Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012

Abstract
:1. Introduction
2. Materials and Methods
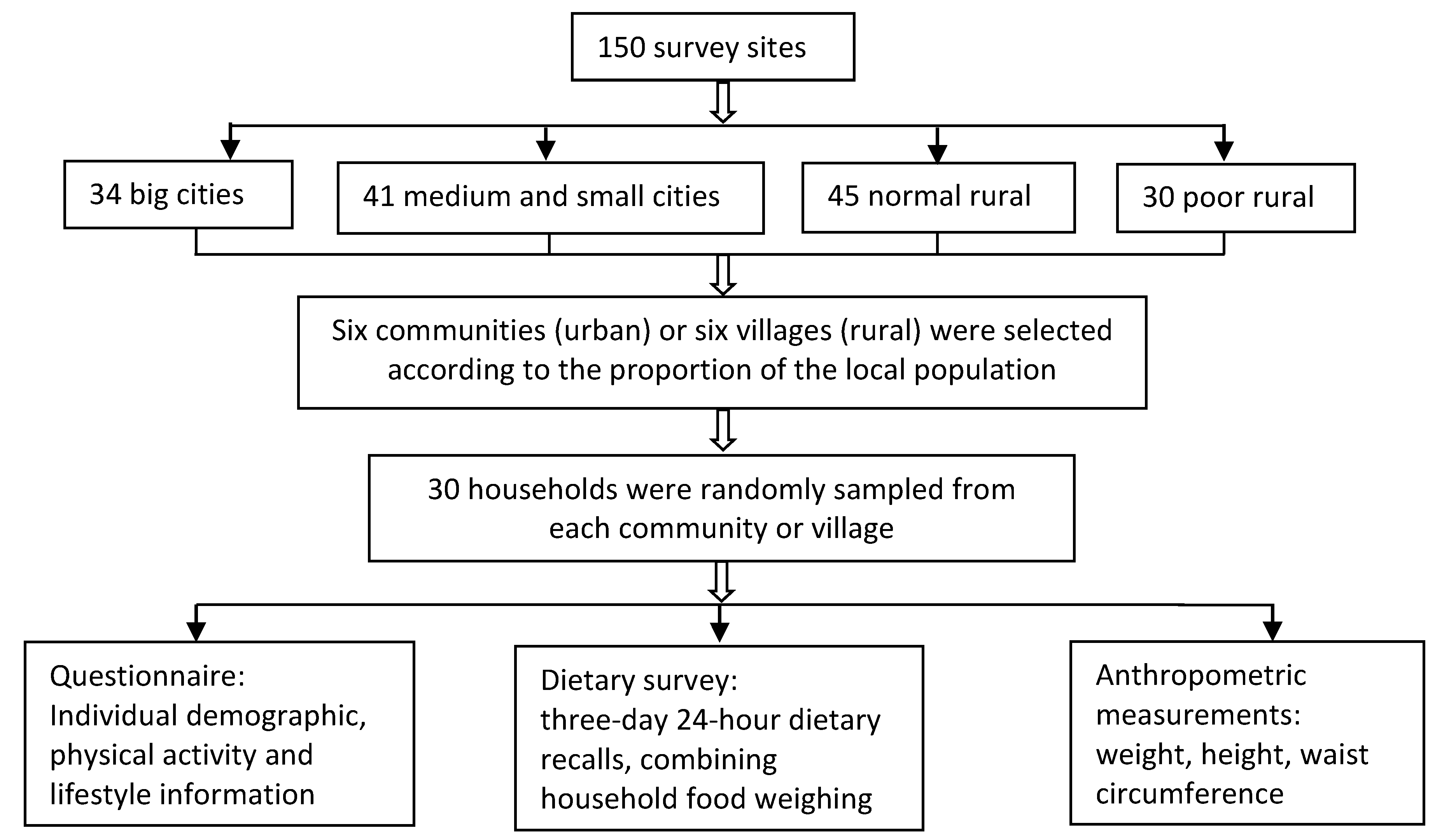
2.1. Data Sources
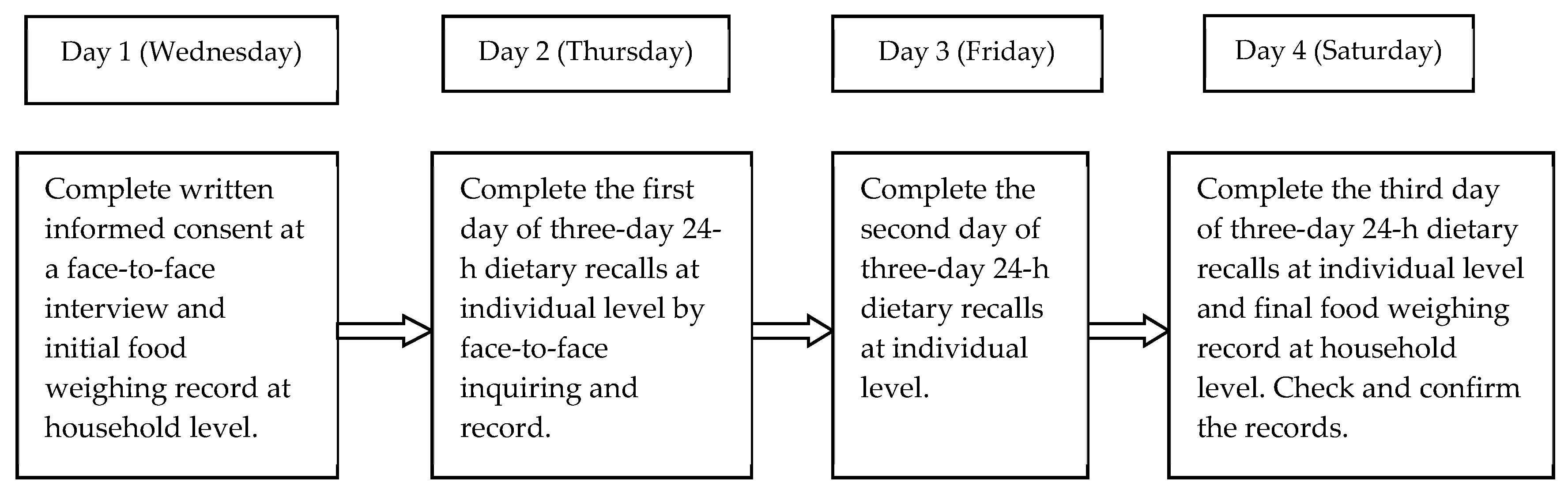
2.2. Subjects and Methods
2.3. Statistical Analysis
3. Results
3.1. Characteristic and Usual Dietary Energy Intake of the Subjects
3.2. Assessment of Dietary Micronutrients Intakes
3.2.1. Assessment of Dietary Micronutrients Intakes between the Two Genders
3.2.2. Assessment of Dietary Micronutrients Intakes between Different Age Groups
3.2.3. Assessment of Dietary Micronutrients Intakes between Northern and Southern Regions
3.2.4. Assessment of Dietary Micronutrients Intakes between in Different Socioeconomic Types
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgment
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Vitamin A & | Vitamin B1 | Vitamin B2 | Vitamin B6 | Vitamin B12 | Folate & | Vitamin C | Vitamin E & | |
|---|---|---|---|---|---|---|---|---|
| EAR (μg/day) | EAR (mg/day) | EAR (mg/day) | EAR (mg/day) | EAR (μg/day) | EAR (μg/day) | EAR (μg/day) | AI (mg/day) | |
| Men | ||||||||
| 50–64 | 560 | 1.2 | 1.2 | 1.3 | 2.0 | 320 | 85 | 14 |
| 65–79 | 560 | 1.2 | 1.2 | 1.3 | 2.0 | 320 | 85 | 14 |
| ≥80 | 560 | 1.2 | 1.2 | 1.3 | 2.0 | 320 | 85 | 14 |
| Female | ||||||||
| 50–64 | 480 | 1.0 | 1.0 | 1.3 | 2.0 | 320 | 85 | 14 |
| 65–79 | 480 | 1.0 | 1.0 | 1.3 | 2.0 | 320 | 85 | 14 |
| ≥80 | 480 | 1.0 | 1.0 | 1.3 | 2.0 | 320 | 85 | 14 |
| Calcium | Potassium | Sodium | Magnesium | Iron | Zinc | Selenium | |
|---|---|---|---|---|---|---|---|
| EAR (mg/day) | AI (mg/day) | AI (mg/day) | EAR (mg/day) | EAR (mg/day) | EAR (mg/day) | EAR (μg/day) | |
| Men | |||||||
| 50–64 | 800 | 2000 | 1400 | 280 | 9 | 10.4 | 50 |
| 65–79 | 800 | 2000 | 1400 | 270 | 9 | 10.4 | 50 |
| ≥80 | 800 | 2000 | 1300 | 260 | 9 | 10.4 | 50 |
| Female | |||||||
| 50–64 | 800 | 2000 | 1400 | 280 | 9 | 6.1 | 50 |
| 65–79 | 800 | 2000 | 1400 | 270 | 9 | 6.1 | 50 |
| ≥80 | 800 | 2000 | 1300 | 260 | 9 | 6.1 | 50 |
References
- Bailey, R.L.; West, K.J.; Black, R.E. The epidemiology of global micronutrient deficiencies. Ann. Nutr. Metab. 2015, 66 (Suppl. 2), 22–33. [Google Scholar] [CrossRef] [PubMed]
- The Micronutrient Initiative. Investing in the Future: A United call to Action on Vitamin and Mineral Deficiencies. Available online: http://www.unitedcalltoaction.org/documents/Investing_in_the_future.pdf (accessed on 15 March 2019).
- Carr, A.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Shin, C.; Baik, I. Longitudinal associations between micronutrient consumption and leukocyte telomere length. J. Hum. Nutr. Diet. 2017, 30, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Olivares, M.; Hertrampf, E.; Capurro, M.T.; Wegner, D. Prevalence of anemia in elderly subjects living at home: Role of micronutrient deficiency and inflammation. Eur. J. Clin. Nutr. 2000, 54, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Whalley, L.J.; Duthie, S.J.; Collins, A.R.; Starr, J.M.; Deary, I.J.; Lemmon, H.; Duthie, A.C.; Murray, A.D.; Staff, R.T. Homocysteine, antioxidant micronutrients and late onset dementia. Eur. J. Nutr. 2014, 53, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Polidori, M.C.; Schulz, R.J. Nutritional contributions to dementia prevention: Main issues on antioxidant micronutrients. Genes Nutr. 2014, 9, 382. [Google Scholar] [CrossRef] [PubMed]
- Visioli, F.; Burgos-Ramos, E. Selected Micronutrients in Cognitive Decline Prevention and Therapy. Mol. Neurobiol. 2016, 53, 4083–4093. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, A.; Amiot, M. Fat-soluble micronutrients and metabolic syndrome. Curr. Opin. Clin. Nutr. 2017, 20, 492–497. [Google Scholar] [CrossRef] [Green Version]
- Grober, U.; Holzhauer, P.; Kisters, K.; Holick, M.F.; Adamietz, I.A. Micronutrients in Oncological Intervention. Nutrients 2016, 8, 163. [Google Scholar] [CrossRef] [PubMed]
- Aslam, T.; Delcourt, C.; Silva, R.; Holz, F.G.; Leys, A.; Garcia, L.A.; Souied, E. Micronutrients in age-related macular degeneration. Ophthalmologica 2013, 229, 75–79. [Google Scholar] [CrossRef]
- Torbergsen, A.C.; Watne, L.O.; Wyller, T.B.; Frihagen, F.; Stromsoe, K.; Bohmer, T.; Mowe, M. Micronutrients and the risk of hip fracture: Case-control study. Clin. Nutr. 2017, 36, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Witte, K.K.; Nikitin, N.P.; Parker, A.C.; von Haehling, S.; Volk, H.D.; Anker, S.D.; Clark, A.L.; Cleland, J.G. The effect of micronutrient supplementation on quality-of-life and left ventricular function in elderly patients with chronic heart failure. Eur. Heart J. 2005, 26, 2238–2244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, E.; Iso, H.; Yamagishi, K.; Ando, M.; Wakai, K.; Tamakoshi, A. Dietary Antioxidant Micronutrients and All-Cause Mortality: The Japan Collaborative Cohort Study for Evaluation of Cancer Risk. J. Epidemiol. 2018, 28, 388–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harding, K.L.; Aguayo, V.M.; Webb, P. Hidden hunger in South Asia: A review of recent trends and persistent challenges. Public Health Nutr. 2018, 21, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.J.; Qaim, M. The human and economic cost of hidden hunger. Food Nutr. Bull. 2007, 28, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Ritz, P. Factors affecting energy and macronutrient requirements in elderly people. Public Health Nutr. 2001, 4, 561–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidari, Z.; Feizi, A.; Azadbakht, L.; Mohammadifard, N.; Maghroun, M.; Sarrafzadegan, N. Usual energy and macronutrient intakes in a large sample of Iranian middle-aged and elderly populations. Nutr. Diet. 2019, 76, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Quann, E.E.; Fulgoni, V.R.; Auestad, N. Consuming the daily recommended amounts of dairy products would reduce the prevalence of inadequate micronutrient intakes in the United States: Diet modeling study based on NHANES 2007–2010. Nutr. J. 2015, 14, 90. [Google Scholar] [CrossRef]
- Mensink, G.B.; Fletcher, R.; Gurinovic, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef] [Green Version]
- Ter Borg, S.; Verlaan, S.; Hemsworth, J.; Mijnarends, D.M.; Schols, J.M.; Luiking, Y.C.; de Groot, L.C. Micronutrient intakes and potential inadequacies of community-dwelling older adults: A systematic review. Br. J. Nutr. 2015, 113, 1195–1206. [Google Scholar] [CrossRef]
- Zhao, L.Y.; Ma, G.S.; Piao, J.H. Overall plan of China national nutrition and health survey in 2010–2012. Chin. J. Prev. Med. 2016, 3, 204–207. [Google Scholar]
- Yang, Y.X. Chinese Food Composition Table; Peking University Medical Press: Beijing, China, 2005; ISBN 978-7-81071-678-9. [Google Scholar]
- Yang, Y.X. Chinese Food Composition Table, 2nd ed; Peking University Medical Press: Beijing, China, 2009; ISBN 978-7-81116-727-6. [Google Scholar]
- USDA. Food Composition Databases: Nutrient Lists. Available online: https://ndb.nal.usda.gov/ndb/nutrients/report/nutrientsfrm?max=25&offset=0&totCount=0&nutrient1=418&nutrient2=&nutrient3=&subset=0&sort=f&measureby=m (accessed on 10 January 2018).
- MEXT. Standard Tables of Food Composition in Japan (Seventh Revised Version). 2015. Available online: http://www.mext.go.jp/en/policy/science_technology/policy/title01/detail01/sdetail01/sdetail01/1385122.htm (accessed on 18 January 2018).
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65 (Suppl. 1), S87–S91. [Google Scholar] [CrossRef] [PubMed]
- Chinese Nutrition Society. Chinese Dietary Reference intakes (2013); Science Press: Beijing, China, 2014; ISBN 978-7-03-041401-4. [Google Scholar]
- Food and Nutrition Board. Nutrient Recommendations: Dietary Reference Intakes (DRI). Available online: https://ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx (accessed on 15 July 2019).
- National Academy of Science Board. Dietary Reference Intakes: Applications in Dietary Assessment; The National Academies Press: Washington, DC, USA, 2000; ISBN 0-309-07311-1. [Google Scholar]
- WHO. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Swizerland, 2012; ISBN 97-92-4-150483-6. [Google Scholar]
- Fan, Y.; Liu, A.; He, Y.; Yang, X.; Xu, G.; Ma, G. Assessment of nutrient adequacy of adult residents in China. Acta Nutr. Sin. 2012, 1, 15–19. [Google Scholar]
- Bailey, R.L.; Fulgoni, V.L.; Taylor, C.L.; Pfeiffer, C.M.; Thuppal, S.V.; McCabe, G.P.; Yetley, E.A. Correspondence of folate dietary intake and biomarker data. Am. J. Clin. Nutr. 2017, 105, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Steluti, J.; Selhub, J.; Paul, L.; Reginaldo, C.; Fisberg, R.M.; Marchioni, D. An overview of folate status in a population-based study from Sao Paulo, Brazil and the potential impact of 10 years of national folic acid fortification policy. Eur. J. Clin. Nutr. 2017, 71, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Sicinska, E.; Wyka, J. Folate intake in Poland on the basis of literature from the last ten years (2000–2010). Roczniki Panstwowego Zakladu Higieny 2011, 62, 247–256. [Google Scholar] [PubMed]
- Hopkins, S.M.; Gibney, M.J.; Nugent, A.P.; McNulty, H.; Molloy, A.M.; Scott, J.M.; Flynn, A.; Strain, J.J.; Ward, M.; Walton, J.; et al. Impact of voluntary fortification and supplement use on dietary intakes and biomarker status of folate and vitamin B-12 in Irish adults. Am. J. Clin. Nutr. 2015, 101, 1163–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenech, M. Folate (vitamin B9) and vitamin B12 and their function in the maintenance of nuclear and mitochondrial genome integrity. Mutat. Res. 2012, 733, 21–33. [Google Scholar] [CrossRef]
- GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 439–458. [Google Scholar] [CrossRef]
- Wang, L.D.; Liu, J.M.; Yang, Y.; Peng, B.; Wang, Y.L. The Prevention and Treatment of Stroke Still Face Huge Challenges—Brief Report on Stroke Prevention and Treatment in China, 2018. Chin. Circ. J. 2019, 2, 105–118. [Google Scholar]
- Chang, X.; DeFries, R.S.; Liu, L.; Davis, K. Understanding dietary and staple food transitions in China from multiple scales. PLoS ONE 2018, 13, e195775. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.Y.; Fang, Y.H.; He, Y.N.; Yu, D.M.; Guo, Q.Y.; Yu, W.T.; Fang, H.Y.; Wang, X.; Zhao, W.H. Trends of food consumption among Chinese population in 1992–2012. J. Hyg. Res. 2016, 4, 522–526. [Google Scholar]
- Wang, J.; Zhao, L.Y.; Yu, D.M.; Li, Y.R.; Huo, J.S.; Huang, J.; Ding, G.Q. Status of nutrition and associated factors among the Chinese aged 60 and above in 2010–2012 in China. J. Hyg. Res. 2019, 2, 200–207. [Google Scholar]
- Su, L.; Dongmei, Y.; Qiya, G.; Xun, W.; Xiaoli, X.; Fengmei, J.; Jie, L.; Liyun, Z. Consumption status and trend of added sugar containing food among Chinese from 2002 to 2012. J. Hyg. Res. 2016, 3, 398–401. [Google Scholar]
- Liu, Z.; Pang, S.J.; Li, Y.Q.; Man, Q.Q.; Li, L.X.; Zhang, J. Consumption status of dairy products in Chinese aged 60 and above in 2010–2012. J. Hyg. Res. 2016, 5, 708–713. [Google Scholar]
- Wang, L.J. Comprehensive Assessment of Iron Status of Chinese Population in Large City and Poor Rural Areas. PhD Thesis, Chinese Center for Disease Control and Prevention, Beijing, China, 2015. [Google Scholar]
- Luan, C.D.; Li, H.; Li, S.J.; Zhao, Z.; Li, X.; Liu, Z.M. Body iron stores and dietary iron intake in relation to diabetes in adults in north China. Diabetes Care 2008, 31, 285–286. [Google Scholar] [CrossRef]
- Shi, Z.; Hu, X.; Yuan, B.; Pan, X.; Meyer, H.E.; Holmboe-Ottesen, G. Association Between Serum Ferritin, Hemoglobin, Iron Intake, and Diabetes in Adults in Jiangsu, China. Diabetes Care 2006, 29, 1878–1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, W.; Rong, Y.; Rong, S.; Liu, L.G. Dietary iron intake, body iron stores, and the risk of type 2 diabetes: A systematic review and meta-analysis. BMC Med. 2012, 10, 119. [Google Scholar] [CrossRef]
- Moore, A.B.; Shannon, J.; Chen, C.; Lampe, J.W.; Ray, R.M.; Lewis, S.K.; Lin, M.G.; Stalsberg, H.; Thomas, D.B. Dietary and stored iron as predictors of breast cancer risk: A nested case–control study in Shanghai. Int. J. Cancer 2009, 125, 1110–1117. [Google Scholar] [CrossRef]
- Shi, Z.M.; Li, M.; Wang, Y.F.; Liu, J.H.; El-Obeid, T. High iron intake is associated with poor cognition among Chinese old adults and varied by weight status-a 15-y longitudinal study in 4852 adults. Am. J. Clin. Nutr. 2019, 109, 109–116. [Google Scholar] [CrossRef]
- Yu, D.M.; He, Y.N.; Guo, Q.Y.; Fang, H.Y.; Xu, X.L.; Fang, Y.H.; Li, J.; Zhao, L.Y. Trends of energy and nutrients intake among Chinese population in 2002–2012. J. Hyg. Res. 2016, 45, 527–533. [Google Scholar]
- He, Y.N.; Li, Y.P.; Yang, X.G.; Hemler, E.C.; Fang, Y.H.; Zhao, L.Y.; Zhang, J.; Yang, Z.Y.; Wang, Z.; He, L.; et al. The dietary transition and its association with cardiometabolic mortality among Chinese adults, 1982–2012: A cross-sectional population-based study. Lancet Diabetes Endocrinol. 2019, 7, 540–548. [Google Scholar] [CrossRef]
- Yang, Q.; Liu, T.; Kuklina, E.V.; Flanders, W.D.; Hong, Y.; Gillespie, C.; Chang, M.H.; Gwinn, M.; Dowling, N.; Khoury, M.J.; et al. Sodium and potassium intake and mortality among US adults: Prospective data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2011, 171, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Okayama, A.; Okuda, N.; Miura, K.; Okamura, T.; Hayakawa, T.; Akasaka, H.; Ohnishi, H.; Saitoh, S.; Arai, Y.; Kiyohara, Y.; et al. Dietary sodium-to-potassium ratio as a risk factor for stroke, cardiovascular disease and all-cause mortality in Japan: The NIPPON DATA80 cohort study. BMJ Open 2016, 6, e11632. [Google Scholar] [CrossRef] [PubMed]
- Willey, J.; Gardener, H.; Cespedes, S.; Cheung, Y.K.; Sacco, R.L.; Elkind, M. Dietary Sodium to Potassium Ratio and Risk of Stroke in a Multiethnic Urban Population: The Northern Manhattan Study. Stroke 2017, 48, 2979–2983. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Issues New Guidance on Dietary Salt and Potassium. 2013. Available online: https://www.who.int/mediacentre/news/notes/2013/salt_potassium_20130131/en/ (accessed on 24 March 2019).
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; O’Leary, N.; Yin, L.; Liu, X.; Swaminathan, S.; Khatib, R.; Rosengren, A.; et al. Joint association of urinary sodium and potassium excretion with cardiovascular events and mortality: Prospective cohort study. BMJ 2019, 364, l772. [Google Scholar] [CrossRef] [PubMed]
- Rippin, H.L.; Hutchinson, J.; Jewell, J.; Breda, J.J.; Cade, J.E. Adult Nutrient Intakes from Current National Dietary Surveys of European Populations. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Zhu, K.; Devine, A.; Suleska, A.; Tan, C.Y.; Toh, C.Z.; Kerr, D.; Prince, R.L. Adequacy and change in nutrient and food intakes with aging in a seven-year cohort study in elderly women. J. Nutr. Health Aging 2010, 14, 723–729. [Google Scholar] [CrossRef]
- Ronni, C. Geriatric Nutrition: The Health Professional’s Handbook, 3rd ed.; Jones & Bartlett: Boston, MA, USA, 2006; ISBN 0763731811. [Google Scholar]
- Song, F.; Cho, M.S. Geography of Food Consumption Patterns between South and North China. Foods 2017, 6. [Google Scholar] [CrossRef]
- Batis, C.; Mendez, M.A.; Gordon-Larsen, P.; Sotres-Alvarez, D.; Adair, L.; Popkin, B. Using both principal component analysis and reduced rank regression to study dietary patterns and diabetes in Chinese adults. Public Health Nutr. 2016, 19, 195–203. [Google Scholar] [CrossRef]
- Zhang, J.G.; Wang, Z.H.; Wang, H.J.; Du, W.W.; Su, C.; Zhang, J.; Jiang, H.R.; Zhai, F.Y.; Zhang, B. Dietary patterns and their associations with general obesity and abdominal obesity among young Chinese women. Eur. J. Clin. Nutr. 2015, 69, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Cembranel, F.; Wagner, K.; Gonzalez-Chica, D.A.; D’Orsi, E. Education and Income Levels are Associated with Energy and Micronutrients Intake. Int. J. Vitam. Nutr. Res. 2019, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Darnton-Hill, I.; Mkparu, U.C. Micronutrients in pregnancy in low- and middle-income countries. Nutrients 2015, 7, 1744–1768. [Google Scholar] [CrossRef] [PubMed]
- Bird, J.; Murphy, R.; Ciappio, E.; McBurney, M. Risk of Deficiency in Multiple Concurrent Micronutrients in Children and Adults in the United States. Nutrients 2017, 9, 655. [Google Scholar] [CrossRef] [PubMed]
- McNeill, G.; Vyvyan, J.; Peace, H.; McKie, L.; Seymour, G.; Hendry, J.; MacPherson, I. Predictors of micronutrient status in men and women over 75 years old living in the community. Br. J. Nutr. 2002, 88, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Weeden, A.; Remig, V.; Holcomb, C.A.; Herald, T.J.; Baybutt, R.C. Vitamin and mineral supplements have a nutritionally significant impact on micronutrient intakes of older adults attending senior centers. J. Nutr. Elder. 2010, 29, 241–254. [Google Scholar] [CrossRef]
- Shakur, Y.A.; Tarasuk, V.; Corey, P.; O’Connor, D.L. A comparison of micronutrient inadequacy and risk of high micronutrient intakes among vitamin and mineral supplement users and nonusers in Canada. J. Nutr. 2012, 142, 534–540. [Google Scholar] [CrossRef]
- Cuskelly, G.J.; Mooney, K.M.; Young, I.S. Folate and vitamin B12: Friendly or enemy nutrients for the elderly. Proc. Nutr. Soc. 2007, 66, 548–558. [Google Scholar] [CrossRef]
- Chen, T.C.; Chimrh, F.; Lu, Z.; Mathieu, J.; Person, K.S.; Zhang, A.; Kohn, N.; Martinello, S.; Berkowitz, R.; Holick, M.F. Factors that influence the cutaneous synthesis and dietary sources of vitamin D. Arch. Biochem. Biophys. 2007, 460, 213–217. [Google Scholar] [CrossRef] [Green Version]
- Ellen, S.; Michalski, E.S.; Nguyen, P.H.; Gonzalez-Casanova, I.; Nguyen, S.V.; Martorell, R.; Tangpricha, V.; Ramakrishnan, U. Serum 25-hydroxyvitamin D but not dietary vitamin D intake is associated with hemoglobin in women of reproductive age in rural northern Vietnam. J. Clin. Transl. Endocrinol. 2017, 8, 41–48. [Google Scholar] [CrossRef]


| Male | Female | Total | |
|---|---|---|---|
| Age, y | 68.92 ± 6.56 | 68.69 ± 6.86 | 68.81 ± 6.71 |
| Socioeconomic types *, n (%) | |||
| Big cities | 2153 (26.4%) | 2436 (28.8%) | 4589 (27.6%) |
| Small and medium sized cities | 2255 (27.7%) | 2264 (26.8%) | 4519 (27.2%) |
| Normal rural | 2413 (29.6%) | 2401 (28.4%) | 4814 (29.0%) |
| Poor rural | 1327 (16.3%) | 1363 (16.0%) | 2690 (16.2%) |
| Age group, n (%) | |||
| 60–74 | 6613 (81.2%) | 6916 (81.7%) | 13,529 (81.4%) |
| ≥75 | 1535 (18.8) | 1548 (18.3%) | 3083 (18.6%) |
| Geographic Region **, n (%) | |||
| North | 3296 (40.5%) | 3515 (41.5%) | 6811 (41.0%) |
| South | 4852 (59.5%) | 4949 (58.5%) | 9801 (59.0%) |
| Energy intake, Mean ± SD (kcal/day) | |||
| 60–64 year | 2078 ± 678 | 1727 ± 534 | 1893 ± 631 |
| 65–79 year | 1899 ± 605 | 1611 ± 561 | 1757 ± 603 |
| ≥80 year | 1663 ± 546 | 1396 ± 535 | 1516 ± 557 |
| Male | Female | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | |
| Vitamin A (μg/day) & | 403.5 ± 312.8 | 326.2 (195.8, 521.1) | 78.9 # | 369.9 ± 299.8 | 294.5 (173.5, 477.8) | 74.6 | 386.4 ± 307.1 | 309.5 (183.6, 498.7) | 76.7 |
| Vitamin B1 (mg/day) | 0.8 ± 0.3 | 0.8 (0.6, 1.1) | 89.3 # | 0.7 ± 0.3 | 0.7 (0.5, 0.9) | 86.0 | 0.8 ± 0.3 | 0.7 (0.5, 0.9) | 87.7 |
| Vitamin B2 (mg/day) | 0.7 ± 0.3 | 0.7 (0.5, 0.8) | 95.5 # | 0.6 ± 0.3 | 0.6 (0.4, 0.7) | 92.6 | 0.7 ± 0.3 | 0.6 (0.5, 0.8) | 94.0 |
| Vitamin B6 (mg/day) | 0.6 ± 0.4 | 0.5 (0.3, 0.8) | 93.9 | 0.5 ± 0.4 | 0.4 (0.2, 0.7) | 96.3 # | 0.5 ± 0.4 | 0.4 (0.3, 0.7) | 95.1 |
| Vitamin B12 (μg/day) | 1.5 ± 1.9 | 0.9 (0.5, 1.7) | 80.3 | 1.3 ± 1.7 | 0.8 (0.4, 1.5) | 83.3 # | 1.4 ± 1.8 | 0.9 (0.4, 1.6) | 81.8 |
| Vitamin C (mg/day) | 73.4 ± 41.2 | 66.2 (44.4, 94.4) | 68.8 | 67.4 ± 39.2 | 60.4 (39.7, 86.9) | 73.1 # | 70.3 ± 40.3 | 63.1 (41.9, 90.6) | 71.0 |
| Folate (μg/day) & | 80.2 ± 65.4 | 63.7 (34.9, 108.4) | 99.3 | 69.1 ± 57.1 | 55.8 (30.3, 92.3) | 99.5 | 74.5 ± 62.4 | 59.2 (32.1, 100.5) | 99.4 |
| Vitamin E (mg/day) *,& | 32.4 ± 35.8 | 25.4 (16.2, 38.2) | - | 27.1 ± 34.4 | 21.5 (14.2, 32.1) | - | 29.5 ± 35.2 | 23.3 (14.9, 35.4) | - |
| Calcium (mg/day) | 356.7 ± 177.1 | 319.8 (235.2, 438.9) | 97.8 | 320.1 ± 165.8 | 284.8 (207.4, 394.6) | 98.5 # | 338.3 ± 173.3 | 301.4 (220.3, 417.4) | 98.2 |
| Potassium (mg/day) * | 1490 ± 569 | 1406 (1097, 1771) | - | 1312 ± 512 | 1234 (954, 1575) | - | 1400 ± 548 | 1317 (1017, 1680) | - |
| Sodium (mg/day) * | 5128 ± 4999 | 4255 (3009, 5931) | - | 4292 ± 4432 | 3569 (2542, 4946) | - | 4702 ± 4739 | 3876 (2741, 5473) | - |
| Magnesium (mg/day) | 264.8 ± 95.1 | 251.2 (198.9, 313.1) | 61.2 | 230.6 ± 83.5 | 217.4 (172.1, 275.7) | 73.7 # | 247.4 ± 91.2 | 234.3 (184.7, 294.5) | 67.5 |
| Iron (mg/day) | 19.4 ± 6.9 | 18.5 (14.9, 22.6) | 2.0 | 16.8 ± 6.1 | 15.9 (12.7, 19.7) | 4.6 # | 18.1 ± 6.6 | 17.1 (13.6, 21.2) | 3.3 |
| Zinc (mg/day) | 9.5 ± 3.3 | 9.4 (7.2, 11.3) | 67.6 # | 8.2 ± 3.0 | 7.7 (6.1, 9.7) | 24.8 | 8.8 ± 3.2 | 8.3 (6.6, 10.5) | 45.8 |
| Selenium (mg/day) | 40.4 ± 18.3 | 37.5 (28.1, 49.3) | 76.6 | 34.8 ± 16.8 | 32.1 (23.7, 42.5) | 85.5 # | 37.6 ± 17.8 | 34.6 (25.7, 46.1) | 81.1 |
| 60–74 years | ≥75 years | |||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | |
| Vitamin A (μg/day) & | 390.4 ± 307.8 | 313.9 (185.4, 505.9) | 76.1 | 368.8 ± 301.3 | 296.2 (175.4, 462.5) | 79.6 # |
| Vitamin B1 (mg/day) | 0.8 ± 0.3 | 0.7 (0.6, 0.9) | 86.5 | 0.7 ± 0.3 | 0.6 (0.5, 0.8) | 92.7 # |
| Vitamin B2 (mg/day) | 0.7 ± 0.3 | 0.6 (0.5, 0.8) | 93.7 | 0.6 ± 0.3 | 0.6 (0.4, 0.7) | 95.4 # |
| Vitamin B6 (mg/day) | 0.5 ± 0.4 | 0.5 (0.3, 0.8) | 94.9 | 0.5 ± 0.4 | 0.4 (0.2, 0.7) | 96.3 # |
| Vitamin B12 (μg/day) | 1.4 ± 1.8 | 0.9 (0.4, 1.6) | 81.6 | 1.3 ± 1.7 | 0.8 (0.4, 1.5) | 82.8 |
| Vitamin C (mg/day) | 72.1 ± 40.5 | 65.2 (43.5, 92.5) | 69.5 | 62.4 ± 38.3 | 54.3 (35.7, 81.3) | 77.5 # |
| Folate (μg/day) & | 75.5 ± 62.5 | 60.6 (32.9, 101.9) | 99.4 | 69.9 ± 57.1 | 56.9 (30.4, 93.4) | 99.3 |
| Vitamin E (mg/day) *,& | 30.7 ± 38.1 | 24.1 (15.5, 36.1) | - | 24.4 ± 17.5 | 20.3 (13.1, 30.2) | - |
| Calcium (mg/day) | 342.4 ± 172.6 | 305.8 (225.1, 421.1) | 98.3 | 318.6 ± 168.5 | 281.5 (200.8, 401.2) | 97.9 |
| Potassium (mg/day) * | 1432 ± 549 | 1346 (1054, 1714) | - | 1256 ± 518 | 1165 (897, 1523) | - |
| Sodium (mg/day) * | 4784 ± 4833 | 3953 (2794, 5563) | - | 4345 ± 4283 | 3595 (2512, 5076) | - |
| Magnesium (mg/day) | 253.4 ± 90.7 | 239.9 (191.4, 300.3) | 66.1 | 221.3 ± 87.4 | 206.6 (160.6, 267.5) | 74.1 # |
| Iron (mg/day) | 18.5 ± 6.6 | 17.5 (14.1, 21.7) | 2.5 | 16.1 ± 6.4 | 15.1 (11.8, 19.1) | 6.9 # |
| Zinc (mg/day) | 9.3 ± 3.2 | 8.5 (6.8, 10.7) | 43.3 | 7.9 ± 3.2 | 7.4 (5.6, 9.6) | 57.0 # |
| Selenium (mg/day) | 38.4 ± 18.1 | 35.5 (26.4, 47.2) | 80.1 | 33.8 ± 16.2 | 31.0 (22.1, 41.6) | 85.7 # |
| North | South | |||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | |
| Vitamin A (μg/day) & | 308.2 ± 225.4 | 256.4 (152.7, 400.9) | 84.2 # | 440.8 ± 345.2 | 357.6 (212.5, 568.9) | 71.6 |
| Vitamin B1 (mg/day) | 0.8 ± 0.3 | 0.7 (0.5, 0.9) | 87.5 | 0.8 ± 0.3 | 0.7 (0.5, 0.9) | 87.7 |
| Vitamin B2 (mg/day) | 0.6 ± 0.3 | 0.6 (0.5, 0.8) | 94.8 # | 0.7 ± 0.3 | 0.6 (0.5, 0.8) | 93.5 |
| Vitamin B6 (mg/day) | 0.4 ± 0.3 | 0.3 (0.2, 0.5) | 99.0 # | 0.6 ± 0.4 | 0.6 (0.3, 0.9) | 92.4 |
| Vitamin B12 (μg/day) | 0.9 ± 1.0 | 0.6 (0.3, 1.1) | 88.2 # | 1.7 ± 2.3 | 1.1 (0.5, 2.0) | 77.4 |
| Vitamin C (mg/day) | 66.8 ± 39.3 | 59.3 (39.1, 85.8) | 74.4 # | 72.8 ± 39.3 | 65.8 (44.1, 93.7) | 68.7 |
| Folate (μg/day) & | 54.5 ± 37.2 | 46.7 (29.3, 70.1) | 99.9 # | 88.2 ± 71.7 | 75.3 (38.1, 117.9) | 99.0 |
| Vitamin E (mg/day) *,& | 33.6 ± 46.4 | 25.5 (17.1, 38.5) | - | 26.7 ± 24.1 | 21.7 (13.6, 32.7) | - |
| Calcium (mg/day) | 324.3 ± 158.2 | 290.3 (215.6, 398.7) | 98.6 # | 347.6 ± 181.5 | 309.4 (223.4, 430.7) | 97.9 |
| Potassium (mg/day) * | 1404 ± 541 | 1324 (1025, 1680) | - | 1396 ± 554 | 1312 (1014, 1679) | - |
| Sodium (mg/day) * | 4897 ± 5092 | 4079 (2878, 5706) | - | 4567 ± 4471 | 3757 (2667, 5293) | - |
| Magnesium (mg/day) | 258.7 ± 96.5 | 244.3 (192.2, 308.2) | 63.6 | 239.6 ± 86.2 | 226.6 (179.2, 285.4) | 70.3 # |
| Iron (mg/day) | 18.3 ± 6.7 | 17.1 (13.6, 21.1) | 3.4 | 18.1 ± 6.6 | 17.1 (13.7, 21.3) | 3.3 |
| Zinc (mg/day) | 8.1 ± 2.8 | 7.7 (6.2, 9.4) | 53.3 # | 9.3 ± 3.4 | 8.9 (6.9, 11.2) | 40.6 |
| Selenium (mg/day) | 38.2 ± 15.5 | 36.4 (27.3, 46.9) | 80.0 | 37.1 ± 19.3 | 33.7 (24.7, 45.4) | 81.9 # |
| Big Cities | Small and Medium-Sized Cities | Normal Rural | Poor Rural | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | Mean ± SD | Median (P25, P75) | Below EAR (%) | |
| Vitamin A (μg/day) &,$ | 468.6 ± 294.3 | 401.2 (264.6, 592.8) | 66.6 # | 430.1 ± 295.8 | 360.1 (228.6, 549.5) | 72.0 # | 342.5 ± 300.8 | 273.4 (166.8, 425.8) | 83.3 # | 246.3 ± 231.9 | 176.4 (100.9, 310.2) | 90.3 |
| Vitamin B1 (mg/day) | 0.8 ± 0.3 | 0.7 (0.5, 0.9) | 88.9 | 0.7 ± 0.3 | 0.7 (0.5, 0.8) | 91.1 # | 0.8 ± 0.3 | 0.7 (0.6, 1.1) | 85.5 | 0.8 ± 0.3 | 0.8 (0.6, 1.0) | 83.6 |
| Vitamin B2 (mg/day) $ | 0.8 ± 0.3 | 0.7 (0.6, 0.9) | 88.2 # | 0.7 ± 0.3 | 0.6 (0.5, 0.8) | 94.5 # | 0.6 ± 0.2 | 0.6 (0.4, 0.7) | 96.8 # | 0.5 ± 0.2 | 0.5 (0.4, 0.7) | 98.4 |
| Vitamin B6 (mg/day) $ | 0.5 ± 0.3 | 0.4 (0.3, 0.6) | 97.7 # | 0.5 ± 0.3 | 0.4 (0.2, 0.6) | 97.6 # | 0.6 ± 0.4 | 0.6 (0.3, 0.9) | 93.1 # | 0.6 ± 0.5 | 0.5 (0.2, 0.9) | 90.1 |
| Vitamin B12 (μg/day) $ | 1.8 ± 1.7 | 1.3 (0.8, 2.3) | 73.1 # | 1.6 ± 2.5 | 0.9 (0.5, 1.7) | 80.9 # | 1.2 ± 1.6 | 0.7 (0.4, 1.4) | 84.8 # | 0.6 ± 0.7 | 0.4 (0.2, 0.8) | 93.1 |
| Vitamin C (mg/day) $ | 76.9 ± 42.8 | 69.4 (47.3, 98.9) | 66.2 # | 72.4 ± 39.9 | 65.4 (43.6, 93.5) | 69.1 # | 66.2 ± 38.7 | 58.8 (39.6, 83.7) | 75.3 | 63.1 ± 37.1 | 56.1 (36.2, 83.6) | 74.9 |
| Folate (μg/day) & | 67.5 ± 48.8 | 57.3 (35.1, 87.3) | 99.6 | 62.8 ± 53.7 | 48.6 (27.3, 82.8) | 99.4 | 86.2 ± 73.2 | 75.3 (37.4, 113.9) | 99.0 # | 84.7 ± 67.1 | 67.1 (32.3, 120.9) | 99.7 |
| Vitamin E (mg/day) *,& | 27.5 ± 20.5 | 23.5 (16.2, 33.3) | - | 28.3 ± 21.7 | 23.2 (15.4, 35.2) | - | 28.1 ± 27.8 | 22.7 (14.2, 34.4) | - | 37.6 ± 30.7 | 24.1 (13.2, 40.2) | - |
| Calcium (mg/day) $ | 422.4 ± 193.7 | 393.1 (286.1, 516.1) | 96.5 # | 353.7 ± 172.8 | 320.4 (239.8, 431.6) | 97.9 # | 290.3 ± 129.3 | 265.6 (204.2, 346.7) | 99.3 # | 250.7 ± 116.9 | 226.6 (169.5, 308.1) | 99.7 |
| Potassium (mg/day) * | 1555 ± 596 | 1464 (1138, 1861) | - | 1366 ± 530 | 1300 (990, 1653) | - | 1351 ± 529 | 1261 (986, 1617) | - | 1277 ± 466 | 1220 (954, 1523) | - |
| Sodium (mg/day) * | 4287 ± 3489 | 3663 (2665, 5051) | - | 4668 ± 4784 | 3859 (2756, 5428) | - | 5063 ± 5739 | 4131 (2914, 5806) | - | 4823 ± 4517 | 3858 (2648, 5708) | - |
| Magnesium (mg/day) | 256.1 ± 95.3 | 241.5 (191.1, 303.1) | 64.3 | 236.3 ± 86.6 | 223.3 (175.5, 282.9) | 72.2 # | 244.1 ± 85.4 | 231.6 (184.4, 290.2) | 68.2 | 257.4 ± 97.8 | 243.6 (189.5, 304.8) | 64.1 |
| Iron (mg/day) | 19.1 ± 7.2 | 18.3 (14.3, 22.3) | 2.9 | 17.7 ± 6.4 | 16.7 (13.4, 20.7) | 3.4 | 17.6 ± 6.3 | 16.7 (13.3, 20.7) | 3.5 | 18.2 ± 6.3 | 17.2 (13.6, 21.5) | 3.6 |
| Zinc (mg/day) | 8.9 ± 3.1 | 8.5 (6.8, 10.5) | 42.6 | 8.6 ± 3.1 | 8.2 (6.4, 10.2) | 48.3 # | 8.8 ± 3.2 | 8.3 (6.6, 10.5) | 46.0 | 8.9 ± 3.6 | 8.3 (6.2, 11.2) | 46.9 |
| Selenium (mg/day) $ | 42.1 ± 17.7 | 39.2 (30.4, 50.8) | 74.9 # | 36.9 ± 17.9 | 34.3 (25.2, 44.9) | 82.8 # | 35.9 ± 18.8 | 33.2 (24.3, 44.3) | 83.3 # | 33.9 ± 14.5 | 31.3 (23.5, 41.7) | 85.2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Z.; Zhao, L.; Man, Q.; Wang, J.; Zhao, W.; Zhang, J. Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012. Nutrients 2019, 11, 1787. https://doi.org/10.3390/nu11081787
Liu Z, Zhao L, Man Q, Wang J, Zhao W, Zhang J. Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012. Nutrients. 2019; 11(8):1787. https://doi.org/10.3390/nu11081787
Chicago/Turabian StyleLiu, Zhen, Liyun Zhao, Qingqing Man, Jingzhong Wang, Wenhua Zhao, and Jian Zhang. 2019. "Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012" Nutrients 11, no. 8: 1787. https://doi.org/10.3390/nu11081787
APA StyleLiu, Z., Zhao, L., Man, Q., Wang, J., Zhao, W., & Zhang, J. (2019). Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012. Nutrients, 11(8), 1787. https://doi.org/10.3390/nu11081787