Food and Nutrient Intake during Pregnancy in Relation to Maternal Characteristics: Results from the NICE Birth Cohort in Northern Sweden

 and
and
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Dietary Assessment
2.3. Food Intake
2.4. Intake of Nutrients
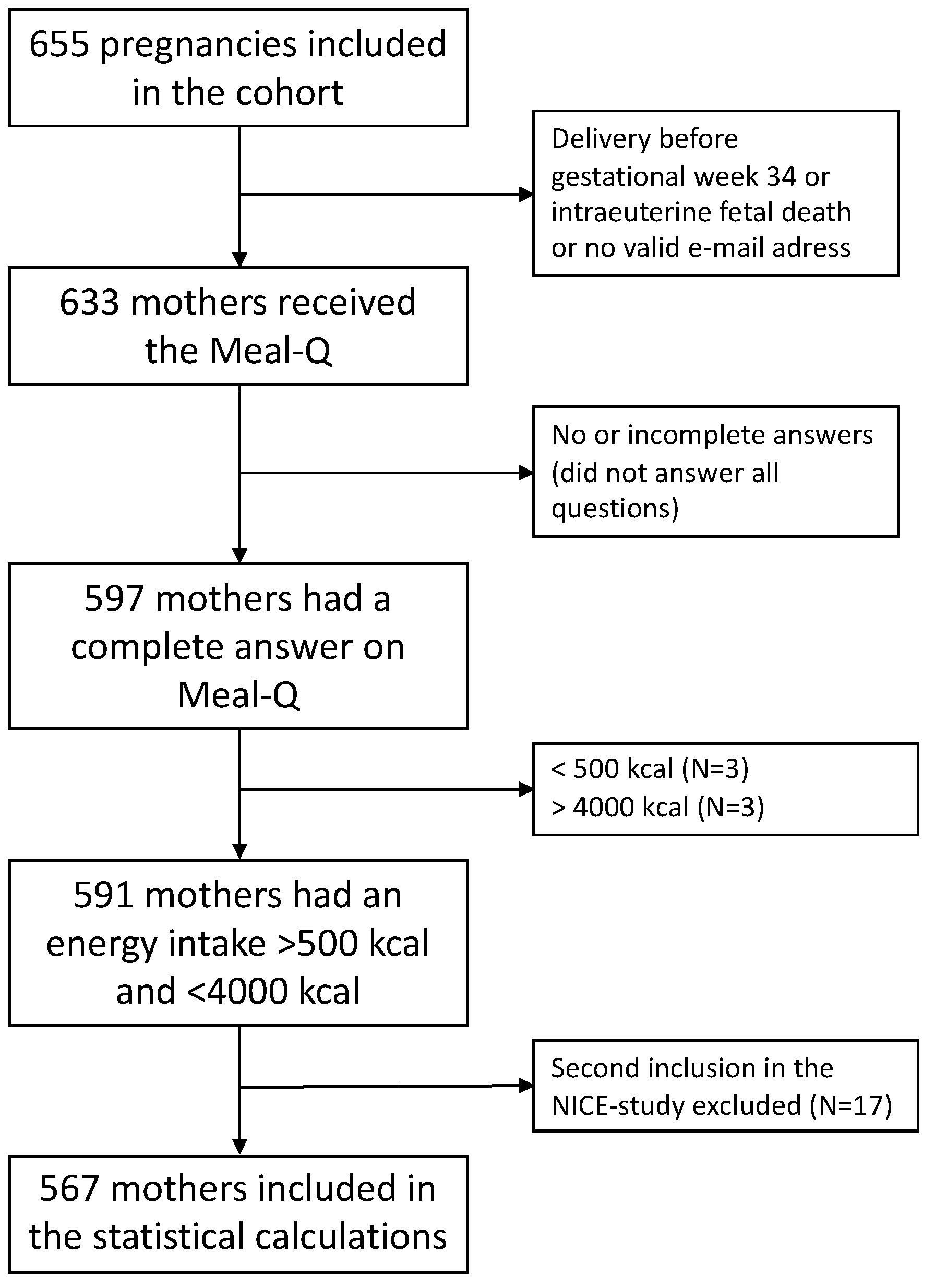
2.5. Inclusion and Exclusion Criteria for the Dietary Study
2.6. Maternal Characteristics
2.7. Data Analysis
3. Results
3.1. Characteristics
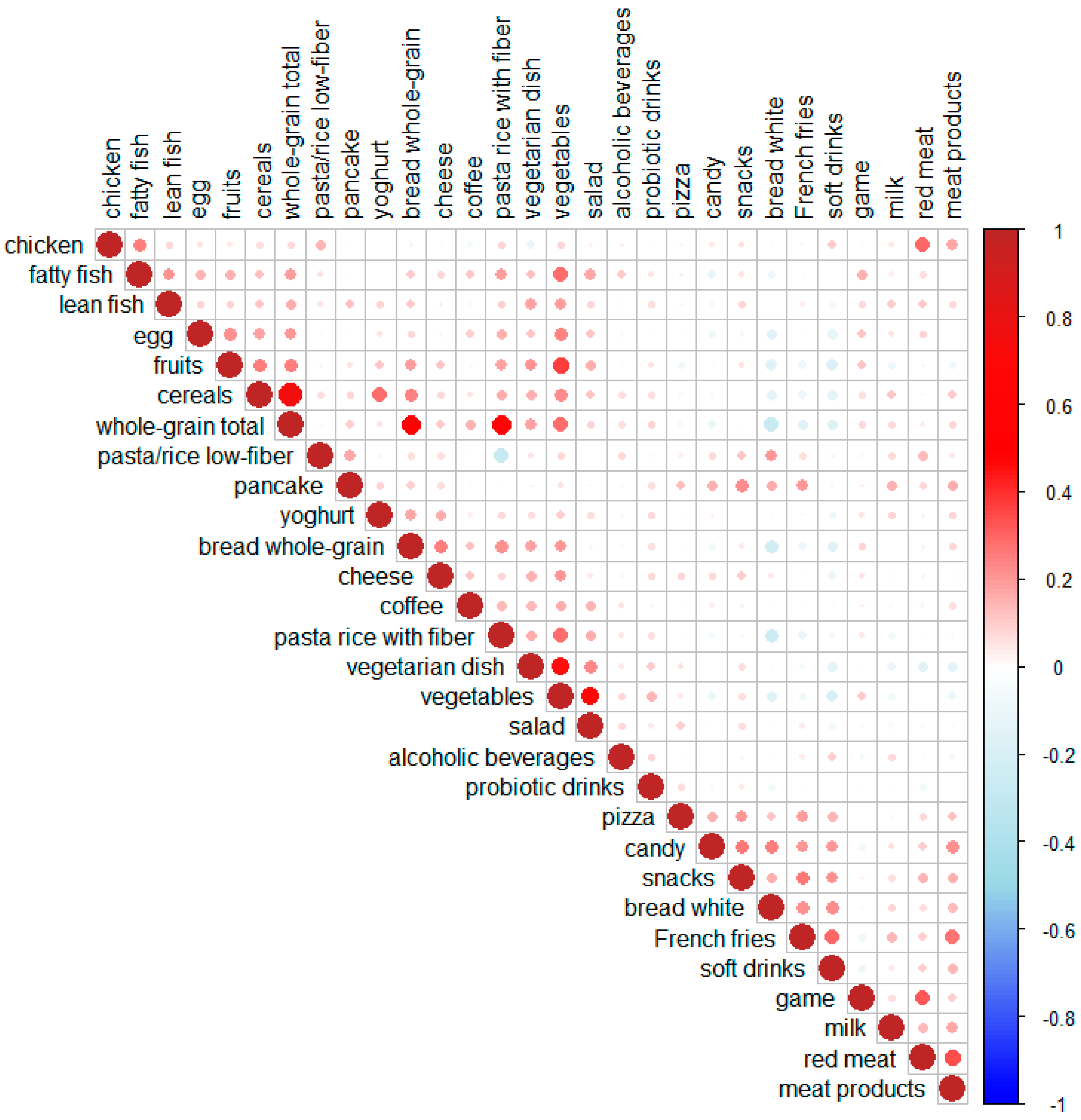
3.2. Food and Beverage Intakes
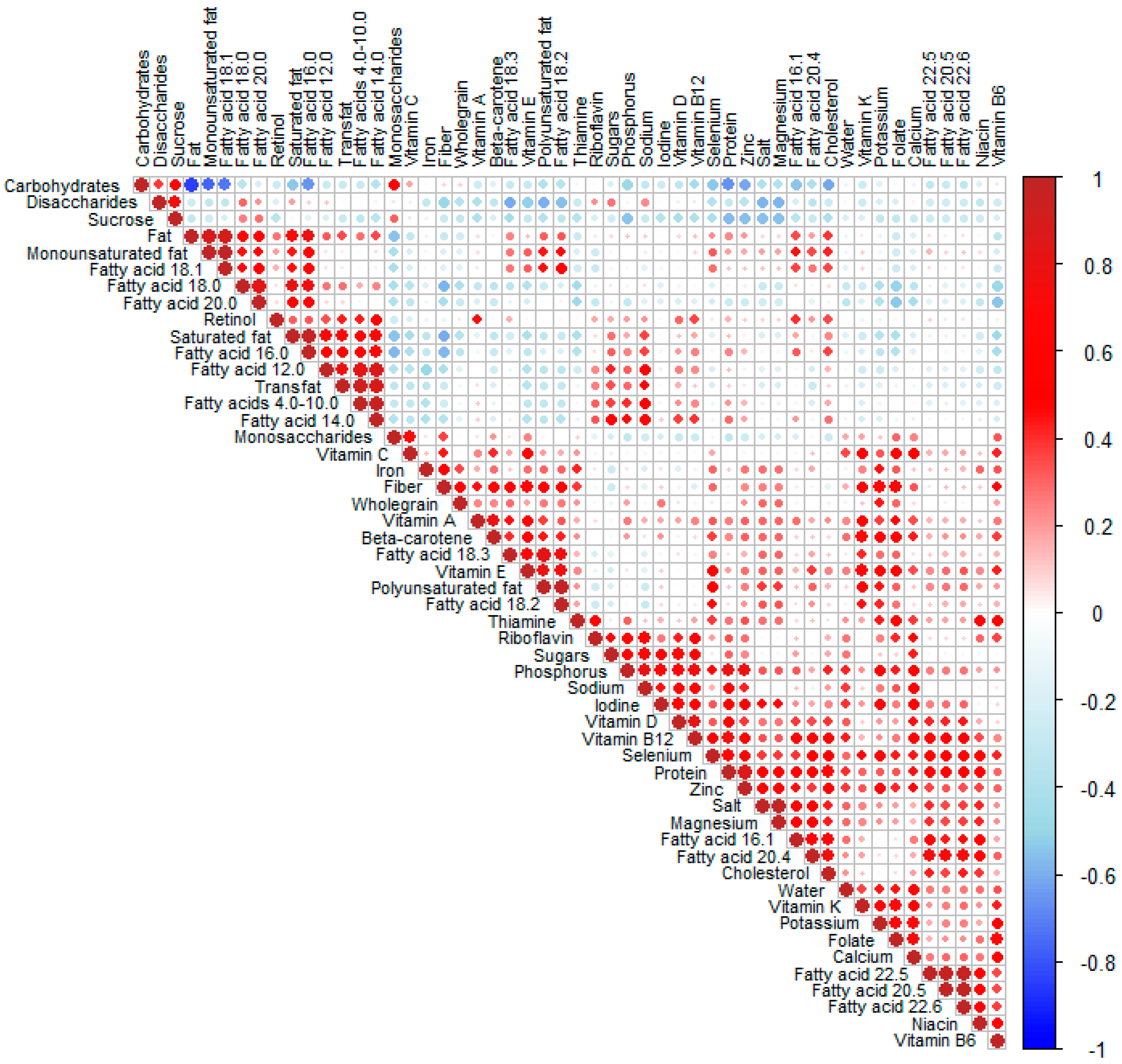
3.3. Intake of Macronutrients
3.4. Intake of Micronutrients
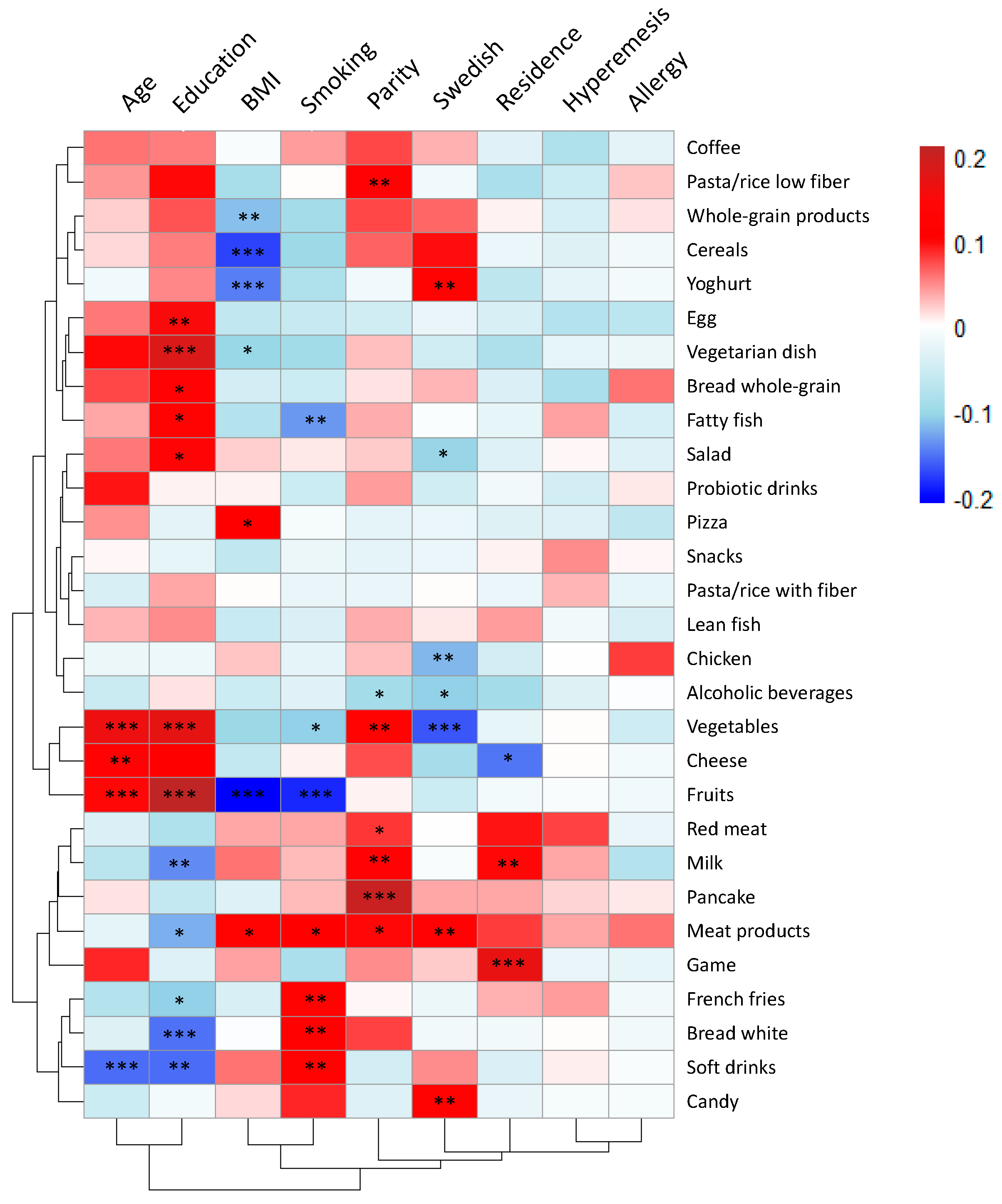
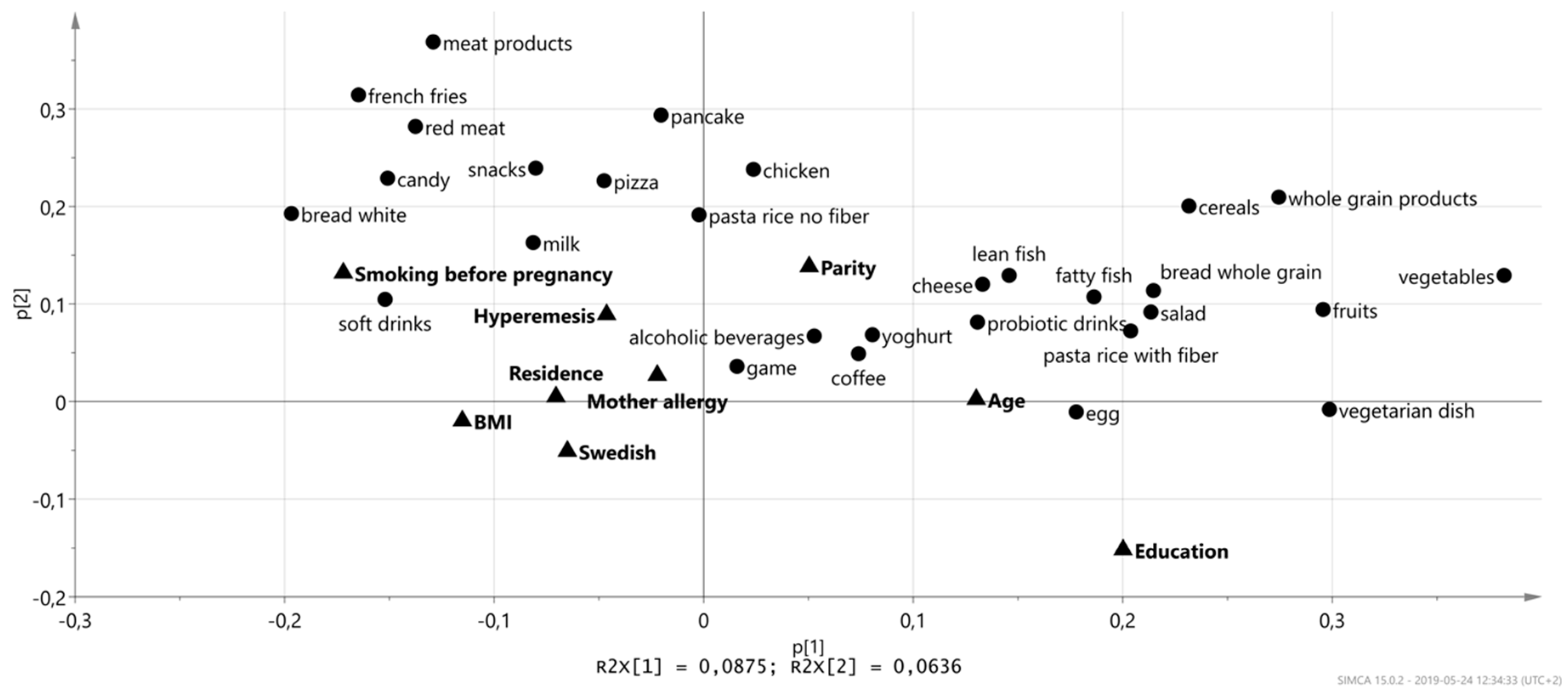
3.5. Associations between Maternal Characteristics and Food Intakes
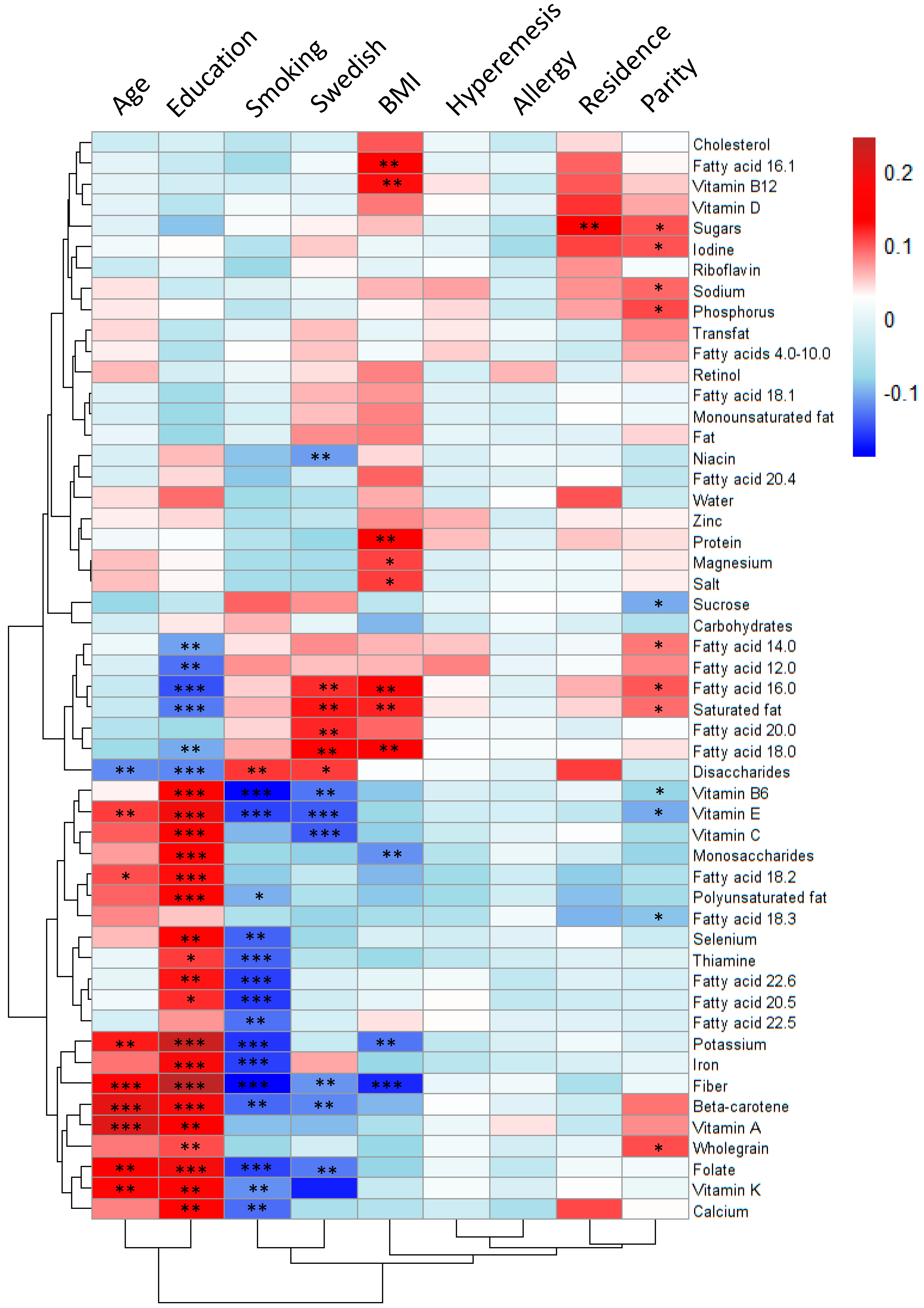
3.6. Associations between Maternal Characteristics and Nutrient Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ramakrishnan, U.; Grant, F.; Goldenberg, T.; Zongrone, A.; Martorell, R. Effect of Women’s Nutrition before and during Early Pregnancy on Maternal and Infant Outcomes: A Systematic Review. Paediatr. Périnat. Epidemiol. 2012, 26, 285–301. [Google Scholar] [CrossRef]
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Georgieff, M.K. Nutrition and the developing brain: Nutrient priorities and measurement. Am. J. Clin. Nutr. 2007, 85, 614–620. [Google Scholar]
- Redman, K.; Ruffman, T.; Fitzgerald, P.; Skeaff, S. Iodine Deficiency and the Brain: Effects and Mechanisms. Crit. Rev. Food Sci. Nutr. 2016, 56, 2695–2713. [Google Scholar] [CrossRef]
- Englund-Ögge, L.; Brantsæter, A.L.; Sengpiel, V.; Haugen, M.; Birgisdottir, B.E.; Myhre, R.; Meltzer, H.M.; Jacobsson, B.; Brantsaeter, A.L. Maternal dietary patterns and preterm delivery: Results from large prospective cohort study. BMJ 2014, 348, g1446. [Google Scholar] [CrossRef]
- Karamanos, B.; Thanopoulou, A.; Anastasiou, E.; Assaad-Khalil, S.; Albache, N.; Bachaoui, M.; Slama, C.B.; El Ghomari, H.; Jotić, A.; The MGSD-GDM Study Group; et al. Relation of the Mediterranean diet with the incidence of gestational diabetes. Eur. J. Clin. Nutr. 2013, 68, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Hillesund, E.R.; Bere, E.; Haugen, M.; Øverby, N.C. Development of a New Nordic Diet score and its association with gestational weight gain and fetal growth—A study performed in the Norwegian Mother and Child Cohort Study (MoBa). Public Health Nutr. 2014, 17, 1909–1918. [Google Scholar] [CrossRef]
- Jonsson, K.; Barman, M.; Moberg, S.; Sjoberg, A.; Brekke, H.K.; Hesselmar, B.; Johansen, S.; Wold, A.E.; Sandberg, A.S. Fat intake and breast milk fatty acid composition in farming and nonfarming women and allergy development in the offspring. Pediatric Res. 2016, 79, 114–123. [Google Scholar] [CrossRef]
- Barman, M.; Murray, F.I.; Bernardi, A.; Broberg, K.; Bölte, S.; Hesselmar, B.; Jacobsson, B.; Jonsson, K.; Kippler, M.; Rabe, H.; et al. Nutritional impact on Immunological maturation during Childhood in relation to the Environment (NICE): A prospective birth cohort in northern Sweden. BMJ Open 2018, 8, e022013. [Google Scholar] [CrossRef]
- Eysenbach, G.; Brantsaeter, A.L.; Barrat, E.E.; Christensen, S.; Möller, E.E.; Bonn, S.; Ploner, A.; Bälter, O.; Lissner, L.; Bälter, K. Relative Validity of Micronutrient and Fiber Intake Assessed with Two New Interactive Meal- and Web-Based Food Frequency Questionnaires. J. Med. Internet Res. 2014, 16, 59. [Google Scholar]
- Christensen, S.E.; Möller, E.; Bonn, S.E.; Ploner, A.; Wright, A.; Sjölander, A.; Bälter, O.; Lissner, L.; Bälter, K.; Eysenbach, G.; et al. Two New Meal- and Web-Based Interactive Food Frequency Questionnaires: Validation of Energy and Macronutrient Intake. J. Med. Internet Res. 2013, 15, e109. [Google Scholar] [CrossRef]
- Administration TSNF. Advice about Food for You Who Are Pregnant. 2008. Available online: https://www.livsmedelsverket.se/globalassets/publikationsdatabas/andra-sprak/advice-about-food-for-you-who-are-pregnant.pdf (accessed on 21 July 2019).
- Nordic Nutrition Recommendations 2012: Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2012.
- Laraia, B.A.; Bodnar, L.M.; Siega-Riz, A.M. Pregravid body mass index is negatively associated with diet quality during pregnancy. Public Health Nutr. 2007, 10, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary Quality during Pregnancy Varies by Maternal Characteristics in Project Viva: A US Cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.; Lee, K.W.; Song, W.O. Pre-Pregnancy Weight Status Is Associated with Diet Quality and Nutritional Biomarkers during Pregnancy. Nutrients 2016, 8, 162. [Google Scholar] [CrossRef]
- De Irala-Estévez, J.; Groth, M.; Johansson, L.; Oltersdorf, U.; Prättälä, R.; Martínez-González, M.A. A systematic review of socio-economic differences in food habits in Europe: Consumption of fruit and vegetables. Eur. J. Clin. Nutr. 2000, 54, 706. [Google Scholar] [CrossRef]
- Hulshof, K.F.; Brussaard, J.H.; Kruizinga, A.G.; Telman, J.; Löwik, M.R. Socio-economic status, dietary intake and 10 y trends: The Dutch National Food Consumption Survey. Eur. J. Clin. Nutr. 2003, 57, 128–137. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Siega-Riz, A.M. A Diet Quality Index for Pregnancy detects variation in diet and differences by sociodemographic factors. Public Health Nutr. 2002, 5, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Arkkola, T.; Uusitalo, U.; Pietikäinen, M.; Metsälä, J.; Kronberg-Kippilä, C.; Erkkola, M.; Veijola, R.; Knip, M.; Virtanen, S.M.; Ovaskainen, M.L. Dietary intake and use of dietary supplements in relation to demographic variables among pregnant Finnish women. Br. J. Nutr. 2006, 96, 913–920. [Google Scholar] [CrossRef] [Green Version]
- Paalanen, L.; Prättälä, R.; Palosuo, H.; Laatikainen, T. Socio-economic differences in the consumption of vegetables, fruit and berries in Russian and Finnish Karelia: 1992–2007. Eur. J. Public Health 2011, 21, 35–42. [Google Scholar] [CrossRef]
- Roos, G.; Johansson, L.; Kasmel, A.; Klumbiene, J.; Prättälä, R. Disparities in vegetable and fruit consumption: European cases from the north to the south. Public Health Nutr. 2001, 4, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Amcoff, E.; Edberg, A.; Enghardt Barbieri, H.; Lindroos, A.-K.; Nälsén, C.; Pearson, M.; Warensjö Lemming, E. Riksmaten–vuxna 2010–2011: Livsmedels- och näringsintag bland vuxna i Sverige; Livsmedelsverket: Uppsala, Sweden, 2012. [Google Scholar]
- Pinheiro, J.; Seabra, D. Changes of food habits during pregnancy and breast-feeding. Acta Médica Port. 2008, 21, 149–160. [Google Scholar]
- Labonte, M.E.; Cyr, A.; Baril-Gravel, L.; Royer, M.M.; Lamarche, B. Validity and reproducibility of a web-based, self-administered food frequency questionnaire. Eur. J. Clin. Nutr.. 2012, 66, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Pinto, E.; Severo, M.; Correia, S.; Silva, I.D.; Lopes, C.; Barros, H. Validity and reproducibility of a semi-quantitative food frequency questionnaire for use among Portuguese pregnant women. Matern. Child Nutr. 2010, 6, 105–119. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Haugen, M.; Alexander, J.; Meltzer, H.M. Validity of a new food frequency questionnaire for pregnant women in the Norwegian Mother and Child Cohort Study (MoBa). Matern. Child Nutr. 2008, 4, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Lutomski, J.E.; van den Broeck, J.; Harrington, J.; Shiely, F.; Perry, I.J. Sociodemographic, lifestyle, mental health and dietary factors associated with direction of misreporting of energy intake. Public Health Nutr. 2011, 14, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Solvoll, K.E.; Bjørneboe, G.E.; Drevon, C.A. Under- and overreporting of energy intake related to weight status and lifestyle in a nationwide sample. Am. J. Clin. Nutr. 1998, 68, 266–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristic | Number of Participants (%) |
|---|---|
| Age (years) | |
| ≤25 | 71 (13) |
| 26–30 | 235 (41) |
| 31–35 | 172 (30) |
| ≥35 | 89 (16) |
| BMI at registration to maternal care, kg/m2 | |
| <18.5 | 9 (2) |
| 18.5–24.9 | 293 (52) |
| 25–29.9 | 155 (27) |
| 30–34.9 | 56 (10) |
| ≥35 | 26 (5) |
| Missing 1 | 28 |
| Highest education level | |
| Elementary school (9 years of schooling) | 12 (2) |
| Senior high school (12 years of schooling) | 153 (27) |
| University or other education after high school (>12 years of full-time studies) | 394 (71) |
| Missing 1 | 8 |
| Smoking before pregnancy | |
| Yes | 32 (6) |
| No | 527 (94) |
| Missing 1 | 8 |
| Parity | |
| No previous children | 280 (50) |
| ≥1 previous child | 281 (50) |
| Missing 1 | 6 |
| Marital status | |
| Married | 23 (4) |
| Cohabitating | 502 (94) |
| Other | 7 (1) |
| Missing 1 | 35 |
| Folic acid intake before pregnancy | |
| Yes | 268 (49) |
| No | 276 (51) |
| Missing 1 | 22 |
| Residential address | |
| Town (central part) | 88 (16) |
| Town (suburb) | 256 (47) |
| Municipality in the countryside | 65 (12) |
| Countryside without animals or stable | 118 (22) |
| Countryside with animals and stable | 13 (2) |
| Missing 1 | 27 |
| Diseases | |
| Any allergy | 211 (37) |
| Asthma | 52 (10) |
| Bowel disease | 6 (1) |
| Chronic hypertension | 4 (1) |
| Diabetes type 1 | 3 (0.5) |
| Gestational diabetes | 7 (1) |
| Hyperemesis | 36 (7) |
| Heart disease | 5 (1) |
| Rheumatoid arthritis | 9 (2) |
| Mean (SD) | Median (IQR) | Min–Max | |
|---|---|---|---|
| Cereals 1 | 81 (119) | 40 (20–99) | 0–1384 |
| Pasta/rice, low-fiber | 74 (45) | 75 (46–98) | 0–260 |
| Pasta/rice, with fiber | 14 (22) | 0 (0–33) | 0–138 |
| Bread, white | 15 (17) | 6 (2–30) | 0–150 |
| Bread, whole-grain | 27 (25) | 21 (9–40) | 0–201 |
| Bread, total | 62 (45) | 53 (35–78) | 0–430 |
| Whole–grain, total 2 | 100 (129) | 64 (25–122) | 0–1502 |
| Milk | 182 (219) | 100 (14–200) | 0–1000 |
| Yoghurt | 133 (130) | 100 (43–200) | 0–1000 |
| Dairy products 3 | 344 (269) | 266 (163–451) | 0–1600 |
| Cheese | 13 (11) | 11 (7–16) | 0–75 |
| Fresh fruits and berries | 219 (159) | 183 (105–297) | 0–1246 |
| Vegetables and roots | 145 (90) | 129 (84–185) | 5–576 |
| Total fruits and vegetables | 363 (208) | 322 (209–475) | 11–1452 |
| Red meat 4 | 66 (33) | 66 (46–80) | 0–214 |
| Meat products 5 | 56 (32) | 51 (36–75) | 0–267 |
| Game meat 6 | 12 (21) | 0 (0–16) | 0–125 |
| Chicken | 22 (16) | 27 (9–27) | 0–125 |
| Total meat 7 | 157 (67) | 153 (116–193) | 0–469 |
| Fatty fish | 18 (14) | 9 (9–28) | 0–85 |
| Lean fish | 14 (12) | 9 (9–27) | 0–98 |
| Seafood | 5 (6) | 7 (0–7) | 0–50 |
| Total fish | 37 (23) | 35 (18–50) | 0–154 |
| Vegetarian dishes | 25 (44) | 18 (0–23) | 0–322 |
| Egg | 13 (17) | 11 (4–11) | 0–200 |
| Coffee | 148 (163) | 118 (0–300) | 0–750 |
| French fries | 16 (12) | 11 (11–32) | 0–75 |
| Pizza | 25 (22) | 25 (25–25) | 0–175 |
| Nuts | 7 (13) | 3 (0–9) | 0–120 |
| Candy 8 | 44 (56) | 29 (0–68) | 0–400 |
| Snacks 9 | 24 (19) | 20 (10–34) | 0–166 |
| Mean (SD) | Median (IQR) | Min–Max | |
|---|---|---|---|
| Energy, kJ | 7440 (2582) | 7240 (5635–8888) | 2421–16,441 |
| Energy, kcal | 1778 (617) | 1730 (1345–2124) | 579–3930 |
| Macronutrient | E% | ||
| Carbohydrates 1 | 48 (5.6) | 48 (44–51) | 27–66 |
| Dietary fibers 1 | 2.2 (0.84) | 2.1 (1.6–2.7) | 0.55–5.4 |
| Proteins 1 | 16 (2.7) | 16 (15–18) | 8.6–27 |
| Total fat 2 | 36 (4.4) | 36 (33–39) | 20–51 |
| Saturated fat 2 | 16 (2.8) | 15 (14–17) | 6.9–25 |
| Monounsaturated fat 2 | 13 (1.8) | 13 (11–14) | 6.9–18 |
| Polyunsaturated fat, sum 2 | 4.6 (1.5) | 4.2 (3.5–5.2) | 2.2–12 |
| Omega-6 polyunsaturated fat 2 | 3.5 (1.2) | 3.2 (2.6–4.1) | 1.5–9.5 |
| Omega-3 polyunsaturated fat 2 | 0.89 (0.34) | 0.83 (0.67–1.0) | 0.36–3.8 |
| Micronutrient | Median (IQR) | Min–Max |
|---|---|---|
| Vitamin A (µg) | 90 (73–120) | 40–340 |
| Vitamin B6 (mg) | 0.24 (0.20–0.27) | 0.11–0.46 |
| Vitamin B12 (µg) | 0.69 (0.56–0.85) | 0.13–1.8 |
| Vitamin C (mg) | 14 (9.4–19) | 0.79–65 |
| Vitamin D (µg) * | 0.85 (0.66–1.2) | 0.14–3.6 |
| Vitamin E (mg) | 1.1 (0.95–1.4) | 0.53–3.6 |
| Vitamin K (µg) | 4.2 (3.2–5.5) | 0.74–17 |
| Calcium (g) | 0.14 (0.12–0.17) | 0.06–0.35 |
| Folate (µg) * | 42 (35–49) | 15–105 |
| Iodine (µg) * | 14 (10–18) | 3.4–70 |
| Iron (mg) * | 1.4 (1.2–1.7) | 0.52–3.9 |
| Magnesium (mg) | 41 (37–46) | 25–74 |
| Niacin (mg) | 2.2 (1.8–2.4) | 0.81–4.8 |
| Phosphorus (mg) | 190 (170–210) | 100–340 |
| Potassium (g) | 0.39 (0.34–0.45) | 0.21–0.64 |
| Riboflavin (mg) | 0.23 (0.20–0.27) | 0.11–0.62 |
| Sodium (g) | 0.31 (0.28–0.35) | 0.13–0.63 |
| Selenium (µg) * | 5.5 (4.4–7.1) | 2.1–17 |
| Thiamin (mg) | 0.18 (0.15–0.20) | 0.74–17 |
| Zinc (mg) | 1.3 (1.2–1.4) | 0.65–2.0 |
| Daily Intake, N (%) | Weekly Intake, N (%) | |
| Multivitamins with minerals | 185 (33) | 48 (9) |
| Vitamin A | 23 (4) | 2 (0) |
| Vitamin B | 42 (7) | 5 (1) |
| Vitamin C | 31 (6) | 14 (3) |
| Vitamin D | 62 (11) | 13 (2) |
| Vitamin E | 23 (4) | 3 (1) |
| Folic acid | 104 (18) | 22 (4) |
| Iron | 220 (39) | 75 (13) |
| Calcium | 35 (6) | 4 (1) |
| Fish oil/omega-3 | 54 (10) | 15 (3) |
| Regular Intake, N (%) | ||
| Beta-carotene 1 | 18 (3) | |
| Selenium 1 | 30 (5) | |
| Zinc 1 | 40 (7) | |
| Magnesium 1 | 60 (11) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stråvik, M.; Jonsson, K.; Hartvigsson, O.; Sandin, A.; Wold, A.E.; Sandberg, A.-S.; Barman, M. Food and Nutrient Intake during Pregnancy in Relation to Maternal Characteristics: Results from the NICE Birth Cohort in Northern Sweden. Nutrients 2019, 11, 1680. https://doi.org/10.3390/nu11071680
Stråvik M, Jonsson K, Hartvigsson O, Sandin A, Wold AE, Sandberg A-S, Barman M. Food and Nutrient Intake during Pregnancy in Relation to Maternal Characteristics: Results from the NICE Birth Cohort in Northern Sweden. Nutrients. 2019; 11(7):1680. https://doi.org/10.3390/nu11071680
Chicago/Turabian StyleStråvik, Mia, Karin Jonsson, Olle Hartvigsson, Anna Sandin, Agnes E. Wold, Ann-Sofie Sandberg, and Malin Barman. 2019. "Food and Nutrient Intake during Pregnancy in Relation to Maternal Characteristics: Results from the NICE Birth Cohort in Northern Sweden" Nutrients 11, no. 7: 1680. https://doi.org/10.3390/nu11071680
APA StyleStråvik, M., Jonsson, K., Hartvigsson, O., Sandin, A., Wold, A. E., Sandberg, A. -S., & Barman, M. (2019). Food and Nutrient Intake during Pregnancy in Relation to Maternal Characteristics: Results from the NICE Birth Cohort in Northern Sweden. Nutrients, 11(7), 1680. https://doi.org/10.3390/nu11071680