Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults


Abstract
:1. Introduction
2. Materials and Methods
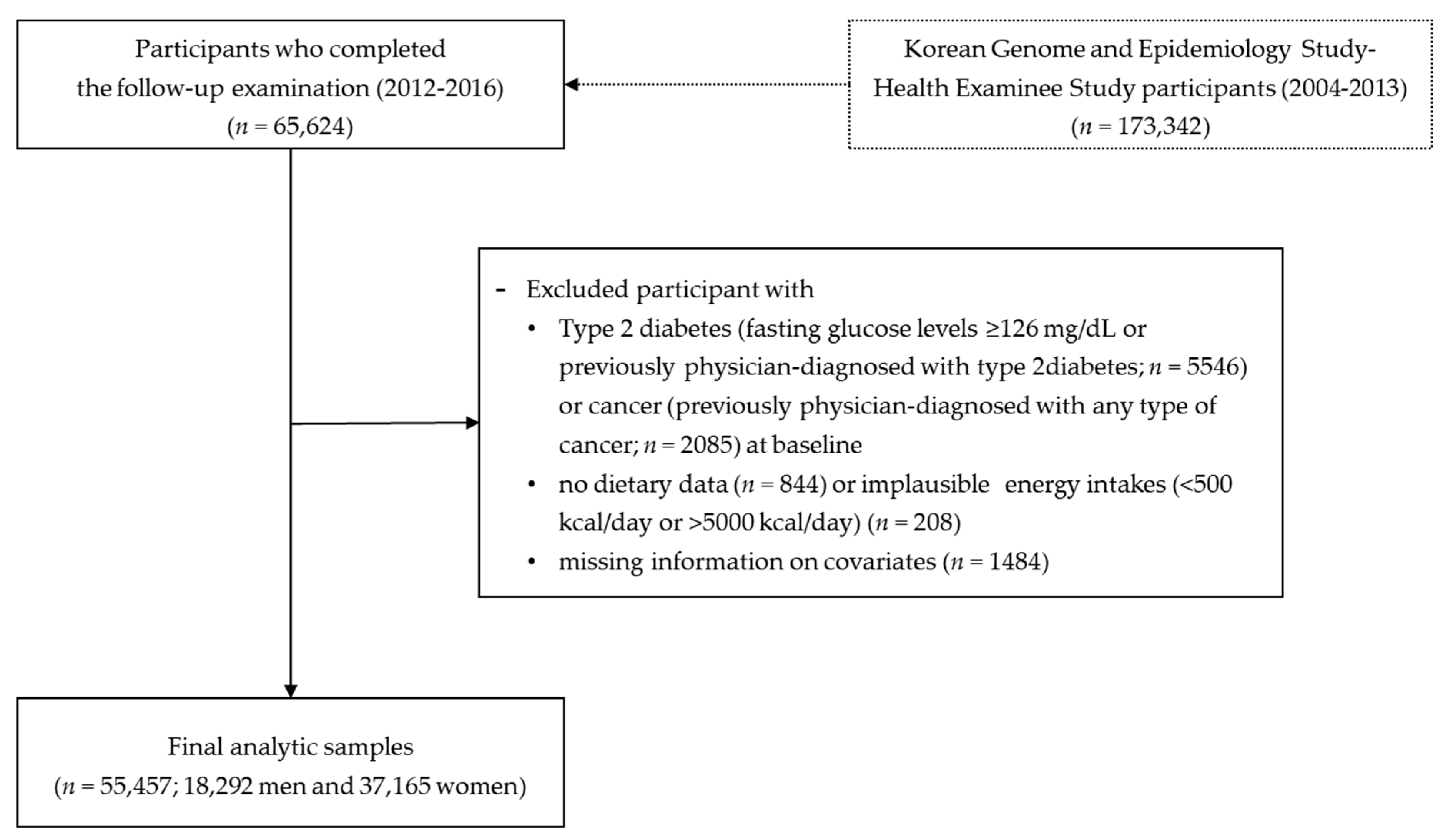
2.1. Data Source and Study Population
2.2. Dietary Assessment
2.3. Outcome Variable
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Korean Ministry of Health and Welfare; Korea Centers for Disease Control and Prevention. Korea Health Statistics 2016: Korea National Health and Nutrition Examination Survey (KNHANES VII-1); Korea Centers for Disease Control and Prevention: Cheongju, Korea, 2017.
- Cho, N.H. Diabetes burden and prevention in Korea and the Western Pacific Region. Diabetes Res. Clin. Pract. 2014, 106, S282–S287. [Google Scholar] [CrossRef]
- Qin, J.; Li, Y.; Cai, Z.; Li, S.; Zhu, J.; Zhang, F.; Liang, S.; Zhang, W.; Guan, Y.; Shen, D. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature 2012, 490, 55–60. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015; Available online: http://www.diabetesatlas.org (accessed on 10 February 2019).
- Bazzano, L.A.; Li, T.Y.; Joshipura, K.J.; Hu, F.B. Intake of fruit, vegetables, and fruit juices and risk of diabetes in women. Diabetes Care 2008, 31, 1311–1317. [Google Scholar] [CrossRef]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Song, Y.; Lee, K.H.; Lee, H.S.; Lee, M.; Jee, S.H.; Joung, H. A fruit and dairy dietary pattern is associated with a reduced risk of metabolic syndrome. Metabolism 2012, 61, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Woo, H.D.; Lee, J.H.; Kim, J. Dietary patterns and risk for metabolic syndrome in Korean women: A cross-sectional study. Medicine 2015, 94, e1424. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.J.; Cho, E.; Lee, H.J.; Fung, T.T.; Rimm, E.; Rosner, B.; Manson, J.E.; Wheelan, K.; Hu, F.B. Instant noodle intake and dietary patterns are associated with distinct cardiometabolic risk factors in Korea. J. Nutr. 2014, 144, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Arganini, C.; Saba, A.; Comitato, R.; Virgili, F.; Turrini, A. Gender differences in food choice and dietary intake in modern western societies. In Public Healtn—Social and Behavioral Health; Maddock, J., Ed.; IntechOpen: London, UK, 2012; Available online: http://www.intechopen.com/books/public-health/gender-differences-in-foodchoice-and-dietary-intake-in-modern-western-societies (accessed on 22 April 2019).
- Eshak, E.S.; Iso, H.; Mizoue, T.; Inoue, M.; Noda, M.; Tsugane, S. Soft drink, 100% fruit juice, and vegetable juice intakes and risk of diabetes mellitus. Clin. Nutr. 2013, 32, 300–308. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.; KoGES group. Cohort profile: The Korean genome and epidemiology study (KoGES) Consortium. Int. J. Epidemiol. 2016, 46, e20. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- The Korean Nutrition Society. Dietary Reference Intakes for Koreans; Hanareum Press: Seoul, Korea, 2015. [Google Scholar]
- Shin, S.; Joung, H. A dairy and fruit dietary pattern is associated with a reduced likelihood of osteoporosis in Korean postmenopausal women. Br. J. Nutr. 2013, 110, 1926–1933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Yu, A.; Choi, B.Y.; Nam, J.H.; Kim, M.K.; Oh, D.H.; Yang, Y.J. Dietary patterns derived by cluster analysis are associated with cognitive function among Korean older adults. Nutrients 2015, 7, 4154–4169. [Google Scholar] [CrossRef] [PubMed]
- Montonen, J.; Knekt, P.; Härkänen, T.; Järvinen, R.; Heliövaara, M.; Aromaa, A.; Reunanen, A. Dietary patterns and the incidence of type 2 diabetes. Am. J. Epidemiol. 2005, 161, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, A.; Ohno, Y.; Tatsumi, Y.; Mizuno, S.; Watanabe, S. Effects of healthy dietary pattern and other lifestyle factors on incidence of diabetes in a rural Japanese population. Asia Pac. J. Clin. Nutr. 2012, 21, 601–608. [Google Scholar] [PubMed]
- Odegaard, A.O.; Koh, W.P.; Butler, L.M.; Duval, S.; Gross, M.D.; Mimi, C.Y.; Yuan, J.M.; Pereira, M.A. Dietary patterns and incident type 2 diabetes in Chinese men and women: The Singapore Chinese Health Study. Diabetes Care 2011, 34, 880–886. [Google Scholar] [CrossRef]
- Cooper, A.J.; Sharp, S.J.; Lentjes, M.A.; Luben, R.N.; Khaw, K.T.; Wareham, N.J.; Forouhi, N.G. A prospective study of the association between quantity and variety of fruit and vegetable intake and incident type 2 diabetes. Diabetes Care 2012, 35, 1293–1300. [Google Scholar] [CrossRef]
- Li, M.; Fan, Y.; Zhang, X.; Hou, W.; Tang, Z. Fruit and vegetable intake and risk of type 2 diabetes mellitus: Meta-analysis of prospective cohort studies. BMJ Open 2014, 4, e005497. [Google Scholar] [CrossRef]
- Yao, B.; Fang, H.; Xu, W.; Yan, Y.; Xu, H.; Liu, Y.; Mo, M.; Zhang, H.; Zhao, Y. Dietary fiber intake and risk of type 2 diabetes: A dose–response analysis of prospective studies. Eur. J. Epidemiol. 2014, 29, 79–88. [Google Scholar] [CrossRef]
- Chatterjee, R.; Colangelo, L.; Yeh, H.; Anderson, C.; Daviglus, M.; Liu, K.; Brancati, F. Potassium intake and risk of incident type 2 diabetes mellitus: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Diabetologia 2012, 55, 1295–1303. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, H.C.; Vitek, L.; Nam, C.M. Algae consumption and risk of type 2 diabetes: Korean National Health and Nutrition Examination Survey in 2005. J. Nutr. Sci. Vitaminol. 2010, 56, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, J.Y.; Choi, W.H.; Lee, S.S. Effects of seaweed supplementation on blood glucose concentration, lipid profile, and antioxidant enzyme activities in patients with type 2 diabetes mellitus. Nutr. Res. Pract. 2008, 2, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, X.; Dong, J.; Wu, Z.; Li, W.; Qin, L. Dairy consumption and risk of type 2 diabetes mellitus: A meta-analysis of cohort studies. Eur. J. Clin. Nutr. 2011, 65, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Schulze, M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dietary patterns, meat intake, and the risk of type 2 diabetes in women. Ann. Int. Med. 2004, 164, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- van Dam, R.M.; Rimm, E.B.; Willett, W.C.; Stampfer, M.J.; Hu, F.B. Dietary patterns and risk for type 2 diabetes mellitus in US men. Ann. Int. Med. 2002, 136, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Schoenaker, D.A.; Dobson, A.J.; Soedamah-Muthu, S.S.; Mishra, G.D. Factor analysis is more appropriate to identify overall dietary patterns associated with diabetes when compared with Treelet transform analysis. J. Nutr. 2013, 143, 392–398. [Google Scholar] [CrossRef]
- Fernandes, A.C.; Medeiros, C.O.; Bernardo, G.L.; Ebone, M.V.; Di Pietro, P.F.; Assis, M.A.; Vasconcelos, F.D. Benefits and risks of fish consumption for the human health. Rev. Nutr. 2012, 25, 283–295. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B.; Bronner, L.; Willett, W.C.; Stampfer, M.J.; Rexrode, K.M.; Albert, C.M.; Hunter, D.; Manson, J.E. Fish and omega-3 fatty acid intake and risk of coronary heart disease in women. JAMA 2002, 287, 1815–1821. [Google Scholar] [CrossRef]
- Koh, A.S.; Pan, A.; Wang, R.; Odegaard, A.O.; Pereira, M.A.; Yuan, J.M.; Koh, W.P. The association between dietary omega-3 fatty acids and cardiovascular death: The Singapore Chinese Health Study. Eur. J. Prev. Cardiol. 2015, 22, 364–372. [Google Scholar] [CrossRef]
- Lohmann, R.; Breivik, K.; Dachs, J.; Muir, D. Global fate of POPs: Current and future research directions. Environ. Pollut. 2007, 150, 150–165. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, I.K.; Jin, S.H.; Steffes, M.; Jacobs, D.R. Association between serum concentrations of persistent organic pollutants and insulin resistance among nondiabetic adults: Results from the National Health and Nutrition Examination Survey 1999–2002. Diabetes Care 2007, 30, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, R.; Rantakokko, P.; Eriksson, J.G.; Blomstedt, P.; Kajantie, E.; Kiviranta, H. Association between type 2 diabetes and exposure to persistent organic pollutants. Diabetes Care 2011, 34, 1972–1979. [Google Scholar] [CrossRef] [PubMed]
- Leblanc, V.; Bégin, C.; Corneau, L.; Dodin, S.; Lemieux, S. Gender differences in dietary intakes: What is the contribution of motivational variables? J. Hum. Nutr. Diet. 2015, 28, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisie, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H. Fruit and vegetable consumption and diabetes mellitus incidence among US adults. Prev. Med. 2001, 32, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Mather, K.; Kim, C.; Christophi, C.; Aroda, V.; Knowler, W.; Edelstein, S.; Florez, J.; Labrie, F.; Kahn, S.; Goldberg, R. Steroid Sex Hormones, Sex Hormone–Binding Globulin, and Diabetes Incidence in the Diabetes Prevention Program. J. Clin. Endocrinol. Metab. 2015, 100, 3778–3786. [Google Scholar] [CrossRef] [PubMed]
- Laaksonen, D.E.; Niskanen, L.; Punnonen, K.; Nyyssönen, K.; Tuomainen, T.P.; Valkonen, V.P.; Salonen, R.; Salonen, J.T. Testosterone and sex hormone–binding globulin predict the metabolic syndrome and diabetes in middle-aged men. Diabetes Care 2004, 27, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Barrett-Connor, E.; Wedick, N.M.; Wingard, D.L. Endogenous sex hormones and the development of type 2 diabetes in older men and women: The Rancho Bernardo study. Diabetes Care 2002, 25, 55–60. [Google Scholar] [CrossRef]
- Goodman-Gruen, D.; Barrett-Connor, E. Sex differences in the association of endogenous sex hormone levels and glucose tolerance status in older men and women. Diabetes Care 2000, 23, 912–918. [Google Scholar] [CrossRef]
- Shungin, D.; Winkler, T.W.; Croteau-Chonka, D.C.; Ferreira, T.; Locke, A.E.; Mägi, R.; Strawbridge, R.J.; Pers, T.H.; Fischer, K.; Justice, A.E. New genetic loci link adipose and insulin biology to body fat distribution. Nature 2015, 518, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Tucker, K.L. Dietary patterns, approaches, and multicultural perspective. Appl. Physiol. Nutr. Metab. 2010, 35, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Michels, K.B.; Schulze, M.B. Can dietary patterns help us detect diet–disease associations? Nutr. Res. Rev. 2005, 18, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Olendzki, B.; Procter-Gray, E.; Magee, M.F.; Youssef, G.; Kane, K.; Churchill, L.; Ockene, J.; Li, W. Racial differences in misclassification of healthy eating based on food frequency questionnaire and 24-hour dietary recalls. J. Nutr. Health Aging 2017, 21, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Lyu, J.; Park, J.K.; Jo, C.; Kim, S.S. Dietary carbohydrate quality and quantity in relation to the incidence of type 2 diabetes: A prospective cohort study of middle-aged and older Korean adults. Nutrition 2019, 57, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.Y.; Kim, M.K.; Jung, S.; Shin, J.; Choi, B.Y. The cross-sectional relationships of dietary and serum vitamin D with cardiometabolic risk factors: Metabolic components, subclinical atherosclerosis, and arterial stiffness. Nutrition 2016, 32, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Dekker, L.H.; Boer, J.M.; Stricker, M.D.; Busschers, W.B.; Snijder, M.B.; Nicolaou, M.; Verschuren, W.M. Dietary patterns within a population are more reproducible than those of individuals. J. Nutr. 2013, 143, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.; Weismayer, C.; Akesson, A.; Tucker, K.L.; Wolk, A. Long-term stability of food patterns identified by use of factor analysis among Swedish women. J. Nutr. 2006, 136, 626–633. [Google Scholar] [CrossRef]
- Abdul-Ghani, M.; DeFronzo, R. Plasma glucose concentration and prediction of future risk of type 2 diabetes. Diabetes Care 2009, 32, S194–S198. [Google Scholar] [CrossRef]


{kind=link}
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
| “Prudent” Pattern | “Fatty Fish, Meat, and Flour-Based Food” Pattern | “Coffee and Sweets” Pattern | “Whole Grain” Pattern | “Prudent” Pattern | “Fatty Fish, Meat, and Flour-Based Food” Pattern | “Coffee and Sweets” Pattern | “White Rice” Pattern | |
| Light-colored vegetables | 0.702 b | 0.678 | ||||||
| Green/yellow vegetables | 0.699 | 0.732 | ||||||
| Lean fish | 0.607 | 0.539 | ||||||
| Seaweeds | 0.599 | 0.599 | ||||||
| Mushrooms | 0.551 | 0.562 | ||||||
| Shellfish | 0.517 | 0.426 | ||||||
| Kimchi | 0.501 | 0.430 | ||||||
| Bone fish | 0.493 | 0.531 | ||||||
| Pickled vegetables | 0.429 | 0.342 | ||||||
| Fruits | 0.412 | 0.457 | ||||||
| Tubers | 0.393 | 0.451 | ||||||
| Legumes and soy products | 0.353 | 0.479 | ||||||
| Milk | 0.323 | 0.324 | ||||||
| Salt-fermented fish | 0.307 | |||||||
| Yogurt | 0.333 | |||||||
| Fatty fish | 0.583 | 0.318 | 0.505 | |||||
| Pizza/hamburger | 0.563 | 0.482 | ||||||
| Processed meats | 0.550 | 0.533 | ||||||
| High-fat red meat | 0.481 | 0.569 | ||||||
| Bread | 0.471 | 0.486 | ||||||
| Poultry | 0.466 | 0.496 | ||||||
| Red meat by-products | 0.460 | 0.475 | ||||||
| Cake/snack/cookie | 0.456 | 0.475 | ||||||
| Noodles/dumpling | 0.405 | 0.404 | ||||||
| Dairy products | 0.404 | |||||||
| Other seafood | 0.384 | 0.418 | ||||||
| Carbonated beverages | 0.381 | 0.331 | ||||||
| Red meat | 0.327 | 0.310 | ||||||
| Sweets | 0.896 | 0.861 | ||||||
| Oils/fats | 0.894 | 0.864 | ||||||
| Coffee | 0.848 | 0.785 | ||||||
| Whole grain | 0.858 | −0.902 | ||||||
| White rice | −0.878 | 0.916 | ||||||
| Variance of intake explained (%) | 11.68 | 7.79 | 6.42 | 5.29 | 11.59 | 7.60 | 5.94 | 4.68 |
| Cumulative variance of intake explained (%) | 11.68 | 19.47 | 25.88 | 31.17 | 11.59 | 19.19 | 25.13 | 29.81 |
| Quintile (Q) of Dietary Pattern Score | p-Value b | |||
|---|---|---|---|---|
| Q1 (Lowest) | Q3 | Q5 (Highest) | ||
| “Prudent” pattern | ||||
| Age, years | 53.4 ± 8.7 a | 54.9 ± 8.4 | 55.4 ± 8.3 | <0.0001 |
| Education, college or higher, % | 43.9 | 45.2 | 47.6 | <0.0001 |
| Current smokers, % | 27.8 | 26.1 | 27.3 | 0.9834 |
| Alcohol, g/day | 13.9 ± 24.4 | 15.5 ± 24.5 | 18.7 ± 30.6 | <0.0001 |
| Regular physical activity, % | 53.7 | 59.9 | 65.5 | <0.0001 |
| Family history of diabetes, % | 14.9 | 13.6 | 13.0 | 0.0227 |
| Body mass index, kg/m2 | 24.2 ± 2.7 | 24.3 ± 2.7 | 24.5 ± 2.6 | <0.0001 |
| “Fatty fish, meat, and flour-based food” pattern | ||||
| Age, years | 58.7 ± 7.4 | 54.8 ± 7.9 | 50.2 ± 8.3 | <0.0001 |
| Education, college or higher, % | 35.0 | 43.9 | 56.0 | <0.0001 |
| Current smokers, % | 22.3 | 26.9 | 32.8 | <0.0001 |
| Alcohol, g/day | 13.6 ± 25.4 | 16.8 ± 27.1 | 18.6 ± 30.5 | <0.0001 |
| Regular physical activity, % | 59.2 | 59.3 | 57.2 | 0.0261 |
| Family history of diabetes, % | 11.3 | 13.0 | 16.9 | <0.0001 |
| Body mass index, kg/m2 | 24.1 ± 2.6 | 24.3 ± 2.6 | 24.6 ± 2.8 | <0.0001 |
| “Coffee and sweets” pattern | ||||
| Age, years | 54.9 ± 8.5 | 54.2 ± 8.5 | 53.5 ± 8.4 | <0.0001 |
| Education, college or higher, % | 46.0 | 50.2 | 39.7 | <0.0001 |
| Current smokers, % | 16.0 | 26.9 | 43.9 | <0.0001 |
| Alcohol, g/day | 17.5 ± 33.1 | 16.8 ± 25.9 | 16.5 ± 29.6 | 0.0119 |
| Regular physical activity, % | 63.4 | 60.2 | 52.8 | <0.0001 |
| Family history of diabetes, % | 13.3 | 14.8 | 13.4 | 0.5869 |
| Body mass index, kg/m2 | 24.0 ± 2.7 | 24.5 ± 2.7 | 24.4 ± 2.6 | <0.0001 |
| “Whole grain” pattern | ||||
| Age, years | 53.2 ± 8.6 | 55.6 ± 8.2 | 54.8 ± 8.5 | <0.0001 |
| Education, college or higher, % | 40.5 | 41.2 | 52.8 | <0.0001 |
| Current smokers, % | 33.9 | 26.1 | 21.5 | <0.0001 |
| Alcohol, g/day | 20.0 ± 34.2 | 16.8 ± 27.9 | 12.3 ± 22.0 | <0.0001 |
| Regular physical activity, % | 47.9 | 60.1 | 67.5 | <0.0001 |
| Family history of diabetes, % | 13.2 | 12.4 | 15.0 | 0.1031 |
| Body mass index, kg/m2 | 24.3 ± 2.6 | 24.3 ± 2.6 | 24.4 ± 2.6 | 0.1125 |
| Quintile (Q) of Dietary Pattern Score | p-Value b | |||
|---|---|---|---|---|
| Q1 (Lowest) | Q3 | Q5 (Highest) | ||
| “Prudent” pattern | ||||
| Age, years | 51.6 ± 7.9 a | 52.7 ± 7.6 | 52.9 ± 7.3 | <0.0001 |
| Education, college or higher, % | 24.3 | 24.5 | 27.2 | <0.0001 |
| Current smokers, % | 2.2 | 1.6 | 1.5 | 0.0016 |
| Alcohol, g/day | 1.8 ± 6.7 | 1.7 ± 7.3 | 1.6 ± 6.1 | 0.1220 |
| Regular physical activity, % | 44.7 | 53.5 | 62.4 | <0.0001 |
| Family history of diabetes, % | 18.9 | 18.3 | 19 | 0.7505 |
| Body mass index, kg/m2 | 23.3 ± 2.9 | 23.5 ± 2.8 | 23.6 ± 2.8 | <0.0001 |
| “Fatty fish, meat, and flour-based food” pattern | ||||
| Age, years | 56.0 ± 7.0 | 52.5 ± 7.3 | 48.7 ± 7.0 | <0.0001 |
| Education, college or higher, % | 15.7 | 24.1 | 36.9 | <0.0001 |
| Current smokers, % | 1.1 | 1.6 | 2.3 | <0.0001 |
| Alcohol, g/day | 0.9 ± 4.7 | 1.7 ± 6.2 | 2.6 ± 7.7 | <0.0001 |
| Regular physical activity, % | 55.7 | 53.7 | 50.1 | <0.0001 |
| Family history of diabetes, % | 16.2 | 19.7 | 22.3 | <0.0001 |
| Body mass index, kg/m2 | 23.7 ± 2.8 | 23.4 ± 2.8 | 23.3 ± 3.0 | <0.0001 |
| “Coffee and sweets” pattern | ||||
| Age, years | 53.9 ± 7.6 | 51.8 ± 7.3 | 52.0 ± 7.7 | <0.0001 |
| Education, college or higher, % | 20.3 | 28.2 | 24.8 | <0.0001 |
| Current smokers, % | 1.0 | 1.5 | 2.8 | <0.0001 |
| Alcohol, g/day | 1.4 ± 6.6 | 1.9 ± 5.8 | 1.9 ± 8.1 | <0.0001 |
| Regular physical activity, % | 54.2 | 56.1 | 48.1 | <0.0001 |
| Family history of diabetes, % | 18.2 | 20.2 | 18.4 | 0.8811 |
| Body mass index, kg/m2 | 23.2 ± 2.8 | 23.6 ± 2.8 | 23.7 ± 3.0 | <0.0001 |
| “White rice” pattern | ||||
| Age, years | 51.4 ± 7.7 | 53.0 ± 7.6 | 51.8 ± 7.6 | <0.0001 |
| Education, college or higher, % | 30.2 | 25.4 | 23.8 | <0.0001 |
| Current smokers, % | 1.2 | 1.6 | 2.8 | <0.0001 |
| Alcohol, g/day | 1.4 ± 5.5 | 1.7 ± 5.8 | 2.3 ± 8.2 | <0.0001 |
| Regular physical activity, % | 55.2 | 54.8 | 44.6 | <0.0001 |
| Family history of diabetes, % | 21.0 | 18.9 | 17.9 | 0.0286 |
| Body mass index, kg/m2 | 23.4 ± 2.8 | 23.5 ± 2.9 | 23.5 ± 2.9 | <0.0001 |
| Quintile (Q) of Dietary Pattern Score | p-Value b | |||
|---|---|---|---|---|
| Q1 (Lowest) | Q3 | Q5 (Highest) | ||
| “Prudent” pattern | ||||
| Total energy, kcal | 1593 ± 457 a | 1801 ± 415 | 2254 ± 580 | <0.0001 |
| Carbohydrate, % of energy | 74.7 ± 5.9 | 71.7 ± 5.8 | 67.1 ± 7.1 | <0.0001 |
| Protein, % of energy | 11.3 ± 1.6 | 13.1 ± 1.7 | 15.8 ± 2.6 | <0.0001 |
| Fat, % of energy | 5.3 ± 2.3 | 6.2 ± 2.1 | 7.5 ± 2.3 | <0.0001 |
| Calcium, mg | 278.4 ± 127.8 | 399.7 ± 141.3 | 537.3 ± 201.8 | <0.0001 |
| Phosphorus, mg | 742.3 ± 109.5 | 871.0 ± 116.1 | 1028.2 ± 166.3 | <0.0001 |
| Iron, mg | 7.4 ± 1.7 | 9.4 ± 1.9 | 12.3 ± 3.6 | <0.0001 |
| Sodium, mg | 1781 ± 977 | 2533 ± 1065 | 3302 ± 1412 | <0.0001 |
| Potassium, mg | 1562 ± 478 | 2129 ± 484 | 2765 ± 670 | <0.0001 |
| Vitamin A, RAE | 273.2 ± 141.9 | 444.9 ± 213.7 | 683.6 ± 361.3 | <0.0001 |
| Carotene, µg | 1272 ± 734 | 2212 ± 1199 | 3564 ± 2107 | <0.0001 |
| Vitamin C, mg | 55.9 ± 31.1 | 93.7 ± 37.9 | 134.2 ± 55.3 | <0.0001 |
| Folate, g | 138.9 ± 52.3 | 201.4 ± 65.1 | 279.4 ± 102.6 | <0.0001 |
| Dietary fiber, g | 3.9 ± 1.3 | 5.4 ± 1.6 | 7.2 ± 2.4 | <0.0001 |
| “Fatty fish, meat, and flour-based food” pattern | ||||
| Total energy, kcal | 1612 ± 395 | 1763 ± 385 | 2329 ± 596 | <0.0001 |
| Carbohydrate, % of energy | 75.9 ± 5.2 | 71.9 ± 5.3 | 65.6 ± 6.6 | <0.0001 |
| Protein, % of energy | 12.7 ± 2.5 | 13.1 ± 2.2 | 14.5 ± 2.5 | <0.0001 |
| Fat, % of energy | 4.5 ± 1.7 | 6.1 ± 1.8 | 8.5 ± 2.2 | <0.0001 |
| Calcium, mg | 453.4 ± 226.0 | 383.9 ± 165.3 | 389.0 ± 136.9 | <0.0001 |
| Phosphorus, mg | 906.3 ± 187.3 | 859.8 ± 150.9 | 881.6 ± 139.9 | <0.0001 |
| Iron, mg | 10.6 ± 3.9 | 9.2 ± 2.4 | 9.5 ± 2.3 | <0.0001 |
| Sodium, mg | 3160 ± 1626 | 2355 ± 1074 | 2328 ± 896 | <0.0001 |
| Potassium, mg | 2424 ± 832 | 2059 ± 609 | 2042 ± 514 | <0.0001 |
| Vitamin A, RAE | 566.3 ± 404.3 | 422.4 ± 226.9 | 430.3 ± 188.5 | <0.0001 |
| Carotene, µg | 3057 ± 2295 | 2092 ± 1244 | 2007 ± 1053 | <0.0001 |
| Vitamin C, mg | 118.1 ± 62.4 | 88.9 ± 42.6 | 83.1 ± 37.0 | <0.0001 |
| Folate, g | 246.2 ± 117.6 | 192.7 ± 72.6 | 190.9 ± 63.3 | <0.0001 |
| Dietary fiber, g | 6.8 ± 2.6 | 5.2 ± 1.7 | 4.9 ± 1.5 | <0.0001 |
| “Coffee and sweets” pattern | ||||
| Total energy, kcal | 1743 ± 531 | 1879 ± 509 | 1995 ± 530 | <0.0001 |
| Carbohydrate, % of energy | 71.8 ± 7.3 | 70.8 ± 6.6 | 70.6 ± 6.4 | <0.0001 |
| Protein, % of energy | 13.5 ± 2.8 | 13.6 ± 2.4 | 13.0 ± 2.3 | <0.0001 |
| Fat, % of energy | 5.9 ± 2.5 | 6.4 ± 2.3 | 6.8 ± 2.2 | <0.0001 |
| Calcium, mg | 400.6 ± 193.6 | 410.7 ± 176.6 | 390.9 ± 156.6 | <0.0001 |
| Phosphorus, mg | 873.7 ± 175.6 | 885.5 ± 155.7 | 873.4 ± 144.6 | 0.0014 |
| Iron, mg | 9.7 ± 3.1 | 9.7 ± 2.9 | 9.4 ± 2.7 | <0.0001 |
| Sodium, mg | 2392 ± 1219 | 2555 ± 1216 | 2573 ± 1166 | <0.0001 |
| Potassium, mg | 1998 ± 720 | 2197 ± 658 | 2241 ± 612 | <0.0001 |
| Vitamin A, RAE | 457.8 ± 274.1 | 463.2 ± 281.0 | 442.6 ± 257.4 | 0.0002 |
| Carotene, µg | 2267 ± 1515 | 2309 ± 1586 | 2228 ± 1482 | 0.0044 |
| Vitamin C, mg | 94.4 ± 52.3 | 96.2 ± 49.4 | 90.6 ± 45.5 | <0.0001 |
| Folate, g | 207.2 ± 90.0 | 206.8 ± 87.1 | 195.9 ± 78.0 | <0.0001 |
| Dietary fiber, g | 5.5 ± 2.1 | 5.5 ± 2.0 | 5.3 ± 1.9 | <0.0001 |
| “Whole grain” pattern | ||||
| Total energy, kcal | 1754 ± 490 | 1700 ± 396 | 2261 ± 487 | <0.0001 |
| Carbohydrate, % of energy | 71.0 ± 7.3 | 73.1 ± 6.1 | 71.8 ± 5.6 | <0.0001 |
| Protein, % of energy | 13.2 ± 2.7 | 12.9 ± 2.2 | 12.9 ± 1.9 | <0.0001 |
| Fat, % of energy | 6.3 ± 2.5 | 5.6 ± 2.1 | 6.4 ± 2.0 | <0.0001 |
| Calcium, mg | 358.5 ± 156.0 | 366.4 ± 171.3 | 427.4 ± 169.1 | <0.0001 |
| Phosphorus, mg | 856.0 ± 151.9 | 848.3 ± 149.4 | 867.7 ± 146.8 | <0.0001 |
| Iron, mg | 8.6 ± 2.7 | 9.4 ± 2.7 | 9.4 ± 2.5 | <0.0001 |
| Sodium, mg | 2634 ± 1302 | 2468 ± 1157 | 2152 ± 860 | <0.0001 |
| Potassium, mg | 2006 ± 619 | 2040 ± 646 | 2126 ± 595 | <0.0001 |
| Vitamin A, RAE | 443.4 ± 277.3 | 429.0 ± 256.3 | 417.2 ± 205.0 | <0.0001 |
| Carotene, µg | 2230 ± 1579 | 2202 ± 1454 | 2033 ± 1180 | <0.0001 |
| Vitamin C, mg | 87.6 ± 44.5 | 87.9 ± 45.7 | 94.3 ± 48.0 | <0.0001 |
| Folate, g | 192.5 ± 84.7 | 195.3 ± 80.0 | 199.4 ± 70.9 | <0.0001 |
| Dietary fiber, g | 5.0 ± 2.0 | 5.4 ± 1.9 | 5.4 ± 1.8 | <0.0001 |
| Quintile (Q) of Dietary Pattern Score | p-Value b | |||
|---|---|---|---|---|
| Q1 (Lowest) | Q3 | Q5 (Highest) | ||
| “Prudent” pattern | ||||
| Total energy, kcal | 1402 ± 454 a | 1654 ± 414 | 2137 ± 576 | <0.0001 |
| Carbohydrate, % of energy | 75.0 ± 6.6 | 72.3 ± 6.1 | 68.5 ± 7.4 | <0.0001 |
| Protein, % of energy | 11.6 ± 1.9 | 13.3 ± 2.0 | 15.7 ± 2.8 | <0.0001 |
| Fat, % of energy | 5.2 ± 2.5 | 6.0 ± 2.2 | 7.1 ± 2.4 | <0.0001 |
| Calcium, mg | 282.7 ± 121.2 | 432.1 ± 148.5 | 601.8 ± 206.4 | <0.0001 |
| Phosphorus, mg | 699.3 ± 107.2 | 834.2 ± 122.8 | 997.0 ± 175.9 | <0.0001 |
| Iron, mg | 7.2 ± 1.7 | 9.3 ± 2.0 | 12.2 ± 3.4 | <0.0001 |
| Sodium, mg | 1671 ± 926 | 2303 ± 1022 | 2950 ± 1264 | <0.0001 |
| Potassium, mg | 1525 ± 452 | 2135 ± 508 | 2847 ± 685 | <0.0001 |
| Vitamin A, RAE | 273.2 ± 147.2 | 4339 ± 200.7 | 662.3 ± 325.6 | <0.0001 |
| Carotene, µg | 1302 ± 800 | 2149 ± 1138 | 3427 ± 1908 | <0.0001 |
| Vitamin C, mg | 64.5 ± 35.0 | 105.9 ± 44.9 | 151.5 ± 61.0 | <0.0001 |
| Folate, g | 141.5 ± 52.7 | 205.5 ± 64.7 | 287.4 ± 97.1 | <0.0001 |
| Dietary fiber, g | 4.0 ± 1.3 | 5.5 ± 1.6 | 7.4 ± 2.3 | <0.0001 |
| “Fatty fish, meat, and flour-based food” pattern | ||||
| Total energy, kcal | 1525 ± 446 | 1589 ± 409 | 2160 ± 602 | <0.0001 |
| Carbohydrate, % of energy | 76.3 ± 5.6 | 72.8 ± 5.4 | 65.8 ± 6.8 | <0.0001 |
| Protein, % of energy | 12.8 ± 2.5 | 13.2 ± 2.3 | 14.8 ± 2.7 | <0.0001 |
| Fat, % of energy | 4.5 ± 1.8 | 5.8 ± 1.8 | 8.4 ± 2.3 | <0.0001 |
| Calcium, mg | 520.5 ± 240.2 | 416.4 ± 178.5 | 409.4 ± 147.7 | <0.0001 |
| Phosphorus, mg | 881.7 ± 198.1 | 823.5 ± 159.1 | 850.9 ± 148.6 | <0.0001 |
| Iron, mg | 10.3 ± 3.7 | 9.1 ± 2.6 | 9.5 ± 2.4 | <0.0001 |
| Sodium, mg | 2765 ± 1404 | 2177 ± 1060 | 2175 ± 861 | <0.0001 |
| Potassium, mg | 2491 ± 837 | 2077 ± 656 | 2069 ± 550 | <0.0001 |
| Vitamin A, RAE | 540.0 ± 345.7 | 422.8 ± 233.0 | 434.2 ± 202.7 | <0.0001 |
| Carotene, µg | 2864 ± 1990 | 2092 ± 1292 | 2050 ± 1127 | <0.0001 |
| Vitamin C, mg | 133.5 ± 68.7 | 101.7 ± 51.0 | 95.1 ± 42.7 | <0.0001 |
| Folate, g | 248.1 ± 108.9 | 199.1 ± 78.1 | 195.8 ± 66.2 | <0.0001 |
| Dietary fiber, g | 6.8 ± 2.5 | 5.3 ± 1.8 | 5.0 ± 1.6 | <0.0001 |
| “Coffee and sweets” pattern | ||||
| Total energy, kcal | 1614 ± 548 | 1694 ± 511 | 1812 ± 531 | <0.0001 |
| Carbohydrate, % of energy | 72.1 ± 8.0 | 71.8 ± 6.7 | 72.0 ± 6.4 | <0.0001 |
| Protein, % of energy | 13.8 ± 3.1 | 13.6 ± 2.5 | 12.9 ± 2.3 | <0.0001 |
| Fat, % of energy | 5.8 ± 2.7 | 6.1 ± 2.3 | 6.4 ± 2.3 | <0.0001 |
| Calcium, mg | 412.8 ± 191.6 | 453.6 ± 194.9 | 429.5 ± 174.5 | <0.0001 |
| Phosphorus, mg | 833.0 ± 181.6 | 853.5 ± 165.5 | 830.8 ± 151.7 | <0.0001 |
| Iron, mg | 9.5 ± 3.1 | 9.7 ± 2.9 | 9.1 ± 2.5 | <0.0001 |
| Sodium, mg | 2109 ± 1077 | 2351 ± 1113 | 2357 ± 1090 | <0.0001 |
| Potassium, mg | 1963 ± 695 | 2248 ± 707 | 2232 ± 641 | <0.0001 |
| Vitamin A, RAE | 444.5 ± 269.2 | 460.3 ± 259.1 | 430.6 ± 239.7 | <0.0001 |
| Carotene, µg | 2221 ± 1496 | 2293 ± 1473 | 2152 ± 1376 | <0.0001 |
| Vitamin C, mg | 101.7 ± 53.6 | 111.3 ± 57.0 | 103.3 ± 50.8 | <0.0001 |
| Folate, g | 205.5 ± 87.1 | 215.1 ± 86.5 | 200.8 ± 78.2 | <0.0001 |
| Dietary fiber, g | 5.5 ± 2.0 | 5.7 ± 2.1 | 5.4 ± 1.9 | <0.0001 |
| “White rice” pattern | ||||
| Total energy, kcal | 2074 ± 472 | 1752 ± 437 | 1574 ± 584 | <0.0001 |
| Carbohydrate, % of energy | 73.5 ± 5.6 | 71.8 ± 6.0 | 69.9 ± 8.4 | <0.0001 |
| Protein, % of energy | 12.3 ± 1.8 | 13.7 ± 2.1 | 14.2 ± 3.4 | <0.0001 |
| Fat, % of energy | 5.8 ± 2.0 | 6.1 ± 2.2 | 6.8 ± 2.8 | <0.0001 |
| Calcium, mg | 364.9 ± 133.9 | 442.5 ± 156.8 | 476.3 ± 239.8 | <0.0001 |
| Phosphorus, mg | 765.0 ± 120.4 | 852.4 ± 130.5 | 885.8 ± 211.9 | <0.0001 |
| Iron, mg | 8.2 ± 1.8 | 9.8 ± 2.3 | 9.8 ± 4.0 | <0.0001 |
| Sodium, mg | 1827 ± 781 | 2348 ± 1023 | 2613 ± 1369 | <0.0001 |
| Potassium, mg | 1832 ± 478 | 2196 ± 535 | 2324 ± 879 | <0.0001 |
| Vitamin A, RAE | 334.6 ± 153.5 | 464.8 ± 219.8 | 524.2 ± 345.1 | <0.0001 |
| Carotene, µg | 1614 ± 872 | 2351 ± 1306 | 2618 ± 1943 | <0.0001 |
| Vitamin C, mg | 83.6 ± 38.1 | 108.0 ± 45.9 | 119.6 ± 67.7 | <0.0001 |
| Folate, g | 171.9 ± 57.4 | 213.4 ± 71.6 | 228.4 ± 110.5 | <0.0001 |
| Dietary fiber, g | 4.7 ± 1.4 | 5.7 ± 1.8 | 5.8 ± 2.6 | <0.0001 |
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Quintile (Q) of Dietary Pattern Score | p for Trend | Quintile (Q) of Dietary Pattern Score | p for Trend | |||||
| Q1 (Lowest) | Q3 | Q5 (Highest) | Q1 (Lowest) | Q3 | Q5 (Highest) | |||
| “Prudent” pattern | ||||||||
| Person-years | 18,246 | 17,750 | 18,001 | - | 36,520 | 36,346 | 38,230 | - |
| Hyperglycemia (cases) | 231 | 240 | 222 | - | 282 | 271 | 282 | - |
| Age-adjusted HR (95% CI) a | 1.00 | 1.10 (0.92–1.32) | 1.00 (0.83–1.20) | 0.9650 | 1.00 | 0.98 (0.83–1.15) | 0.85 (0.72–1.01) | 0.0427 |
| Multivariate-adjusted HR (95% CI) | 1.00 | 1.07 (0.89–1.29) | 0.93 (0.75–1.15) | 0.4457 | 1.00 | 0.91 (0.77–0.99) | 0.75 (0.63–0.89) | 0.0003 |
| “Fatty fish, meat, and flour-based food” pattern | ||||||||
| Person-years | 18,229 | 17,868 | 17,658 | - | 37,780 | 36,471 | 36,906 | - |
| Hyperglycemia (cases) | 245 | 248 | 210 | - | 305 | 274 | 265 | - |
| Age-adjusted HR (95% CI) | 1.00 | 1.15 (0.96–1.37) | 1.06 (0.88–1.29) | 0.5544 | 1.00 | 1.27 (1.08–1.50) | 1.39 (1.17–1.65) | 0.0002 |
| Multivariate-adjusted HR (95% CI) | 1.00 | 1.10 (0.91–1.32) | 1.04 (0.83–1.30) | 0.6834 | 1.00 | 1.13 (0.92–1.38) | 1.22 (1.03–1.44) | 0.0210 |
| “Coffee and sweets” pattern | ||||||||
| Person-years | 18,161 | 18,187 | 17,430 | - | 37,000 | 36,453 | 36,618 | - |
| Hyperglycemia (cases) | 210 | 252 | 218 | - | 304 | 270 | 290 | - |
| Age-adjusted HR (95% CI) | 1.00 | 1.21 (1.01–1.46) | 1.19 (0.99–1.44) | 0.1259 | 1.00 | 1.06 (0.90–1.25) | 1.09 (0.93–1.28) | 0.0177 |
| Multivariate-adjusted HR (95% CI) | 1.00 | 1.20 (0.99–1.45) | 1.06 (0.87–1.30) | 0.7622 | 1.00 | 0.97 (0.82–1.15) | 0.94 (0.80–1.11) | 0.7350 |
| “Whole grain (men)/white rice (women)” pattern | ||||||||
| Person-years | 18,411 | 17,986 | 17,442 | - | 35,949 | 36,887 | 37,756 | - |
| Hyperglycemia (cases) | 247 | 241 | 200 | - | 245 | 298 | 308 | - |
| Age-adjusted HR (95% CI) | 1.00 | 1.06 (0.89–1.26) | 0.89 (0.74–1.08) | 0.3313 | 1.00 | 1.03 (0.87–1.22) | 1.04 (0.88–1.23) | 0.3762 |
| Multivariate-adjusted HR (95% CI) | 1.00 | 0.99 (0.82–1.19) | 0.98 (0.80–1.21) | 0.9672 | 1.00 | 1.01 (0.84–1.20) | 0.99 (0.82–1.19) | 0.4459 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.W.; Woo, H.D.; Cho, M.J.; Park, J.K.; Kim, S.S. Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults. Nutrients 2019, 11, 1801. https://doi.org/10.3390/nu11081801
Lee KW, Woo HD, Cho MJ, Park JK, Kim SS. Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults. Nutrients. 2019; 11(8):1801. https://doi.org/10.3390/nu11081801
Chicago/Turabian StyleLee, Kyung Won, Hae Dong Woo, Mi Jin Cho, Jae Kyung Park, and Sung Soo Kim. 2019. "Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults" Nutrients 11, no. 8: 1801. https://doi.org/10.3390/nu11081801
APA StyleLee, K. W., Woo, H. D., Cho, M. J., Park, J. K., & Kim, S. S. (2019). Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults. Nutrients, 11(8), 1801. https://doi.org/10.3390/nu11081801