Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review



Abstract
:1. Introduction
2. Material and Methods
2.1. Types of Studies
2.2. Type of Participants
2.3. Types of Interventions
2.4. Types of Outcome Measures
2.5. Search Methods
2.6. Selection of Articles
2.7. Data Extraction and Management
2.8. Assessment of Risk of Bias in Included Studies
2.9. Measures of Treatment Effect
2.10. Dealing with Missing Data
2.11. Assessment of Heterogeneity
2.12. Data Synthesis
3. Results
3.1. Bias Assessment
3.2. Summary of Findings
3.2.1. Therapeutic Trials (Gastroenteritis)
Heat-Killed L. Acidophilus LB
Fermented Formula with B. Breve C50 and Str. Thermophilus 065
3.2.2. Prevention Trials
Heat-Killed L. Paracasei CBA L74
Fermented Formula with B. Breve C50 (BbC50) and Str. Thermophilus 065
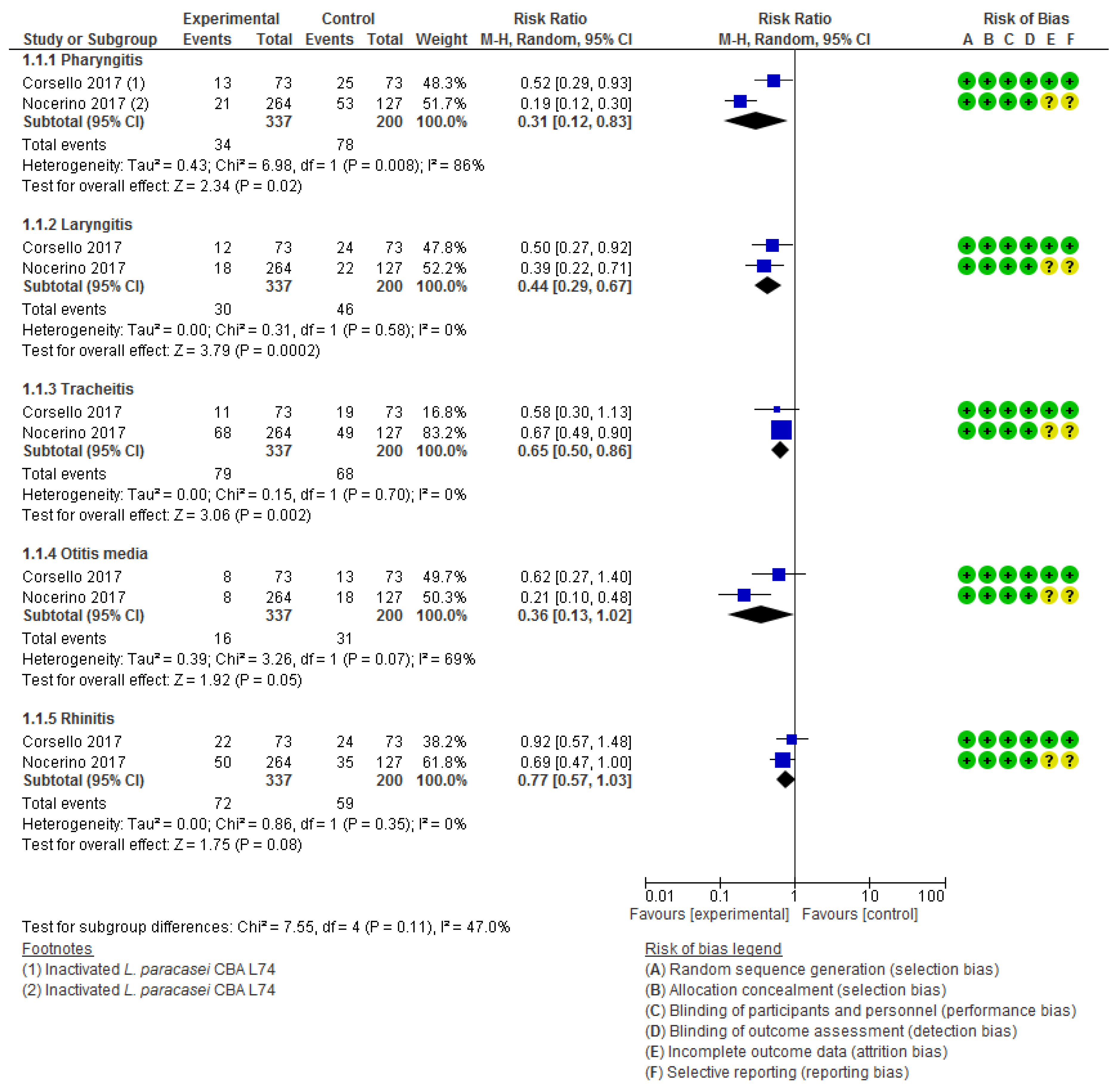
Heat-Inactivated L. Paracasei CBA L74
3.3. Adverse Effects
4. Discussion
4.1. Limitations
4.2. Comparison with Previous Reports
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Maldonado, J.; Cañabate, F.; Sempere, L.; Vela, F.; Sánchez, A.; Narbona, E.; López-Huertas, E.; Geerlings, A.; Valero, A.; Olivares, M.; et al. Human Milk Probiotic Lactobacillus fermentum CECT5716 Reduces the Incidence of Gastrointestinal and Upper Respiratory Tract Infections in Infants. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 55–61. [Google Scholar] [CrossRef]
- Wang, Y.; Li, X.; Ge, T.; Xiao, Y.; Liao, Y.; Cui, Y.; Zhang, Y.; Ho, W.; Yu, G.; Zhang, T. Probiotics for prevention and treatment of respiratory tract infections in children. Medicine (Baltimore) 2016, 95. [Google Scholar] [CrossRef] [PubMed]
- Amaral, M.A.; Guedes, G.H.B.F.; Epifanio, M.; Wagner, M.B.; Jones, M.H.; Mattiello, R. Network meta-analysis of probiotics to prevent respiratory infections in children and adolescents. Pediatr. Pulmonol. 2017, 52, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Bidossi, A.; De Grandi, R.; Toscano, M.; Bottagisio, M.; De Vecchi, E.; Gelardi, M.; Drago, L. Probiotics Streptococcus salivarius 24SMB and Streptococcus oralis 89a interfere with biofilm formation of pathogens of the upper respiratory tract. BMC Infect. Dis. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Kara, S.S.; Volkan, B.; Erten, I. Lactobacillus rhamnosus GG can protect malnourished children. Benef. Microbes 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hojsak, I. Probiotics in Children: What Is the Evidence? Pediatr. Gastroenterol. Hepatol. Nutr. 2017, 20, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emblelton, N.; Zalewski, S.; Berrington, J. Probiotics for prevention of necrotizing enterocolitis and sepsis in preterm infants. –PubMed–NCBI. Available online: https://www.ncbi.nlm.nih.gov/pubmed/27023404 (accessed on 14 March 2019).
- Dani, C.; Coviello, C.C.; Corsini, I.I.; Arena, F.; Antonelli, A.; Rossolini, G.M. Lactobacillus Sepsis and Probiotic Therapy in Newborns: Two New Cases and Literature Review. AJP Rep. 2016, 6, e25–e29. [Google Scholar] [PubMed] [Green Version]
- Kane, A.F.; Bhatia, A.D.; Denning, P.W.; Shane, A.L.; Patel, R.M. Routine Supplementation of Lactobacillus rhamnosus GG and Risk of Necrotizing Enterocolitis in Very Low Birth Weight Infants. J. Pediatr. 2018, 195, 73–79.e2. [Google Scholar] [CrossRef]
- Robin, F.; Paillard, C.; Marchandin, H.; Demeocq, F.; Bonnet, R.; Hennequin, C. Lactobacillus rhamnosus Meningitis following Recurrent Episodes of Bacteremia in a Child Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. J. Clin. Microbiol. 2010, 48, 4317–4319. [Google Scholar] [CrossRef] [Green Version]
- Reid, B.M.; Thompson-Branch, A. Necrotizing Enterocolitis: A Narrative Review of Updated Therapeutic and Preventive Interventions. J. Pediatr. Rev. 2016, 4, e6093. [Google Scholar] [CrossRef]
- Rowan, N.J.; Deans, K.; Anderson, J.G.; Gemmell, C.G.; Hunter, I.S.; Chaithong, T. Putative virulence factor expression by clinical and food isolates of Bacillus spp. after growth in reconstituted infant milk formulae. Appl. Environ. Microbiol. 2001, 67, 3873–3881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, A.; Ngu, D.Y.S.; Dan, L.A.; Ooi, A.; Lim, R.L.H. Detection of antibiotic resistance in probiotics of dietary supplements. Nutr. J. 2015, 14, 95. [Google Scholar] [CrossRef] [PubMed]
- Aceti, A.; Beghetti, I.; Maggio, L.; Martini, S.; Faldella, G.; Corvaglia, L. Filling the Gaps: Current Research Directions for a Rational Use of Probiotics in Preterm Infants. Nutrients 2018, 10, 1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaila, M.; Isolauri, E.; Saxelin, M.; Arvilommi, H.; Vesikari, T. Viable versus inactivated lactobacillus strain GG in acute rotavirus diarrhoea. Arch. Dis. Child. 1995, 72, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Merenstein, D.; Murphy, M.; Fokar, A.; Hernandez, R.K.; Park, H.; Nsouli, H.; Sanders, M.E.; Davis, B.A.; Niborski, V.; Tondu, F.; et al. Use of a fermented dairy probiotic drink containing Lactobacillus casei (DN-114 001) to decrease the rate of illness in kids: The DRINK study A patient-oriented, double-blind, cluster-randomized, placebo-controlled, clinical trial. Eur. J. Clin. Nutr. 2010, 64, 669–677. [Google Scholar] [CrossRef] [Green Version]
- Campeotto, F.; Suau, A.; Kapel, N.; Magne, F.; Viallon, V.; Ferraris, L.; Waligora-Dupriet, A.-J.; Soulaines, P.; Leroux, B.; Kalach, N.; et al. A fermented formula in pre-term infants: Clinical tolerance, gut microbiota, down-regulation of faecal calprotectin and up-regulation of faecal secretory IgA. Br. J. Nutr. 2011, 105, 1843–1851. [Google Scholar] [CrossRef]
- Collado, M.C.; Vinderola, G.; Salminen, S. Postbiotics: Facts and open questions. A position paper on the need for a consensus definition. Benef. Microbes 2019, 10, 711–719. [Google Scholar] [CrossRef]
- Chapot-Chartier, M.-P.; Vinogradov, E.; Sadovskaya, I.; Andre, G.; Mistou, M.-Y.; Trieu-Cuot, P.; Furlan, S.; Bidnenko, E.; Courtin, P.; Péchoux, C.; et al. Cell Surface of Lactococcus lactis Is Covered by a Protective Polysaccharide Pellicle. J. Biol. Chem. 2010, 285, 10464–10471. [Google Scholar] [CrossRef] [Green Version]
- Paul, D.; Manna, S.; Mandal, S.M. Antibiotics Associated Disorders and Post-biotics Induced Rescue in Gut Health. Curr. Pharm. Des. 2018, 24, 821–829. [Google Scholar] [CrossRef]
- Frece, J.; Kos, B.; Svetec, I.K.; Zgaga, Z.; Mrša, V.; Šušković, J. Importance of S-layer proteins in probiotic activity of Lactobacillus acidophilus M92. J. Appl. Microbiol. 2005, 98, 285–292. [Google Scholar] [CrossRef]
- Mogensen, T.H. Pathogen Recognition and Inflammatory Signaling in Innate Immune Defenses. Clin. Microbiol. Rev. 2009, 22, 240–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawai, T.; Akira, S. The roles of TLRs, RLRs and NLRs in pathogen recognition. Int. Immunol. 2009, 21, 317–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feerick, C.L.; McKernan, D.P. Understanding the regulation of pattern recognition receptors in inflammatory diseases—A ‘Nod’ in the right direction. Immunology 2017, 150, 237–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.W.; Kang, S.; Woo, S.; Park, O.; Ahn, K.B.; Song, K.; Lee, H.; Yun, C.; Han, S.H. Lipoteichoic Acid of Probiotic Lactobacillus plantarum Attenuates Poly I: C-Induced IL-8 Production in Porcine Intestinal Epithelial Cells. Front. Microbiol. 2017, 8, 1–8. [Google Scholar] [CrossRef]
- Miniello, V.L.; Colasanto, A.; Cristofori, F.; Diaferio, L.; Ficele, L.; Lieggi, M.S.; Santoiemma, V.; Francavilla, R. Gut microbiota biomodulators, when the stork comes by the scalpel. Clin. Chim. Acta 2015, 451, 88–96. [Google Scholar] [CrossRef]
- Romond, M.B.; Ais, A.; Yazourh, A.; Romond, C. Cell-free Wheys From Bifidobacteria Fermented Milks Exert a Regulatory Effect on the Intestinal Microflora of Mice and Humans. Anaerobe 1997, 3, 137–143. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions. 2019. Available online: https://training.cochrane.org/handbook (accessed on 29 January 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Home–ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ (accessed on 30 January 2020).
- EU Clinical Trials Register–Update. Available online: https://www.clinicaltrialsregister.eu/ (accessed on 30 January 2020).
- National Health and Medical Research Council PROSPERO. Available online: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=133387 (accessed on 30 January 2020).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Chapter 8: Assessing risk of bias in a randomized trial. 2019. Available online: https://training.cochrane.org/handbook/current/chapter-08 (accessed on 29 January 2020).
- Nocerino, R.; Paparo, L.; Terrin, G.; Pezzella, V.; Amoroso, A.; Cosenza, L.; Cecere, G.; De Marco, G.; Micillo, M.; Albano, F.; et al. Cow’s milk and rice fermented with Lactobacillus paracasei CBA L74 prevent infectious diseases in children: A randomized controlled trial. Clin. Nutr. 2017, 36, 118–125. [Google Scholar] [CrossRef]
- Boulloche, J.; Mouterde, O.; Mallet, E. Management of Acute Diarrhea in Infants and Toddlers - Controlled-Study. Ann. Pédiatrie 1994, 41, 457–463. [Google Scholar]
- Liévin-Le Moal, V.; Sarrazin-Davila, L.E.; Servin, A.L. An Experimental Study and a Randomized, Double-Blind, Placebo-Controlled Clinical Trial to Evaluate the Antisecretory Activity of Lactobacillus acidophilus Strain LB Against Nonrotavirus Diarrhea. Pediatrics 2007, 120, e795–e803. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Lindo, E.; Figueroa-Quintanilla, D.; Caciano, M.; Reto-Valiente, V.; Chauviere, G.; Colin, P. Effectiveness and Safety of Lactobacillus LB in the Treatment of Mild Acute Diarrhea in Children. J. Pediatr. Gastroenterol. Nutr. 2007, 44, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Simakachorn, N.; Pichaipat, V.; Rithipornpaisarn, P.; Kongkaew, C.; Tongpradit, P.; Varavithya, W. Clinical Evaluation of the Addition of Lyophilized, Heat-Killed Lactobacillus acidophilus LB to Oral Rehydration Therapy in the Treatment of Acute Diarrhea in Children. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Thibault, H.; Aubert-Jacquin, C.; Goulet, O. Effects of Long-term Consumption of a Fermented Infant Formula (with Bifidobacterium breve c50 and Streptococcus thermophilus 065) on Acute Diarrhea in Healthy Infants. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 147–152. [Google Scholar] [CrossRef]
- Corsello, G.; Carta, M.; Marinello, R.; Picca, M.; De Marco, G.; Micillo, M.; Ferrara, D.; Vigneri, P.; Cecere, G.; Ferri, P.; et al. Preventive Effect of Cow’s Milk Fermented with Lactobacillus paracasei CBA L74 on Common Infectious Diseases in Children: A Multicenter Randomized Controlled Trial. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Sharieff, W.; Bhutta, Z.; Schauer, C.; Tomlinson, G.; Zlotkin, S. Micronutrients (including zinc) reduce diarrhoea in children: The Pakistan Sprinkles Diarrhoea Study. Arch. Dis. Child. 2006, 91, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Azad, M.A.K.; Sarker, M.; Wan, D. Immunomodulatory Effects of Probiotics on Cytokine Profiles. Available online: https://www.hindawi.com/journals/bmri/2018/8063647/ (accessed on 29 January 2020).
- Łukasik, J.; Salminen, S.; Szajewska, H. Rapid review shows that probiotics and fermented infant formulas do not cause d-lactic acidosis in healthy children. Acta Paediatr. 2018, 107, 1322–1326. [Google Scholar] [CrossRef]
- Wegh, C.A.M.; Geerlings, S.Y.; Knol, J.; Roeselers, G.; Belzer, C. Postbiotics and Their Potential Applications in Early Life Nutrition and Beyond. Int. J. Mol. Sci. 2019, 20. [Google Scholar] [CrossRef] [Green Version]
- Taverniti, V.; Guglielmetti, S. The immunomodulatory properties of probiotic microorganisms beyond their viability (ghost probiotics: Proposal of paraprobiotic concept). Genes Nutr. 2011, 6, 261–274. [Google Scholar] [CrossRef] [Green Version]
- Ouwehand, A.C.; Tölkkö, S.; Kulmala, J.; Salminen, S.; Salminen, E. Adhesion of inactivated probiotic strains to intestinal mucus. Lett. Appl. Microbiol. 2000, 31, 82–86. [Google Scholar] [CrossRef]
- Szajewska, H.; Ruszczyński, M.; Kolaček, S. Meta-analysis shows limited evidence for using Lactobacillus acidophilus LB to treat acute gastroenteritis in children. Acta Paediatr. 2014, 103, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Liévin-Le Moal, V. A gastrointestinal anti-infectious biotherapeutic agent: The heat-treated Lactobacillus LB. Ther. Adv. Gastroenterol. 2016, 9, 57–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szajewska, H.; Guarino, A.; Hojsak, I.; Indrio, F.; Kolacek, S.; Shamir, R.; Vandenplas, Y.; Weizman, Z. Use of Probiotics for Management of Acute Gastroenteritis: A Position Paper by the ESPGHAN Working Group for Probiotics and Prebiotics. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 531–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szajewska, H.; Skórka, A.; Pieścik-Lech, M. Fermented infant formulas without live bacteria: A systematic review. Eur. J. Pediatr. 2015, 174, 1413–1420. [Google Scholar] [CrossRef]
- Agostoni, C.; Goulet, O.; Kolacek, S.; Koletzko, B.; Moreno, L.; Puntis, J.; Rigo, J.; Shamir, R.; Szajewska, H.; Turck, D. Fermented Infant Formulae Without Live Bacteria. J. Pediatr. Gastroenterol. Nutr. 2007, 44, 392–397. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year, Country) | Age | Population (n) | Intervention and Control Group | Duration of the Intervention | Primary Outcome Measured | Definition of the Primary Outcome |
|---|---|---|---|---|---|---|
| Boulloche J, 1994 (France) [36] | 1 to 48 mo | Acute diarrhoea (n = 71) | Heat killed L. acidophilus LB vs placebo | 4 days | Duration of diarrhoea | The first normal stool. |
| Simakachorn (Thailand) N,2000 [39] | 3 to 24 mo | Acute diarrhoea without severe dehydration (n = 73) | Lyophilized heat-killed L. acidophilus LB vs placebo | 5 days | Diarrhoea duration | The end of the diarrhoea was defined as two consecutive well-formed stools followed an unformed stool or when no stool was passed for 12 h. |
| Thibault H, 2004 (France) [40] | 4 to 6 mo | Healthy infants (n = 913) | Fermented formula with heat-killed Bifidobacterium breve C50 and Streptococcus thermophilus vs placebo | 5 months |
| Duration was defined as the time passed between the first diarrhoea episode and when the stools were formed. |
| Salazar-Lindo, 2007 (Peru) [38] | 3 to 48 mo | Acute diarrhoea (less than 3 days) (n = 80) | Heat killed Lactobacillus LB vs placebo | 4,5 days | Duration of diarrhoea caused by non-rotavirus | The time to the first normal stool followed by 2 consecutive normal stools |
| Levin-Le Moal, V., 2007 (Ecuador) [37] | 1 to 12 mo | Acute diarrhoea (n = 80) | Heat killed L. acidophilus LB vs placebo | 4 days | Duration of the diarrhoea episode | Time passed between the first diarrhoea episode and when the stools were formed. |
| Nocerino R, 2017 (Italy) [35] | 12 to 48 mo | Healthy children attending to day care or preschool at least five days a week (n = 377) | Cow’s milk or rice with fermented milk with L. paracasei CBA L74 and inactivated vs placebo | 3 months | Proportion of children experiencing at least one episode of common infectious disease |
|
| Corsello G, 2017 (Italy) [41] | 12 to 48 mo | Healthy children, attending day care or preschool for at least 5 days a week (n = 146). | Lyophilized heat-killed L. paracasei CBA L74 vs placebo | 3 months | The rate of children experiencing at least one episode of Common infectious disease |
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malagón-Rojas, J.N.; Mantziari, A.; Salminen, S.; Szajewska, H. Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review. Nutrients 2020, 12, 389. https://doi.org/10.3390/nu12020389
Malagón-Rojas JN, Mantziari A, Salminen S, Szajewska H. Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review. Nutrients. 2020; 12(2):389. https://doi.org/10.3390/nu12020389
Chicago/Turabian StyleMalagón-Rojas, Jeadran N., Anastasia Mantziari, Seppo Salminen, and Hania Szajewska. 2020. "Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review" Nutrients 12, no. 2: 389. https://doi.org/10.3390/nu12020389
APA StyleMalagón-Rojas, J. N., Mantziari, A., Salminen, S., & Szajewska, H. (2020). Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review. Nutrients, 12(2), 389. https://doi.org/10.3390/nu12020389