Acute/Subacute and Sub-Chronic Oral Toxicity of a Hidroxytyrosol-Rich Virgin Olive Oil Extract


 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
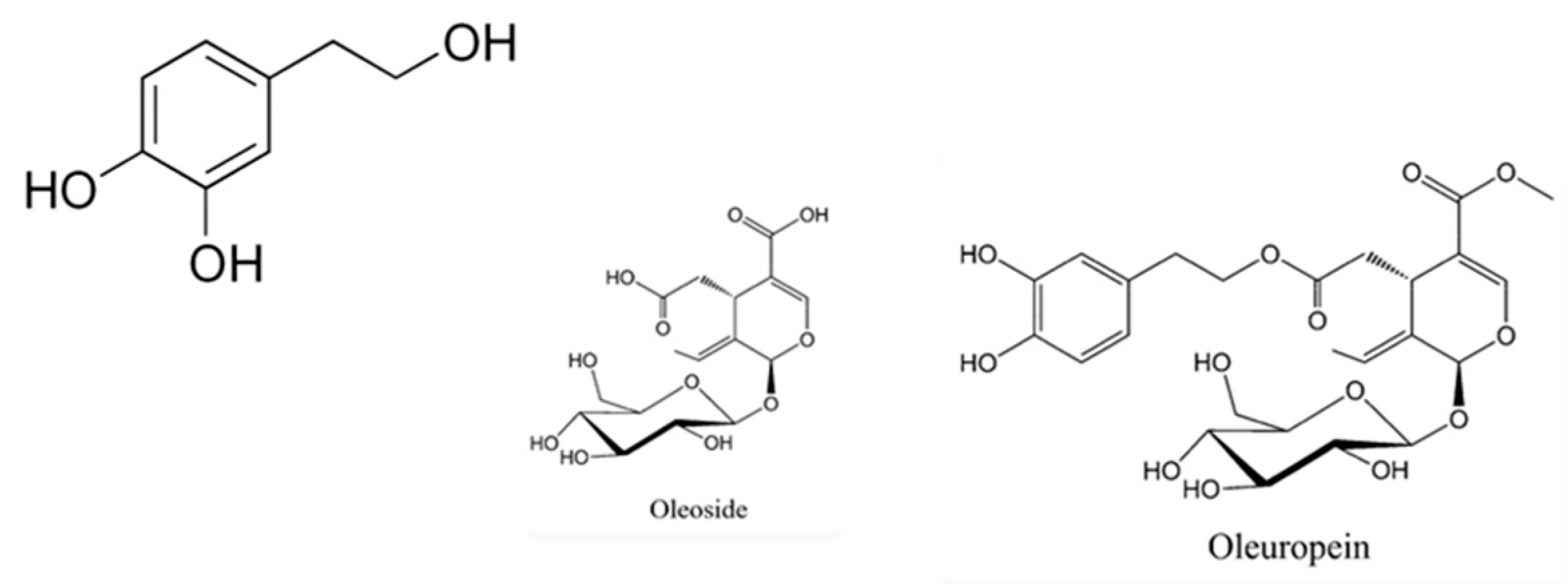
2.1. Hydroxytyrosol Isolation from a VOO Extract
2.2. Fine Tunning Study
2.3. Study Design
2.3.1. Acute/Subacute Toxicity
2.3.2. Sub Chronic Toxicity
2.4. Clinical Evaluation (Irwin Test)
2.5. Hematological and Biochemical Analyses
2.6. Histopathological Examination
2.7. Statistical Analysis
3. Results
3.1. Acute/Subacute Oral ToxicityWeight Evolution during the 14 Days of Intervention
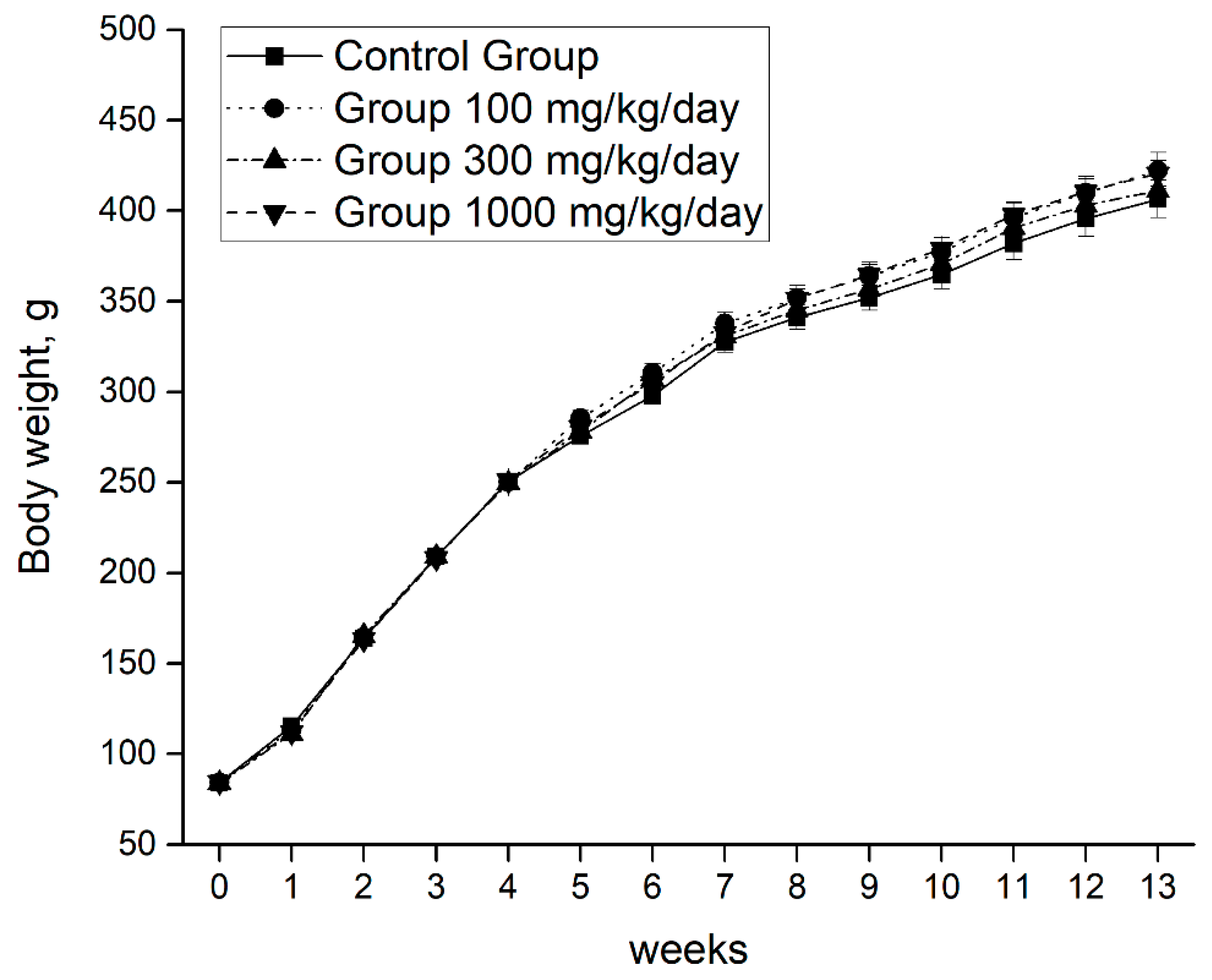
3.2. Sub Chronic Oral Toxicity Water Consumption and Weight Evolution during the 90 Days of Intervention
3.3. Clinical Evaluation: Irwin Test
3.3.1. Acute/Subacute Oral Toxicity
3.3.2. Sub Chronic Oral Toxicity
3.4. Hematological and Biochemical Biomarkers
3.4.1. Acute/Subacute Hematological Biomarkers
3.4.2. Sub Chronic Hematological Biomarkers
3.4.3. Acute/Subacute Biochemical Biomarkers
3.4.4. Sub Chronic Biochemical Biomarkers
3.5. Histopathological Examination
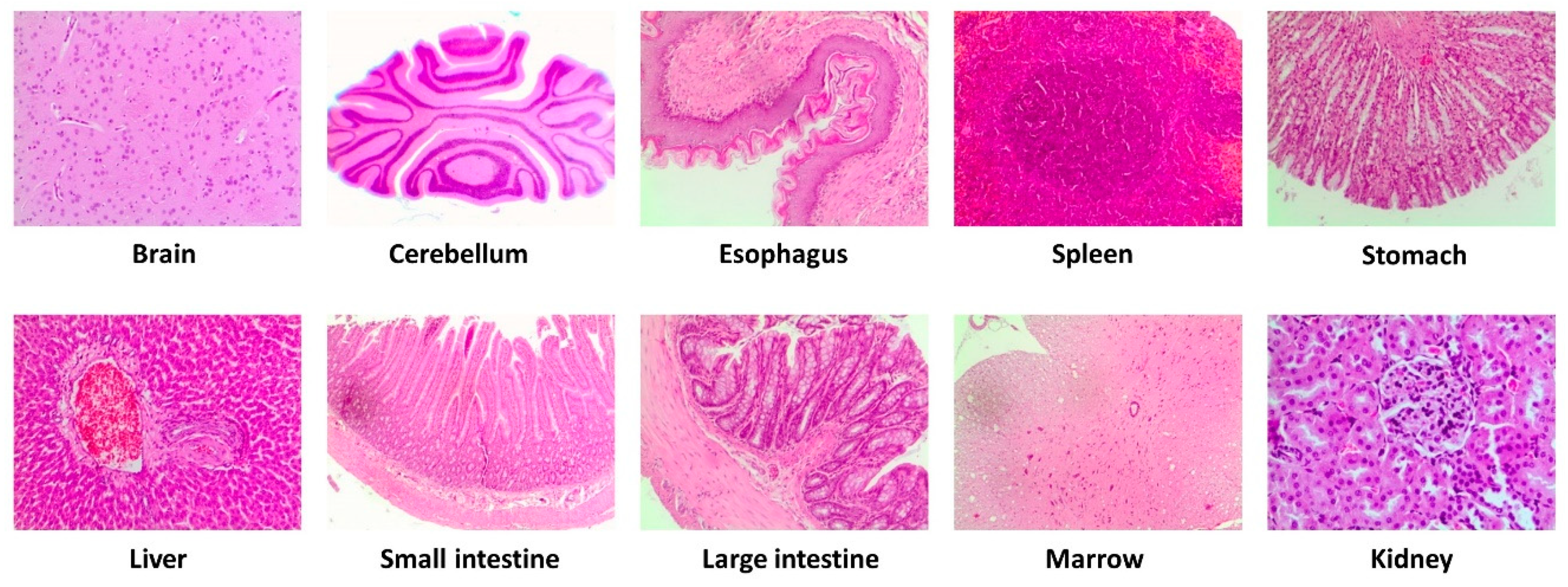
3.5.1. Acute/Subacute Oral Toxicity
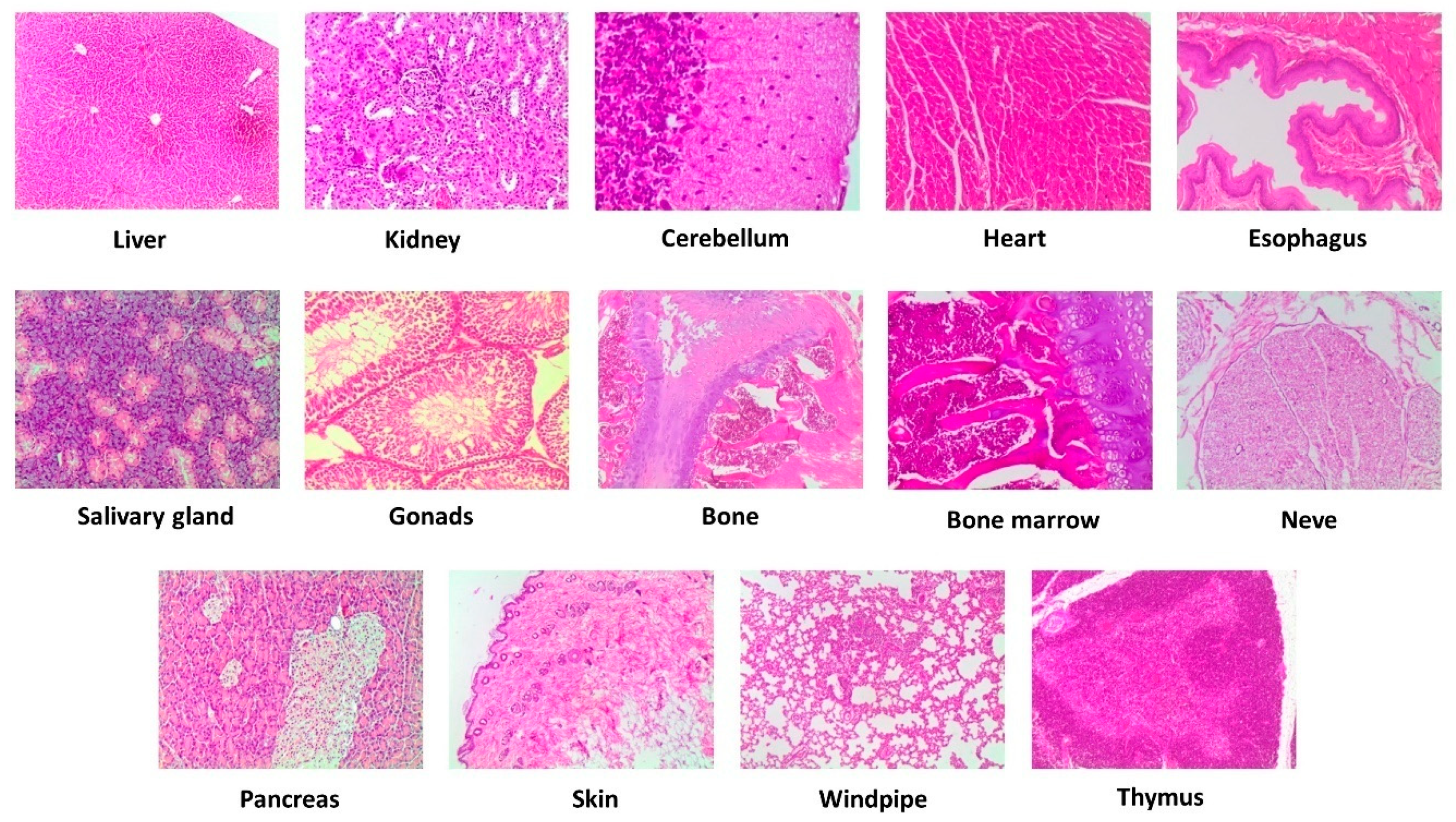
3.5.2. Sub Chronic Oral Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghamdim, S. The association between olive oil consumption and primary prevention of cardiovascular diseases. J. Fam. Med. Prim. Care 2018, 7, 859–864. [Google Scholar] [CrossRef]
- Tsartsoum, E.; Proutsosm, N.; Castanasm, E.; Kampam, M. Networkmeta-analysis of metabolic effects of olive-oil in humans shows the importance of olive oil consumption with moderate polyphenol levels as part of the mediterranean diet. Front. Nutr. 2019, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Robles-Almazan, M.; Pulido-Moran, M.; Moreno Fernández, J.; Ramírez-Tortosa, C.; Rodriguez-Garcia, C.; Quiles, J.L.; Ramirez-Tortosa, M.C. Hydroxytyrosol: Bioavailability, toxicity, and clinical applications. Food Res. Int. 2018, 105, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Marcosm, L.V.; Lou-Bonafontem, J.M.; Arnalm, C.; Navarrom, M.A.; Osadam, J. Transcriptomics and the mediterranean diet: A systematic review. Nutrients 2017, 9, 472. [Google Scholar] [CrossRef] [PubMed]
- Tejada, S.; Pinya, S.; del Mar Bibiloni, M.; Tur, J.A.; Pons, A.; Suredam, A. Cardioprotective effects of the polyphenol hydroxytyrosol from olive oil. Curr. Drug Targets. 2017, 18, 1477–1486. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to olive oil and maintenance of normal blood LDL-cholesterol concentrations (ID 1316:1332), maintenance of normal (fasting) blood concentrations of triglycerides (ID 1316:1332), maintenance of normal blood HDL cholesterol concentrations (ID 1316:1332) and maintenance of normal blood glucose concentrations (ID 4244) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2011, 9, 2044. [Google Scholar] [CrossRef]
- Vazquez, A.; Sanchez-Rodriguez, E.; Vargas, F.; Montoro-Molina, S.; Romero, M.; Espejo-Calvo, J.A.; Vilchez, P.; Jaramillo, S.; Olmo-García, L.; Carrasco-Pancorbo, A.; et al. Cardioprotective effect of a virgin olive oil enriched with bioactive compounds in spontaneously hypertensiverats. Nutrients 2019, 11, 1728. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, E.; Lima-Cabello, E.; Biel-Glesson, S.; Fernandez-Navarro, J.R.; Calleja, M.A.; Roca, M.; Espejo-Calvo, J.A.; Gil-Extremera, B.; Soria-Florido, M.; de la Torre, R.; et al. Effects of virgin olive oils differing in their bioactive compound contents on metabolic syndrome and endothelial functional risk biomarkers in healthy adults: A randomized double-blind controlled trial. Nutrients 2018, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, E.; Biel-Glesson, S.; Fernandez-Navarro, J.R.; Calleja, M.A.; Espejo-Calvo, J.A.; Gil-Extremera, B.; de la Torre, R.; Fito, M.; Covas, M.I.; Vilchez, P.; et al. Effects of virgin olive oils differing in their bioactive compound contents on biomarkers of oxidative stress and inflammation in healthy adults: A randomized double-blind controlled trial. Nutrients 2019, 11, 561. [Google Scholar] [CrossRef]
- Casuso, R.A.; Al-Fazazi, S.; Hidalgo-Gutierrez, A.; López, L.C.; Plaza-Díaz, J.; Rueda-Robles, A.; Huertas, J.R. Hydroxytyrosol influences exercise-induced mitochondrial respiratory complex assembly into supercomplexes in rats. Free Radic. Biol. Med. 2019, 134, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Al Fazazi, S.; Casuso, R.A.; Aragón-Vela, J.; Casals, C.; Huertas, J.R. Effects of hydroxytyrosol dose on the redox status of exercised rats: The role of hydroxytyrosol in exercise performance. J. Int. Soc. Sports Nutr. 2018, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Organization for Economic Cooperation and Development (OECD). OECD Guidelines for Testing of Chemicals, N° 420, Acute and Oral Toxicity: Up and Down Procedure; OECD: Paris, France, 21 September 1998. [Google Scholar]
- Organization for Economic Cooperation and Development (OECD). OECD Guidelines for Testing of Chemicals, N° 408, Repeated Dose 90-day Oral Toxicity Study in Rodents; OECD: Paris, France, 21 September 1998. [Google Scholar]
- Feldman, D.B.; Seely, J.C. Necropsy Guide: Rodent and the Rabbit; CRC Press: Boca Raton, Florida, FL, USA, 1988; p. 197. [Google Scholar]
- Yubero-Serrano, E.M.; Lopez-Moreno, J.; Gomez-Delgado, F.; Lopez-Miranda, J. Extra virgin olive oil: More than a healthy fat. Eur. J. Clin. Nutr. 2019, 72, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Castellano, S.; Ray, S.; Grosso, G.; Galvano, F. Dietary polyphenol intake and depression: Results from the mediterranean healthy eating, lifestyle and aging (meal) study. Molecules 2018, 23, 999. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G. Effects of polyphenol-Rich. foods on human health. Nutrients 2018, 10, 1089. [Google Scholar] [CrossRef] [PubMed]
- Borzì, A.; Biondi, A.; Basile, F.; Luca, S.; Vicari, E.; Vacante, M. Olive oil effects on colorectal cancer. Nutrients 2019, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Soni, M.G.; Burdock, G.A.; Christian, M.S.; Bitler, C.M.; Crea, R. Safety assessment of aqueous olive pulp extract as an antioxidant or antimicrobial agent in foods. Food Chem. Toxicol. 2006, 44, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Christian, M.S.; Sharper, V.A.; Hoberman, A.M.; Seng, J.E.; Fu, L.; Covell, D.; Diener, R.M.; Bitler, C.M.; Crea, R. The toxicity profile of hydrolyzed aqueous olive pulp extract. Drug Chem. Toxicol. 2004, 27, 309–330. [Google Scholar] [CrossRef]
- Heilman, J.; Anyangwe, N.; Tran, N.; Edwards, J.; Beilstein, P.; López, J. Toxicological evaluation of an olive extract, H35: Subchronic toxicity in the rat. Food Chem. Toxicol. 2015, 84, 18–28. [Google Scholar] [CrossRef]
- Kirkland, D.; Edwards, J.; Woehrle, T.; Beilstein, P. Investigations into the genotoxic potential of olive extracts. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2015, 777, 17–28. [Google Scholar] [CrossRef]
- Parkinson, L.; Cicerale, S. The health benefiting mechanisms of virgin olive oil phenolic compounds. Molecules 2016, 21, 1734. [Google Scholar] [CrossRef] [PubMed]
- de Pablos, R.M.; Espinosa-Oliva, A.M.; Hornedo-Ortega, R.; Cano, M.; Arguelles, S. Hydroxytyrosol protects from aging process via AMPK and autophagy; a review of its effects on cancer, metabolic syndrome, osteoporosis, immune-mediated and neurodegenerative diseases. Pharmacol. Res. 2019, 143, 58–72. [Google Scholar] [CrossRef] [PubMed]
- Karković Marković, A.; Torić, J.; Barbarić, M.; Jakobušić Brala, C. Hydroxytyrosol, tyrosol and derivatives and their potential effects on human health. Molecules 2019, 24, 2001. [Google Scholar] [CrossRef] [PubMed]
- Auñon-Calles, D.; Canut, L.; Visioli, F. Toxicological evaluation of pure hydroxytyrosol. Food Chem. Toxicol. 2013, 55, 498–504. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.; Manna, C.; Migliardi, V.; Mazzoni, O.; Morrica, P.; Capasso, G.; Pontoni, G.; Galletti, P.; Zappia, V. Pharmacokinetics and metabolism of hydroxytyrosol, a natural antioxidant from olive oil. Drug Metab. Dispos. 2001, 29, 1492–1498. [Google Scholar] [PubMed]
- Martínez, M.A.; Ares, I.; Martínez-Larrañaga, M.R.; Anadón, A.; Casado, V.; Vazquez, L.; Martin, D.; Reglero, G.; Torres, C. Acute and repeated dose (28 days) oral safety studies of phosphatidyl-hydroxytyrosol. Food Chem. Toxicol. 2018, 120, 462–471. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | 300 mg/kg (Intermediate Dose) | 2000 mg/kg/d (Maximum Dose) | p | |
|---|---|---|---|---|
| RBC (106/µL) | 7.05 ± 0.21 ab | 4.57 ± 1.26 a | 7.58 ± 0.21 b | 0.005 |
| Hemoglobin (g/dL) | 14.0 ± 0.4 a | 10.1 ± 2.7 b | 14.8 ± 0.3 ab | 0.029 |
| PCV% | 38.5 ± 1.2 a | 27.7 ± 7.8 b | 14.8 ± 0.3 ab | 0.033 |
| MCV (fl) | 54.63 ± 0.99 | 60.0 ± 5.65 | 53.87 ± 1.06 | 0.199 |
| MCH | 19.94 ± 0.38 | 22.16 ± 2.29 | 36.32 ± 0.28 | 0.167 |
| MCHC (g Hb/dL) | 36.53 ± 0.27 | 36.90 ± 0.81 | 36.32 ± 0.28 | 0.708 |
| RDW | 15.27 ± 1.14 | 15.0 ± 0.94 | 15.0 ± 0.94 | 0.511 |
| WBC (106/µL) | 8.86 ± 0.82 | 6.13 ± 1.61 | 13.60 ± 4.47 | 0.146 |
| LYM (106/µL) | 4.66 ± 0.49 | 4.03 ± 1.31 | 4.72 ± 0.46 | 0.804 |
| MON (106/µL) | 0.11 ± 0.02 | 0.20 ± 0.05 | 0.12 ± 0.02 | 0.165 |
| EOS (106/µL) | 0.11 ± 0.06 | 0.06 ± 0.03 | 0.07 ± 0.04 | 0.882 |
| BAS(106/µL) | 0.17 ± 0.03 | 0.13 ± 0.03 | 0.25 ± 0.02 | 0.267 |
| LYM% | 83.8 ± 0.8 | 85.9 ± 2.2 | 78.2 ± 5.3 | 0.190 |
| MON% | 1.9 ± 0.1 a | 3.5 ± 0.3 b | 2.3 ± 0.4 ab | 0.017 |
| EOS% | 2.14 ± 0.91 | 1.43 ± 0.35 | 1.42 ± 0.53 | 0.818 |
| BAS% | 3.2 ± 0.2 | 2.9 ± 0.6 | 4.4 ± 0.8 | 0.147 |
| PLT (103/µL) | 732.0 ± 96.7 | 596.0 ± 252.0 | 660.5 ± 168.3 | 0.811 |
| MPV (fL) | 6.60 ± 0.36 | 7.80 ± 0.68 | 6.80 ± 0.30 | 0.238 |
| PCT% | 0.48 ± 0.07 | 0.49 ± 0.21 | 0.44 ± 0.11 | 0.974 |
| PDW | 13.28 ± 1.42 | 14.43 ± 0.63 | 16.22 ± 3.64 | 0.614 |
| Control | 100 mg (Low Dose) | 300 mg (Intermediate Dose) | 1000 mg (High Dose) | P Value | |
|---|---|---|---|---|---|
| RBC (106/µL) | 7.51 ± 0.32 ab | 6.22 ± 0.42 a | 7.59 ± 0.25 ab | 7.99 ± 0.49 b | 0.010 |
| Hemoglobin (g/dL) | 14.0 ± 0.5 | 12.1 ± 0.8 | 14.3 ± 0.5 | 13.2 ± 0.7 | 0.071 |
| PCV% | 41.4 ± 1.6 ab | 33.9 ± 2.3 a | 41.0 ± 1.4 ab | 44.7 ± 3.1 b | 0.010 |
| MCV (fl) | 54.64 ± 0.50 ab | 54.71 ± 0.63 a | 54.0 ± 0.38 ab | 56.8 ± 0.80 b | 0.010 |
| MCH | 18.85 ± 0.22 a | 19.84 ± 0.71 ab | 18.79 ± 0.26 a | 16.17 ± 0.96 b | 0.001 |
| MCHC (g Hb/dL) | 34.50 ± 0.305 a | 36.18 ± 1.00 a | 34.79 ± 0.34 a | 28.85 ± 1.86 b | 0.001 |
| RDW | 14.04 ± 0.12 | 14.92 ± 0.62 | 13.79 ± 0.14 | 14.77 ± 0.21 | 0.055 |
| WBC (106/µL) | 4.85 ± 0.46 | 3.19 ± 0.37 | 4.44 ± 0.51 | 4.21 ± 0.44 | 0.063 |
| LYM (106/µL) | 3.80 ± 0.36 | 2.54 ± 0.40 | 3.42 ± 0.50 | 3.60 ± 0.40 | 0.156 |
| MON (106/µL) | 0.06 ± 0.02 | 0.08 ± 0.03 | 0.07 ± 0.01 | 0.10 ± 0.02 | 0.706 |
| NEU (106/µL) | 0.76 ± 0.09 | 0.51 ± 0.09 | 0.63 ± 0.09 | 0.48 ± 0.08 | 0.094 |
| EOS (106/µL) | 0.05 ± 0.02 | 0.09 ± 0.03 | 0.16 ± 0.01 | 0.10 ± 0.04 | 0.636 |
| BAS(106/µL) | 0.13 ± 0.01 | 0.08 ± 0.02 | 0.12 ± 0.02 | 0.09 ± 0.02 | 0.083 |
| LYM% | 78.0 ± 1.6 | 73.8 ± 2.8 | 75.9 ± 4.1 | 84.1 ± 1.4 | 0.055 |
| MON% | 1.4 ± 0.3 | 2.3 ± 0.7 | 1.5 ± 0.2 | 2.9 ± 0.7 | 0.145 |
| NEU% | 16.0 ± 1.2 a | 16.60 ± 2.09 a | 15.51 ± 1.82 a | 8.26 ± 1.28 b | 0.001 |
| EOS% | 1.5 ± 0.5 | 3.86 ± 1.20 | 3.99 ± 2.52 | 3.1 ± 1.00 | 0.634 |
| BAS% | 3.0 ± 0.3 | 3.45 ± 0.50 | 3.08 ± 0.33 | 2.66 ± 0.26 | 0.506 |
| PLT (103/µL) | 684.5 ± 70.9 a | 399.1 ± 68.3 b | 541.7 ± 63.8 ab | 424.8 ± 72.2 ab | 0.016 |
| MPV (fL) | 6.13 ± 0.06 a | 7.23 ± 0.38 bc | 6.43 ± 0.18 ab | 7.19 ± 0.30 c | 0.001 |
| PCT% | 0.38 ± 0.034 | 0.26 ± 0.04 | 0.33 ± 0.04 | 0.28 ± 0.05 | 0.120 |
| PDW | 12.02±1.02 | 13.20 ± 1.03 | 13.56 ± 1.20 | 12.70 ± 1.56 | 0.825 |
| Control | 300 mg (Low Dose) | 2000 mg (Intermediate Dose) | p Value | |
|---|---|---|---|---|
| Glucose (mg/dL) | 149.91 ± 5.27 | 135.07 ± 11.73 | 145.11 ± 9.15 | 0.452 |
| Cholesterol (mg/dL) | 64.54 ± 2.87 | 64.39 ± 7.01 | 77.89 ± 3.09 | 0.062 |
| Triacylglycerides (mg/dL) | 99.12 ± 13.97 | 101.82 ± 22.55 | 69.72 ± 13.70 | 0.424 |
| Proteins (g/dL) | 5.72 ± 0.11 | 5.60 ± 0.10 | 5.86 ± 0.15 | 0.554 |
| Albumin (g/dL) | 3.05 ± 0.03 | 2.93 ± 0.06 | 3.04 ± 0.04 | 0.328 |
| AST (U/L) | 89.74 ± 6.13 | 91.19 ± 9.57 | 81.17 ± 7.56 | 0.677 |
| ALT (U/L) | 35.59 ± 2.44 | 32.06 ± 0.86 | 31.19 ± 1.83 | 0.433 |
| Bilirrubin (mg/dL) | 0.15 ± 0.03 | 0.14 ± 0.02 | 0.12 ± 0.01 | 0.859 |
| Urea (mg/kg/dL) | 27.7 ± 1.6 | 26.9 ± 4.06 | 29.6 ± 2.5 | 0.783 |
| Creatinine (mg/kg/dL) | 0.12 ± 0.02 | 0.08 ± 0.03 | 0.05 ± 0.02 | 0.212 |
| Sodium (mg/kg/dL) | 232.73 ± 5.79 | 242.77 ± 17.33 | 250.99 ± 14.50 | 0.417 |
| Potassium (mg/kg/dL) | 123.55 ± 21.35 | 210.04 ± 27.07 | 134.44 ± 41.81 | 0.186 |
| Chloride (mg/kg/dL) | 310.5 ± 2.0 | 300.0 ± 2.3 | 303.1 ± 6.4 | 0.119 |
| Phosphorus (mg/dL) | 3.8 ± 0.13 | 3.9 ± 0.17 | 4.1 ± 0.18 | 0.584 |
| CK-MB (U/L) | 374.6 ± 36.3 a | 549.8 ± 22.14 b | 418.0 ± 29.8 ab | 0.041 |
| Control | 100 mg (Low Dose) | 300 mg (Intermediate Dose) | 1000 mg (High Dose) | p Value | |
|---|---|---|---|---|---|
| Glucose (mg/dL) | 180.99 ± 9.58 ab | 154.38 ± 6.74 ab | 151.23 ± 10.52 a | 188.20 ± 11.65 b | 0.018 |
| Cholesterol (mg/dL) | 73.83 ± 3.20 | 76.34 ± 2.98 | 65.70 ± 4.29 | 76.12 ± 3.77 | 0.137 |
| Triglycerides (mg/dL) | 105.1 ± 10.3 | 103.9 ± 7.7 | 101.3 ± 8.5 | 122.3 ± 9.6 | 0.357 |
| Proteins (g/dL) | 6.36 ± 0.06 a | 6.05 ± 0.11 ab | 5.88 ± 0.17 b | 6.25 ± 0.10 ab | 0.024 |
| Albumin (g/dL) | 3.2 ± 0.02 | 3.2 ± 0.03 | 3.2 ± 0.07 | 3.4 ± 0.115 | 0.295 |
| Albumin/Globulin | 1.0 ± 0.5 | 1.0 ± 0.3 | 1.1 ± 0.7 | 1.2 ± 0.3 | 0.159 |
| AST (U/L) | 96.20 ± 8.73 | 87.38 ± 17.18 | 68.08 ± 6.38 | 92.11 ± 12.90 | 0.368 |
| ALT (U/L) | 43.03 ± 3.74 | 33.33 ± 1.93 | 34.41 ± 2.85 | 37.04 ± 3.31 | 0.118 |
| Bilirubin (mg/dL) | 0.69 ± 0.005 a | 0.74 ± 0.005 ab | 0.77 ± 0.004 b | 0.70 ± 0.024 a | <0.001 |
| Urea (mg/kg/dL) | 45.8 ± 1.4 | 41.1 ± 1.5 | 43.2 ± 1.9 | 43.4 ± 1.7 | 0.289 |
| Creatinine (mg/kg/dL) | 0.32 ± 0.02 | 0.26 ± 0.02 | 0.27 ± 0.03 | 0.25±0.02 | 0.067 |
| Sodium (mg/kg/dL) | 183.60 ± 4.52 a | 237.14 ± 8.64 b | 214.06 ± 7.75 b | 226.28 ± 8.16 b | 0.001 |
| Potassium (mg/kg/dL) | 105.69 ± 8.34 | 116.67 ± 8.78 | 119.31 ± 10.15 | 114.95 ± 10.54 | 0.759 |
| Chloride (mg/kg/dL) | 366.6 ± 7.9 | 334.4 ± 3.1 | 342.5 ± 17.8 | 337.5 ± 2.8 | 0.090 |
| Phosphorus (mg/dL) | 5.7 ± 0.0.21 | 4.9 ± 0.21 | 6.7 ± 0.93 | 5.8 ± 0.24 | 0.095 |
| CK-MB (U/L) | 463.5 ± 58.2 | 376.5 ± 69.3 | 308.0 ± 34.0 | 410.9 ± 52.2 | 0.250 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Lara, A.; Mesa, M.D.; Aragón-Vela, J.; Casuso, R.A.; Casals Vázquez, C.; Zúñiga, J.M.; Huertas, J.R. Acute/Subacute and Sub-Chronic Oral Toxicity of a Hidroxytyrosol-Rich Virgin Olive Oil Extract. Nutrients 2019, 11, 2133. https://doi.org/10.3390/nu11092133
Rodríguez-Lara A, Mesa MD, Aragón-Vela J, Casuso RA, Casals Vázquez C, Zúñiga JM, Huertas JR. Acute/Subacute and Sub-Chronic Oral Toxicity of a Hidroxytyrosol-Rich Virgin Olive Oil Extract. Nutrients. 2019; 11(9):2133. https://doi.org/10.3390/nu11092133
Chicago/Turabian StyleRodríguez-Lara, Avilene, María Dolores Mesa, Jerónimo Aragón-Vela, Rafael A. Casuso, Cristina Casals Vázquez, Jesús M. Zúñiga, and Jesús R. Huertas. 2019. "Acute/Subacute and Sub-Chronic Oral Toxicity of a Hidroxytyrosol-Rich Virgin Olive Oil Extract" Nutrients 11, no. 9: 2133. https://doi.org/10.3390/nu11092133
APA StyleRodríguez-Lara, A., Mesa, M. D., Aragón-Vela, J., Casuso, R. A., Casals Vázquez, C., Zúñiga, J. M., & Huertas, J. R. (2019). Acute/Subacute and Sub-Chronic Oral Toxicity of a Hidroxytyrosol-Rich Virgin Olive Oil Extract. Nutrients, 11(9), 2133. https://doi.org/10.3390/nu11092133