Mobile Phone Text Message Intervention on Diabetes Self-Care Activities, Cardiovascular Disease Risk Awareness, and Food Choices among Type 2 Diabetes Patients



Abstract
:1. Introduction
2. Materials and Methods
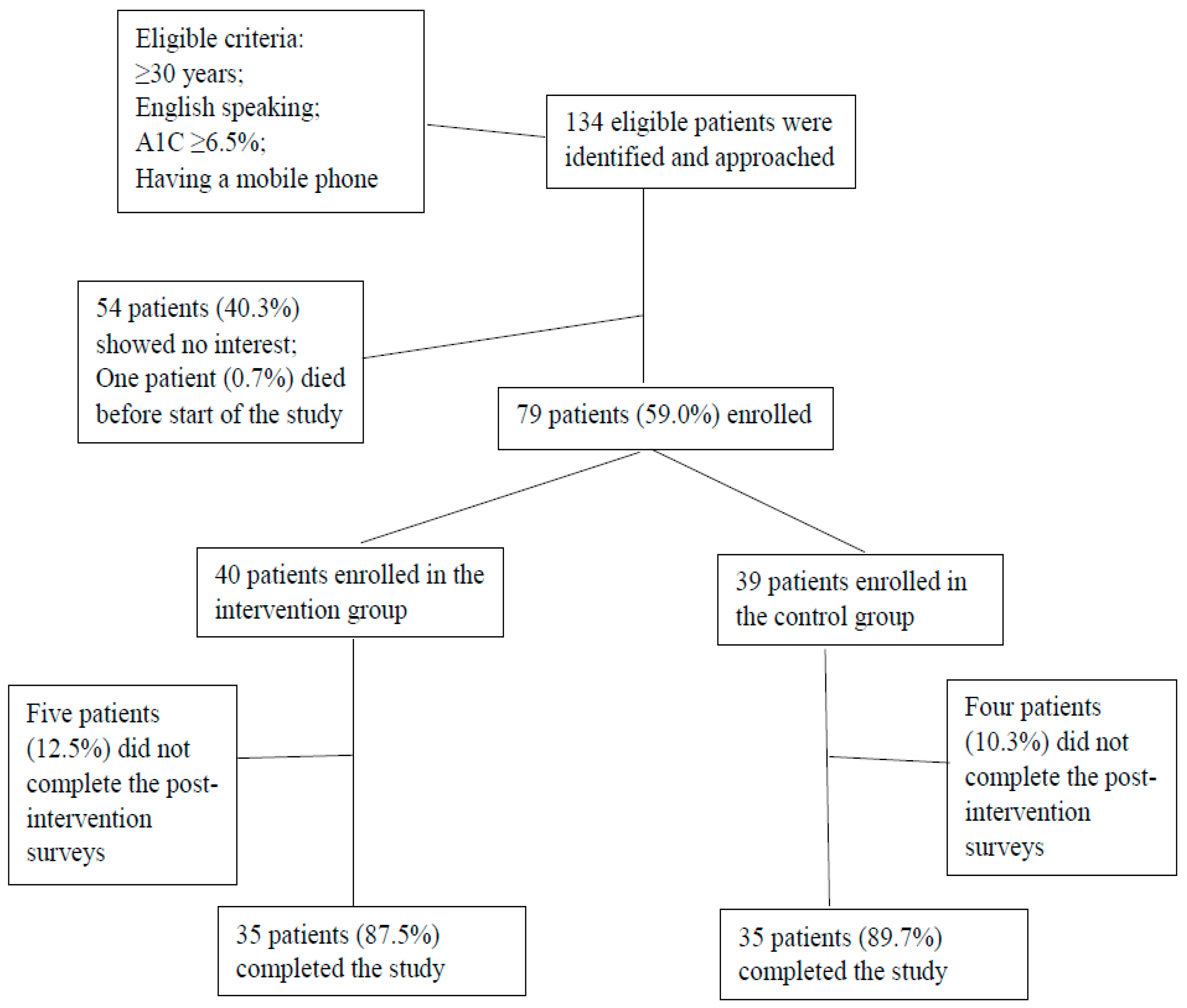
2.1. Participants
2.2. Study Design
2.3. Outcome Measures
2.3.1. Diabetes Self-Care Activities
2.3.2. Dietary Intake and Physical Activity
2.3.3. CVD Risk Awareness
2.3.4. Home Food Self-Inventory
2.4. Data Analysis
3. Results
3.1. Characteristics of Study Participants and Usefulness of Educational Text Messages
3.2. Diabetes Self-Care Activities, Dietary Intake, Physical Activity, and Awareness of CVD Risk
3.3. Home Food Availabilities Related to Food Choices
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. 2017. Available online: https://www.cdc.gov/diabetes/pdfs/data/statistics/national diabetes-statistics-report.pdf (accessed on 21 March 2018).
- Nesto, R. CHD: A major burden in type 2 diabetes. Acta Diabetol. 2001, 38, S3–S8. [Google Scholar] [CrossRef]
- Choi, S.; Rankin, S.; Steward, A.; Oka, R. Perceptions of Coronary Heart Disease risk in Korean immigrants with type 2 diabetes. Diabetes Educ. 2008, 34, 484–492. [Google Scholar] [CrossRef]
- Carroll, C.; Naylor, E.; Marsden, P.; Dornan, T. How do people with type 2 diabetes perceive and respond to cardiovascular risk? Diabet. Med. 2003, 20, 355–360. [Google Scholar] [CrossRef]
- American Diabetes Association. Prevention of delay of type 2 diabetes: Standards of medical care in diabetes—2018. Diabetes Care 2018, 41 (Suppl. 1), S51–S54. [Google Scholar] [CrossRef]
- American Diabetes Association. Evidence-based nutrition principles and recommendations for the treatment and prevention of diabetes and related complications. Diabetes Care 2002, 25, S50–S60. [Google Scholar] [CrossRef]
- Miller, C.; Edwards, L. Development and validation of a shelf inventory to evaluate household food purchases among older adults with diabetes mellitus. J. Nutr. Educ. Behav. 2002, 34, 261–267. [Google Scholar] [CrossRef]
- Tomky, D.; Cypress, M.; Dang, D.; Maryniuk, M.; Peyrot, M.; Mensing, C. AADE Position Statement. AADE7 Self-Care Behaviors. Diabetes Educ. 2008, 34, 445–449. [Google Scholar] [CrossRef]
- Ancker, J.S.; Senathirajah, Y.; Kukafka, R.; Starren, J.B. Design features of graphs in health risk communication: A systematic review. J. Am. Med. Inform Assoc. 2006, 13, 608–618. [Google Scholar] [CrossRef]
- Fjeldsoe, B.S.; Marshall, A.L.; Miller, V.D. Behavior change interventions delivered by mobile telephone short-message service. Am. J. Prev. Med. 2009, 35, 165–173. [Google Scholar] [CrossRef]
- Kim, H.S.; Hwang, Y.; Lee, J.H.; Oh, H.Y.; Kim, Y.J.; Kwon, H.Y.; Kang, H.; Kim, H.; Park, R.W.; Kim, J.H. Future prospects of health management systems using cellular phones. Telemed. J. E Health 2014, 20, 544–551. [Google Scholar] [CrossRef]
- Fortmann, A.L.; Gallo, L.C.; Garcia, M.I.; Taleb, M.; Euyoque, J.A.; Clark, T.; Skidmore, J.; Ruiz, M.; Dharkar-Surber, S.; Schultz, J.; et al. Dulce Digital: An mHealth SMS-Based Intervention Improves Glycemic Control in Hispanics With Type 2 Diabetes. Diabetes Care 2017, 40, 1349–1355. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, M.; Wu, S. Phone messaging to prompt physical activity and social support among low-income Latino patients with Type 2 diabetes: A randomized pilot study. J. Med. Internet Res. 2017, 2, e8. [Google Scholar] [CrossRef]
- Sawesi, S.; Rashrash, M.; Phalakornkule, K.; Carpenter, J.S.; Jones, J.F. The impact of information technology on patient engagement and health behavior change: A systematic review of the literature. J. Med. Internet Res. 2016, 4, e1. [Google Scholar] [CrossRef]
- Arora, S.; Peters, A.L.; Burner, E.; Lam, C.N.; Menchine, M. Trial to examine text message-based mHealth in emergency department patients with diabetes (TExT-MED): A randomized controlled trial. Ann. Emerg. Med. 2014, 63, 745–754. [Google Scholar] [CrossRef]
- American Association of Diabetes Educators (AADE) AADE7. Self-Care Behaviors. Available online: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors (accessed on 21 March 2018).
- Toobert, D.J.; Hampson, S.E.; Glasgow, R.E. The summary of diabetes self-care activities measure. Diabetes Care 2000, 23, 943–950. [Google Scholar] [CrossRef]
- NutritionQuest. Assessment and Analysis Services. Block Food Screeners; Fat/Sugar/Fruit/Vegetable Screener. Available online: http://www.nutritionquest.com/assessment/ (accessed on 21 March 2018).
- NutritionQuest. Assessment and Analysis Services. Block Food Screeners; Physical Activity Screener. Available online: http://www.nutritionquest.com/assessment/ (accessed on 21 March 2018).
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A Second Update of Codes and MET Values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Becker, D.M.; Levine, D.M. Risk perception, knowledge, and lifestyles in siblings of people with premature coronary disease. Am. J. Prev. Med. 1987, 3, 45–50. [Google Scholar] [CrossRef]
- Nepper, M.J.; Chai, W. Validation of a home food checklist to assess the home food environment of school-age children. Health Behav. Policy Rev. 2016, 3, 348–360. [Google Scholar] [CrossRef]
- Boles, R.E.; Scharf, C.; Filigno, S.S.; Saelens, B.E.; Stark, L.J. Differences in home food and activity environments between obese and healthy weight families of preschool children. J. Nutr. Educ. Behav. 2013, 45, 222–231. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Nelson, M.C.; Lytle, L.; Moe, S.; Heitzler, C.; Pasch, K.E. The validation of a home food inventory. Int. J. Behav. Nutr. Phys. Act 2008, 5. [Google Scholar] [CrossRef]
- U.S. Department of Health & Human Services, National Heart, Lung, and Blood Institute. Choosing foods for your family: Go, Slow, Whoa Foods. Adapted from Catch: Coordinated Approach to School Heart. Available online: https://www.nhlbi.nih.gov/health/educational/wecan/eat-right/choosing-foods.htm (accessed on 19 April 2016).
- American Diabetes Association. Glycemic Index and Diabetes. Available online: http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/understanding-carbohydrates/glycemic-index-and-diabetes.html (accessed on 29 January 2019).
- Shadish, W.; Cook, T.D.; Campbell, D.T. Experimental and Quasi-Experimental Designs for Generalized Causal Inference; Houghton, Mifflin and Company: Boston, MA, USA, 2002. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 115–159. [Google Scholar] [CrossRef]
- Nundy, S.; Mishra, A.; Hogan, P.; Lee, S.M.; Solomon, M.C.; Peek, M.E. How do mobile phone diabetes programs drive behavior change? Diabetes Educ. 2014, 40, 806–819. [Google Scholar] [CrossRef]
- Tamban, C.; Isip-Tan, I.T.; Jimeno, C. Use of short message services (SMS) for the management of Type 2 diabetes: A randomized controlled trial. JASEAN Fed. Endocr. Soc. 2013, 28, 143–148. [Google Scholar] [CrossRef]


{kind=link}
| AADE7TM Handout Titles/Topics | Contents of Text Messages a |
|---|---|
| Healthy Eating (Weeks 1 and 7) | 1) Eat breakfast every day! |
| 2) There are only three main types of nutrients in foods: carbohydrates, proteins, and fats. A healthy meal will include all three of these. | |
| 3) Do not skip meals! Remember to eat regular meals and snacks every day. | |
| For more info: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/healthy-eating | |
| Healthy Coping (Weeks 2 and 8) | 1) Think positive! Feeling down? Remember your successes and feel good about your progress with diabetes. |
| 2) Build healthy relationships. You are not alone when you have diabetes. | |
| 3) If you are sad, anxious or stressed, go for a walk or stand up and stretch. | |
| For more info: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/healthy-coping | |
| Monitoring (Weeks 3 and 9) | 1) Checking your blood sugars gives you vital information about your diabetes control. |
| 2) Monitoring your blood sugars helps you know when they are on target. | |
| 3) Call your doctor or diabetes educator if you are concerned about your blood sugars. | |
| For more info: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/ aade7-self-care-behaviors-monitoring | |
| Being Active (Weeks 4 and 10) | 1) Being active has many health benefits, like improving blood pressure and blood sugars. |
| 2) If you haven’t exercised for a while, start with a five minute walk and increase gradually. | |
| 3) Break activity into three ten minute sessions. | |
| For more info: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/being-active | |
| Taking Medication and Problem Solving (Weeks 5 and 11) | 1) Take notes when you visit with your doctor about your medication. |
| 2) Learn what causes your blood sugar to go above or below target. | |
| 3) Talk to your doctor about how to improve your blood sugar. | |
| For more info: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/ taking-medication https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/problem-solving | |
| Reducing Risks (Weeks 6 and 12) | 1) See your eye doctor at least once a year |
| 2) Keep a wallet card that lists all of the tests you should be regularly getting and the targets for each. | |
| 3) Lowering your cholesterol can decrease your risk for a stroke. Talk to your doctor about what you can do. | |
| For more info: https://www.diabeteseducator.org/patient-resources/aade7-self-care-behaviors/reducing-risks |
| Characteristics | Intervention | Control | p Value b |
|---|---|---|---|
| N | 40 | 39 | |
| Age (year) | 58.0 ± 10.6 | 55.7 ± 12.2 | 0.21 |
| Sex (%) | 0.82 | ||
| Male | 34.7 | 32.9 | |
| Female | 65.3 | 67.1 | |
| Race/ethnicity (%) | 0.01 | ||
| White | 84.0 | 93.2 | |
| Black | 2.7 | 5.4 | |
| Hispanic | 8.0 | 0 | |
| Asian | 2.7 | 0 | |
| Other | 2.7 | 1.4 | |
| BMI (kg/m2) | 34.6 ± 9.05 | 35.9 ± 6.1 | 0.30 |
| Hemoglobin A1C (%) c | 7.8 ± 1.4 | 8.2 ± 1.9 | 0.09 |
| College graduate (%) | 49.3 | 33.8 | 0.05 |
| Having diabetes <1 year (%) | 12.0 | 20.3 | 0.17 |
| Having diabetes ≥5 years (%) | 73.3 | 58.1 | 0.05 |
| Taking diabetes medication (%) | 92.0 | 91.9 | 0.98 |
| Current smoker (%) | 4.0 | 8.0 | 0.30 |
| Variable | Baseline | 12-Week Follow-Up | Absolute Change a | Relative Change b | |||
|---|---|---|---|---|---|---|---|
| Mean (SE)c | pd | Mean (SE) c | pd | Mean (SE)c | pe | ||
| Diabetes Self-Care Activities (day/week) | |||||||
| General diet for healthy eating | |||||||
| Intervention | 4.66 (0.43) | 0.14 | 5.18 (0.46) | 0.61 | 0.76 (0.52) | 0.15 | 16% |
| Control | 5.22 (0.46) | 4.98 (0.48) | |||||
| Specific diet for healthy eating | |||||||
| Intervention | 4.20 (0.40) | 0.93 | 4.03 (0.43) | 0.62 | −0.21 (0.48) | 0.67 | −5% |
| Control | 4.17 (0.43) | 4.21 (0.45) | |||||
| Exercise | |||||||
| Intervention | 5.14 (0.61) | 0.67 | 4.45 (0.65) | 0.77 | −0.07 (0.74) | 0.93 | −1% |
| Control | 4.91 (0.65) | 4.29 (0.68) | |||||
| Blood glucose testing | |||||||
| Intervention | 5.06 (0.62) | 0.08 | 5.28 (0.66) | 0.49 | 0.57 (0.75) | 0.45 | 11% |
| Control | 6.01 (0.67) | 5.66 (0.69) | |||||
| Medication adherence | |||||||
| Intervention | 6.05 (0.35) | 0.51 | 6.35 (0.38) | 0.09 | 0.33 (0.42) | 0.44 | 5% |
| Control | 5.85 (0.38) | 5.82 (0.39) | |||||
| Foot care | |||||||
| Intervention | 4.23 (0.41) | 0.79 | 4.86 (0.43) | 0.08 | 0.53 (0.49) | 0.28 | 13% |
| Control | 4.13 (0.43) | 4.23 (0.45) | |||||
| CVD Risk Awareness | |||||||
| Intervention | 1.01 (0.23) | 0.21 | 1.26 (0.25) | 0.13 | 0.58 (0.29) | 0.04 | 57% |
| Control | 1.27 (0.25) | 0.94 (0.26) | |||||
| PA (METfminute/week) | |||||||
| Total PA | |||||||
| Intervention | 4806 (1451) | 0.08 | 5548 (1645) | 0.02 | 768 (1533) | 0.62 | 16% |
| Control | 2904 (1541) | 2877 (1602) | |||||
| Moderate/vigorous PA | |||||||
| Intervention | 2112 (1435) | 0.25 | 3163 (1555) | 0.006 | 1688 (1300) | 0.20 | 80% |
| Control | 1042 (1430) | 405 (1532) | |||||
| Dietary Intake | |||||||
| Total calories (kcal/day) | |||||||
| Intervention | 1598 (152) | 0.43 | 1499 (161) | 0.79 | −134 (176) | 0.45 | −8% |
| Control | 1417 (161) | 1452 (9168) | |||||
| Carbohydrates (g/day) | |||||||
| Intervention | 162.3 (17.3) | 0.54 | 153.4 (18.2) | 0.81 | −12.5 (20.0) | 0.53 | −8% |
| Control | 140.2 (18.3) | 143.9 (19.1) | |||||
| Total sugar (g/day) | |||||||
| Intervention | 58.9 (8.4) | 0.52 | 52.4 (8.9) | 0.50 | 0.4 (9.7) | 0.96 | 1% |
| Control | 49.6 (8.9) | 44.7 (9.3) | |||||
| Added sugar (g/day) | |||||||
| Intervention | 34.8 (7.3) | 0.39 | 29.6 (7.7) | 0.25 | 2.1 (8.4) | 0.80 | 6% |
| Control | 30.1 (7.7) | 22.9 (8.0) | |||||
| Total fat (g/day) | |||||||
| Intervention | 67.3 (7.0) | 0.28 | 61.1 (7.4) | 0.89 | −7.0 (8.1) | 0.39 | −10% |
| Control | 60.1 (7.4) | 60.9 (7.7) | |||||
| Saturated fat (g/day) | |||||||
| Intervention | 23.1 (2.5) | 0.30 | 21.0 (2.6) | 0.98 | −2.1 (2.9) | 0.47 | −9% |
| Control | 21.3 (2.7) | 21.3 (2.8) | |||||
| Protein (g/day) | |||||||
| Intervention | 70.4 (6.9) | 0.71 | 68.3 (7.2) | 0.62 | −5.1 (7.9) | 0.53 | −7% |
| Control | 62.4 (7.3) | 65.3 (7.6) | |||||
| Food Availability | Baseline | 12-Week Follow-Up | Absolute Change a | Relative Change b | |||
|---|---|---|---|---|---|---|---|
| Mean (SE) c | pd | Mean (SE) c | pd | Mean (SE) c | pe | ||
| Fruits | |||||||
| Total | |||||||
| Intervention | 0.06 (0.04) | 0.29 | 0.08 (0.04) | 0.001 | 0.04 (0.03) | 0.15 | 67% |
| Control | 0.03 (0.04) | 0.01 (0.04) | |||||
| Fresh | |||||||
| Intervention | 0.05 (0.09) | 0.94 | 0.17 (0.08) | 0.0005 | 0.16 (0.06) | 0.01 | 320% |
| Control | 0.05 (0.09) | 0.01 (0.09) | |||||
| Canned/jarred/dried | |||||||
| Intervention | 0.06 (0.06) | 0.15 | 0.04 (0.05) | 0.35 | −0.02 (0.04) | 0.63 | −33% |
| Control | 0.01 (0.06) | 0.02 (0.06) | |||||
| Frozen | |||||||
| Intervention | 0.05 (0.04) | 0.18 | 0.02 (0.04) | 0.27 | −0.008 (0.03) | 0.78 | −16% |
| Control | 0.02 (0.04) | −0.005 (0.04) | |||||
| Vegetables | |||||||
| Total | |||||||
| Intervention | 0.13 (0.05) | 0.79 | 0.11 (0.05) | 0.98 | −0.009 (0.04) | 0.82 | −7% |
| Control | 0.12 (0.05) | 0.11 (0.05) | |||||
| Fresh | |||||||
| Intervention | 0.06 (0.09) | 0.94 | 0.18 (0.09) | 0.0008 | 0.15 (0.07) | 0.02 | 250% |
| Control | 0.06 (0.09) | 0.02 (0.09) | |||||
| Canned/jarred/dried | |||||||
| Intervention | 0.06 (0.06) | 0.12 | 0.05 (0.05) | 0.31 | −0.02 (0.04) | 0.62 | −33% |
| Control | 0.01 (0.05) | 0.02 (0.06) | |||||
| Frozen | |||||||
| Intervention | 0.04 (0.03) | 0.21 | 0.02 (0.03) | 0.11 | 0.003 (0.02) | 0.90 | 8% |
| Control | 0.02 (0.03) | −0.005 (0.03) | |||||
| All healthy foodsf | |||||||
| Intervention | 1.00 (0.06) | 0.45 | 1.08 (0.06) | 0.68 | 0.01 (0.06) | 0.82 | 1% |
| Control | 1.04 (0.06) | 1.10 (0.06) | |||||
| All unhealthy foods | |||||||
| Intervention | 1.41 (0.09) | 0.83 | 1.50 (0.09) | 0.75 | 0.04 (0.10) | 0.70 | 3% |
| Control | 1.42 (0.09) | 1.47 (0.10) | |||||
| Based on Glycemic Index (GI)g | |||||||
| Fruits | |||||||
| Low GI | |||||||
| Intervention | 11.03 (2.15) | 0.25 | 10.68 (2.17) | 0.05 | 1.43 (2.35) | 0.54 | 13% |
| Control | 9.06 (2.23) | 7.28 (2.34) | |||||
| Medium GI | |||||||
| Intervention | 14.75 (3.15) | 0.43 | 17.51 (3.17) | 0.004 | 5.27 (3.43) | 0.13 | 36% |
| Control | 12.78 (3.27) | 10.27 (3.42) | |||||
| High GI | |||||||
| Intervention | 8.07 (9.68) | 0.02 | 40.02 (9.75) | 0.03 | 34.79 (10.54) | 0.001 | 431% |
| Control | 25.96 (10.04) | 23.13 (10.50) | |||||
| Vegetables | |||||||
| Low GI | |||||||
| Intervention | 8.90 (1.34) | 0.77 | 9.09 (1.35) | 0.69 | 0.74 (1.46) | 0.61 | 8% |
| Control | 9.31 (1.39) | 8.67 (1.45) | |||||
| Medium GI | |||||||
| Intervention | 47.83 (7.85) | 0.67 | 32.24 (7.91) | 0.009 | −19.33 (0.03) | 0.03 | −40% |
| Control | 45.13 (8.15) | 48.87 (8.52) | |||||
| High GI | |||||||
| Intervention | 91.58 (15.60) | 0.90 | 65.08 (15.72) | 0.08 | −23.68(16.99) | 0.17 | −26% |
| Control | 90.01 (16.20) | 87.20 (16.93) | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nepper, M.J.; McAtee, J.R.; Wheeler, L.; Chai, W. Mobile Phone Text Message Intervention on Diabetes Self-Care Activities, Cardiovascular Disease Risk Awareness, and Food Choices among Type 2 Diabetes Patients. Nutrients 2019, 11, 1314. https://doi.org/10.3390/nu11061314
Nepper MJ, McAtee JR, Wheeler L, Chai W. Mobile Phone Text Message Intervention on Diabetes Self-Care Activities, Cardiovascular Disease Risk Awareness, and Food Choices among Type 2 Diabetes Patients. Nutrients. 2019; 11(6):1314. https://doi.org/10.3390/nu11061314
Chicago/Turabian StyleNepper, Martha J., Jennifer R. McAtee, Lorey Wheeler, and Weiwen Chai. 2019. "Mobile Phone Text Message Intervention on Diabetes Self-Care Activities, Cardiovascular Disease Risk Awareness, and Food Choices among Type 2 Diabetes Patients" Nutrients 11, no. 6: 1314. https://doi.org/10.3390/nu11061314
APA StyleNepper, M. J., McAtee, J. R., Wheeler, L., & Chai, W. (2019). Mobile Phone Text Message Intervention on Diabetes Self-Care Activities, Cardiovascular Disease Risk Awareness, and Food Choices among Type 2 Diabetes Patients. Nutrients, 11(6), 1314. https://doi.org/10.3390/nu11061314