Osmolality of Commercially Available Oral Rehydration Solutions: Impact of Brand, Storage Time, and Temperature


Abstract
:1. Introduction
2. Materials and Methods
2.1. Drink and Drink Preparations
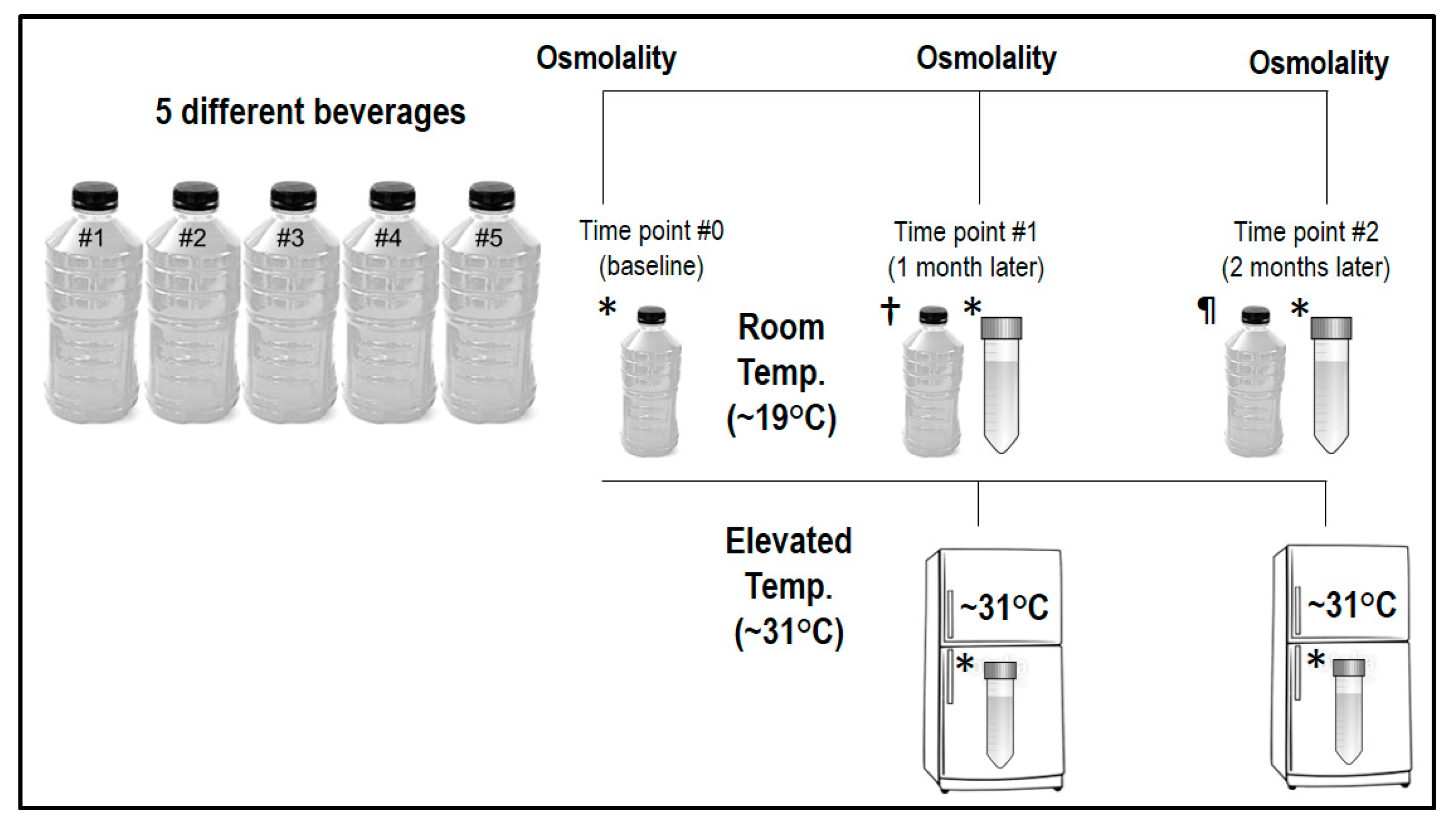
2.2. Study Overview
2.3. Osmometry
2.4. Water Content
2.5. Statistics and Data Presentation
3. Results
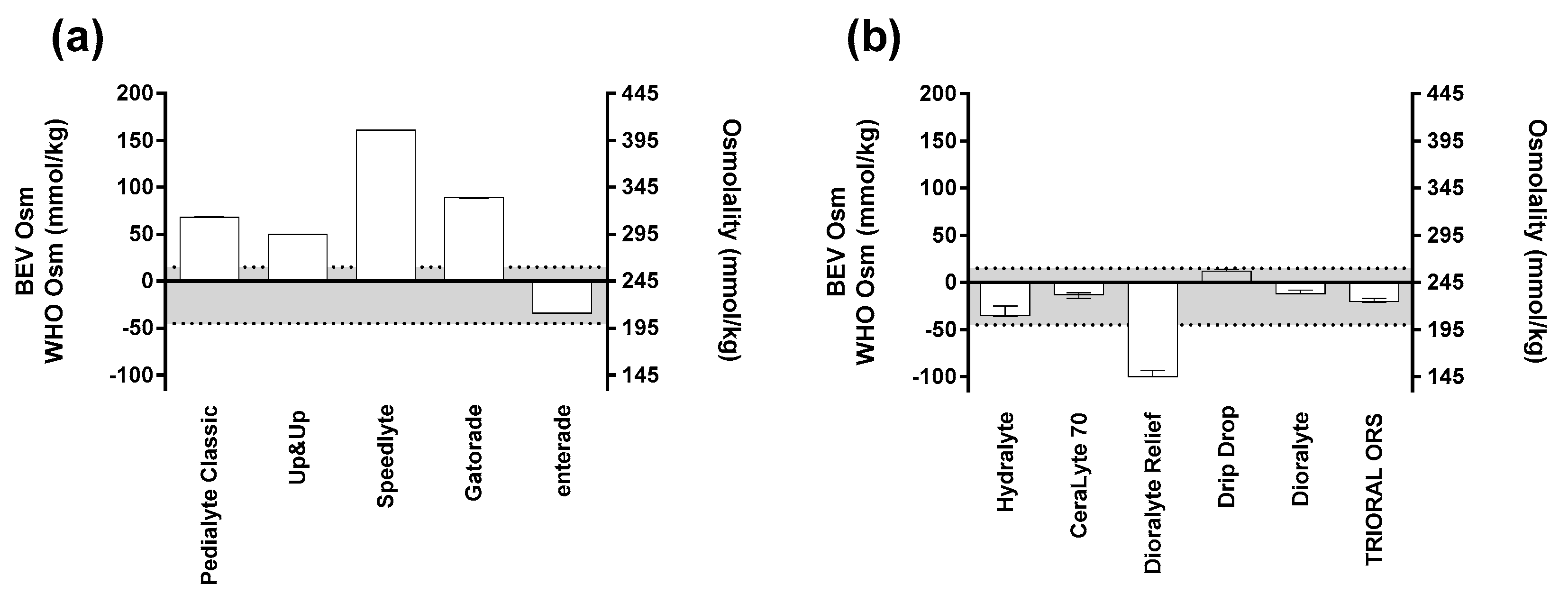
3.1. Pre-Mixed ORS Variability
3.2. Powdered ORS Variability
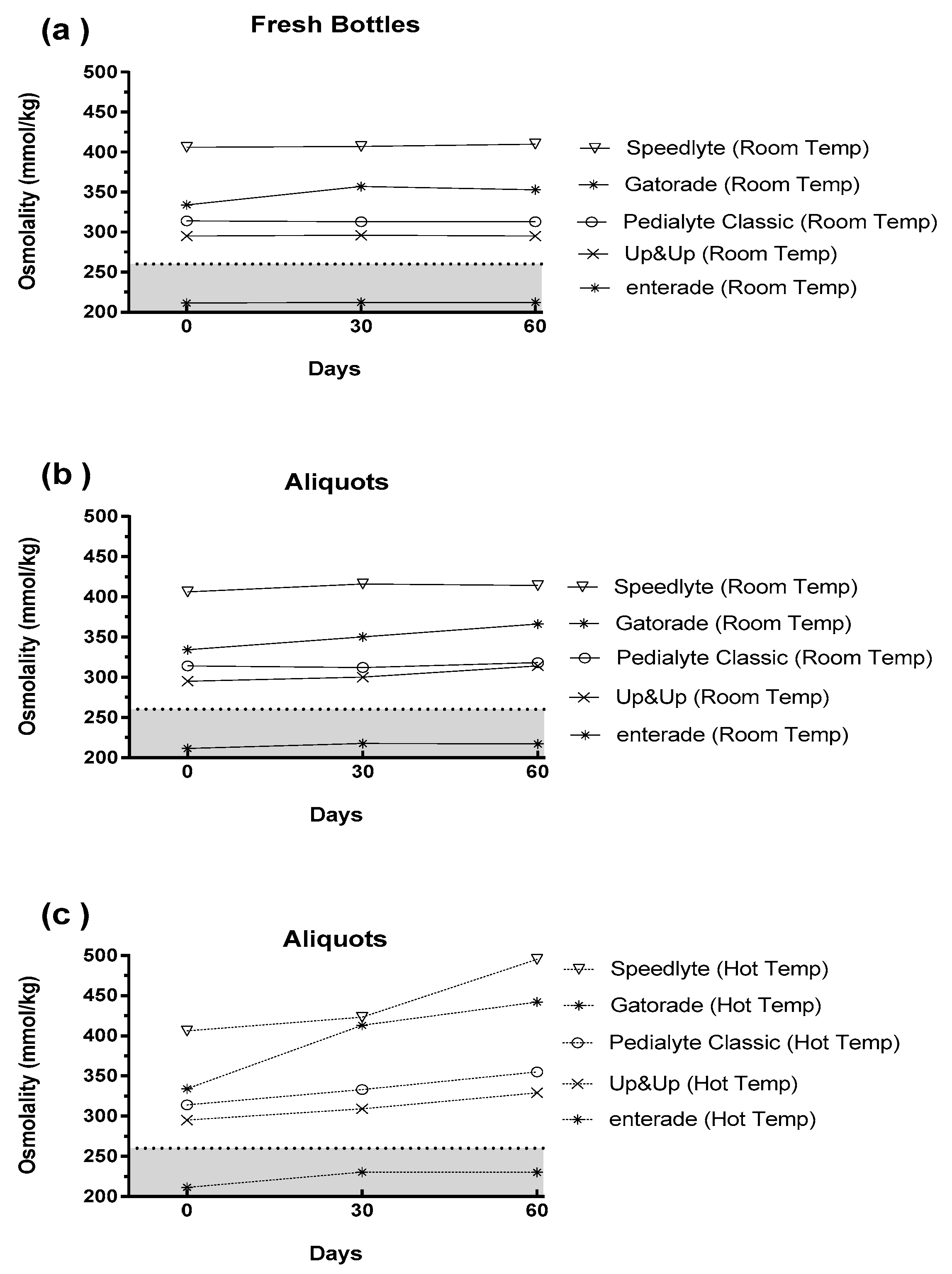
3.3. Impact of Time and Temperature
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Beverage Name | Ingredients |
|---|---|
| Pedialyte® Classic mixed (fruit flavor) | Water, Dextrose. Less than 2% of: Citric Acid, Natural & Artificial Flavor, Potassium Citrate, Salt, Sodium Citrate, Sucralose, Acesulfame Potassium, Zinc Gluconate, and Yellow 6. |
| Pediatric Oral Electrolyte Solution (fruit flavor) | Water, Dextrose, Citric Acid, Potassium Citrate, Sodium Chloride, Sodium Citrate, Acesulfame Potassium, Zinc Gluconate, Natural & Artificial Fruit Flavor, Sucralose, FD&C Yellow #6. |
| Speedlyte® (wild orange flavor) | Purified water; Less than 2% of: Dextrose, Sucrose, Liposomal Salt [Citrate, Chloride, Sodium, Potassium, Soy Lecithin, Xanthan Gum], Citric Acid, Sodium Benzoate, Stevia Extract, Monk Fruit, Beta Carotene, Rose Anthocyanin, Methylparaben, Sodium Metabisulfite, Natural Flavor. |
| enterade®AD ORS (orange flavor) | Water, Amino Acid Blend (L-Valine, L-Aspartic Acid, L-Serine, L-Isoleucine, L-Threonine, L-Lysine, L-Glycine, L-Tyrosine), sodium chloride, potassium citrate, trisodium citrate, natural flavor, magnesium citrate, calcium chloride, stevia. |
| Gatorade® (orange flavor) | Water, Sugar, Dextrose, Citric Acid, Salt, Sodium Citrate, Monopotassium Phosphate, Gum Arabic, Natural Flavor, Sucrose Acetate Isobutyrate, Glycerol Ester of Rosin, Yellow 6 |
References
- King, C.K.; Glass, R.; Bresee, J.S.; Duggan, C. Managing acute gastroenteritis among children: Oral rehydration, maintenance, and nutritional therapy. MMWR. Recomm. Rep. 2003, 52, 1–16. [Google Scholar] [PubMed]
- Kosek, M.; Bern, C.; Guerrant, R.L. The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bull. World Health Organ. 2003, 81, 197–204. [Google Scholar] [PubMed]
- Farthing, M.J. Oral rehydration: An evolving solution. J. Pediatr. Gastroenterol. Nutr. 2002, 34 (Suppl. 1), S64–67. [Google Scholar] [CrossRef] [PubMed]
- Nalin, D.R.; Cash, R.A. 50 years of oral rehydration therapy: The solution is still simple. Lancet 2018, 392, 536–538. [Google Scholar] [CrossRef]
- Hirschhorn, N. The treatment of acute diarrhea in children. An historical and physiological perspective. Am. J. Clin. Nutr. 1980, 33, 637–663. [Google Scholar] [CrossRef] [Green Version]
- Banks, M.R.; Farthing, M.J. Fluid and electrolyte transport in the small intestine. Curr. Opin. Gastroenterol. 2002, 18, 176–181. [Google Scholar] [CrossRef]
- Crane, R.K. Hypothesis for mechanism of intestinal active transport of sugars. Fed. Proc. 1962, 21, 891–895. [Google Scholar]
- Curran, P.F. Coupling between transport processes in intestine. Physiologist 1968, 11, 3–23. [Google Scholar]
- Fordtran, J.S.; Rector, F.C., Jr.; Carter, N.W. The mechanisms of sodium absorption in the human small intestine. J. Clin. Invest. 1968, 47, 884–900. [Google Scholar] [CrossRef] [Green Version]
- Schultz, S.G.; Zalusky, R. Ion transport in isolated rabbit ileum. I. Short-circuit current and Na fluxes. J. Gen. Physiol. 1964, 47, 567–584. [Google Scholar] [CrossRef]
- Schultz, S.G.; Zalusky, R. Ion transport in isolated rabbit ileum. II. The interaction between active sodium and active sugar transport. J. Gen. Physiol. 1964, 47, 1043–1059. [Google Scholar] [CrossRef] [PubMed]
- Atia, A.N.; Buchman, A.L. Oral rehydration solutions in non-cholera diarrhea: A review. Am. J. Gastroenterol. 2009, 104, 2596–2604, quiz 2605. [Google Scholar] [CrossRef] [PubMed]
- Impact of glycine-containing ORS solutions on stool output and duration of diarrhoea: A meta-analysis of seven clinical trials. The International Study Group on Improved ORS. Bull. World Health Organ. 1991, 69, 541–548.
- Duggan, C.; Fontaine, O.; Pierce, N.F.; Glass, R.I.; Mahalanabis, D.; Alam, N.H.; Bhan, M.K.; Santosham, M. Scientific rationale for a change in the composition of oral rehydration solution. JAMA 2004, 291, 2628–2631. [Google Scholar] [CrossRef] [PubMed]
- WHO. Reduced Osmolarity Oral Rehydration Salts (ORS) Formulation: A Report from a Meeting of Expert Jointly Organised by UNICEF and WHO: UNICEF House, New York, USA, July 18, 2001. Available online: https://apps.who.int/iris/handle/10665/67322 (accessed on 7 April 2019).
- Leiper, J.B. Fate of ingested fluids: Factors affecting gastric emptying and intestinal absorption of beverages in humans. Nutr. Rev. 2015, 73 Suppl. 2, 57–72. [Google Scholar] [CrossRef]
- Izgu, E.; Baykara, T. The solid state stability of oral rehydration salts. J. Clin. Hosp. Pharm. 1981, 6, 135–144. [Google Scholar] [CrossRef] [PubMed]
- WHO. Climate Change and Human Health: Risk and Responses; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Mora, C.; Dousset, B.; Caldwell, I.R.; Powell, F.E.; Geronimo, R.C.; Bielecki, C.R.; Counsell, C.W.; Dietrich, B.S.; Johnston, E.T.; Louis, L.V.; et al. Global risk of deadly heat. Nat. Clim. Chang. 2017, 7, 501. [Google Scholar] [CrossRef]
- Goldberg, R.N.; Tewari, Y.B.; Ahluwalia, J.C. Thermodynamics of the hydrolysis of sucrose. J. Bio. Chem. 1989, 264, 9901–9904. [Google Scholar]
- Pantenburg, B.; Ochoa, T.J.; Ecker, L.; Ruiz, J. Use of Commercially Available Oral Rehydration Solutions in Lima, Peru. Am. J. Trop. Med. Hyg. 2012, 86, 922–924. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.S.; Summers, R.W.; Rao, G.R.; Ramana, S.; Devi, U.; Zimmerman, B.; Pratap, B.C. Oral rehydration for viral gastroenteritis in adults: A randomized, controlled trial of 3 solutions. JPEN J. Parenter. Enteral. Nutr. 2006, 30, 433–439. [Google Scholar] [CrossRef]
- Sollanek, K.J.; Kenefick, R.W.; Cheuvront, S.N. Importance of sample volume to the measurement and interpretation of plasma osmolality. J. Clin. Lab. Anal. 2019, 33, e22727. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Kenefick, R.W.; Heavens, K.R.; Spitz, M.G. A comparison of whole blood and plasma osmolality and osmolarity. J. Clin. Lab. Anal. 2014, 28, 368–373. [Google Scholar] [CrossRef]
- Bohnen, N.; Terwel, D.; Markerink, M.; Ten Haaf, J.A.; Jolles, J. Pitfalls in the measurement of plasma osmolality pertinent to research in vasopressin and water metabolism. Clin. Chem. 1992, 38, 2278–2280. [Google Scholar]
- Plaisier, A.; Maingay-de Groof, F.; Mast-Harwig, R.; Kalkman, P.M.; Wulkan, R.W.; Verwers, R.; Neele, M.; Hop, W.C.; Groeneweg, M. Plasma water as a diagnostic tool in the assessment of dehydration in children with acute gastroenteritis. Eur. J. Pediatr. 2010, 169, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Eisenman, A.J.; Mackenzie, L.B.; Peters, J.P. Protein and water of serum and cells of human blood, with a note on the measurement of red blood cell volume. J. Biol. Chem. 1936, 116, 33–45. [Google Scholar]
- Al-Ramahi, R.; Zaid, A.; Hussein, A.; Yaseen, A.; Abdallah, K.; Odeh, M. Evaluation of mothers’ practice in the treatment of children diarrhea and measurement of the osmolality and PH of some oral rehydration solutions and carbonated beverages. An-Najah Univ. J. Res. (N. Sc.) 2016, 30, 269–282. [Google Scholar]
- Mettler, S.; Rusch, C.; Colombani, P.C. Osmolality and pH of sport and other drinks available in Switzerland. Schweiz. Z. Med. Traumatol. 2006, 54, 92. [Google Scholar]
- Wesley, J.F. Osmolality—A novel and sensitive tool for detection of tampering of beverages adulterated with ethanol, γ-butyrolactone, and 1,4-butanediol, and for detection of dilution-tampered demerol syringes. Microgram J. 2003, 8–17. [Google Scholar]
- Clarke, M.A. Technological value of sucrose in food products. In Sucrose: Properties and Applications; Mathlouthi, M., Reiser, P., Eds.; Springer: Boston, MA, USA, 1995. [Google Scholar]
- Hofman, D.L.; van Buul, V.J.; Brouns, F.J. Nutrition, Health, and Regulatory Aspects of Digestible Maltodextrins. Crit. Rev. Food Sci. Nutr. 2016, 56, 2091–2100. [Google Scholar] [CrossRef] [PubMed]
- Nicastro, A.; Barbarini, A.L.; Souss, G.M. Liposomal Rehydration Salt Formulation and Associated Method of Use. U.S. Patent 15/797,031, 22 February 2018. [Google Scholar]
- Yin, L.; Gupta, R.; Vaught, L.; Grosche, A.; Okunieff, P.; Vidyasagar, S. An amino acid-based oral rehydration solution (AA-ORS) enhanced intestinal epithelial proliferation in mice exposed to radiation. Sci. Rep. 2016, 6, 37220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.; Vijaygopal, P.; MacGregor, G.G.; Menon, R.; Ranganathan, P.; Prabhakaran, S.; Zhang, L.; Zhang, M.; Binder, H.J.; Okunieff, P.; et al. Glucose stimulates calcium-activated chloride secretion in small intestinal cells. Am. J. Physiol. Cell Physiol. 2014, 306, C687–C696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.; Menon, R.; Gupta, R.; Vaught, L.; Okunieff, P.; Vidyasagar, S. Glucose enhances rotavirus enterotoxin-induced intestinal chloride secretion. Pflugers Arch. 2017, 469, 1093–1105. [Google Scholar] [CrossRef] [PubMed]
- Hodges, K.; Gill, R. Infectious diarrhea: Cellular and molecular mechanisms. Gut Microbes 2010, 1, 4–21. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sollanek, K.J.; Kenefick, R.W.; Cheuvront, S.N. Osmolality of Commercially Available Oral Rehydration Solutions: Impact of Brand, Storage Time, and Temperature. Nutrients 2019, 11, 1485. https://doi.org/10.3390/nu11071485
Sollanek KJ, Kenefick RW, Cheuvront SN. Osmolality of Commercially Available Oral Rehydration Solutions: Impact of Brand, Storage Time, and Temperature. Nutrients. 2019; 11(7):1485. https://doi.org/10.3390/nu11071485
Chicago/Turabian StyleSollanek, Kurt J., Robert W. Kenefick, and Samuel N. Cheuvront. 2019. "Osmolality of Commercially Available Oral Rehydration Solutions: Impact of Brand, Storage Time, and Temperature" Nutrients 11, no. 7: 1485. https://doi.org/10.3390/nu11071485
APA StyleSollanek, K. J., Kenefick, R. W., & Cheuvront, S. N. (2019). Osmolality of Commercially Available Oral Rehydration Solutions: Impact of Brand, Storage Time, and Temperature. Nutrients, 11(7), 1485. https://doi.org/10.3390/nu11071485