The Effects of Beetroot Juice on Blood Pressure, Microvascular Function and Large-Vessel Endothelial Function: A Randomized, Double-Blind, Placebo-Controlled Pilot Study in Healthy Older Adults


Abstract
:1. Introduction
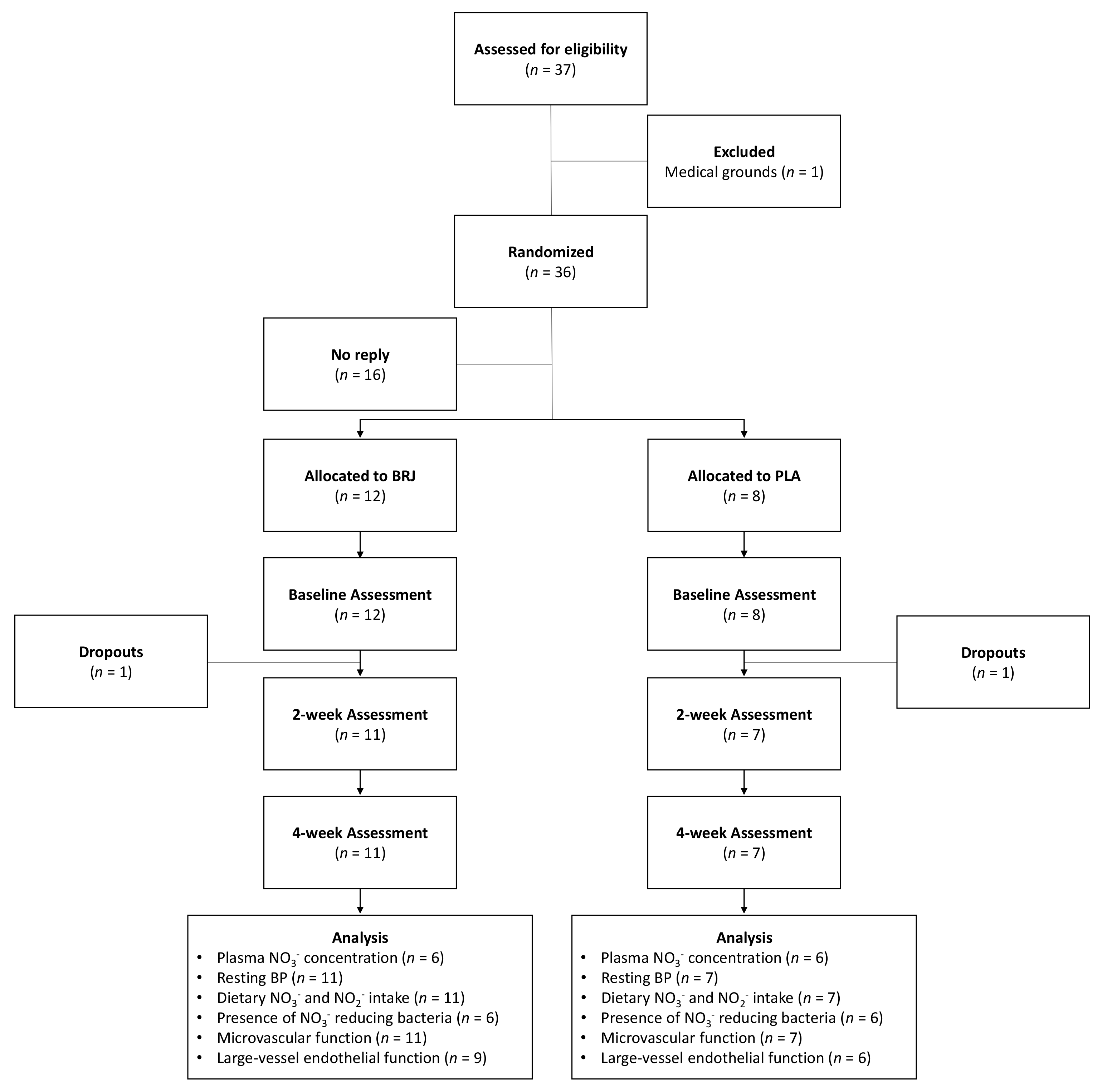
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Drink Intervention
2.4. Dietary NO3− and NO2− Intake
2.5. Presence of NO3− Bacteria
2.6. Microvascular Function
2.7. Large-Vessel Endothelial Function
2.8. Analysis of NO3− Concentration
2.9. Statistical Analysis
3. Results
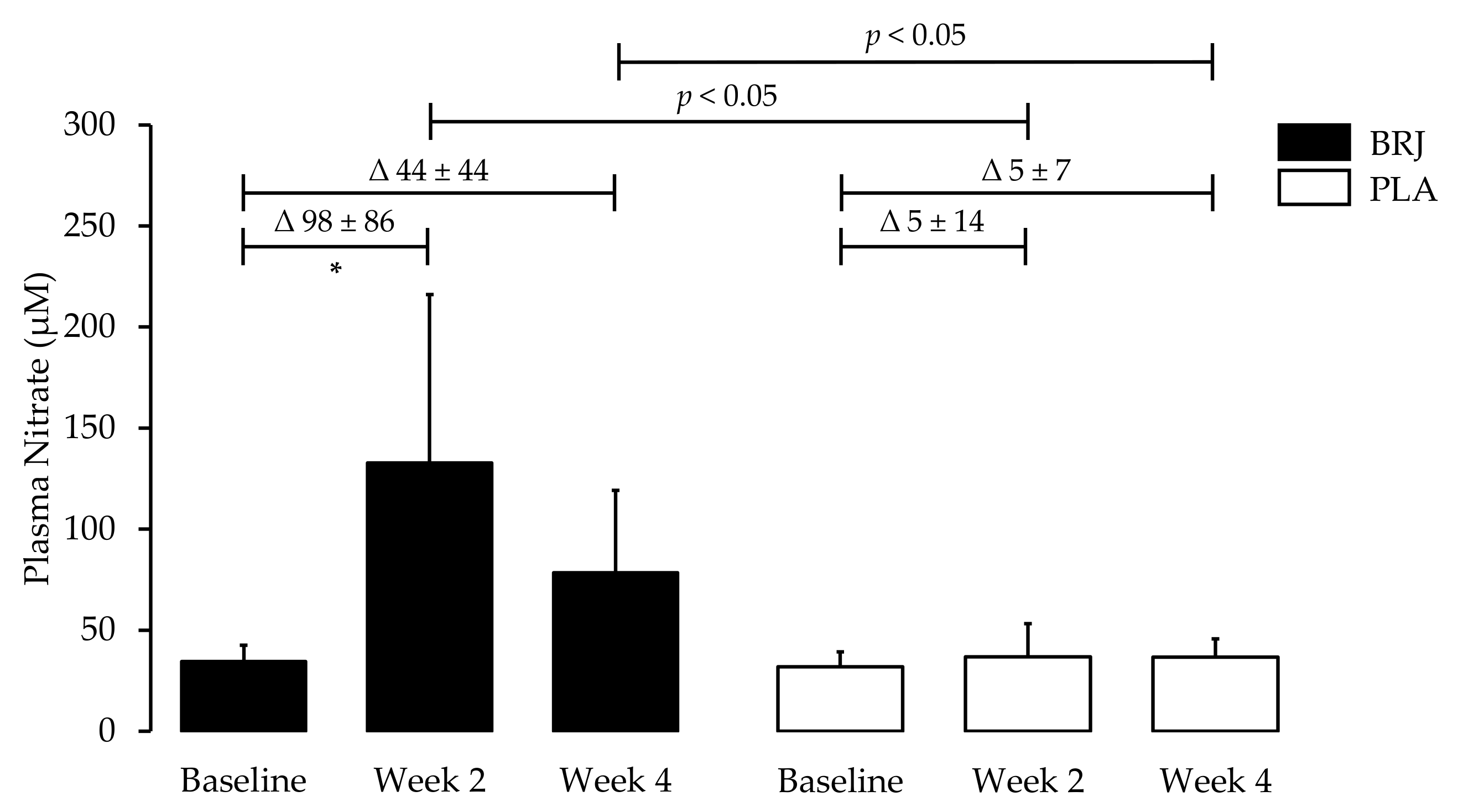
3.1. Plasma Nitrate Concentrations
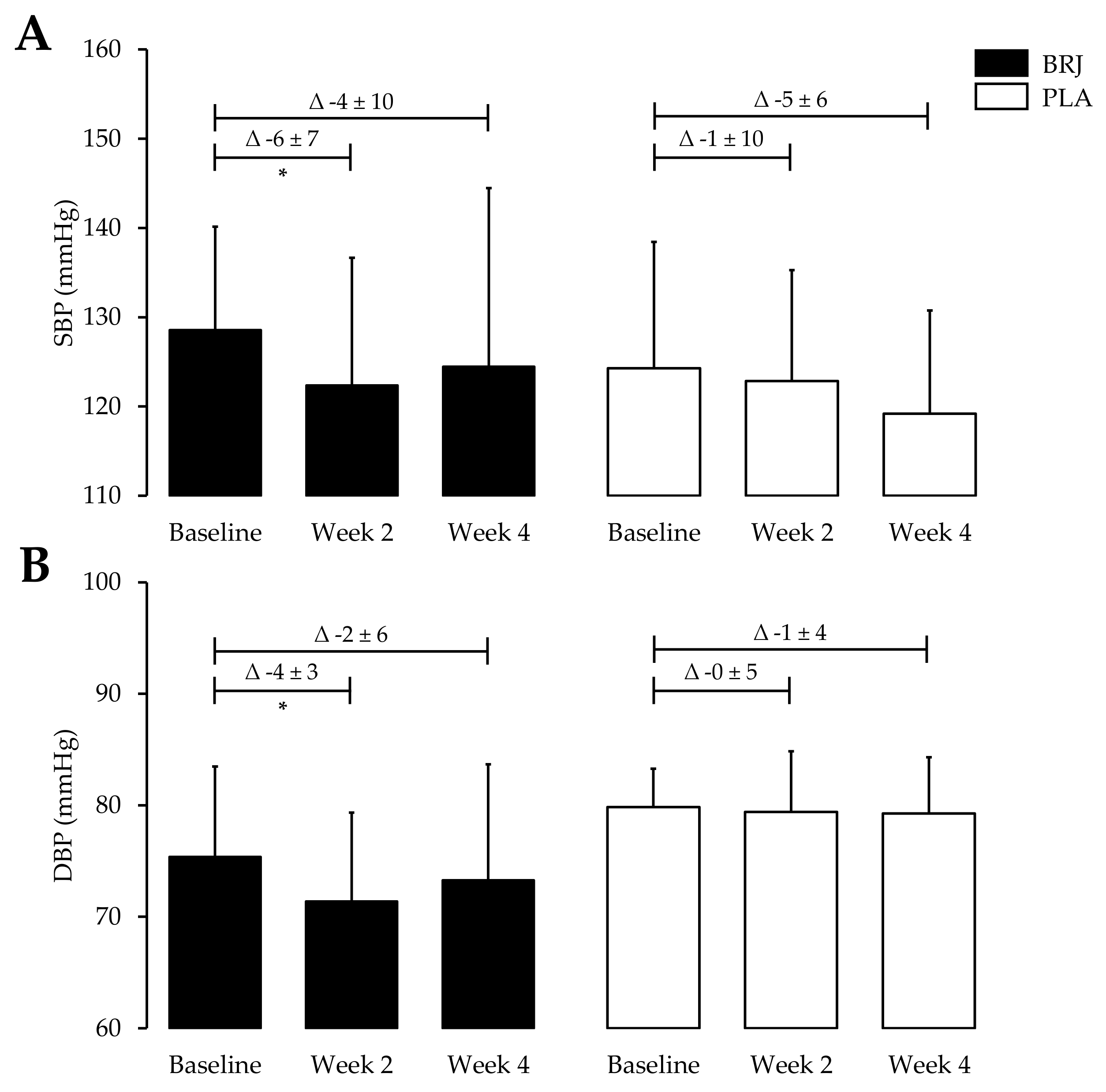
3.2. Resting Blood Pressure
3.3. Dietary NO3− and NO2− Intake
3.4. Presence of NO3− Reducing Bacteria
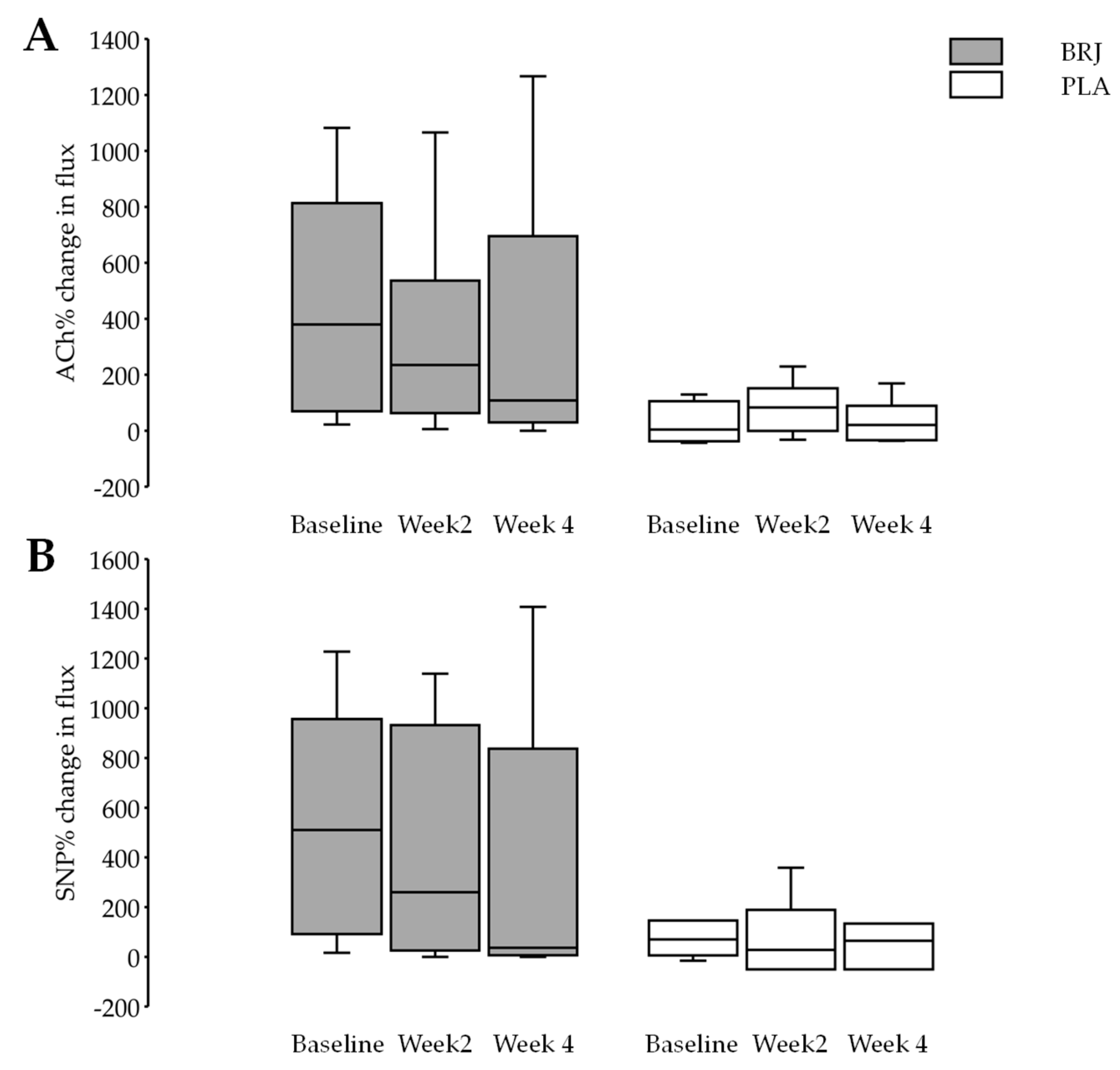
3.5. Microvascular Function
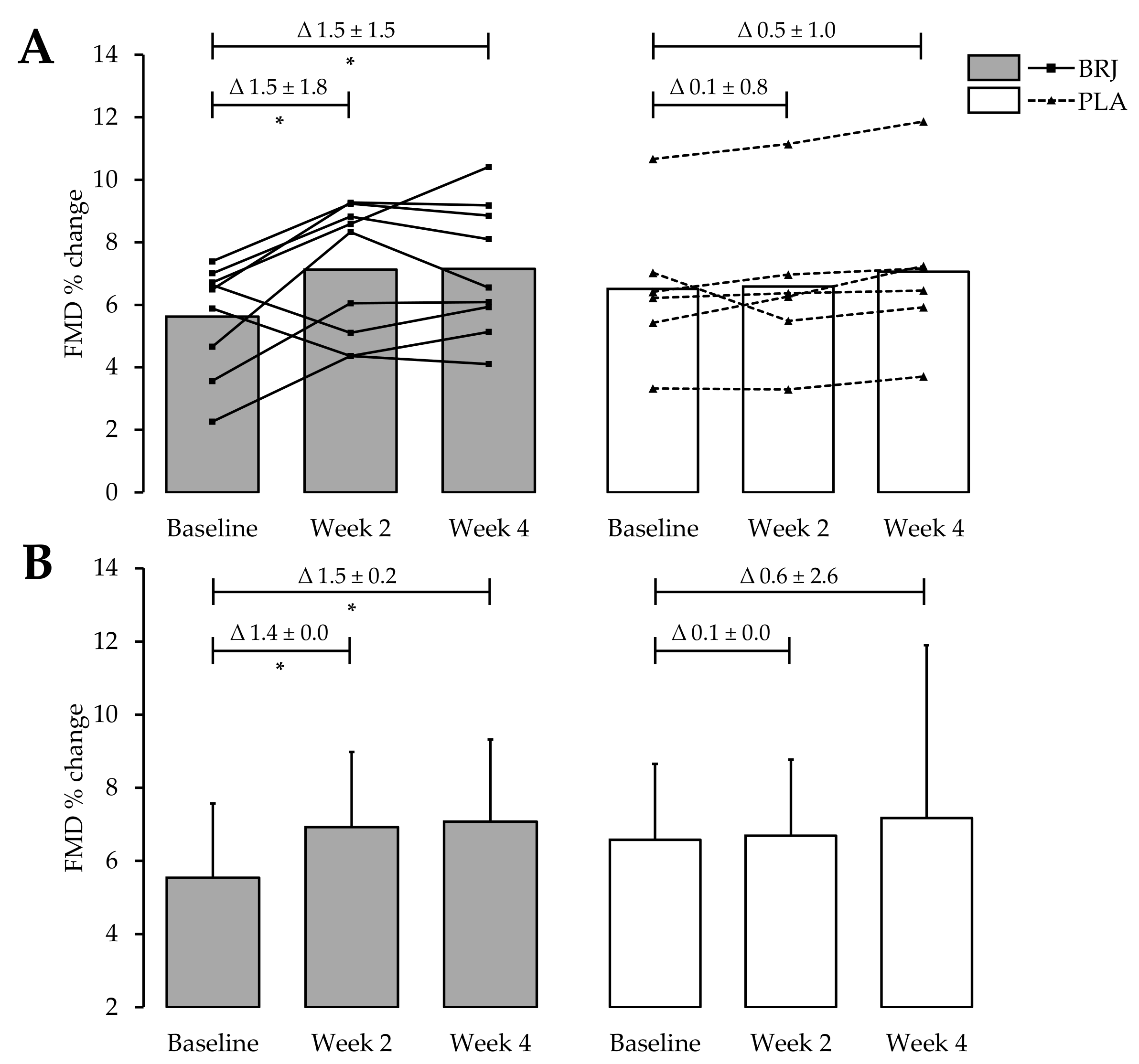
3.6. Large-Vessel Endothelial Function
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sandoo, A.; Veldhuijzen van Zanten, J.J.C.S.; Metsios, G.S.; Carroll, D.; Kitas, G.D. The Endothelium and Its Role in Regulating Vascular Tone. Open Cardiovasc. Med. J. 2010, 4, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Furchgott, R.F.; Zawadzki, J.V. The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature 1980, 288, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Seals, D.R.; Jablonski, K.L.; Donato, A.J. Aging and vascular endothelial function in humans. Clin. Sci. 2011, 120, 357–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sverdlov, A.L.; Ngo, D.T.M.; Chan, W.P.A.; Chirkov, Y.Y.; Horowitz, J.D. Aging of the Nitric Oxide System: Are We as Old as Our NO? J. Am. Heart Assoc. 2014, 3, e000973. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, N.; O’Driscoll, F.; Dougall, H.; Duncan, C.; Smith, L.; Golden, M.; McKenzie, H. Stomach NO synthesis. Nature 1994, 368, 502. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.O.; Govoni, M. Inorganic nitrate is a possible source for systemic generation of nitric oxide. Free Radic. Biol. Med. 2004, 37, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Cosby, K.; Partovi, K.S.; Crawford, J.H.; Patel, R.P.; Reiter, C.D.; Martyr, S.; Yang, B.K.; Waclawiw, M.A.; Zalos, G.; Xu, X.; et al. Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circulation. Nat. Med. 2003, 9, 1498–1505. [Google Scholar] [CrossRef]
- Shiva, S.; Huang, Z.; Grubina, R.; Sun, J.; Ringwood, L.A.; MacArthur, P.H.; Xu, X.; Murphy, E.; Darley-Usmar, V.M.; Gladwin, M.T. Deoxymyoglobin is a Nitrite Reductase That Generates Nitric Oxide and Regulates Mitochondrial Respiration. Circ. Res. 2007, 100, 654–661. [Google Scholar] [CrossRef]
- Webb, A.J.; Patel, N.; Loukogeorgakis, S.; Okorie, M.; Aboud, Z.; Misra, S.; Rashid, R.; Miall, P.; Deanfield, J.; Benjamin, N.; et al. Acute Blood Pressure Lowering, Vasoprotective, and Antiplatelet Properties of Dietary Nitrate via Bioconversion to Nitrite. Hypertension 2008, 51, 784–790. [Google Scholar] [CrossRef] [Green Version]
- Zweier, J.L.; Wang, P.; Samouilov, A.; Kuppusamy, P. Enzyme-independent formation of nitric oxide in biological tissues. Nat. Med. 1995, 1, 804–809. [Google Scholar] [CrossRef]
- Nohl, H.; Staniek, K.; Sobhian, B.; Bahrami, S.; Redl, H.; Kozlov, A.V. Mitochondria recycle nitrite back to the bioregulator nitric monoxide. Acta Biochim. Pol. 2000, 47, 913–921. [Google Scholar] [PubMed]
- Lundberg, J.O.; Weitzberg, E.; Gladwin, M.T. The nitrate–nitrite–nitric oxide pathway in physiology and therapeutics. Nat. Rev. Drug Discov. 2008, 7, 156–167. [Google Scholar] [CrossRef]
- Jackson, J.K.; Patterson, A.J.; MacDonald-Wicks, L.K.; Oldmeadow, C.; McEvoy, M.A. The role of inorganic nitrate and nitrite in cardiovascular disease risk factors: A systematic review and meta-analysis of human evidence. Nutr. Rev. 2018, 76, 348–371. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.H.; Bondonno, C.P.; Russell, J.; Flood, V.M.; Lewis, J.R.; Croft, K.D.; Woodman, R.J.; Lim, W.H.; Kifley, A.; Wong, G.; et al. Relationship of dietary nitrate intake from vegetables with cardiovascular disease mortality: A prospective study in a cohort of older Australians. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Bondonno, C.P.; Lewis, J.R.; Devine, A.; Woodman, R.J.; Croft, K.D.; Lim, W.H.; Wong, G.; Beilin, L.J.; Prince, R.L.; et al. Association of dietary nitrate with atherosclerotic vascular disease mortality: A prospective cohort study of older adult women. Am. J. Clin. Nutr. 2017, 106, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Capurso, C.; Massaro, M.; Scoditti, E.; Vendemiale, G.; Capurso, A. Vascular effects of the Mediterranean diet Part I: Anti-hypertensive and anti-thrombotic effects. Vascul. Pharmacol. 2014, 63, 118–126. [Google Scholar] [CrossRef]
- Sobko, T.; Marcus, C.; Govoni, M.; Kamiya, S. Dietary nitrate in Japanese traditional foods lowers diastolic blood pressure in healthy volunteers. Nitric Oxide 2010, 22, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Velmurugan, S.; Gan, J.M.; Rathod, K.S.; Khambata, R.S.; Ghosh, S.M.; Hartley, A.; Van Eijl, S.; Sagi-Kiss, V.; Chowdhury, T.A.; Curtis, M.; et al. Dietary nitrate improves vascular function in patients with hypercholesterolemia: A randomized, double-blind, placebo-controlled study. Am. J. Clin. Nutr. 2016, 103, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Kapil, V.; Khambata, R.S.; Robertson, A.; Caulfield, M.J.; Ahluwalia, A. Dietary Nitrate Provides Sustained Blood Pressure Lowering in Hypertensive Patients. Hypertension 2015, 65, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jajja, A.; Sutyarjoko, A.; Lara, J.; Rennie, K.; Brandt, K.; Qadir, O.; Siervo, M. Beetroot supplementation lowers daily systolic blood pressure in older, overweight subjects. Nutr. Res. 2014, 34, 868–875. [Google Scholar] [CrossRef]
- Khambata, R.S.; Ghosh, S.M.; Rathod, K.S.; Thevathasan, T.; Filomena, F.; Xiao, Q.; Ahluwalia, A. Antiinflammatory actions of inorganic nitrate stabilize the atherosclerotic plaque. Proc. Natl. Acad. Sci. USA 2017, 114, E550–E559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, S.M.; Kapil, V.; Fuentes-Calvo, I.; Bubb, K.J.; Pearl, V.; Milsom, A.B.; Khambata, R.; Maleki-Toyserkani, S.; Yousuf, M.; Benjamin, N.; et al. Enhanced Vasodilator Activity of Nitrite in Hypertension. Hypertension 2013, 61, 1091–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.; Fulford, J.; Vanhatalo, A.; Blackwell, J.R.; French, O.; Bailey, S.J.; Gilchrist, M.; Winyard, P.G.; Jones, A.M. Effects of short-term dietary nitrate supplementation on blood pressure, O2 uptake kinetics, and muscle and cognitive function in older adults. Am. J. Physiol. Integr. Comp. Physiol. 2013, 304, R73–R83. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, D.A.; Kaffa, N.; George, T.W.; Methven, L.; Lovegrove, J.A. Blood pressure-lowering effects of beetroot juice and novel beetroot-enriched bread products in normotensive male subjects. Br. J. Nutr. 2012, 108, 2066–2074. [Google Scholar] [PubMed] [Green Version]
- Kapil, V.; Milsom, A.B.; Okorie, M.; Maleki-Toyserkani, S.; Akram, F.; Rehman, F.; Arghandawi, S.; Pearl, V.; Benjamin, N.; Loukogeorgakis, S.; et al. Inorganic Nitrate Supplementation Lowers Blood Pressure in Humans. Hypertension 2010, 56, 274–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triggle, C.R.; Ding, H. The endothelium in compliance and resistance vessels. Front. Biosci. (Schol. Ed.) 2011, 3, 730–744. [Google Scholar] [PubMed]
- Houben, A.J.H.M.; Martens, R.J.H.; Stehouwer, C.D.A. Assessing Microvascular Function in Humans from a Chronic Disease Perspective. J. Am. Soc. Nephrol. 2017, 28, 3461–3472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aird, W.C. Phenotypic Heterogeneity of the Endothelium. Circ. Res. 2007, 100, 158–173. [Google Scholar] [CrossRef] [PubMed]
- Sandoo, A.; Carroll, D.; Metsios, G.S.; Kitas, G.D.; Veldhuijzen van Zanten, J.J. The association between microvascular and macrovascular endothelial function in patients with rheumatoid arthritis: A cross-sectional study. Arthritis Res. Ther. 2011, 13, R99. [Google Scholar] [CrossRef]
- Gilchrist, M.; Winyard, P.G.; Aizawa, K.; Anning, C.; Shore, A.; Benjamin, N. Effect of dietary nitrate on blood pressure, endothelial function, and insulin sensitivity in type 2 diabetes. Free Radic. Biol. Med. 2013, 60, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Roustit, M.; Cracowski, J.-L. Assessment of endothelial and neurovascular function in human skin microcirculation. Trends Pharmacol. Sci. 2013, 34, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Berry, M.J.; Justus, N.W.; Hauser, J.I.; Case, A.H.; Helms, C.C.; Basu, S.; Rogers, Z.; Lewis, M.T.; Miller, G.D. Dietary nitrate supplementation improves exercise performance and decreases blood pressure in COPD patients. Nitric Oxide 2015, 48, 22–30. [Google Scholar] [CrossRef] [PubMed]
- McMahon, N.; Pavey, T.; Desbrow, B.; Leveritt, M. Developing of a nitrate, nitrite, and nitrosamines food and beverage composition database for use with a food frequency questionnaire: A Systematic Review. Unpubl. Manuscr. 2017, 20 (suppl. 3), 22. [Google Scholar] [CrossRef]
- Griesenbeck, J.S.; Steck, M.D.; Huber, J.C.; Sharkey, J.R.; Rene, A.A.; Brender, J.D. Development of estimates of dietary nitrates, nitrites, and nitrosamines for use with the short willet food frequency questionnaire. Nutr. J. 2009, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Honikel, K.-O. The use and control of nitrate and nitrite for the processing of meat products. Meat Sci. 2008, 78, 68–76. [Google Scholar] [CrossRef]
- Walker, R. Nitrates, nitrites and N-nitrosocompounds: A review of the occurrence in food and diet and the toxicological implications. Food Addit. Contam. 1990, 7, 717–768. [Google Scholar] [CrossRef] [PubMed]
- Foodworks. Research Edition (v9) [Computer Software] Brisbane, Qld: Xyris Software. 2019. Available online: https://foodworks.com.au/ (accessed on 5 June 2019).
- Nutritics. Research Edition (v5.02) [Computer Software]. Dublin. 2018. Available online: www.nutritics.com (accessed on 5 June 2019).
- Schakel, S.F.; Buzzard, I.M.; Gebhardt, S.E. Procedures for Estimating Nutrient Values for Food Composition Databases. J. Food Compos. Anal. 1997, 10, 102–114. [Google Scholar] [CrossRef] [Green Version]
- Sandoo, A.; Kitas, G.D. A Methodological Approach to Non-invasive Assessments of Vascular Function and Morphology. J. Vis. Exp. 2015, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ndiaye, B.P.; Thienemann, F.; Ota, M.; Landry, B.S.; Camara, M.; Dièye, S.; Dieye, T.N.; Esmail, H.; Goliath, R.; Huygen, K.; et al. Safety, immunogenicity, and efficacy of the candidate tuberculosis vaccine MVA85A in healthy adults infected with HIV-1: A randomised, placebo-controlled, phase 2 trial. Lancet Respir. Med. 2015, 3, 190–200. [Google Scholar] [CrossRef]
- Rodriguez-Miguelez, P.; Seigler, N.; Harris, R.A. Ultrasound Assessment of Endothelial Function: A Technical Guideline of the Flow-mediated Dilation Test. J. Vis. Exp. 2016. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, D.H.J.; Black, M.A.; Pyke, K.E.; Padilla, J.; Atkinson, G.; Harris, R.A.; Parker, B.; Widlansky, M.E.; Tschakovsky, M.E.; Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. Am. J. Physiol. Circ. Physiol. 2011, 300, H2–H12. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Batterham, A.M. Allometric scaling of diameter change in the original flow-mediated dilation protocol. Atherosclerosis 2013, 226, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Granger, D.L.; Taintor, R.R.; Boockvar, K.S.; Hibbs, J.B. Measurement of nitrate and nitrite in biological samples using nitrate reductase and Griess reaction. Methods Enzymol. 1996, 268, 142–151. [Google Scholar] [PubMed]
- Miranda, K.M.; Espey, M.G.; Wink, D.A. A Rapid, Simple Spectrophotometric Method for Simultaneous Detection of Nitrate and Nitrite. Nitric Oxide 2001, 5, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, S.; Sattar, N.; Petrie, J.R.; Cobbe, S.M.; Ferrell, W.R. Reproducibility and repeatability of peripheral microvascular assessment using iontophoresis in conjunction with laser Doppler imaging. J. Cardiovasc. Pharmacol. 2007, 50, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Franklin, S.S.; Thijs, L.; Hansen, T.W.; O’Brien, E.; Staessen, J.A. White-Coat Hypertension. Hypertension 2013, 62, 982–987. [Google Scholar] [CrossRef]
- Siervo, M.; Lara, J.; Ogbonmwan, I.; Mathers, J.C. Inorganic Nitrate and Beetroot Juice Supplementation Reduces Blood Pressure in Adults: A Systematic Review and Meta-Analysis. J. Nutr. 2013, 143, 818–826. [Google Scholar] [CrossRef]
- Carlström, M.; Lundberg, J.O.; Weitzberg, E. Mechanisms underlying blood pressure reduction by dietary inorganic nitrate. Acta Physiol. 2018, 224, e13080. [Google Scholar] [CrossRef]
- Bond, V.; Curry, B.H.; Adams, R.G.; Asadi, M.S.; Millis, R.M.; Haddad, G.E. Effects of Dietary Nitrates on Systemic and Cerebrovascular Hemodynamics. Cardiol. Res. Pract. 2013, 2013, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Pries, A.R.; Secomb, T.W.; Gaehtgens, P. Structural Autoregulation of Terminal Vascular Beds. Hypertension 1999, 33, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, B.J.; Keen, J.T.; Levitt, E.L. Cutaneous reactive hyperaemia is unaltered by dietary nitrate supplementation in healthy humans. Clin. Physiol. Funct. Imaging 2018, 38, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, S.; Minson, C.T. Human cutaneous reactive hyperaemia: Role of BK Ca channels and sensory nerves. J. Physiol. 2007, 585, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.; Belch, J.J.F.; Khan, F. Current Concepts in Assessment of Microvascular Endothelial Function Using Laser Doppler Imaging and Iontophoresis. Trends Cardiovasc. Med. 2008, 18, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Marsch, E.; Theelen, T.L.; Janssen, B.J.A.; Briede, J.J.; Haenen, G.R.; Senden, J.M.G.; van Loon, L.J.C.; Poeze, M.; Bierau, J.; Gijbels, M.J.; et al. The effect of prolonged dietary nitrate supplementation on atherosclerosis development. Atherosclerosis 2016, 245, 212–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Allocation | BRJ | PLA | Significance |
|---|---|---|---|
| Demographics | |||
| n | 11 | 7 | |
| Age (y) | 65 ± 8 | 61 ± 5 | 0.34 |
| Height (cm) | 167.4 ± 9.5 | 165.3 ± 6.2 | 0.62 |
| Weight (kg) | 73.2 ± 16.6 | 73.3 ± 8.0 | 0.99 |
| BMI (kg/m2) | 26.2 ± 6.3 | 26.9 ± 2.1 | 0.80 |
| Body Fat (%) | 30.7 ± 10.5 | 33.8 ± 7.7 | 0.51 |
| Dietary Intake | |||
| NO3− | 151.8 ± 77.8 | 185.3 ± 75.7 | 0.78 |
| NO2− | 7.4 ± 3.8 | 5.8 ± 1.9 | 0.49 |
| Clinical BP | |||
| SBP | 129 ± 12 | 124 ± 14 | 0.46 |
| DBP | 75 ± 8 | 79 ± 3 | 0.23 |
| BRJ | PLA | P (Comparison between BRJ and PLA) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 2 | Week 4 | ∆ Week 2 − Baseline | ∆ Week 4 − Week 2 | ∆ Week 4 − Baseline | Baseline | Week 2 | Week 4 | ∆ Week 2 − Baseline | ∆ Week 4 − Week 2 | ∆ Week 4 − Baseline | ∆ Week 2 − Baseline | ∆ Week 4 − Week 2 | ∆ Week 4 − Baseline | |
| SBP (mmHg) | 129 ± 12 | 122 ± 14 | 124 ± 20 | −6 ± 7 | 2 ± 7 | −4 ± 10 | 124 ± 14 | 123 ± 12 | 119 ± 11 | −1 ± 10 | −4 ± 7 | −5 ± 6 | 0.23 | 0.12 | 0.84 |
| DBP (mmHg) | 75 ± 8 | 71 ± 8 | 73 ± 10 | −4 ± 3 | 2 ± 4 | −2 ± 6 | 79 ± 3 | 79 ± 5 | 79 ± 5 | 0 ± 5 | 0 ± 3 | −1 ± 4 | 0.08 | 0.29 | 0.55 |
| ACh (%) | 447.30 ± 364.82 | 304.59 ± 326.87 | 343.65 ± 425.80 | −142.71 ± 295.97 | 39.05 ± 411.12 | −103.66 ± 340.20 | 66.16 ± 65.02 | 116.30 ± 88.28 | 68.58 ± 71.58 | 50.14 ± 142.28 | −47.72 ± 143.64 | 2.42 ± 71.20 | 0.13 | 0.60 | 0.43 |
| SNP (%) | 537.53 ± 434.81 | 449.00 ± 451.84 | 358.91 ± 534.79 | −88.54 ± 341.96 | −90.09 ± 497.00 | −178.62 ± 357.99 | 216.99 ± 305.40 | 122.15 ± 143.08 | 171.28 ± 279.98 | −98.84 ± 373.01 | 49.13 ± 364.91 | −45.71 ± 394.21 | 0.97 | 0.53 | 0.47 |
| FMD (%) | 5.26 ± 1.75 | 7.12 ± 2.12 | 7.15 ± 2.09 | 1.50 ± 1.81 | 0.02 ± 1.03 | 1.53 ± 1.49 | 6.38 ± 2.36 | 6.45 ± 2.52 | 6.91 ± 2.63 | 0.07 ± 0.83 | 0.46 ± 0.33 | 0.54 ± 0.97 | 0.10 | 0.34 | 0.18 |
| Treatment Allocation | BRJ | PLA | Significance |
|---|---|---|---|
| NO3− (mg) | |||
| Baseline | 151.8 ± 77.8 | 185.3 ± 75.7 | 1.00 |
| WK2 | 182.5 ± 72.4 | 200.2 ± 63.2 | 0.66 |
| WK4 | 195.4 ± 66.9 | 190.4 ± 113.6 | 0.47 |
| NO2− (mg) | |||
| Baseline | 7.4 ± 3.8 | 5.8 ± 1.9 | 0.12 |
| WK2 | 6.2 ± 4.0 | 8.2 ± 2.9 | 0.43 |
| WK4 | 8.1 ± 4.4 | 5.1 ± 2.3 | 0.07 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, T.; Dunn, E.L.; Macdonald, J.H.; Kubis, H.-P.; McMahon, N.; Sandoo, A. The Effects of Beetroot Juice on Blood Pressure, Microvascular Function and Large-Vessel Endothelial Function: A Randomized, Double-Blind, Placebo-Controlled Pilot Study in Healthy Older Adults. Nutrients 2019, 11, 1792. https://doi.org/10.3390/nu11081792
Jones T, Dunn EL, Macdonald JH, Kubis H-P, McMahon N, Sandoo A. The Effects of Beetroot Juice on Blood Pressure, Microvascular Function and Large-Vessel Endothelial Function: A Randomized, Double-Blind, Placebo-Controlled Pilot Study in Healthy Older Adults. Nutrients. 2019; 11(8):1792. https://doi.org/10.3390/nu11081792
Chicago/Turabian StyleJones, Tomos, Emily Louise Dunn, Jamie Hugo Macdonald, Hans-Peter Kubis, Nicholas McMahon, and Aamer Sandoo. 2019. "The Effects of Beetroot Juice on Blood Pressure, Microvascular Function and Large-Vessel Endothelial Function: A Randomized, Double-Blind, Placebo-Controlled Pilot Study in Healthy Older Adults" Nutrients 11, no. 8: 1792. https://doi.org/10.3390/nu11081792
APA StyleJones, T., Dunn, E. L., Macdonald, J. H., Kubis, H. -P., McMahon, N., & Sandoo, A. (2019). The Effects of Beetroot Juice on Blood Pressure, Microvascular Function and Large-Vessel Endothelial Function: A Randomized, Double-Blind, Placebo-Controlled Pilot Study in Healthy Older Adults. Nutrients, 11(8), 1792. https://doi.org/10.3390/nu11081792