduct Problems Among Adolescents in Oslo, Norway. Am. J. Public Health 2006, 96, 1815–1820. [Google Scholar] [CrossRef]
- Wansick, B.; Chandon, P. Can “Low-Fat” Nutrition Labels Lead to Obesity? J. Mark. Res. 2006, 43, 605–617. [Google Scholar] [CrossRef]
- Scholsser, E. Fast-Food Nation; Allen Lane The Penguin Press: London, UK, 2001. [Google Scholar]
- Schlosser, E. Still a Fast Food Nation: Eric Schlosser Reflects on 10 Years Later. Retrieved 2012, 2, 2017. [Google Scholar]
- Public Health England. Sugar Reduction and Wider Reformulation Programme: Report on Progress towards the First 5% Reduction and Next Steps. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/709008/Sugar_reduction_progress_report.pdf (accessed on 29 March 2019).
- Nestle, M. Food Politics: How the Food Industry Manipulates What We Eat to the Detriment of Our Health; University of California Press: Berkeley, CA, USA, 2002. [Google Scholar]
- Critser, G. Fat Land: How Americans Became the Fattest People in the World; Houghton Mifflin: New York, NY, USA, 2002. [Google Scholar]
- Garde, A.; Jeffery, B.; Rigby, N. Implementing the WHO Recommendations whilst Avoiding Real, Perceived or Potential Conflicts of Interest. Eur. J. Risk Regul. 2017, 8, 237–250. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Salt Targets 2017: Progress Report a Report on the Food Industry’s Progress towards Meeting the 2017 Salt Targets. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/765571/Salt_targets_2017_progress_report.pdf (accessed on 3 February 2019).
- Garde, A.; Davies, S.; Landon, J. The UK Rules on Unhealthy Food Marketing to Children. Eur. J. Risk Regul. 2017, 8, 270–280. [Google Scholar] [CrossRef]
- Nestle, M. Food Marketing and Childhood Obesity—A Matter of Policy. N. Engl. J. Med. 2006, 354, 2527–2529. [Google Scholar] [CrossRef] [PubMed]
- Cezar, A. The Effects of Television Food Advertising on Childhood Obesity. Nev. J. Public Health 2008, 5, 2. [Google Scholar]
- WHO. Evaluating Implementation of the WHO Set of Recommendations on the Marketing of Foods and Non-Alcoholic Beverages to Children, Progress, Challenges and Guidance for Next Steps in the WHO European Region. Available online: http://www.euro.who.int/__data/assets/pdf_file/0003/384015/food-marketing-kids-eng.pdf (accessed on 20 February 2019).
- Fuhrer, R.; Shipley, M.J.; Chastang, J.F.; Schmaus, A.; Niedhammer, I.; Stansfeld, S.A.; Goldberg, M.; Marmot, M.G. Socioeconomic position, health, and possible explanations: A tale of two cohorts. Am. J. Public Health 2002, 92, 1290–1294. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroder, H.; Marrugat, J.; Covas, M.I. High monetary costs of dietary patterns associated with lower body mass index: A population-based study. Int. J. Obes. 2006, 30, 1574–1579. [Google Scholar] [CrossRef] [PubMed]
- Power, E.M. SUPPLEMENT 3: Understanding the Forces That Influence Our Eating Habits: What We Know and Need to Know (JULY/AUGUST 2005). Can. J. Public Health 2005, 96, S37–S42. Available online: https://www.jstor.org/stable/41994471 (accessed on 20 February 2019).
- Phull, S. The Mediterranean Diet: Socio-cultural Relevance for Contemporary Health Promotion. Open Public Health J. 2015, 8, 35–40. [Google Scholar] [CrossRef] [Green Version]
- UNESCO. Representative List of the Intangible Cultural Heritage of Humanity. 2013. Available online: Http://www.unesco.org/ culture/ich/RL/ (accessed on 29 April 2014).
- Keys, A. Mediterranean diet and public health: Personal reflections. Am. J. Clin. Nutr. 1995, 61 (Suppl. 6), 1321S–1323S. [Google Scholar] [CrossRef] [PubMed]
- León-Munoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Mesas, A.E.; Aguilera, M.T.; Banegas, J.R.; Rodríguez-Artalejo, F. Adherence to The Mediterranean Diet pattern has declined in Spanish adults. J. Nutr. 2012, 142, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Eichelsdoerfer, P. Mediterr. Diet: Does It Have Cost More? Public Health Nutr. 2009, 12, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- OECD. Measuring Leisure in OECD Countries. In Society at a Glance 2009; OECD Social Indicators; OECD: Paris, France, 2009; pp. 19–49. [Google Scholar]
- Laverack, G. Public Health, Power, Empowerment and Professional Practice; Palgrave McMillan: Basingstoke, UK, 2009. [Google Scholar]
- Handy, S.L.; Boarnet, M.G.; Ewing, R.; Killingsworth, R.E. How the built environment affects physical activity: Views from urban planning. Am. J. Prev. Med. 2002, 23, 64–73. [Google Scholar] [CrossRef]
- Thorndike, A.N.; Sonnenberg, L.; Riis, J.; Barraclough, S.; Levy, D.E. A 2-Phase Labeling and Choice Architecture Intervention to Improve Healthy Food and Beverage Choices. Am. J. Public Health 2012, 102, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Wansink, B.; Just, D.R.; Payne Collin, R. Mindless Eating and Healthy Heuristics for the Irrational. Am. Econ. Rev. 2009, 99, 165–169. [Google Scholar] [CrossRef]
- Bourdieu, P.; Saint-Martin, M. Anatomie dugoût. Actes Rech. Sci. Soc. 1976, 2, 18–43. [Google Scholar]
- Napier, A.D.; Ancarno, C.; Butler, B.; Calabrese, J.; Chater, A.; Chatterjee, H.; Guesnet, F.; Horne, R.; Jacyna, S.; Jadhav, S.; et al. Culture and health. Lancet 2014, 384, 1607–1639. [Google Scholar] [CrossRef]
- Marrone, G. Semiotica del Gusto. Linguaggi Della Cucina, del Cibo, Della Tavola; Mimesis Insegne: Sesto San Giovanni, Milano, Italy, 2016. [Google Scholar]
- World Health Organization (WHO). Behaviour Change Strategies and Health: The Role of Health Systems; EUR/RC58/Tbilisi, Georgia; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Sassi, F.; Cecchini, M.; Lauer, J.; Chisholm, D. Improving lifestyles, tackling obesity: The health and economic impact of prevention strategies. In OECD Health Working Papers; OECD Publishing: Paris, France, 2009. [Google Scholar]
- Ward, D.S.; Welker, E.; Choate, A.; Henderson, K.E.; Lott, M.; Tovar, A.; Wilson, A.; Sallis, J.F. Strength of obesity prevention interventions in early care and education settings: A systematic review. Prev. Med. 2017, 95, S37–S52. [Google Scholar] [CrossRef]
- Abraham, C.; Kok, G.; Schaalma, H.; Luszczynska, A. Health Promotion. The International Association of Applied Psychology Handbook of Applied Psychology; Martin, P., Cheung, F., Kyrios, M., Littlefield, L., Knowles, L., Overmier, M., Eds.; Wiley-Blackwell: Oxford, UK, 2010. [Google Scholar]
- Nixon, C.A.; Moore, H.J.; Douthwaite, W.; Gibson, E.L.; Vogele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Summerbell, C. Identifying effective behavioural models and behaviour change strategies underpinning preschool-and school-based obesity prevention interventions aimed at 4–6-year-olds: A systematic review. Obes. Rev. 2012. [Google Scholar] [CrossRef]
- Britt, E.; Hudson, S.M.; Blampied, N.M. Motivational interviewing in health settings: A review. Patient Educ. Couns. 2004, 53, 147–155. [Google Scholar] [CrossRef]
- Bernhardt, J.M. Communication at the Core of Effective Public Health. Am. J. Public Health 2004, 94, 2051–2053. [Google Scholar] [CrossRef] [PubMed]
- George, E.; Kucianski, T.; Mayr, H.; Moschonis, G.; Tierney, A.; Itsiopoulos, C. A Mediterranean diet model in Australia: Strategies for Translating the Traditional Mediterranean Die tinto a Multicultural Setting. Nutrients 2018, 10, 465. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Foods | Mediterranean Diet | Western Diets |
|---|---|---|
| Vegetables | Every main meal (≥2 servings) | Rarely |
| Fruits | Every main meal (1-2 servings) | Rarely |
| Bread/pasta/rice/couscous/other cereals | Every main meal (1-2 servings, preferably whole grain) | Rarely whole grain cereals, often refined grains |
| Olive Oil | Every main meal (3-4 servings, expecially extra virgin) | Rarely olive oil, often replaced by margarine and butter |
| Nuts/seeds/olives | Every day (1-2 servings) | Occasionally |
| Dairy Foods | Every day in moderate portions (2 servings, preferably low fat) | Often high fat dairy foods |
| Herbs/spices/garlic/onions | Every day (less added salt) | Less often |
| Legumes | Weekly (≥2 servings) | Less often |
| Potatoes | Weekly (≤3 servings) | Less often |
| Eggs | Weekly (2-4 servings) | Less often |
| Fish/seafood | Weekly (≥2 servings) | Less often |
| White meat | Weekly (2 servings) | Less often |
| Red meat | Weekly (<2 servings) | Often |
| Processed meat | Weekly (≤1 serving) | Often |
| Sweets | Weekly (≤2 servings) | Often |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients 2019, 11, 1306. https://doi.org/10.3390/nu11061306
D’Innocenzo S, Biagi C, Lanari M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients. 2019; 11(6):1306. https://doi.org/10.3390/nu11061306
Chicago/Turabian StyleD’Innocenzo, Santa, Carlotta Biagi, and Marcello Lanari. 2019. "Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet" Nutrients 11, no. 6: 1306. https://doi.org/10.3390/nu11061306
APA StyleD’Innocenzo, S., Biagi, C., & Lanari, M. (2019). Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients, 11(6), 1306. https://doi.org/10.3390/nu11061306