First-degree Relatives of Celiac Disease Patients Have Increased Seroreactivity to Serum Microbial Markers

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. CD Autoantibodies and Genotyping
2.3. Microbial Antibodies
2.4. Statistical Analysis
2.5. Ethical Aspects
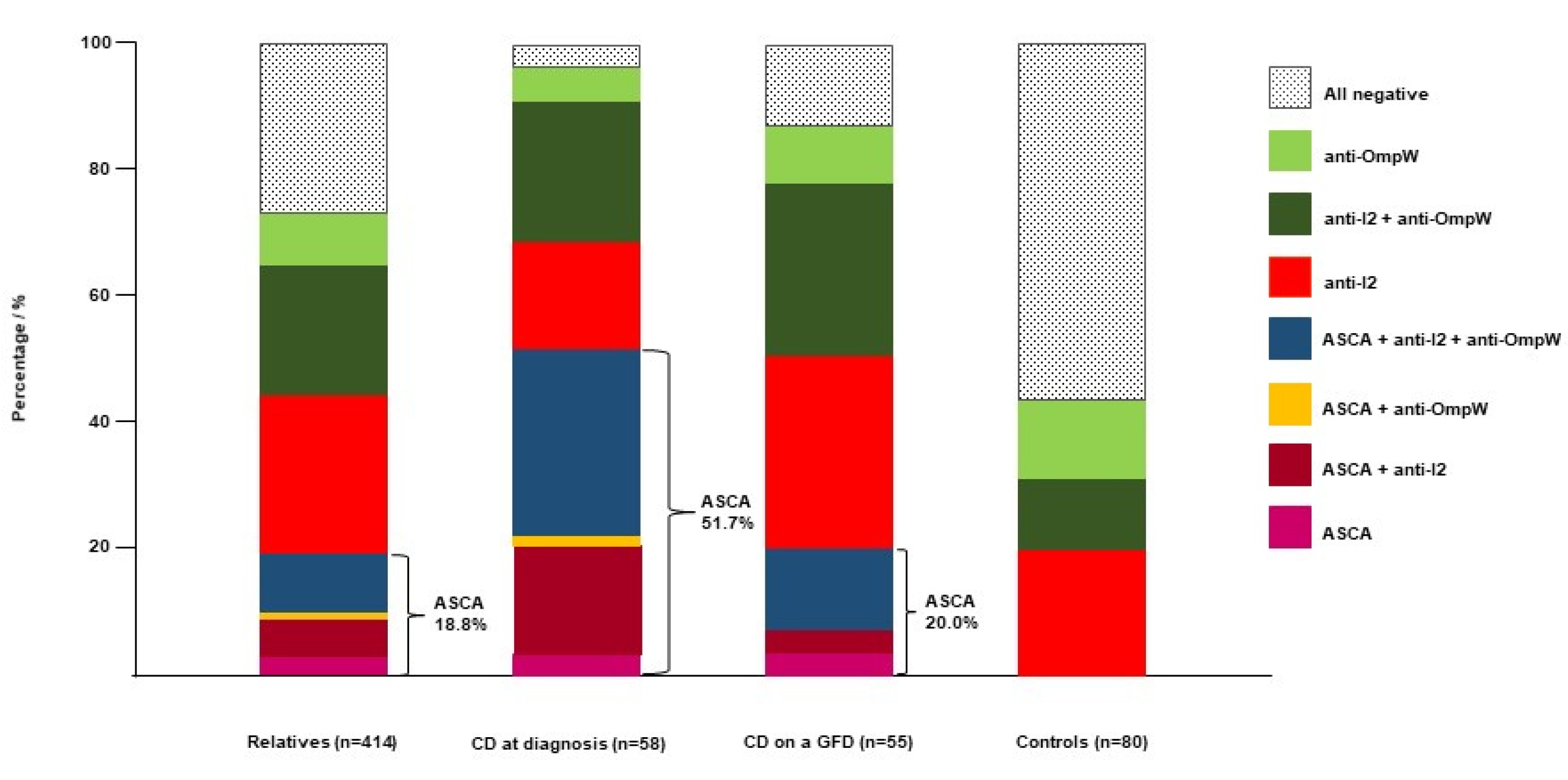
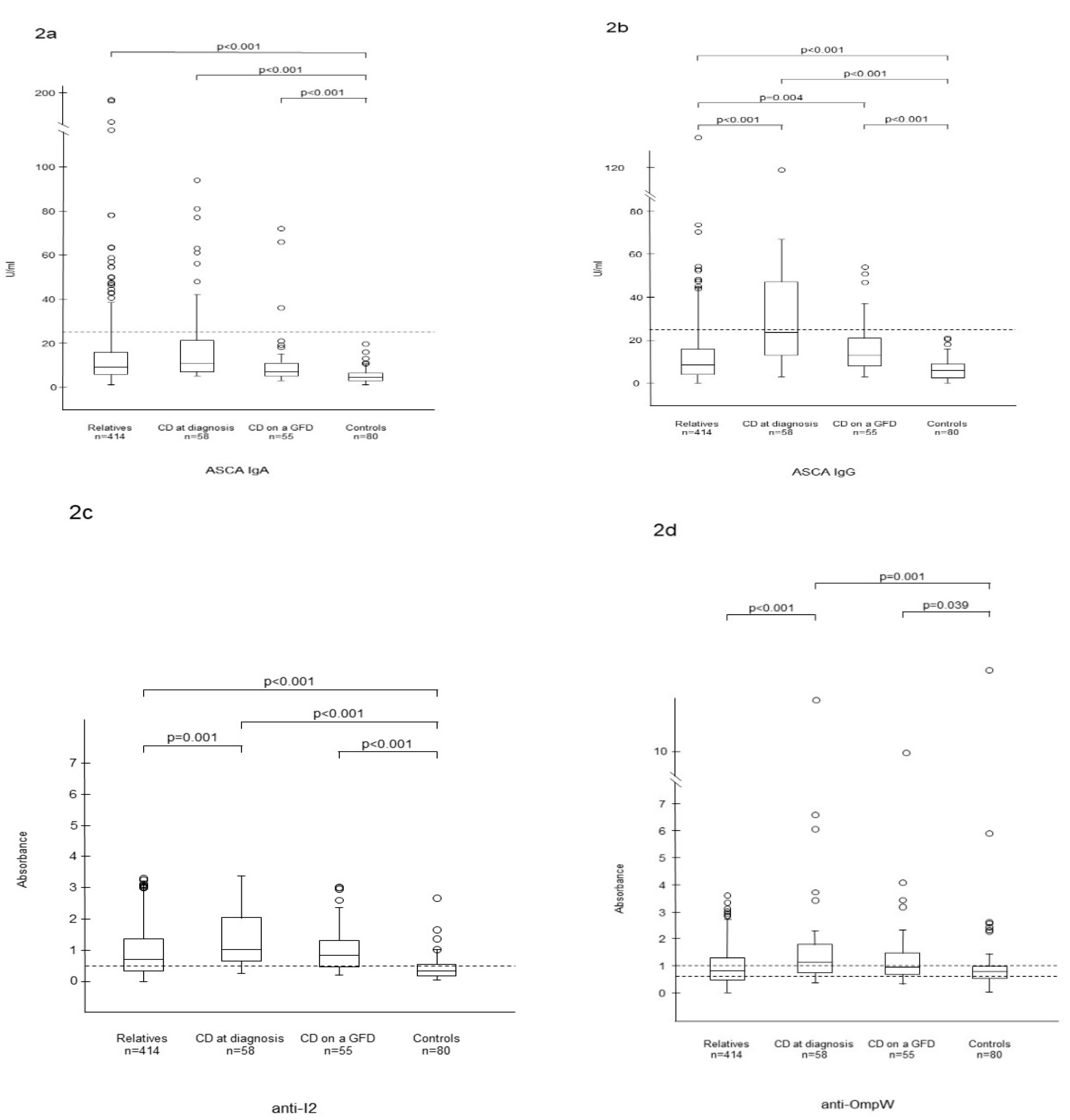
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kapitany, A.; Toth, L.; Tumpek, J.; Csipo, I.; Sipos, E.; Woolley, N.; Partanen, J.; Szegedi, G.; Olah, E.; Sipka, S.; et al. Diagnostic significance of HLA-DQ typing in patients with previous coeliac disease diagnosis based on histology alone. Aliment. Pharmacol. Ther. 2006, 24, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Wijmenga, C.; Gutierrez-Achury, J. Celiac disease genetics: Past, present and future challenges. J. Pediatr. Gastroenterol. Nutr. 2014, 59, S4–S7. [Google Scholar] [CrossRef] [PubMed]
- Trynka, G.; Hunt, K.A.; Bockett, N.A.; Romanos, J.; Mistry, V.; Szperl, A.; Bakker, S.F.; Bardella, M.T.; Bhaw-Rosun, L.; Castillejo, G.; et al. Dense genotyping identifies and localizes multiple common and rare variant association signals in celiac disease. Nat. Genet. 2011, 43, 1193–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, C.; Quinn, E.M.; Ryan, A.W.; Conroy, J.; Trimble, V.; Mahmud, N.; Kennedy, N.; Corvin, A.P.; Morris, D.W.; Donohoe, G.; et al. Common polygenic variation in coeliac disease and confirmation of ZNF335 and NIFA as disease susceptibility loci. Eur. J. Hum. Genet. 2016, 24, 291–297. [Google Scholar] [CrossRef]
- Singh, P.; Arora, S.; Lal, S.; Strand, T.A.; Makharia, G.K. Risk of celiac Disease in the first- and second-degree relatives of patients with celiac disease: A systematic review and meta-analysis. Am. J. Gastroenterol. 2015, 110, 1539–1548. [Google Scholar] [CrossRef]
- Lohi, S.; Mustalahti, K.; Kaukinen, K.; Laurila, K.; Collin, P.; Rissanen, H.; Lohi, O.; Bravi, E.; Gasparin, M.; Reunanen, A.; et al. Increasing prevalence of coeliac disease over time. Aliment. Pharmacol. Ther. 2007, 26, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Mäki, M.; Mustalahti, K.; Kokkonen, J.; Kulmala, P.; Haapalahti, M.; Karttunen, T.; Ilonen, J.; Laurila, K.; Dahlbom, I.; Hansson, T.; et al. Prevalence of celiac disease among children in Finland. N. Engl. J. Med. 2003, 348, 2517–2524. [Google Scholar] [CrossRef] [Green Version]
- Hervonen, K.; Karell, K.; Holopainen, P.; Collin, P.; Partanen, J.; Reunala, T. Concordance of dermatitis herpetiformis and celiac disease in monozygous twins. J. Invest. Dermatol. 2000, 115, 990–993. [Google Scholar] [CrossRef] [Green Version]
- Kuja-Halkola, R.; Lebwohl, B.; Halfvarson, J.; Wijmenga, C.; Magnusson, P.K.; Ludvigsson, J.F. Heritability of non-HLA genetics in coeliac disease: A population-based study in 107,000 twins. Gut 2016, 65, 1793–1798. [Google Scholar] [CrossRef] [Green Version]
- Kondrashova, A.; Mustalahti, K.; Kaukinen, K.; Viskari, H.; Volodicheva, V.; Haapala, A.M.; Ilonen, J.; Knip, M.; Mäki, M.; Hyöty, H.; et al. Lower economic status and inferior hygienic environment may protect against celiac disease. Ann. Med. 2008, 40, 223–231. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Kyle, R.A.; Kaplan, E.L.; Johnson, D.R.; Page, W.; Erdtmann, F.; Brantner, T.L.; Kim, W.R.; Phelps, T.K.; Lahr, B.D.; et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology 2009, 137, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catassi, C.; Kryszak, D.; Bhatti, B.; Sturgeon, C.; Helzlsouer, K.; Clipp, S.L.; Gelfond, D.; Puppa, E.; Sferruzza, A.; Fasano, A. Natural history of celiac disease autoimmunity in a USA cohort followed since 1974. Ann. Med. 2010, 42, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Nadal, I.; Donat, E.; Ribes-Koninckx, C.; Calabuig, M.; Sanz, Y. Imbalance in the composition of the duodenal microbiota of children with coeliac disease. J. Med. Microbiol. 2007, 56, 1669–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Palma, G.; Nadal, I.; Medina, M.; Donat, E.; Ribes-Koninckx, C.; Calabuig, M.; Sanz, Y. Intestinal dysbiosis and reduced immunoglobulin-coated bacteria associated with coeliac disease in children. BMC Microbiol. 2010, 10, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collado, M.C.; Donat, E.; Ribes-Koninckx, C.; Calabuig, M.; Sanz, Y. Specific duodenal and faecal bacterial groups associated with paediatric coeliac disease. J. Clin. Pathol. 2009, 62, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iltanen, S.; Tervo, L.; Halttunen, T.; Wei, B.; Braun, J.; Rantala, I.; Honkanen, T.; Kronenberg, M.; Cheroutre, H.; Turovskaya, O.; et al. Elevated serum anti-I2 and anti-OmpW antibody levels in children with IBD. Inflamm. Bowel Dis. 2006, 12, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Ashorn, S.; Honkanen, T.; Kolho, K.L.; Ashorn, M.; Välineva, T.; Wei, B.; Braun, J.; Rantala, I.; Luukkaala, T.; Iltanen, S. Fecal calprotectin levels and serological responses to microbial antigens among children and adolescents with inflammatory bowel disease. Inflamm. Bowel Dis. 2009, 15, 199–205. [Google Scholar] [CrossRef]
- Landers, C.J.; Cohavy, O.; Misra, R.; Yang, H.; Lin, Y.C.; Braun, J.; Targan, S.R. Selected loss of tolerance evidenced by Crohn’s disease-associated immune responses to auto- and microbial antigens. Gastroenterology 2002, 123, 689–699. [Google Scholar] [CrossRef]
- Ashorn, S.; Raukola, H.; Välineva, T.; Ashorn, M.; Wei, B.; Braun, J.; Rantala, I.; Kaukinen, K.; Luukkaala, T.; Collin, P.; et al. Elevated serum anti-Saccharomyces cerevisiae, anti-I2 and anti-OmpW antibody levels in patients with suspicion of celiac disease. J. Clin. Immunol. 2008, 28, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Ashorn, S.; Välineva, T.; Kaukinen, K.; Ashorn, M.; Braun, J.; Raukola, H.; Rantala, I.; Collin, P.; Mäki, M.; Luukkaala, T.; et al. Serological responses to microbial antigens in celiac disease patients during a gluten-free diet. J. Clin. Immunol. 2009, 29, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Viitasalo, L.; Niemi, L.; Ashorn, M.; Ashorn, S.; Braun, J.; Huhtala, H.; Collin, P.; Mäki, M.; Kaukinen, K.; Kurppa, K.; et al. Early microbial markers of celiac disease. J. Clin. Gastroenterol. 2014, 48, 620–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladinser, B.; Rossipal, E.; Pittschieler, K. Endomysium antibodies in coeliac disease: An improved method. Gut 1994, 35, 776–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadithi, M.; von Blomberg, B.M.; Crusius, J.B.; Bloemena, E.; Kostense, P.J.; Meijer, J.W.; Mulder, C.J.; Stehouwer, C.D.; Pena, A.S. Accuracy of serologic tests and HLA-DQ typing for diagnosing celiac disease. Ann. Intern. Med. 2007, 147, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Monsuur, A.J.; de Bakker, P.I.; Zhernakova, A.; Pinto, D.; Verduijn, W.; Romanos, J.; Auricchio, R.; Lopez, A.; van Heel, D.A.; Crusius, J.B.; et al. Effective detection of human leukocyte antigen risk alleles in celiac disease using tag single nucleotide polymorphisms. PLoS ONE 2008, 28, e2270. [Google Scholar]
- Koskinen, L.; Romanos, J.; Kaukinen, K.; Mustalahti, K.; Korponay-Szabo, I.; Barisani, D.; Bardella, M.T.; Ziberna, F.; Vatta, S.; Szeles, G.; et al. Cost-effective HLA typing with tagging SNPs predicts celiac disease risk haplotypes in the Finnish, Hungarian, and Italian populations. Immunogenetics 2009, 61, 247–256. [Google Scholar] [CrossRef]
- Sutton, C.L.; Kim, J.; Yamane, A.; Dalwadi, H.; Wei, B.; Landers, C.; Targan, S.R.; Braun, J. Identification of a novel bacterial sequence associated with Crohn’s disease. Gastroenterology 2000, 119, 23–31. [Google Scholar] [CrossRef]
- Wei, B.; Dalwadi, H.; Gordon, L.K.; Landers, C.; Bruckner, D.; Targan, S.R.; Braun, J. Molecular cloning of a bacteroides caccae TonB-linked outer membrane protein identified by an inflammatory bowel disease marker antibody. Infect. Immunol. 2001, 69, 6044–6054. [Google Scholar] [CrossRef] [Green Version]
- Da Silva Kotze, L.M.; Nisihara, R.M.; Nass, F.R.; Theiss, P.M.; Silva, I.G.; da Rosa Utiyama, S.R. Anti-Saccharomyces cerevisiae antibodies in first-degree relatives of celiac disease patients. J. Clin. Gastroenterol. 2010, 44, 308. [Google Scholar] [CrossRef]
- Setty, M.; Discepolo, V.; Abadie, V.; Kamhawi, S.; Mayassi, T.; Kent, A.; Ciszewski, C.; Maglio, M.; Kistner, E.; Bhagat, G.; et al. Distinct and synergistic contributions of epithelial stress and adaptive immunity to functions of intraepithelial killer cells and active celiac disease. Gastroenterology 2015, 149, 681–691. [Google Scholar] [CrossRef] [Green Version]
- Bosca-Watts, M.M.; Minguez, M.; Planelles, D.; Navarro, S.; Rodriguez, A.; Santiago, J.; Tosca, J.; Mora, F. HLA-DQ: Celiac disease vs inflammatory bowel disease. World J. Gastroenterol. 2018, 24, 96–103. [Google Scholar] [CrossRef]
- Amcoff, K.; Joossens, M.; Pierik, M.J.; Jonkers, D.; Bohr, J.; Joossens, S.; Romberg-Camps, M.; Nyhlin, N.; Wickbom, A.; Rutgeerts, P.J.; et al. Concordance in anti-OmpC and anti-I2 indicate the influence of genetic predisposition: Results of a European study of twins with crohn’s disease. J. Crohns. Colitis. 2016, 10, 695–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halfvarson, J.; Standaert-Vitse, A.; Jarnerot, G.; Sendid, B.; Jouault, T.; Bodin, L.; Duhamel, A.; Colombel, J.F.; Tysk, C.; Poulain, D. Anti-Saccharomyces cerevisiae antibodies in twins with inflammatory bowel disease. Gut 2005, 54, 1237–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andren Aronsson, C.; Lee, H.S.; Koletzko, S.; Uusitalo, U.; Yang, J.; Virtanen, S.M.; Liu, E.; Lernmark, A.; Norris, J.M.; Agardh, D.; et al. Effects of gluten intake on risk of celiac disease: A case-control study on a Swedish birth cohort. Clin. Gastroenterol. Hepatol. 2016, 14, 403–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andren Aronsson, C.; Lee, H.S.; Hard Af Segerstad, E.M.; Uusitalo, U.; Yang, J.; Koletzko, S.; Liu, E.; Kurppa, K.; Bingley, P.J.; Toppari, J.; et al. Association of gluten intake during the first 5 years of life with incidence of celiac disease autoimmunity and celiac disease among children at increased risk. JAMA 2019, 322, 514–523. [Google Scholar] [CrossRef]
- Kemppainen, K.M.; Lynch, K.F.; Liu, E.; Lönnrot, M.; Simell, V.; Briese, T.; Koletzko, S.; Hagopian, W.; Rewers, M.; She, J.X.; et al. Factors that increase risk of celiac disease autoimmunity after a gastrointestinal infection in early life. Clin. Gastroenterol. Hepatol. 2017, 15, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Kahrs, C.R.; Chuda, K.; Tapia, G.; Stene, L.C.; Marild, K.; Rasmussen, T.; Ronningen, K.S.; Lundin, K.E.A.; Kramna, L.; Cinek, O.; et al. Enterovirus as trigger of coeliac disease: Nested case-control study within prospective birth cohort. BMJ 2019, 364, 231. [Google Scholar] [CrossRef] [Green Version]
- Stene, L.C.; Honeyman, M.C.; Hoffenberg, E.J.; Haas, J.E.; Sokol, R.J.; Emery, L.; Taki, I.; Norris, J.M.; Erlich, H.A.; Eisenbarth, G.S.; et al. Rotavirus infection frequency and risk of celiac disease autoimmunity in early childhood: A longitudinal study. Am. J. Gastroenterol. 2006, 101, 2333–2340. [Google Scholar] [CrossRef]
- Marild, K.; Kahrs, C.R.; Tapia, G.; Stene, L.C.; Stordal, K. Infections and risk of celiac disease in childhood: A prospective nationwide cohort study. Am. J. Gastroenterol. 2015, 110, 1475–1484. [Google Scholar] [CrossRef]
- Kemppainen, K.M.; Vehik, K.; Lynch, K.F.; Larsson, H.E.; Canepa, R.J.; Simell, V.; Koletzko, S.; Liu, E.; Simell, O.G.; Toppari, J.; et al. Association between early-life antibiotic use and the risk of islet or celiac disease autoimmunity. JAMA Pediatr. 2017, 171, 1217–1225. [Google Scholar] [CrossRef]
- Sander, S.D.; Nybo Andersen, A.M.; Murray, J.A.; Karlstad, O.; Husby, S.; Stordal, K. Association between antibiotics in the first year of life and celiac disease. Gastroenterology 2019, 156, 2217–2229. [Google Scholar] [CrossRef] [Green Version]
- Riddle, M.S.; Murray, J.A.; Cash, B.D.; Pimentel, M.; Porter, C.K. Pathogen-specific risk of celiac disease following bacterial causes of foodborne illness: A retrospective cohort study. Dig. Dis. Sci. 2013, 58, 3242–3245. [Google Scholar] [CrossRef] [PubMed]
- Bach, J.F. The hygiene hypothesis in autoimmunity: The role of pathogens and commensals. Nat. Rev. Immunol. 2018, 18, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Verdu, E.F.; Galipeau, H.J.; Jabri, B. Novel players in coeliac disease pathogenesis: Role of the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Kupfer, S.S.; Jabri, B. Pathophysiology of celiac disease. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 639–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schumann, M.; Siegmund, B.; Schulzke, J.D.; Fromm, M. Celiac disease: Role of the epithelial barrier. Cell Mol. Gastroenterol. Hepatol. 2017, 3, 150–162. [Google Scholar] [CrossRef] [Green Version]
- Kalliomäki, M.; Satokari, R.; Lähteenoja, H.; Vahamiko, S.; Gronlund, J.; Routi, T.; Salminen, S. Expression of microbiota, Toll-like receptors, and their regulators in the small intestinal mucosa in celiac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 727–732. [Google Scholar] [CrossRef]
- Petersen, J.; Ciacchi, L.; Tran, M.T.; Loh, K.L.; Kooy-Winkelaar, Y.; Croft, N.P.; Hardy, M.Y.; Chen, Z.; McCluskey, J.; Anderson, R.P.; et al. T cell receptor cross-reactivity between gliadin and bacterial peptides in celiac disease. Nat. Struct. Mol. Biol. 2020, 27, 49–61. [Google Scholar] [CrossRef]
- Torres, J.; Petralia, F.; Sato, T.; Wang, P.; Telesco, S.E.; Choung, R.S.; Strauss, R.; Li, X.J.; Laird, R.M.; Gutierrez, R.L.; et al. Serum biomarkers identify patients who will develop inflammatory bowel diseases up to 5 y before diagnosis. Gastroenterology 2020, (in press). [Google Scholar] [CrossRef]
- Schaffer, T.; Muller, S.; Flogerzi, B.; Seibold-Schmid, B.; Schoepfer, A.M.; Seibold, F. Anti-Saccharomyces cerevisiae mannan antibodies (ASCA) of Crohn’s patients crossreact with mannan from other yeast strains, and murine ASCA IgM can be experimentally induced with Candida albicans. Inflamm. Bowel Dis. 2007, 13, 1339–1346. [Google Scholar] [CrossRef]
- Mallant-Hent, R.C.; Mooij, M.; von Blomberg, B.M.; Linskens, R.K.; van Bodegraven, A.A.; Savelkoul, P.H. Correlation between Saccharomyces cerevisiae DNA in intestinal mucosal samples and anti-Saccharomyces cerevisiae antibodies in serum of patients with IBD. World J. Gastroenterol. 2006, 12, 292–297. [Google Scholar] [CrossRef]
- Viitasalo, L.; Kurppa, K.; Ashorn, M.; Saavalainen, P.; Huhtala, H.; Ashorn, S.; Mäki, M.; Ilus, T.; Kaukinen, K.; Iltanen, S. Microbial Biomarkers in Patients with Nonresponsive Celiac Disease. Dig. Dis. Sci. 2018, 63, 3434–3441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pekki, H.; Kurppa, K.; Mäki, M.; Huhtala, H.; Sievänen, H.; Laurila, K.; Collin, P.; Kaukinen, K. Predictors and significance of incomplete mucosal recovery in celiac disease after 1 year on a gluten-free diet. Am. J. Gastroenterol. 2015, 110, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.; Fan, Y.; Lv, B.; Ji, C.; Xu, L. Diagnostic utility of serological biomarkers in patients with Crohn’s disease: A case-control study. Medicine 2018, 97, e11772. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Seropositive Relatives | Seronegative Relatives * | CD at Diagnosis | CD on GFD | Non-CD Controls | |
|---|---|---|---|---|---|
| n = 49 | n = 414 | n = 58 | n = 55 | n = 80 | |
| Females, % | 42.9 | 57.2 | 77.6 | 76.4 | 35.0 |
| Age, median (quartiles), y | 41 (31–54) | 42 (28–59) | 45 (36–59) | 46 (38-60) | 41 (31–56) |
| DQ2 n = 233 | DQ8 n = 67 | DQ2 + DQ8 n = 8 | DQ2/8 Negative n = 89 | |
|---|---|---|---|---|
| % | % | % | % | |
| ASCA IgA | 11.2 | 10.4 | 12.5 | 10.1 |
| ASCA IgG | 12.9 | 13.4 | 0 | 14.6 |
| Anti-I2 | 58.4 | 61.2 | 75.0 | 66.3 |
| Anti-OmpW | 39.5 | 35.8 | 25.0 | 43.8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viitasalo, L.; Iltanen, S.; Huhtala, H.; Saavalainen, P.; Kaukinen, K.; Lindfors, K.; Kurppa, K. First-degree Relatives of Celiac Disease Patients Have Increased Seroreactivity to Serum Microbial Markers. Nutrients 2020, 12, 1073. https://doi.org/10.3390/nu12041073
Viitasalo L, Iltanen S, Huhtala H, Saavalainen P, Kaukinen K, Lindfors K, Kurppa K. First-degree Relatives of Celiac Disease Patients Have Increased Seroreactivity to Serum Microbial Markers. Nutrients. 2020; 12(4):1073. https://doi.org/10.3390/nu12041073
Chicago/Turabian StyleViitasalo, Liisa, Sari Iltanen, Heini Huhtala, Päivi Saavalainen, Katri Kaukinen, Katri Lindfors, and Kalle Kurppa. 2020. "First-degree Relatives of Celiac Disease Patients Have Increased Seroreactivity to Serum Microbial Markers" Nutrients 12, no. 4: 1073. https://doi.org/10.3390/nu12041073
APA StyleViitasalo, L., Iltanen, S., Huhtala, H., Saavalainen, P., Kaukinen, K., Lindfors, K., & Kurppa, K. (2020). First-degree Relatives of Celiac Disease Patients Have Increased Seroreactivity to Serum Microbial Markers. Nutrients, 12(4), 1073. https://doi.org/10.3390/nu12041073