Role of Fibre in Nutritional Management of Pancreatic Diseases

 , , , , , and
, , , , , and
Abstract
:1. Introduction
1.1. Fibres in Human Health
1.2. Pathophysiology of Digestion and Absorption in Pancreatic Diseases
2. Use of Fibre in Pancreatic Diseases
2.1. Fibre in Acute Pancreatitis
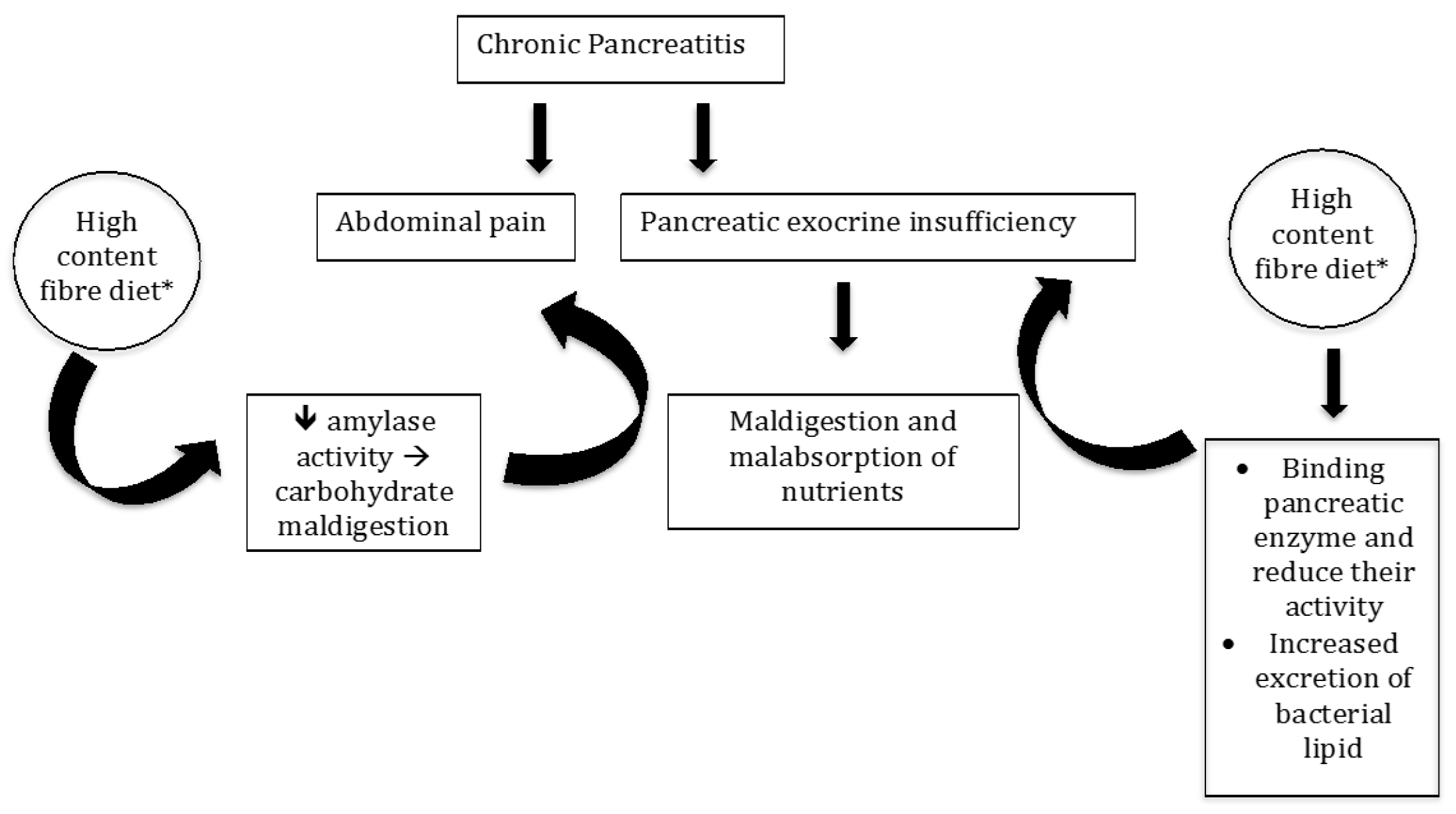
2.2. Fibre in Chronic Pancreatitis
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- The European Commission’s Science and Knowledge Service. Available online: https://ec.europa.eu/jrc/en/healthknowledgegateway/promotionprevention/nutrition/fibre (accessed on 17 May 2019).
- Eshak, E.S.; Iso, H.; Date, C.; Kikuchi, S.; Watanabe, Y.; Wada, Y.; Wakai, K.; Tamakoshi, A. JACC Study Group. Dietary fiber intake is associated with reduced risk of mortality from cardiovascular disease among Japanese men and women. J. Nutr. 2010, 140, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, Y.; Iso, H.; Saito, I.; Yamagishi, K.; Ishihara, J.; Inoue, M.; Tsugane, S.; JPHC Study Group. Dietary fiber intake and risk of cardiovascular disease in the Japanese population: The Japan Public Health Center-based study cohort. Eur. J. Clin. Nutr. 2011, 65, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Bahadoran, Z.; Khalili Moghadam, S.; Zadeh Vakili, A.; Azizi, F. A Prospective Study of Different Types of Dietary Fiber and Risk of Cardiovascular Disease: Tehran Lipid and Glucose Study. Nutritents 2016, 8, 686. [Google Scholar] [CrossRef] [PubMed]
- Wei, B.; Liu, Y.; Lin, X.; Fang, Y.; Cui, J.; Wan, J. Dietary fiber intake and risk of metabolic syndrome: A meta-analysis of observational studies. Clin. Nutr. 2018, 37, 1935–1942. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.P.; Chen, G.C.; Wang, X.P.; Qin, L.; Bai, Y. Dietary Fiber and Metabolic Syndrome: A Meta-Analysis and Review of Related Mechanisms. Nutrients 2017, 10, 24. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Pandol, S.J.; Porcel, J.; Wei, P.C.; Wilkens, L.R.; Le Marchand, L.; Pike, M.C.; Monroe, K.R. Dietary Factors Reduce Risk of Acute Pancreatitis in a Large Multiethnic Cohort. Clin. Gastroenterol. Hepatol. 2017, 15, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Prizment, A.E.; Jensen, E.H.; Hopper, A.M.; Virnig, B.A.; Anderson, K.E. Risk factors for pancreatitis in older women: The Iowa Women’s Health Study. Ann. Epidemiol. 2015, 25, 544–548. [Google Scholar] [CrossRef]
- Stephen, A.M.; Champ, M.M.; Cloran, S.J.; Fleith, M.; van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef]
- Dhingra, D.; Michael, M.; Rajput, H.; Patil, R.T. Dietary fibre in foods: A review. J. Food Sci. Technol. 2012, 49, 255–266. [Google Scholar] [CrossRef]
- Mejri, F.; Selmi, S.; Martins, A.; Benkhoud, H.; Baati, T.; Chaabane, H.; Njim, L.; Serralheiro, M.L.M.; Rauter, A.P.; Hosni, K. Broad bean (Viciafaba L.) pods: A rich source of bioactive ingredients with antimicrobial, antioxidant, enzyme inhibitory, anti-diabetic and health-promoting properties. Food Funct. 2018, 9, 2051–2069. [Google Scholar] [CrossRef]
- Müller, M.; Canfora, E.E.; Blaak, E.E. Gastrointestinal transit time, glucose homeostasis and metabolic health: Modulation by dietary fibers. Nutritents 2018, 10, 275. [Google Scholar] [CrossRef] [PubMed]
- Dahl, W.J.; Stewart, M.L. Position of the Academy of Nutrition and Dietetics: Health Implications of Dietary Fiber. J. Acad. Nutr. Diet. 2015, 115, 1861–1870. [Google Scholar] [CrossRef] [PubMed]
- Badiali, D.; Corazziari, E.; Habib, F.I.; Tomei, E.; Bausano, G.; Magrini, P.; Anzini, F.; Torsoli, A. Effect of wheat bran in treatment of chronic nonorganic constipation. A double-blind controlled trial. Dig. Dis. Sci 1995, 40, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, A.; Pelipyagina, T.; Rueffer, M.; Evans, M.; Ouwehand, A.C. Efficacy of Polydextrose Supplementation on Colonic Transit Time, Bowel Movements, and Gastrointestinal Symptoms in Adults: A Double-Blind, Randomized, Placebo-Controlled Trial. Nutrients 2019, 11, 439. [Google Scholar] [CrossRef] [PubMed]
- O’Grady, J.; Shanahan, F. Dietary Fiber and Gastrointestinal Disease: An Evolving Story. Curr. Gastroenterol. Rep. 2018, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Major, G.; Murray, K.; Singh, G.; Nowak, A.; Hoad, C.L.; Marciani, L.; Silos-Santiago, A.; Kurtz, C.B.; Johnston, J.M.; Gowland, P.; et al. Demonstration of differences in colonic volumes, transit, chyme consistency, and response to psyllium between healthy and constipated subjects using magnetic resonance imaging. Neurogastroenterol. Motil. 2018, 30, 13400. [Google Scholar] [CrossRef] [PubMed]
- Spiller, R.; Marciani, L. Intraluminal Impact of Food: New Insights from MRI. Nutrients 2019, 11, 1147. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.K.; Hlasko, J. Dietary fiber in pancreatic disease: Effect of high fiber diet on fat malabsorption in pancreatic insufficiency and in vitro study of the interaction of dietary fiber with pancreatic enzymes. Am. J. Clin. Nutr. 1985, 41, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, G.; Lundquist, I.; Ihse, I. Effect of dietary fiber on pancreatic enzyme activity in vitro. Gastroenterology 1982, 82, 918–924. [Google Scholar] [PubMed]
- Slanc, P.; Doljak, B.; Kreft, S.; Lunder, M.; Janeš, D.; Štrukelj, B. Screening of selected food and medicinal plant extracts for pancreatic lipase inhibition. Phytother. Res. 2009, 23, 874–877. [Google Scholar] [CrossRef]
- Conforti, F.; Perri, V.; Menichini, F.; Marrelli, M.; Uzunov, D.; Statti, G.A.; Menichini, F. Wild Mediterranean dietary plants as inhibitors of pancreatic lipase. Phytother. Res. 2012, 26, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Naumann, S.; Schweiggert-Weisz, U.; Bader-Mittermaier, S.; Haller, D.; Eisner, P. Differentiation of Adsorptive and Viscous Effects of Dietary Fibres on Bile Acid Release by Means of In Vitro Digestion and Dialysis. Int. J. Mol. Sci. 2018, 19, 2193. [Google Scholar] [CrossRef] [PubMed]
- Birkner, H.I.; Kern, F. In vitro adsorption of bile salts to food residues, salicylazosulphapyridine and hemicellulose. Gastroenterology 1974, 67, 237–244. [Google Scholar] [CrossRef]
- Dunaif, G.; Schneeman, B.O. The effect of dietary fiber on human pancreatic enzyme activity in vitro. Am. J. Clin. Nutr. 1981, 34, 1034–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneeman, B.O. Effect of plant fiber on lipase, trypsin and chymotrypsin activity. J. Food Sci. 1978, 43, 634–635. [Google Scholar] [CrossRef]
- Sarwar Gilani, G.; Wu Xiao, C.; Cockell, K.A. Impact of Antinutritional Factors in Food Proteins on the Digestibility of Protein and the Bioavailability of Amino Acids and on Protein Quality. Br. J. Nutr. 2012, 108, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Gemede, A.; Ratta, N. Antinutritional Factors in Plant Foods: Potential Health Benefits and Adverse Effects. Int. J. Food Sci. Nutr. 2014, 3, 284–289. [Google Scholar] [CrossRef]
- Subandi, W.; Wijaya, M.; Sudarmo, T.; Suarsini, E. Saponin isolates from cucumber (Cucumissativus L.) Fruit mesocarp and their activity as pancreatic lipase inhibitor. In Proceedings of the 8th Annual Basic Science International Conference: Coverage of Basic Sciences toward the World’s Sustainability Challenges, East Java, Indonesia, 6–7 March 2018; AIP Publishing: Melville, NY, USA, 2018; Volume 2021, p. 070016. [Google Scholar] [CrossRef]
- Birari, R.B.; Bhutani, K.K. Pancreatic lipase inhibitors from natural sources: Unexplored potential. Drug Discov. Today 2007, 12, 879–889. [Google Scholar] [CrossRef]
- Singh, G.; Suresh, S.; Bayineni, V.K.; Kadeppagari, R.K. Lipase inhibitors from plants and their medical applications. Int. J. Pharm. Pharm. Sci. 2015, 7, 1–5. [Google Scholar]
- Sugiyama, H.; Akazome, Y.; Shoji, T.; Yamaguchi, A.; Yasue, M.; Kanda, T.; Ohtake, Y. Oligomericprocyanidins in apple polyphenol are main active components for inhibition of pancreatic lipase and triglyceride absorption. J. Agric. Food Chem. 2007, 55, 4604–4609. [Google Scholar] [CrossRef]
- Satouchi, K.; Matsushita, S. Purification and properties of a lipase inhibiting protein from soybean cotyledons. Agric. Biol. Chem. 1976, 40, 889–897. [Google Scholar] [CrossRef]
- Zheng, Q.; Koike, K.; Han, L.K.; Okuda, H.; Nikaido, T. New biologically active triterpenoid saponins from Scabiosa tschiliensis. J. Nat. Prod. 2004, 67, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Pei, Y.; Ai, T.; Deng, Z.; Wu, D.; Liang, H.; McClements, D.J.; Li, B. Impact of plant extract on the gastrointestinal fate of nutraceutical-loaded nanoemulsions: Phytic acid inhibits lipid digestion but enhances curcumin bioaccessibility. Food Funct. 2019, 10, 3344–3355. [Google Scholar] [CrossRef] [PubMed]
- Working Group IAP; Acute Pancreatitis Guidelines APA. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Pezzilli, R.; Zerbi, A.; Campra, D.; Capurso, G.; Golfieri, R.; Arcidiacono, P.G.; Billi, P.; Butturini, G.; Calculli, L.; Italian Association for the Study of the Pancreas (AISP); et al. Consensus guidelines on severe acute pancreatitis. Dig. Liver Dis. 2015, 47, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N.; American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology 2018, 154, 1096–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutch Pancreatitis Study Group; Hollemans, R.A.; Hallensleben, N.D.L.; Mager, D.J.; Kelder, J.C.; Besselink, M.G.; Bruno, M.J.; Verdonk, R.C.; van Santvoort, H.C. Pancreatic exocrine insufficiency following acute pancreatitis: Systematic review and study level meta-analysis. Pancreatology 2018, 18, 253–262. [Google Scholar]
- Löhr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Haas, S.; Akisik, F.; Kartalis, N.; HaPanEU/UEG Working Group; et al. UEG Evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United Eur. Gastroenterol. J. 2017, 5, 153–199. [Google Scholar] [CrossRef]
- Whitcomb, D.C.; Frulloni, L.; Garg, P.; Greer, J.B.; Schneider, A.; Yadav, D.; Shimosegawa, T. Chronic pancreatitis: An international draft consensus proposal for a new mechanistic definition. Pancreatology 2016, 16, 218–224. [Google Scholar] [CrossRef]
- Frulloni, L.; Falconi, M.; Gabbrielli, A.; Gaia, E.; Graziani, R.; Pezzilli, R.; Uomo, G.; Andriulli, A.; Balzano, G.; Benini, L.; et al. Italian consensus guidelines for chronic pancreatitis. Dig. Liver Dis. 2010, 42 (Suppl. 6), S381–S406. [Google Scholar] [CrossRef]
- Capurso, G.; Traini, M.; Piciucchi, M.; Signoretti, M.; Arcidiacono, P.G. Exocrine pancreatic insufficiency: Prevalence, diagnosis and clinical management. Clin. Exp. Gastroenterol. 2019, 12, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Lindkvist, B.; Phillips, M.E.; Domínguez-Munoz, J.E. Clinical, anthropometric and laboratory nutritional markers of pancreatic exocrine insufficiency: Prevalence and diagnostic use. Pancreatology 2015, 15, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Andersen, D.K. The practical importance of recognizing pancreatogenic or type 3c diabetes. Diabetes Metab. Res. Rev. 2012, 28, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Magruder, J.T.; Elahi, D.; Andersen, D.K. Diabetes and pancreatic cancer: Chicken or egg? Pancreas 2011, 40, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S. Diabetes of the exocrine pancreas: American Diabetes Association-compliant lexicon. Pancreatology 2017, 17, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Hart, P.A.; Bellin, M.D.; Andersen, D.K.; Bradley, D.; Cruz-Monserrate, Z.; Forsmark, C.E.; Goodarzi, M.O.; Habtezion, A.; Korc, M.; Kudva, Y.C.; et al. Type 3c (pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer. Lancet Gastroenterol. Hepatol 2016, 1, 226–237. [Google Scholar] [CrossRef] [Green Version]
- Abu-El-Haija, M.; Hornung, L.; Denson, L.A.; Husami, A.; Lin, T.K.; Matlock, K.; Nathan, J.D.; Palermo, J.J.; Thompson, T.; Valencia, C.A.; et al. Prevalence of abnormal glucose metabolism in pediatric acute, acute recurrent and chronic pancreatitis. PLoS ONE 2018, 13, e0204979. [Google Scholar] [CrossRef]
- Ewald, N.; Kaufmann, C.; Raspe, A.; Kloer, H.U.; Bretzel, R.G.; Hardt, P.D. Prevalence of diabetes mellitus secondary to pancreatic diseases (type 3c). Diabetes Metab. Res. Rev. 2012, 28, 338–342. [Google Scholar] [CrossRef]
- Das, S.L.; Singh, P.P.; Phillips, A.R.; Murphy, R.; Windsor, J.A.; Petrov, M.S. Newly diagnosed diabetes mellitus after acute pancreatitis: A systematic review and meta-analysis. Gut 2014, 63, 818–831. [Google Scholar] [CrossRef]
- Shen, H.N.; Yang, C.C.; Chang, Y.H.; Lu, C.L.; Li, C.Y. Risk of Diabetes Mellitus after First-Attack Acute Pancreatitis: A National Population-Based Study. Am. J. Gastroenterol. 2015, 110, 1698–1706. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.K.; Huang, M.Y.; Hsu, C.Y.; Su, Y.C. Bidirectional Relationship Between Diabetes and Acute Pancreatitis: A Population-Based Cohort Study in Taiwan. Medicine (Baltimore) 2016, 95, e2448. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Meier, J.J. Incretin hormones: Their role in health and disease. Diabetes Obes. Metab. 2018, 20 (Suppl. 1), S5–S21. [Google Scholar] [CrossRef]
- Ewald, N.; Hardt, P.D. Diagnosis and treatment of diabetes mellitus in chronic pancreatitis. World J. Gastroenterol. 2013, 19, 7276–7281. [Google Scholar] [CrossRef] [PubMed]
- Knop, F.K. Incretin hormones and beta cell function in chronic pancreatitis. Dan. Med. Bull. 2010, 57, B4163. [Google Scholar] [PubMed]
- Das, S.L.; Kennedy, J.I.; Murphy, R.; Phillips, A.R.; Windsor, J.A.; Petrov, M.S. Relationship between the exocrine and endocrine pancreas after acute pancreatitis. World J. Gastroenterol. 2014, 20, 17196–17205. [Google Scholar] [CrossRef] [PubMed]
- Duggan, S.N.; Ewald, N.; Kelleher, L.; Griffin, O.; Gibney, J.; Conlon, K.C. The nutritional management of type 3c (pancreatogenic) diabetes in chronic pancreatitis. Eur. J. Clin. Nutr. 2017, 71, 3–8. [Google Scholar] [CrossRef]
- Knop, F.K.; Vilsbøll, T.; Larsen, S.; Højberg, P.V.; Vølund, A.; Madsbad, S.; Holst, J.J.; Krarup, T. Increased postprandial responses of GLP-1 and GIP in patients with chronic pancreatitis and steatorrhea following pancreatic enzyme substitution. Am. J. Physiol. Endocrinol. Metab. 2007, 292, 324–330. [Google Scholar] [CrossRef]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M.; Food and Nutrition Board of the Institute of Medicine; The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and aminoacids. J. Am. Diet. Assoc 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Singh, S.; Midha, S.; Singh, N.; Joshi, Y.K.; Garg, P.K. Dietary counseling versus dietary supplements for malnutrition in chronic pancreatitis: A randomized controlled trial. Clin. Gastroenterol. Hepatol. 2008, 6, 353–359. [Google Scholar] [CrossRef]
- Duggan, S.; O’Sullivan, M.; Feehan, S.; Ridgway, P.; Conlon, K. Nutrition treatment of deficiency and malnutrition in chronic pancreatitis: A review. Nutr. Clin. Pract. 2010, 25, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Oláh, A.; Belágyi, T.; Pótó, L.; Romics, L., Jr.; Bengmark, S. Synbiotic control of inflammation and infection in severe acute pancreatitis: A prospective, randomized, double blind study. Hepatogastroenterology 2007, 54, 590–594. [Google Scholar] [PubMed]
- Karakan, T.; Ergun, M.; Dogan, I.; Cindoruk, M.; Unal, S. Comparison of early enteral nutrition in severe acute pancreatitis with prebiotic fiber supplementation versus standard enteral solution: A prospective randomized double-blind study. World J. Gastroenterol. 2007, 13, 2733–2737. [Google Scholar] [CrossRef] [PubMed]
- DiMagno, E.P.; Malagelada, J.R.; Go, V.L.; Moertel, C.G. Fate of orally ingested enzymes in pancreatic insufficiency. Comparison of two dosage schedules. N. Engl. J. Med. 1977, 296, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.K.; Bustin, M.P.; Russell, R.M.; Costa, B.S. Deficiency of fat-soluble vitamins in treated patients with pancreatic insufficiency. Ann. Intern. Med. 1982, 97, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Eckerwall, G.E.; Tingstedt, B.B.; Bergenzaun, P.E.; Andersson, R.G. Immediate oral feeding in patients with mild acute pancreatitis is safe and may accelerate recovery—A randomized clinical study. Clin. Nutr. 2007, 26, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xue, G.J.; Liu, Y.L.; Javed, M.A.; Zhao, X.L.; Wan, M.H.; Chen, G.Y.; Altaf, K.; Huang, W.; Tang, W.F. Early oral refeeding wisdom in patients with mild acute pancreatitis. Pancreas 2013, 42, 88–91. [Google Scholar] [CrossRef]
- Jafari, T.; Feizi, A.; Askari, G.; Fallah, A.A. Parenteral immunonutrition in patients with acute pancreatitis: A systematic review and meta-analysis. Clin. Nutr. 2015, 34, 35–43. [Google Scholar] [CrossRef]
- Pan, L.L.; Li, J.; Shamoon, M.; Bhatia, M.; Sun, J. Recent Advances on Nutrition in Treatment of Acute Pancreatitis. Front. Immunol. 2017, 8, 762. [Google Scholar] [CrossRef] [Green Version]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Society of Critical Care Medicine; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN). J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Zhang, M.M.; Cheng, J.Q.; Lu, Y.R.; Yi, Z.H.; Yang, P.; Wu, X.T. Use of pre-, pro- and synbiotics in patients with acute pancreatitis: A meta-analysis. World J. Gastroenterol. 2010, 16, 3970–3978. [Google Scholar] [CrossRef]
- Oláh, A.; Belágyi, T.; Issekutz, A.; Gamal, M.E.; Bengmark, S. Randomized clinical trial of specific lactobacillus and fibre supplement to early enteral nutrition in patients with acute pancreatitis. Br. J. Surg. 2002, 89, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, H.H.; Irtun, O.; Olesen, S.S.; Drewes, A.M.; Holst, M. Nutrition in chronic pancreatitis. World J. Gastroenterol. 2013, 19, 7267–7275. [Google Scholar] [CrossRef] [PubMed]
- Fieker, A.; Philpott, J.; Armand, M. Enzyme replacement therapy for pancreatic insufficiency: Present and future. Clin. Exp. Gastroenterol. 2011, 4, 55–73. [Google Scholar] [CrossRef] [PubMed]
- Holtmann, G.; Kelly, D.G.; Sternby, B.; DiMagno, E.P. Survival of human pancreatic enzymes during small bowel transit: Effect of nutrients, bile acids, and enzymes. Am. J. Physiol. 1997, 273 Pt 1 (Suppl. 2), G553–G558. [Google Scholar] [CrossRef]
- Moore, W.E.; Holdeman, L.V. Human fecal flora: The normal flora of 20 Japanese-Hawaiians. Appl. Microbiol. 1974, 27, 961–979. [Google Scholar] [PubMed]
- Stephen, A.M.; Cummings, J.H. Mechanism of action of dietary fibre in the human colon. Nature 1980, 284, 283–284. [Google Scholar] [CrossRef]
- Bryant, M.P. Nutritional features and ecology of predominant anaerobic bacteria of the intestinal tract. Am. J. Clin. Nutr. 1974, 27, 1313–1319. [Google Scholar] [CrossRef]
- Baird, I.M.; Walters, R.L.; Davies, P.S.; Hill, M.J.; Drasar, B.S.; Southgate, D.A. The effects of two dietary fiber supplements on gastrointestinal transit, stool weight and frequency, and bacterial flora, and fecal bile acids in normal subjects. Metabolism 1977, 26, 117–128. [Google Scholar] [CrossRef]
- Draser, B.S.; Jenkins, D.I.A.; Cummings, O.H. The influence of diet rich in wheat fiber on the human fend flora. J. Med. Microbiol. 1976, 9, 423–443. [Google Scholar] [CrossRef]
- Varel, V.H.; Pond, W.G.; Pekas, J.C.; Yen, J.T. Influence of high-fiber diet on bacterial populations in gastrointestinal tracts of obese- and lean-genotype pigs. Appl. Environ. Microbiol. 1982, 44, 107–112. [Google Scholar] [Green Version]
- Miranda, P.M.; Horwitz, D.L. High-fiber diets in the treatment of diabetes mellitus. Ann. Intern. Med. 1978, 88, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Schneeman, B.O.; Richter, B.D.; Jacobs, L.R. Response to dietary wheat bran in the exocrine pancreas and intestine of rats. J. Nutr. 1982, 112, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Forman, L.P.; Schneeman, B.O. Effects of dietary pectin and fat on the small intestinal contents and exocrine pancreas of rats. J. Nutr. 1980, 110, 1992–1999. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Muñoz, J.E. Pancreatic enzyme therapy for pancreatic exocrine insufficiency. Curr. Gastroenterol. Rep. 2007, 9, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Meier, R.F.; Beglinger, C. Nutrition in pancreatic diseases. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 507–529. [Google Scholar] [CrossRef] [PubMed]
- Meier, R.; Ockenga, J.; Pertkiewicz, M.; Pap, A.; Milinic, N.; Macfie, J.; Löser, C.; Keim, V.; DGEM (German Society for Nutritional Medicine); ESPEN (European Society for Parenteral and Enteral Nutrition). ESPEN guidelines on enteral nutrition: Pancreas. Clin. Nutr. 2006, 25, 275–284. [Google Scholar] [CrossRef]
- Plauth, M.; Cabré, E.; Campillo, B.; Kondrup, J.; Marchesini, G.; Schütz, T.; Shenkin, A.; Wendon, J. ESPEN Guidelines on Parenteral Nutrition: Hepatology. Clin. Nutr. 2009, 28, 436–444. [Google Scholar] [CrossRef]
- Dos Santos, P.Q.; Guedes, J.C.; de Jesus, R.P.; Santos, R.R.D.; Fiaconne, R.L. Effects of using symbiotics in the clinical nutritional evolution of patients with chronic pancreatitis: Study prospective, randomized, controlled, double blind. Clin. Nutr ESPEN 2017, 18, 9–15. [Google Scholar] [CrossRef]
- Adolph, T.E.; Mayr, L.; Grabherr, F.; Schwärzler, J.; Tilg, H. Pancreas-Microbiota Cross Talk in Health and Disease. Annu. Rev. Nutr. 2019, 39, 249–266. [Google Scholar] [CrossRef]
- Gou, S.; Yang, Z.; Liu, T.; Wu, H.; Wang, C. Use of probiotics in the treatment of severe acute pancreatitis: A systematic review and meta-analysis of randomized controlled trials. Crit. Care 2014, 18, 57. [Google Scholar] [CrossRef]


{kind=link}
| Anti-Nutrients | Alimentary Products |
|---|---|
| Saponins [34] | soybeans |
| Phytate [27] | grains (rice polished, wheat bran), oilseeds, legumes |
| Lectins [28] | legumes, oilseeds (soybeans) |
| Trypsin inhibitors [27] | soybeans, legumes (beans, peas) |
| Tannins [27] | legumes (beans, peas), cereals (sorghum, millet) |
| Polyphenols [30] | extracts of citrus fruits, grape seeds, tea (oolong tea), peanut shells, apples |
| Study | N Patients | Pre-Probiotic Group | Control Group | Outcomes |
|---|---|---|---|---|
| Olah A. (2002) [74] | 45 | Live L. plantarum 299 + oat fibre | Inactiveted L. plantarum 299 + oat fibre | ↓ infected pancreatic necrosis (1/22 (4.5%) vs. 7/23 (30.4%) p < 0.05) and surgical interventions (1/22 (4.5%) vs. 7/23 (30.4%) p < 0.05). |
| Olah A. (2007) [64] | 62 | Inulin, beta-glucan, resistant starch, pectin + Lactobacilli | Inulin, beta-glucan, resistant starch, pectin | ↓ incidence of SIRS and OF (8/33 (24.2%) vs. 14/29 (48.3%) p < 0.05); ↓ overall complications (9/33 (27.3%) vs. 15/29 (51.7%) p < 0.05). |
| Karakan T. (2007) [65] | 30 | Soluble + Insoluble fibre | Standard enteral solution | ↓ hospital stay (10 ± 4 vs. 15 ± 6 p < 0.05), overall complications (7/15 (46.6%) vs. 9/15 (60%) p < 0.05). |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribichini, E.; Stigliano, S.; Rossi, S.; Zaccari, P.; Sacchi, M.C.; Bruno, G.; Badiali, D.; Severi, C. Role of Fibre in Nutritional Management of Pancreatic Diseases. Nutrients 2019, 11, 2219. https://doi.org/10.3390/nu11092219
Ribichini E, Stigliano S, Rossi S, Zaccari P, Sacchi MC, Bruno G, Badiali D, Severi C. Role of Fibre in Nutritional Management of Pancreatic Diseases. Nutrients. 2019; 11(9):2219. https://doi.org/10.3390/nu11092219
Chicago/Turabian StyleRibichini, Emanuela, Serena Stigliano, Sara Rossi, Piera Zaccari, Maria Carlotta Sacchi, Giovanni Bruno, Danilo Badiali, and Carola Severi. 2019. "Role of Fibre in Nutritional Management of Pancreatic Diseases" Nutrients 11, no. 9: 2219. https://doi.org/10.3390/nu11092219
APA StyleRibichini, E., Stigliano, S., Rossi, S., Zaccari, P., Sacchi, M. C., Bruno, G., Badiali, D., & Severi, C. (2019). Role of Fibre in Nutritional Management of Pancreatic Diseases. Nutrients, 11(9), 2219. https://doi.org/10.3390/nu11092219