Breastfeeding for 3 Months or Longer but Not Probiotics Is Associated with Reduced Risk for Inattention/Hyperactivity and Conduct Problems in Very-Low-Birth-Weight Children at Early Primary School Age

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Patients and Methods
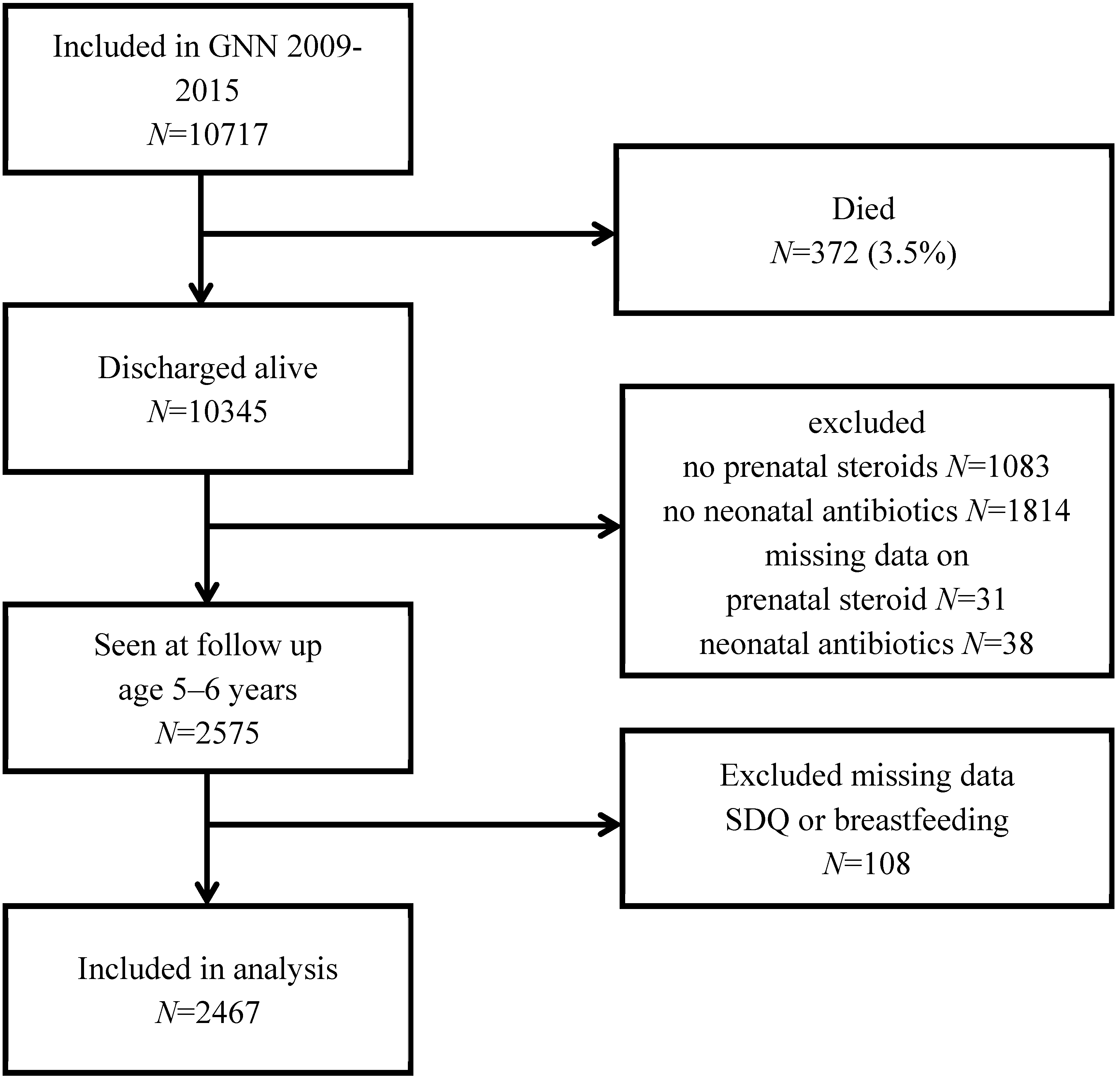
2.1. Cohort
2.2. Variables
2.2.1. Primary Outcome
2.2.2. Main Treatments
2.2.3. Control Variables
2.3. Statistical Analyzes
2.4. Ethical Approval
3. Results
3.1. Breastfeeding ≥3 months and Behavioral Outcome and IQ at Early Primary School Age
3.2. Neonatal Probiotic Treatment and Behavioral Outcome/IQ at Early Primary School Age
3.3. Long-Term Physical Impairments and Neurobehavioral Outcome at Early Primary School Age
4. Discussion
4.1. Breastfeeding and Behavioral Outcome and IQ at School Age
4.2. Probiotic Treatment and Neurocognitive and Behavioral Outcome at School Age
4.3. The Pivotal Interface Between Somatic and Mental Health
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A


{kind=link}
| Model 1 Unadj. B (95% CI) | Model 2 Adj. B (95% CI) | Model 3 Adj. B (95% CI) | |
|---|---|---|---|
| Breastfeeding ≥ 3 vs < 3 months | |||
| Total SDQ score | −1.55 (−2.22–(−0.88)) | −0.76 (−1.54−0.02) | −0.58 (−0.14–0.18) |
| Emotional symptoms | −0.01 (−0.23–0.23) | 0.21 (−0.06–0.49) | 0.23 (−0.05–0.50) |
| Conduct problems | −0.44 (−0.63–(−0.25)) | −0.26 (−0.48–(−0.04)) | −0.25 (−0.47–(−0.03)) |
| Hyperactivity/inattention | −0.82 (−0.14–(−0.51)) | −0.53 (−0.90–(−0.17)) | −0.46 (−0.81–(−0.10)) |
| Peer problems | −0.29 (−0.51–(−0.07)) | −0.18 (−0.44–0.08) | −0.10 (−0.36–0.15) |
| Prosocial behaviour | 0.29 (0.06–0.52) | 0.13 (−0.14–0.40) | 0.07 (−0.20–0.34) |
| Full-scale IQ | 5.43 (3.70–7.16) | 2.72 (0.88–4.55) | 2.20 (0.43–3.97) |
| Probiotic treatment (yes vs no) | |||
| Total SDQ score | 0.24 (−0.34–0.83) | 0.08 (−0.51–0.66) | 0.12 (−0.45–0.69) |
| Emotional symptoms | −0.09 (−0.29–0.12) | −0.11 (−0.31–0.10) | −0.10 (−0.31–0.10) |
| Conduct problems | 0.03 (−0.14–0.19) | 0.03 (−0.14–0.20) | 0.03 (−0.13–0.20) |
| Hyperactivity/inattention | 0.11 (−0.16–0.39) | 0.03 (−0.24–0.30) | 0.05 (−0.21–0.31) |
| Peer problems | 0.18 (−0.01–0.38) | −0.18 (−0.44–0.08) | −0.10 (−0.36–0.15) |
| Prosocial behaviour | −0.16 (−0.36–0.04) | −0.18 (−0.39–0.02) | −0.19(−0.39–0.01) |
| Full-scale IQ | 0.66 (−0.78–2.10) | 1.02 (−0.35–2.38) | 0.94 (−0.37–2.26) |
| Breastfeeding and Probiotics N = 1218 B (95% CI) | Breastfeeding Only N = 407 | Probiotics Only N = 174 | |
|---|---|---|---|
| SDQ, total score | 0.06 (−1.5–1.6) | 0.02 (−1.6–1.6) | 0.8 (−0.9–2.5) |
| Emotional symptoms | −0.31 (−0.9–0.2) | −0.28 (−0.9–0.3) | −0.68 (−1.3–(−0.01)) |
| Conduct problems | −0.04 (−0.5–0.4) | −0.05 (−0.5–0.4) | 0.26 (−0.2–0.8) |
| Hyperactivity/inattention | 0.16 (−0.5–0.9) | 0.2 (−0.5–0.9) | 0.79 (0.01–1.6) |
| Peer problems | 0.26 (−0.3–0.8) | 0.15 (−0.4–0.7) | 0.43 (−0.1–1.0) |
| Prosocial behaviour | −0.19 (−0.7–0.4) | −0.02 (−0.6–0.5) | −0.29 (−0.9–0.3) |
| Full-scale IQ | 1.9 (−1.6–5.4) | 0.7 (−2.9–4.4) | −0.7 (−4.6–3.1) |
References
- Ask, H.; Gustavson, K.; Ystrom, E.; Havdahl, K.A.; Tesli, M.; Askeland, R.B.; Reichborn-Kjennerud, T. Association of gestational age at birth with symptoms of attention-deficit/hyperactivity disorder in children. JAMA Pediatrics 2018, 172, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Bull-Larsen, S.; Mohajeri, M.H. The potential influence of the bacterial microbiome on the development and progression of adhd. Nutrients 2019, 11, 2805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humberg, A.; Spiegler, J.; Fortmann, M.I.; Zemlin, M.; Marissen, J.; Swoboda, I.; Rausch, T.K.; Herting, E.; Göpel, W.; Härtel, C. Surgical necrotizing enterocolitis but not spontaneous intestinal perforation is associated with adverse neurological outcome at school age. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keunen, K.; van Elburg, R.M.; van Bel, F.; Benders, M.J. Impact of nutrition on brain development and its neuroprotective implications following preterm birth. Pediatric Res. 2015, 77, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclercq, S.; Mian, F.M.; Stanisz, A.M.; Bindels, L.B.; Cambier, E.; Ben-Amram, H.; Koren, O.; Forsythe, P.; Bienenstock, J. Low-dose penicillin in early life induces long-term changes in murine gut microbiota, brain cytokines and behavior. Nat. Commun. 2017, 8, 15062. [Google Scholar] [CrossRef] [PubMed]
- Slykerman, R.F.; Coomarasamy, C.; Wickens, K.; Thompson, J.M.D.; Stanley, T.V.; Barthow, C.; Kang, J.; Crane, J.; Mitchell, E.A. Treatment to antibiotics in the first 24 months of life and neurocognitive outcomes at 11 years of age. Psychopharmacology 2019, 236, 1573–1582. [Google Scholar] [CrossRef] [PubMed]
- Astiz, M.; Heyde, I.; Fortmann, M.I.; Bossung, V.; Roll, C.; Stein, A.; Gruttner, B.; Gopel, W.; Hartel, C.; Obleser, J.; et al. The circadian phase of antenatal glucocorticoid treatment affects the risk of behavioral disorders. Nat. Commun. 2020, 11, 3593. [Google Scholar] [CrossRef]
- Agostoni, C.; Mazzocchi, A.; Leone, L.; Ciappolino, V.; Delvecchio, G.; Altamura, C.A.; Brambilla, P. The first model of keeping energy balance and optimal psycho affective development: Breastfed children. J. Affect. Disord. 2017, 224, 10–15. [Google Scholar] [CrossRef]
- Boucher, O.; Julvez, J.; Guxens, M.; Arranz, E.; Ibarluzea, J.; Sanchez de Miguel, M.; Fernandez-Somoano, A.; Tardon, A.; Rebagliato, M.; Garcia-Esteban, R.; et al. Association between breastfeeding duration and cognitive development, autistic traits and adhd symptoms: A multicenter study in spain. Pediatric Res. 2017, 81, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Tseng, P.T.; Yen, C.F.; Chen, Y.W.; Stubbs, B.; Carvalho, A.F.; Whiteley, P.; Chu, C.S.; Li, D.J.; Chen, T.Y.; Yang, W.C.; et al. Maternal breastfeeding and attention-deficit/hyperactivity disorder in children: A meta-analysis. Eur. Child Adolesc. Psychiatry 2019, 28, 19–30. [Google Scholar] [CrossRef]
- Flacking, R.; Ewald, U.; Nyqvist, K.H.; Starrin, B. Trustful bonds: A key to “becoming a mother” and to reciprocal breastfeeding. Stories of mothers of very preterm children at a neonatal unit. Soc. Sci. Med. 2006, 62, 70–80. [Google Scholar] [CrossRef]
- Ericson, J.; Flacking, R.; Hellstrom-Westas, L.; Eriksson, M. Changes in the prevalence of breast feeding in preterm children discharged from neonatal units: A register study over 10 years. BMJ Open 2016, 6, e012900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ericson, J.; Palmer, L. Cessation of breastfeeding in mothers of preterm children-a mixed method study. PLoS ONE 2020, 15, e0233181. [Google Scholar] [CrossRef]
- Underwood, M.A.; German, J.B.; Lebrilla, C.B.; Mills, D.A. Bifidobacterium longum subspecies infantis: Champion colonizer of the infant gut. Pediatric Res. 2015, 77, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Tarr, P.I.; Warner, B.B. Gut bacteria and late-onset neonatal bloodstream infections in preterm children. Semin. Fetal Neonatal Med. 2016, 21, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Fortmann, I.; Marissen, J.; Siller, B.; Spiegler, J.; Humberg, A.; Hanke, K.; Faust, K.; Pagel, J.; Eyvazzadeh, L.; Brenner, K.; et al. Lactobacillus acidophilus/bifidobacterium infantis probiotics are beneficial to extremely low gestational age children fed human milk. Nutrients 2020, 12, 850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graspeuntner, S.; Waschina, S.; Kunzel, S.; Twisselmann, N.; Rausch, T.K.; Cloppenborg-Schmidt, K.; Zimmermann, J.; Viemann, D.; Herting, E.; Gopel, W.; et al. Gut dysbiosis with bacilli dominance and accumulation of fermentation products precedes late-onset sepsis in preterm children. Clin. Infect. Dis. 2019, 69, 268–277. [Google Scholar] [CrossRef]
- Cowan, C.S.M.; Stylianakis, A.A.; Richardson, R. Early-life stress, microbiota, and brain development: Probiotics reverse the effects of maternal separation on neural circuits underpinning fear expression and extinction in infant rats. Dev. Cogn. Neurosci. 2019, 37, 100627. [Google Scholar] [CrossRef]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Klasen, H.; Woerner, W.; Rothenberger, A.; Goodman, R. [German version of the strength and difficulties questionnaire (sdq-german)-overview and evaluation of initial validation and normative results]. Prax. Kinderpsychol. Kinderpsychiatr. 2003, 52, 491–502. [Google Scholar]
- Julvez, J.; Ribas-Fito, N.; Forns, M.; Garcia-Esteban, R.; Torrent, M.; Sunyer, J. Attention behaviour and hyperactivity at age 4 and duration of breast-feeding. Acta Paediatr. 2007, 96, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Hartel, C.; Pagel, J.; Rupp, J.; Bendiks, M.; Guthmann, F.; Rieger-Fackeldey, E.; Heckmann, M.; Franz, A.; Schiffmann, J.H.; Zimmermann, B.; et al. Prophylactic use of lactobacillus acidophilus/bifidobacterium infantis probiotics and outcome in very low birth weight children. J. Pediatrics 2014, 165, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.; Bartlett, D. Gross motor function classification system: Impact and utility. Dev. Med. Child Neurol. 2004, 46, 60–65. [Google Scholar] [CrossRef]
- Elvrum, A.K.; Andersen, G.L.; Himmelmann, K.; Beckung, E.; Ohrvall, A.M.; Lydersen, S.; Vik, T. Bimanual fine motor function (bfmf) classification in children with cerebral palsy: Aspects of construct and content validity. Phys. Occup. Ther. Pediatrics 2016, 36, 1–16. [Google Scholar] [CrossRef]
- Voigt, M.; Rochow, N.; Schneider, K.; Hagenah, H.-P.; Scholz, R.; Hesse, V.; Wittwer-Backofen, U.; Straube, S.; Olbertz, D. Neue perzentilwerte für die körpermaße neugeborener einlinge: Ergebnisse der deutschen perinatalerhebung der jahre 2007–2011 unter beteiligung aller 16 bundesländer. Z. Geburtshilfe Neonatol. 2014, 218, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.L. The international standard classification of education 2011. In Class and Stratification Analysis; Emerald Group Publishing Limited: Melbourne, Australia, 2013. [Google Scholar]
- Girard, L.C.; Doyle, O.; Tremblay, R.E. Breastfeeding and externalising problems: A quasi-experimental design with a national cohort. Eur. Child Adolesc. Psychiatry 2018, 27, 877–884. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.S.; Fombonne, E.; Igumnov, S.; Vanilovich, I.; Matush, L.; Mironova, E.; Bogdanovich, N.; Tremblay, R.E.; Chalmers, B.; Zhang, X.; et al. Effects of prolonged and exclusive breastfeeding on child behavior and maternal adjustment: Evidence from a large, randomized trial. Pediatrics 2008, 121, e435–e440. [Google Scholar] [CrossRef] [Green Version]
- Jackson, D.B. Breastfeeding duration and offspring conduct problems: The moderating role of genetic risk. Soc. Sci. Med. 2016, 166, 128–136. [Google Scholar] [CrossRef]
- Spiegler, J.; Preuss, M.; Gebauer, C.; Bendiks, M.; Herting, E.; Gopel, W.; German Neonatal Network. Does breastmilk influence the development of bronchopulmonary dysplasia? J. Pediatrics 2016, 169, 76–80.e74. [Google Scholar] [CrossRef]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Bar, S.; Milanaik, R.; Adesman, A. Long-term neurodevelopmental benefits of breastfeeding. Curr. Opin. Pediatrics 2016, 28, 559–566. [Google Scholar] [CrossRef]
- Zivkovic, A.M.; German, J.B.; Lebrilla, C.B.; Mills, D.A. Human milk glycobiome and its impact on the infant gastrointestinal microbiota. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4653–4658. [Google Scholar] [CrossRef] [Green Version]
- Pirr, S.; Richter, M.; Fehlhaber, B.; Pagel, J.; Hartel, C.; Roth, J.; Vogl, T.; Viemann, D. High amounts of s100-alarmins confer antimicrobial activity on human breast milk targeting pathogens relevant in neonatal sepsis. Front. Immunol. 2017, 8, 1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willers, M.; Ulas, T.; Vollger, L.; Vogl, T.; Heinemann, A.S.; Pirr, S.; Pagel, J.; Fehlhaber, B.; Halle, O.; Schoning, J.; et al. S100a8 and s100a9 are important for postnatal development of gut microbiota and immune system in mice and children. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Oades, R.D.; Myint, A.M.; Dauvermann, M.R.; Schimmelmann, B.G.; Schwarz, M.J. Attention-deficit hyperactivity disorder (adhd) and glial integrity: An exploration of associations of cytokines and kynurenine metabolites with symptoms and attention. Behav. Brain Funct. 2010, 6, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, B.; Aulenbach, J.; Meyer, T.; Wiegering, A.; Eyrich, M.; Schlegel, P.G.; Wiegering, V. Formula-feeding is associated with shift towards th1 cytokines. Eur. J. Nutr. 2015, 54, 129–138. [Google Scholar] [CrossRef]
- Caspi, A.; Williams, B.; Kim-Cohen, J.; Craig, I.W.; Milne, B.J.; Poulton, R.; Schalkwyk, L.C.; Taylor, A.; Werts, H.; Moffitt, T.E. Moderation of breastfeeding effects on the iq by genetic variation in fatty acid metabolism. Proc. Natl. Acad. Sci. USA 2007, 104, 18860–18865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krol, K.M.; Grossmann, T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 977–985. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Kim, B.N.; Kim, J.W.; Shin, M.S.; Yoo, H.J.; Cho, S.C. Protective effect of breastfeeding with regard to children’s behavioral and cognitive problems. Nutr. J. 2014, 13, 111. [Google Scholar] [CrossRef] [Green Version]
- Stadler, D.D.; Musser, E.D.; Holton, K.F.; Shannon, J.; Nigg, J.T. Recalled initiation and duration of maternal breastfeeding among children with and without adhd in a well characterized case-control sample. J. Abnorm. Child Psychol. 2016, 44, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Adesman, A.; Soled, D.; Rosen, L. Formula feeding as a risk factor for attention-deficit/hyperactivity disorder: Is bisphenol a treatment a smoking gun? J. Dev. Behav. Pediatrics 2017, 38, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Tillisch, K.; Labus, J.; Kilpatrick, L.; Jiang, Z.; Stains, J.; Ebrat, B.; Guyonnet, D.; Legrain-Raspaud, S.; Trotin, B.; Naliboff, B.; et al. Consumption of fermented milk product with probiotic modulates brain activity. Gastroenterology 2013, 144, 1394–1401. [Google Scholar] [CrossRef] [Green Version]
- Hartel, C.; Pagel, J.; Spiegler, J.; Buma, J.; Henneke, P.; Zemlin, M.; Viemann, D.; Gille, C.; Gehring, S.; Frommhold, D.; et al. Lactobacillus acidophilus/bifidobacterium infantis probiotics are associated with increased growth of vlbwi among those exposed to antibiotics. Sci. Rep. 2017, 7, 5633. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.; Wolke, D. A comparison of prematurity and small for gestational age as risk factors for age 6–13 year emotional problems. Early Hum. Dev. 2012, 88, 797–804. [Google Scholar] [CrossRef]
- Sell, K.; Rapp, M.; Muehlan, H.; Spiegler, J.; Thyen, U. Frequency of participation and association with functioning in adolescents born extremely preterm-findings from a population-based cohort in northern germany. Early Hum. Dev. 2018, 120, 67–73. [Google Scholar] [CrossRef]
- Michels, K.A.; Ghassabian, A.; Mumford, S.L.; Sundaram, R.; Bell, E.M.; Bello, S.C.; Yeung, E.H. Breastfeeding and motor development in term and preterm children in a longitudinal us cohort. Am. J. Clin. Nutr. 2017, 106, 1456–1462. [Google Scholar] [CrossRef] [Green Version]
- Linsell, L.; Malouf, R.; Morris, J.; Kurinczuk, J.J.; Marlow, N. Prognostic factors for poor cognitive development in children born very preterm or with very low birth weight: A systematic review. JAMA Pediatrics 2015, 169, 1162–1172. [Google Scholar] [CrossRef] [Green Version]
- Linsell, L.; Malouf, R.; Johnson, S.; Morris, J.; Kurinczuk, J.J.; Marlow, N. Prognostic factors for behavioral problems and psychiatric disorders in children born very preterm or very low birth weight: A systematic review. J. Dev. Behav. Pediatrics 2016, 37, 88–102. [Google Scholar] [CrossRef] [Green Version]
- Walfisch, A.; Sermer, C.; Cressman, A.; Koren, G. Breast milk and cognitive development-the role of confounders: A systematic review. BMJ Open 2013, 3, e003259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banaschewski, T.; Becker, K.; Dopfner, M.; Holtmann, M.; Rosler, M.; Romanos, M. Attention-deficit/hyperactivity disorder. Dtsch. Arztebl. Int. 2017, 114, 149–159. [Google Scholar] [PubMed] [Green Version]
- Instanes, J.T.; Klungsoyr, K.; Halmoy, A.; Fasmer, O.B.; Haavik, J. Adult adhd and comorbid somatic disease: A systematic literature review. J. Atten. Disord. 2018, 22, 203–228. [Google Scholar] [CrossRef] [Green Version]
| Excluded | Included in Analysis | ||||
|---|---|---|---|---|---|
| N = 8250 | Breastfeeding < 3 month N = 298 | Breastfeeding ≥ 3 month N = 2169 | p-Value | ||
| Gestational age (weeks) | 29.1 (26.8–31.0) # | 28.1 (26.0–29.4) | 27.9 (26.1–29.4) | n.s. | |
| Female gender | 4043/8250 (49.0%) | 138/298 (46.3%) | 1034/2169 (47.7%) | n.s. | |
| Multiple | 2707/10717 (32.8%) # | 116/298 (38.9%) | 869/2169 (40.1%) | n.s. | |
| Birth weight | 1125 (840–1350) # | 960 (730–1210) | 980 (745–1220) | n.s. | |
| SGA | 1616/8250 (19.6%) # | 50/298 (16.8%) | 296/2169 (13.6%) | n.s. | |
| BPD | 1269/8246 (15.4%) # | 82/298 (27.5%) | 438/2169 (20.2%) | 0.004 | |
| IVH | 1373/8238 (16.7%) # | 48/298 (16.1%) | 407/2169 (18.8%) | n.s. | |
| Probiotics | 4787/6776 (70.3%) # | 174/226 (77%) | 1218/1625 (75%) | n.s. | |
| Maternal age | 31 (27–35) # | 31 (27–35) | 31 (28–32) | 0.04 | |
| Motor impairment | 98/298 (32.9%) | 569/2169 (26.2%) | 0.015 | ||
| Maternal education | Low | 93/278 (33.5%) | 280/2096 (13.4%) | <0.001 | |
| Medium | 109/278 (39.2%) | 714/2096 (34.1%) | |||
| High | 76/278 (27.3%) | 1102/2096 (52.6%) | |||
| SDQ total score | 10 (6–15) | 9 (5–13) | <0.001 | ||
| SDQ inattention/hyperactivity | 5 (3–7) | 4 (2–5) | <0.001 | ||
| Outcome Treatments | SDQ Total Score B (95% CI) | Emotional Symptoms B (95% CI) | Conduct Problems B (95% CI) | Hyperactivity/Inattention B (95% CI) | Peer Relationship Problems B (95% CI) | Prosocial Behavior B (95% CI) | IQ B (95% CI) |
|---|---|---|---|---|---|---|---|
| Sex: female vs male | −0.53 (−1.02–(−0.04)) | 0.40 (0.22–0.57) | −0.22 (−0.37–(−0.08)) | −0.59 (−0.82–(−0.36)) | −0.12 (−0.28–0.05) | 0.57 (0.40–0.74) | −0.13 (−1.27–1.00) |
| Gestational age (in weeks) | −0.31 (−0.43–(−0.19)) | −0.02 (−0.06–0.02) | −0.01 (−0.04–0.03) | −0.17 (−0.23–(−0.12)) | −0.11 (−0.15–(−0.07)) | 0.03 (−0.01–0.08) | 1.00 (0.73–1.28) |
| High vs medium/low maternal education | −0.82 (−1.16–(−0.48)) | −0.13 (−0.25–(−0.004)) | −0.28 (−0.38–(−0.18)) | −0.36 (−0.52–(−0.20)) | −0.05 (−0.17–0.06) | 0.07 (−0.05–0.19) | 4.31 (3.51–5.11) |
| SGA (yes vs no) | 1.28 (0.55–2.01) | 0.14 (−0.12–0.4) | 0.15 (−0.06–0.36) | 0.81 (0.47–1.15) | 0.18 (−0.06–0.42) | −0.17 (−0.43–0.19) | −3.31 (−5.04–(−1.58) |
| Multiples (yes vs no) | −0.81 (−1.31–(−0.30)) | −0.29 (−0.47–(−0.11)) | 0.02 (−0.13–0.17) | −0.45 (−0.68–(−0.21)) | −0.09 (−0.26–0.08) | −0.04 (−0.22–0.13) | −0.72 (−1.87–0.43) |
| Maternal age (in years) | −0.08 (−0.13–(−0.04)) | −0.03 (−0.05–(−0.02)) | −0.01 (0.02–0.01) | −0.05 (−0.07–(−0.03)) | 0.004 (−0.01–0.02) | −0.01 (−0.02–0.01) | 0.15 (0.41–0.26) |
| BPD (yes vs no) | 1.31 (0.65–1.97) | 0.16 (−0.07–0.40) | 0.07 (−0.13–0.26) | 0.64 (0.33–0.94) | 0.45 (0.23–0.67) | −0.34 (−0.57–(−0.11)) | −2.93 (−4.51–(−1.34)) |
| Motor impairment (yes vs no) | 1.31 (0.70–1.92) | 0.05 (−0.172–0.27) | 0.01 (−0.17–0.19) | 0.49 (0.21–0.77) | 0.76 (0.56–0.96) | −0.57 (−0.78–(−0.36)) | −6.18 (−7.65–(−4.71)) |
| Probiotics (yes vs no) | 0.12 (−0.45–0.69) | −0.10 (−0.31–0.10) | 0.03 (−0.13–0.20) | 0.05 (−0.21–0.31) | 0.14 (−0.05–0.33) | −0.19 (−0.39–0.01) | 0.94 (−0.37–2.26) |
| Breastfeeding ≥ 3 vs < 3 months | −0.58 (−1.35–0.18) | 0.23 (−0.05–0.50) | −0.25 (−0.47–(−0.03)) | −0.46 (−0.81–(−0.10)) | −0.10 (−0.36–0.15) | 0.07 (−0.20–0.34) | 2.20 (0.43–3.97) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Härtel, C.; Spiegler, J.; Fortmann, I.; Astiz, M.; Oster, H.; Siller, B.; Viemann, D.; Keil, T.; Banaschewski, T.; Romanos, M.; et al. Breastfeeding for 3 Months or Longer but Not Probiotics Is Associated with Reduced Risk for Inattention/Hyperactivity and Conduct Problems in Very-Low-Birth-Weight Children at Early Primary School Age. Nutrients 2020, 12, 3278. https://doi.org/10.3390/nu12113278
Härtel C, Spiegler J, Fortmann I, Astiz M, Oster H, Siller B, Viemann D, Keil T, Banaschewski T, Romanos M, et al. Breastfeeding for 3 Months or Longer but Not Probiotics Is Associated with Reduced Risk for Inattention/Hyperactivity and Conduct Problems in Very-Low-Birth-Weight Children at Early Primary School Age. Nutrients. 2020; 12(11):3278. https://doi.org/10.3390/nu12113278
Chicago/Turabian StyleHärtel, Christoph, Juliane Spiegler, Ingmar Fortmann, Mariana Astiz, Henrik Oster, Bastian Siller, Dorothee Viemann, Thomas Keil, Tobias Banaschewski, Marcel Romanos, and et al. 2020. "Breastfeeding for 3 Months or Longer but Not Probiotics Is Associated with Reduced Risk for Inattention/Hyperactivity and Conduct Problems in Very-Low-Birth-Weight Children at Early Primary School Age" Nutrients 12, no. 11: 3278. https://doi.org/10.3390/nu12113278
APA StyleHärtel, C., Spiegler, J., Fortmann, I., Astiz, M., Oster, H., Siller, B., Viemann, D., Keil, T., Banaschewski, T., Romanos, M., Herting, E., & Göpel, W. (2020). Breastfeeding for 3 Months or Longer but Not Probiotics Is Associated with Reduced Risk for Inattention/Hyperactivity and Conduct Problems in Very-Low-Birth-Weight Children at Early Primary School Age. Nutrients, 12(11), 3278. https://doi.org/10.3390/nu12113278