Growth, Feeding Tolerance and Metabolism in Extreme Preterm Infants under an Exclusive Human Milk Diet

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Standardized Feeding Regimen and Study Groups
2.1.1. HMF Group
2.1.2. BMF Group
2.2. Outcome Measures
2.2.1. Parameters of Growth
2.2.2. Time to Full Enteral Feeding and Feeding Tolerance
2.2.3. Parameters of Glucose and Fat Metabolism
2.2.4. Morbidity
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics, Morbidity and Mortality
3.2. Primary and Secondary Outcomes
3.2.1. Growth
3.2.2. Time to full enteral feedings
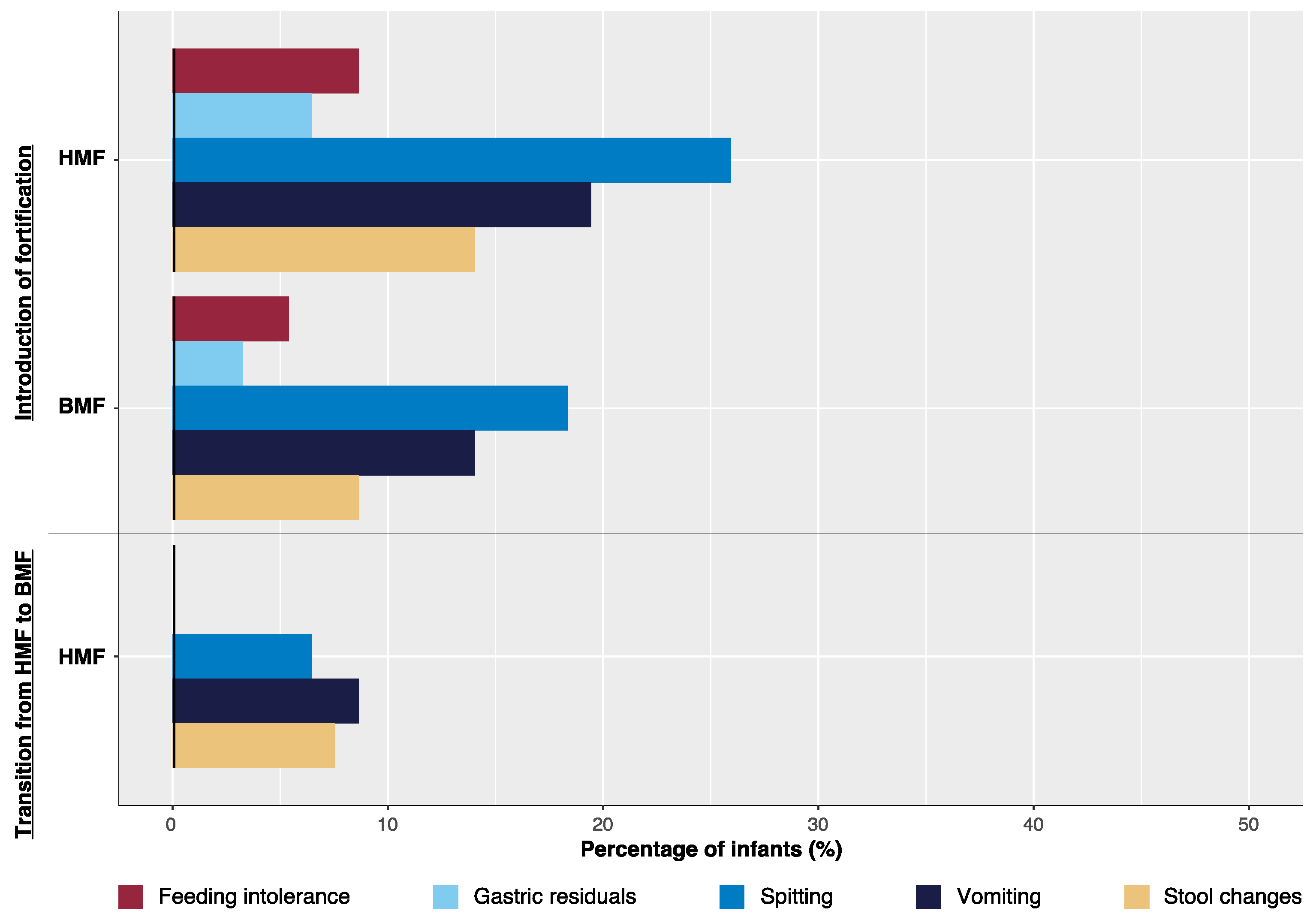
3.2.3. Fortifier Introduction and Transition from HMF to BMF Fortification
3.2.4. Transition of Fortifier
3.2.5. Parameters of Glucose and Fat Metabolism
3.2.6. Morbidity and Mortality
4. Discussion
4.1. Growth
4.2. Time to Full Enteral Feedings, Fortifier Introduction and Transition
4.3. Morbidity and Mortality
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Horbar, J.D.; Ehrenkranz, R.A.; Badger, G.J.; Edwards, E.M.; Morrow, K.A.; Soll, R.F.; Buzas, J.S.; Bertino, E.; Gagliardi, L.; Bellù, R.; et al. Weight Growth Velocity and Postnatal Growth Failure in Infants 501 to 1500 Grams: 2000–2013. Pediatrics 2015, 136, e84–e92. [Google Scholar] [CrossRef] [PubMed]
- Nutrition AAoPCo. Nutritional needs of Low-Birth-Weight Infants. Pediatrics 1977, 60, 519–530. [Google Scholar]
- Nutrition AAoPCo. Nutritional Needs of Low-Birth-Weight Infants. Pediatrics 1985, 75, 976–986. [Google Scholar]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [PubMed]
- Corpeleijn, W.E.; Kouwenhoven, S.M.; Paap, M.C.; Van Vliet, I.; Scheerder, I.; Muizer, Y.; Helder, O.K.; Van Goudoever, J.B.; Vermeulen, M.J. Intake of own mother’s milk during the first days of life is associated with decreased morbidity and mortality in very low birth weight infants during the first 60 days of life. Neonatology 2012, 102, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Kuschel, C.A.; Harding, J.E. Multicomponent fortified human milk for promoting growth in preterm infants. Cochrane Database Syst. Rev. 2004, CD000343. [Google Scholar] [CrossRef]
- Liu, T.T.; Dang, D.; Lv, X.M.; Wang, T.F.; Du, J.F.; Wu, H. Human milk fortifier with high versus standard protein content for promoting growth of preterm infants: A meta-analysis. J. Int. Med. Res. 2015, 43, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Young, L.; Embleton, N.D.; McCormick, F.M.; McGuire, W. Multinutrient fortification of human breast milk for preterm infants following hospital discharge. Cochrane Libr. 2013. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A.; Das, A.; Wrage, L.A.; Poindexter, B.B.; Higgins, R.D.; Stoll, B.J.; Oh, W. Early nutrition mediates the influence of severity of illness on extremely LBW infants. Pediatr. Res. 2011, 69, 522–529. [Google Scholar] [CrossRef]
- Sullivan, S.; Schanler, R.J.; Kim, J.H.; Patel, A.L.; Trawöger, R.; Kiechl-Kohlendorfer, U.; Chan, G.M.; Blanco, C.L.; Abrams, S.; Cotten, C.M.; et al. An Exclusively Human Milk-Based Diet Is Associated with a Lower Rate of Necrotizing Enterocolitis than a Diet of Human Milk and Bovine Milk-Based Products. J. Pediatr. 2009, 156, 562–567. [Google Scholar] [CrossRef]
- Assad, M.; Elliott, M.J.; Abraham, J.H. Decreased cost and improved feeding tolerance in VLBW infants fed an exclusive human milk diet. J. Perinatol. 2016, 36, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R.; Parenteral Nutrition Guidelines Working Group. 1. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J. Pediatr. Gastroenterol. Nutr. 2005, 41 (Suppl 2), S1–87. [Google Scholar] [PubMed]
- Tsang, U.; Zlotkin, K. Nutrition of the Preterm Infant-Scientific Basis and Practical Guidelines, 2nd ed.; Digital Educational Publishing Inc.: Cincinatti, OH, USA, 2005. [Google Scholar]
- Morgan, J.; Young, L.; McGuire, W. Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Huston, R.K.; Markell, A.M.; McCulley, E.A.; Gardiner, S.K.; Sweeney, S.L. Improving Growth for Infants ≤ 1250 Grams Receiving an Exclusive Human Milk Diet. Nutr. Clin. Pract. 2018, 33, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.L.; Engstrom, J.L.; Meier, P.P.; Kimura, R.E. Accuracy of methods for calculating postnatal growth velocity for extremely low birth weight infants. Pediatrics 2005, 116, 1466–1473. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC Pediatr. 2003, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.A.; Wilson, M.E. Feeding intolerance: A concept analysis. Adv. Neonatal Care 2011, 11, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Volpe, J. Neurology of the Newborn, 4th ed.; Saunders: Philadelphia, PA, USA, 2001. [Google Scholar]
- Kliegman, R.M.; Walsh, M.C. Neonatal necrotizing enterocolitis: Pathogenesis, classification, and spectrum of illness. Curr. Probl. Pediatr. 1987, 17, 213–288. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- De Vries, L.S.; Eken, P.; Dubowitz, L.M. The spectrum of leukomalacia using cranial ultrasound. Behav. Brain Res. 1992, 49, 1–6. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Donahue, L. Spontaneous intestinal perforation. Neonatal Netw. 2007, 26, 335–351. [Google Scholar] [CrossRef] [PubMed]
- Colacci, M.; Murthy, K.; DeRegnier, R.A.O.; Khan, J.Y.; Robinson, D.T. Growth and Development in Extremely Low Birth Weight Infants After the Introduction of Exclusive Human Milk Feedings. Am. J. Perinatol. 2017, 34, 130–137. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.L.; Kiss, A.; Tomlinson, C.; Bando, N.; Bayliss, A.; Campbell, D.M.; Daneman, A.; Francis, J.; Kotsopoulos, K.; Shah, P.S.; et al. Nutrient enrichment of human milk with human and bovine milk-based fortifiers for infants born weighing <1250 g: A randomized clinical trial. Am. J. Clin. Nutr. 2018, 108, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clin. Nutr. 2018, 37 Pt B, 2309–2314. [Google Scholar] [CrossRef]
- Hair, A.B.; Hawthorne, K.M.; Chetta, K.E.; Abrams, S.A. Human milk feeding supports adequate growth in infants ≤ 1250 grams birth weight. BMC Res. Notes 2013, 6, 459. [Google Scholar] [CrossRef]
- Lindquist, S.; Hernell, O. Lipid digestion and absorption in early life: An update. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 314–320. [Google Scholar] [CrossRef]
- Van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; de Pipaon, M.S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Decsi, T.; Domellöf, M.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin. Nutr. 2018, 37 Pt B, 2315–2323. [Google Scholar] [CrossRef] [Green Version]
- Cristofalo, E.A.; Schanler, R.J.; Blanco, C.L.; Sullivan, S.; Trawoeger, R.; Kiechl-Kohlendorfer, U.; Dudell, G.; Rechtman, D.J.; Lee, M.L.; Lucas, A.; et al. Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants. J. Pediatr. 2013, 163, 1592–1595. [Google Scholar] [CrossRef]
- Hair, A.B.; Rechtman, D.J.; Lee, M.L.; Niklas, V. Beyond Necrotizing Enterocolitis: Other Clinical Advantages of an Exclusive Human Milk Diet. Breastfeed. Med. 2018, 13, 408–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, A.B.; Blanco, C.L.; Moreira, A.G.; Hawthorne, K.M.; Lee, M.L.; Rechtman, D.J.; Abrams, S.A. Randomized trial of human milk cream as a supplement to standard fortification of an exclusive human milk-based diet in infants 750–1250 g birth weight. J. Pediatr. 2014, 165, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Chee, Y.Y.; Wong, M.S.; Wong, R.M.; Wong, K.Y. Neonatal outcomes of preterm or very-low-birth-weight infants over a decade from Queen Mary Hospital, Hong Kong: Comparison with the Vermont Oxford Network. Hong Kong Med. J. 2017, 23, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Hair, A.B.; Peluso, A.M.; Hawthorne, K.M.; Perez, J.; Smith, D.P.; Khan, J.Y.; O’Donnell, A.; Powers, R.J.; Lee, M.L.; Abrams, S.A.; et al. Beyond Necrotizing Enterocolitis Prevention: Improving Outcomes with an Exclusive Human Milk-Based Diet. Breastfeed. Med. 2016, 11, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Jasani, B.; Patole, S. Standardized feeding regimen for reducing necrotizing enterocolitis in preterm infants: An updated systematic review. J. Perinatol. 2017, 37, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Rozé, J.C.; Ancel, P.Y.; Lepage, P.; Martin-Marchand, L.; Al Nabhani, Z.; Delannoy, J.; Picaud, J.C.; Lapillonne, A.; Aires, J.; Durox, M.; et al. Nutritional strategies and gut microbiota composition as risk factors for necrotizing enterocolitis in very-preterm infants. Am. J. Clin. Nutr. 2017, 106, 821–830. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Macronutrient | ESPGHAN Recommendations | HM (100 mL) | HM + HMF (100 mL) | HM + BMF (100 mL) |
| Energy (kcal) | 110–135/kg/day | 70 | 91 | 85.27 |
| Protein (g) | 4.0–4.5/kg/day | 1.81 | 3.07 | 2.92 |
| Fat (g) | 4.8–6.6/kg/day | 4.0 | 5.5 | 4.0 |
| Carbohydrates (g) | - | 6.95 | 7.63 | 9.69 |
| Macronutrient-Energy-Ratio | ESPGHAN Recommendations | HM (100 kcal) | HM + HMF (100 kcal) | HM + BMF (100 kcal) |
| Protein-energy-ratio (g/100 kcal) | 3.6–4.1 | 2.59 | 3.37 | 3.42 |
| Carbohydrate-energy-ratio (g/100 kcal) | 10.5–12.0 | 9.9 | 8.4 | 11.4 |
| Lipid-energy-ratio (g/100kcal) | 4.4–6.0 | 5.7 | 6.0 | 4.7 |
| Variable | HMF Group (n = 96) | BMF Group (n = 96) | p-Value |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| Gestational age (weeks + days) | 26+1 (24+6, 27+1) | 25+6 (24+5, 27+3) | n.s. |
| Birth weight (g) | 752 (659, 893) | 773 (650, 890) | n.s. |
| Birth weight (zscore) | −0.3 (−1.1, 0.3) | −0.4 (−1.2, 0.2) | n.s. |
| Birth length (cm) | 32.8 (30.9, 34.5) | 33.0 (31.0, 35.0) | n.s. |
| Birth length (zscore) | −0.6 (−1.4, 0.0) | −0.5 (−1.4, 0.1) | n.s. |
| Birth head circumference (cm) | 23.5 (22.3, 24.5) | 23.5 (22.5, 24.5) | n.s. |
| Birth head circumference (zscore) | −0.3 (−1.1, 0.3) | −0.2 (−1.1, 0.3) | n.s. |
| Apgar-Score 5 min | 8 (8, 9) | 8 (8, 9) | n.s. |
| Apgar-Score 10 min | 9 (9, 9) | 9 (9, 9) | n.s. |
| Arterial umbilical cord pH | 7.3 (7.2, 7.3) | 7.3 (7.2, 7.4) | n.s. |
| n (%) | n (%) | ||
| Small for gestational age | 21 (22%) | 15 (16%) | n.s. |
| Male | 45 (47%) | 42 (44%) | n.s. |
| Multiple births | 24 (25%) | 36 (38%) | n.s. |
| Sectio caesearea | 80 (83%) | 82 (85%) | n.s. |
| Lung maturation | 89 (93%) | 90 (94%) | n.s. |
| Lung maturation complete | 71 (74%) | 69 (72%) | n.s. |
| Premature rupture of membranes | 38 (40%) | 22 (23%) | <0.05 |
| Preeclampsia/Eclampsia | 11 (11%) | 9 (9%) | n.s. |
| Variable | HMF Group (n = 96) | BMF Group (n = 96) | p-Value |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| Hierarchical structure of endpoints | |||
| Growth velocity (g/kg/d) birth to 37+0 weeks | 15.2 (14.2, 16.7) | 15.6 (13.9, 16.7) | n.s. |
| Growth velocity (g/kg/d) fortifier introduction to 32+0 weeks | 16.5 (14.5, 19.1) | 18.9 (15.3, 21.3) | 0.009 |
| Growth velocity (g/kg/d) birth to fortifier introduction | 13.5 (7.4, 16.8) | 10.7 (4.8, 15.3) | 0.09 |
| Growth velocity (g/kg/d) birth to 32+0 weeks | 15.3 (14.0, 17.7) | 15.1 (13.6, 17.0) | n.s. |
| Growth velocity (g/kg/d) 32+0 to 37+0 weeks | 15.5 (13.2, 17.2) | 15.9 (13.9, 17.7) | n.s. |
| 32+0 weeks of gestational age | |||
| weight (g) | 1442 (1267, 1580) | 1430 (1240, 1598) | n.s. |
| weight (zscore) | −1.0 (−1.5, −0.7) | −1.1 (−1.5, −0.6) | n.s. |
| length increase (cm/week) | 1.0 (0.7, 1.3) | 0.9 (0.6, 1.3) | n.s. |
| length (cm) | 38.0 (36.0, 39.4) | 38.0 (36.7, 39.5) | n.s. |
| length (zscore) | −2.1 (−2.9, −1.5) | −2.1 (−2.6, −1.5) | n.s. |
| head circumference increase (cm/week) | 0.6 (0.4, 0.8) | 0.6 (0.4, 0.8) | n.s. |
| head circumference (cm) | 26.5 (25.3, 27.5) | 26.6 (25.5, 27.5) | n.s. |
| head circumference (zscore) | −2.0 (−2.8, −1.5) | −2.0 (−2.0, −1.4) | n.s. |
| 37+0 weeks of gestational age | |||
| weight (g) | 2500 (2136, 2722) | 2427 (2155, 2722) | n.s. |
| weight (zscore) | −1.0 (−1.8, −0.6) | −1.2 (−1.8, −0.6) | n.s. |
| length gain (cm/week) | 1.1 (1.0, 1.3) | 1.1 (0.9, 1.2) | n.s. |
| length (cm) | 44.0 (43.0, 45.5) | 44.5 (43.0, 46.0) | n.s. |
| length (zscore) | −1.9 (−2.3, −1.2) | −1.7 (−2.3, −1.0) | n.s. |
| head circumference gain (cm/week) | 0.8 (0.7, 0.9) | 0.8 (0.7, 0.8) | n.s. |
| head circumference (cm) | 31.2 (30.0, 32.0) | 31.5 (30.5, 32.5) | n.s. |
| head circumference (zscore) | −1.3 (−2.0, −0.9) | −1.2 (−1.7, −0.6) | n.s. |
| Variable | HMF Group (n = 96) | BMF Group (n = 96) | p-Value |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| Time to full enteral feedings (days) | 26 (19, 38) | 20 (14, 32) | 0.0018 |
| Parenteral Nutrition (days) | 28 (19, 44) | 22 (15, 40) | 0.01 |
| Central line (days) | 30 (20, 49) | 24 (15, 45) | 0.01 |
| Fortifier days up to 32+0 weeks | 20 (8, 28) | 19 (10, 30) | n.s. |
| Fortifier days up to 37+0 weeks | 48 (35, 59) | 45 (31, 57) | n.s. |
| n (%) | n (%) | p-value | |
| Enteral nutrition up to 32+0 weeks | |||
| - HM + Fortifier | 84 (88%) | 89 (93%) | n.s. |
| - deceased | 3 (3%) | 3 (3%) | n.s. |
| Enteral nutrition at 37+0 weeks | |||
| - HM | 5 (5%) | 0 (0%) | n.s. |
| - HM + BMF | 39 (41%) | 38 (39.5%) | n.s. |
| - Formula | 36 (38%) | 37 (38.5%) | n.s. |
| - Mixed | 13 (14%) | 18 (19%) | n.s. |
| HMF Group n (%) | BMF Group n (%) | p-Value | ||
|---|---|---|---|---|
| Present study *1 | Feeding intolerance | 8 (8%) | 5 (5%) | n.s. |
| Gastric residuals | 6 (6%) | 3 (3%) | n.s. | |
| Interruption | 22 (21%) | 18 (19%) | n.s. | |
| O’Connor et al. [27] *2 | Feeding intolerance | 9 (14.4%) | 0 (0%) | n.s. |
| Gastric residuals | 26 (40.6%) | 25 (41.1%) | n.s. | |
| Interruption | 17 (26.6%) | 20 (32.8%) | n.s. |
| Variable | HMF Group (n = 96) n (%) | BMF Group (n = 96) n (%) | p-Value |
|---|---|---|---|
| Mortality | 5 (5%) | 3 (3%) | n.s. |
| IVH | 26 (27%) | 23 (24%) | n.s. |
| - I and II | 13 (14%) | 15 (16%) | |
| - III and IV | 13 (14%) | 8 (8%) | |
| PVL | 3 (4%) | 1 (1%) | n.s. |
| Sepsis | 45 (47%) | 41 (43%) | n.s. |
| PDA | 58 (60%) | 56 (58%) | n.s. |
| - Ligature | 4 (4%) | 5 (5%) | |
| BPD | 29 (30%) | 23 (23%) | n.s. |
| ROP | 53 (55%) | 45 (47%) | n.s. |
| - I-III | 53 (55%) | 43 (45%) | |
| - III+ | 0 (0%) | 2 (2%) | |
| NEC | 10 (10%) | 8 (8%) | n.s. |
| - Abdominal surgery | 7 (7%) | 7 (7%) | n.s. |
| FIP | 5 (5%) | 5 (5%) | n.s. |
| Study | HMF Group | BMF Group | p- Value | Method | Timeframe |
|---|---|---|---|---|---|
| Present study | n = 96 | n = 96 | n.s. | Patel | Birth to 37+0 |
| BW, median (IQR) | 752 (659, 893) | 773 (650, 890) | |||
| GV, median (IQR) | 15.2 (14.2, 16.7) | 15.6 (13.9, 16.7) | |||
| Sullivan et al. [11] | n = 67 | n = 69 | n.s. | Daily weights | *1 |
| BW, mean (SD) | 14.2 (11.9, 15.8) | 15.1 (12.8, 17.0) | |||
| GV, median (IQR) | 945 (± 202) | 922 (± 197) | |||
| Colacci et al. [26] | n = 39 | n = 46 | n.s. | Patel | Birth to discharge |
| BW, mean (SD) | 783 (± 143) | 770 (± 137) | |||
| GV, mean (SD) | 13.1 (± 4.0) | 12.1 (± 5.2) | |||
| Hair et al. 2013 [29] | n = 104 | - | - | Daily weights | Birth to discharge |
| BW, mean (SD) | 913 (±182) | ||||
| GV, mean (SD) | 24.8 (± 5.4) | ||||
| Huston et al. [16] *2 | n = 94 | n = 111 | - | Patel | Birth to discharge |
| BW, mean (SD) | 904 (± 200) | 959 (±174) | |||
| GV, mean (SD) | 13.6 (± 1.6) | 14.1 (± 1.8) | |||
| Assad et al. [12] | n = 87 | n = 127 | n.s. | Two-point average | Birth to discharge |
| BW, range | 490–1700 g | 490–1700 g | |||
| GV, mean (SD) | 11.6 (± 2.7) | 11.6 (± 2.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eibensteiner, F.; Auer-Hackenberg, L.; Jilma, B.; Thanhaeuser, M.; Wald, M.; Haiden, N. Growth, Feeding Tolerance and Metabolism in Extreme Preterm Infants under an Exclusive Human Milk Diet. Nutrients 2019, 11, 1443. https://doi.org/10.3390/nu11071443
Eibensteiner F, Auer-Hackenberg L, Jilma B, Thanhaeuser M, Wald M, Haiden N. Growth, Feeding Tolerance and Metabolism in Extreme Preterm Infants under an Exclusive Human Milk Diet. Nutrients. 2019; 11(7):1443. https://doi.org/10.3390/nu11071443
Chicago/Turabian StyleEibensteiner, Fabian, Lorenz Auer-Hackenberg, Bernd Jilma, Margarita Thanhaeuser, Martin Wald, and Nadja Haiden. 2019. "Growth, Feeding Tolerance and Metabolism in Extreme Preterm Infants under an Exclusive Human Milk Diet" Nutrients 11, no. 7: 1443. https://doi.org/10.3390/nu11071443
APA StyleEibensteiner, F., Auer-Hackenberg, L., Jilma, B., Thanhaeuser, M., Wald, M., & Haiden, N. (2019). Growth, Feeding Tolerance and Metabolism in Extreme Preterm Infants under an Exclusive Human Milk Diet. Nutrients, 11(7), 1443. https://doi.org/10.3390/nu11071443