Targeted Breast Milk Fortification for Very Low Birth Weight (VLBW) Infants: Nutritional Intake, Growth Outcome and Body Composition

Abstract
:1. Introduction
2. Materials and Methods
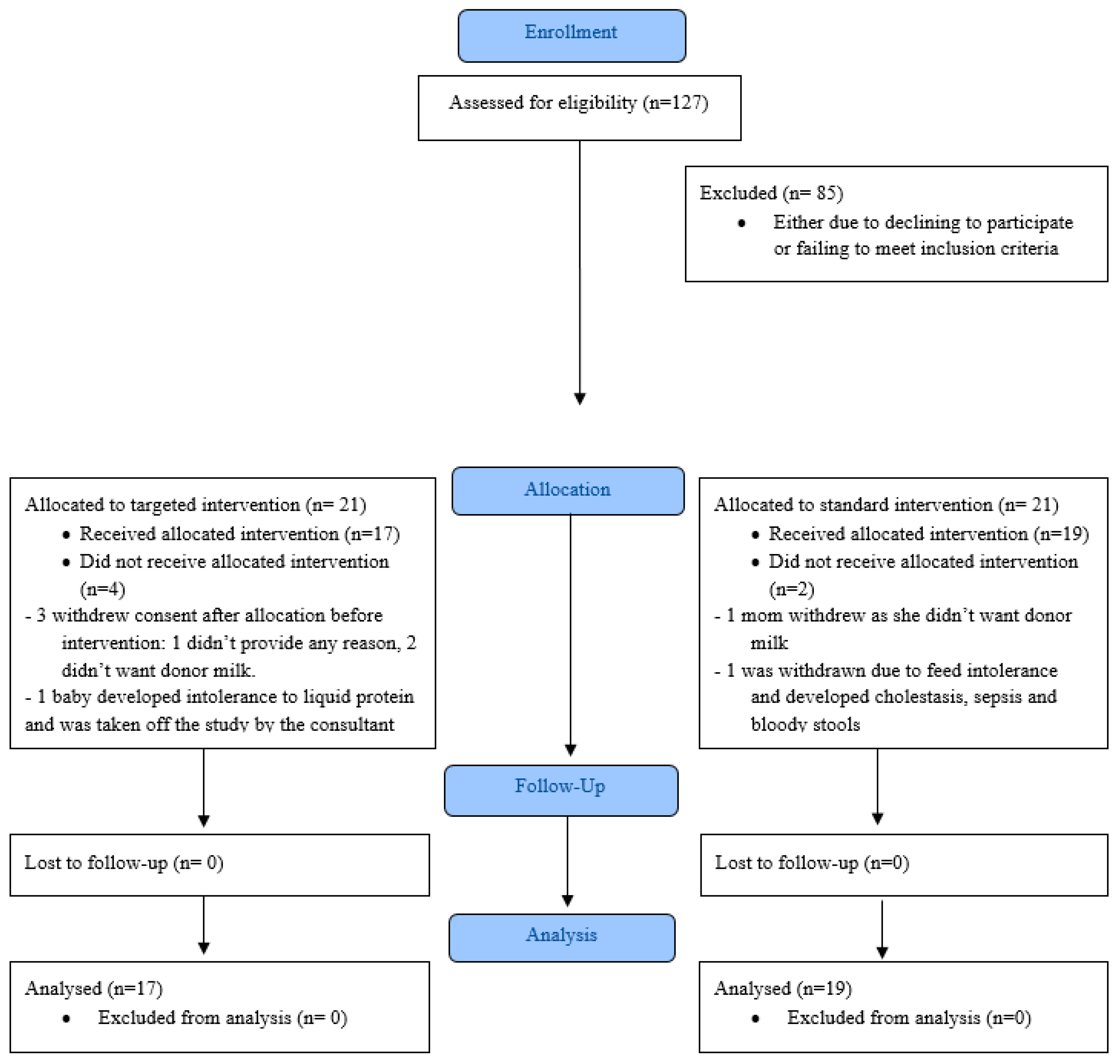
2.1. Study Design and Subjects
2.2. Human Milk Collection and Storage
2.3. Nutritional Practices
2.4. Milk Fortification
2.5. Body Composition Assessment
2.6. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Academy of Pediatrics. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreault, S.; Bellanger, A.; Berneau, P.; De La Pintière, A.; Lallemant, C.; Beuchée, A. Impact of early protein and energy intakes on neurodevelopment at 2 years of corrected age in very low birth weight infants: A single-center observational study. PLoS ONE 2019, 14, e0218887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arslanoglu, S.; Boquien, C.-Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- De Halleux, V.; Rigo, J. Variability in human milk composition: Benefit of individualized fortification in very-low-birth-weight infants. Am. J. Clin. Nutr. 2013, 98, 529s–535s. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, E.E. Meeting the nutritional needs of the low-birth-weight infant. Ann. Nutr. Metab. 2011, 58 (Suppl. 1), 8–18. [Google Scholar] [CrossRef]
- Wojcik, K.; Rechtman, D.; Lee, M.; Montoya, A.; Medo, E. Macronutrient analysis of a nationwide sample of donor breast milk. J. Am. Diet. Assoc. 2009, 109, 137–140. [Google Scholar] [CrossRef]
- Brown, J.V.; Embleton, N.D.; Harding, J.E.; McGuire, W. Multi-nutrient fortification of human milk for preterm infants. Cochrane Database Syst. Rev. 2016, 8, CD000343. [Google Scholar] [CrossRef] [Green Version]
- Picaud, J.C.; Houeto, N.; Buffin, R.; Loys, C.M.; Godbert, I.; Hays, S. Additional Protein Fortification Is Necessary in Extremely Low-Birth-Weight Infants Fed Human Milk. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 103–105. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; et al. Target fortification of breast milk with fat, protein, and carbohydrates for preterm infants. J. Pediatr. 2013, 163, 1001–1007. [Google Scholar] [CrossRef]
- Morlacchi, L.; Mallardi, D.; Gianni, M.L.; Roggero, P.; Amato, O.; Piemontese, P.; Consonni, D.; Mosca, F. Is targeted fortification of human breast milk an optimal nutrition strategy for preterm infants? An interventional study. J. Transl. Med. 2016, 14, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reali, A.; Greco, F.; Marongiu, G.; Deidda, F.; Atzeni, S.; Campus, R.; Dessi, A.; Fanos, V. Individualized fortification of breast milk in 41 Extremely Low Birth Weight (ELBW) preterm infants. Clin. Chim. Acta 2015, 451, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Polberger, S., III. Individualized Fortification of Human Milk: Targeted Fortification. J. Pediatr. Gastroenterol. Nutr. 2015, 61 (Suppl. 1), S3–S4. [Google Scholar] [CrossRef] [PubMed]
- McLeod, G.; Sherriff, J.; Hartmann, P.E.; Nathan, E.; Geddes, D.; Simmer, K. Comparing different methods of human breast milk fortification using measured v. assumed macronutrient composition to target reference growth: A randomised controlled trial. Br. J. Nutr. 2015, 115, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Preterm infants fed fortified human milk receive less protein than they need. J. Perinatol. 2009, 29, 489–492. [Google Scholar] [CrossRef] [Green Version]
- Corvaglia, L.; Aceti, A.; Paoletti, V.; Mariani, E.; Patrono, D.; Ancora, G.; Capretti, M.G.; Faldella, G. Standard fortification of preterm human milk fails to meet recommended protein intake: Bedside evaluation by Near-Infrared-Reflectance-Analysis. Early Hum. Dev. 2010, 86, 237–240. [Google Scholar] [CrossRef]
- Macedo, I.; Pereira-da-Silva, L.; Cardoso, M. The fortification method relying on assumed human milk composition overestimates the actual energy and macronutrient intakes in very preterm infants. Matern Health Neonatol. Perinatol. 2018, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Stephens, B.; Walden, R.; Gargus, R.; Tucker, R.; McKinley, L.; Mance, M.; Nye, J.; Vohr, B. First-Week Protein and Energy Intakes Are Associated with 18-Month Developmental Outcomes in Extremely Low Birth Weight Infants. Pediatrics 2009, 123, 1337–1343. [Google Scholar] [CrossRef]
- Cormack, B.E.; Bloomfield, F.H. Increased protein intake decreases postnatal growth faltering in ELBW babies. Arch. Dis. Child. 2013, 98, F399–F404. [Google Scholar] [CrossRef]
- Atchley, C.B.; Cloud, A.; Thompson, D.; Blunt, M.H.; Satnes, K.J.; Szyld, E.; Ernst, K.D. Enhanced Protein Diet for Preterm Infants: A Prospective, Randomized, Double-blind, Controlled Trial. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 218–223. [Google Scholar] [CrossRef]
- Larcade, J.; Pradat, P.; Buffin, R.; Leick-Courtois, C.; Jourdes, E.; Picaud, J.C. Estimation of fat-free mass at discharge in preterm infants fed with optimized feeding regimen. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Groh-Wargo, S.; Valentic, J.; Khaira, S.; Super, D.M.; Colin, M. Considering Human Milk Variability in the Nutritional Management of Low-Birth-Weight Infants. ICAN Infant Child Adolesc. Nutr. 2014, 6, 301–302. [Google Scholar] [CrossRef] [Green Version]
- Parat, S.; Groh-Wargo, S.; Merlino, S.; Wijers, C.; Super, D.M. Validation of mid-infrared spectroscopy for macronutrient analysis of human milk. J. Perinatol. 2017, 37, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Demerath, E.W.; Fields, D.A. Body composition assessment in the infant. Am. J. Hum. Biol. 2014, 26, 291–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, G.; Yao, M.; Liu, Y.; Lin, A.; Zou, H.; Urlando, A.; Wong, W.W.; Nommsen-Rivers, L.; Dewey, K.G. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 2004, 79, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Roggero, P.; Giannì, M.L.; Amato, O.; Piemontese, P.; Morniroli, D.; Wong, W.W.; Mosca, F. Evaluation of air-displacement plethysmography for body composition assessment in preterm infants. Pediatr. Res. 2012, 72, 316–320. [Google Scholar] [CrossRef] [Green Version]
- Mazahery, H.; Von Hurst, P.R.; McKinlay, C.D.; Cormack, B.E.; Conlon, C.A. Air displacement plethysmography (pea pod) in full-term and pre-term infants: A comprehensive review of accuracy, reproducibility, and practical challenges. Matern. Health Neonatol. Perinatol. 2018, 4, 12. [Google Scholar] [CrossRef]
- Walyat, N.; Groh-Wargo, S.; Collin, M.; Super, D.M.; Manning, J. Good news or bad news? Accumulation of fat in preterm infants approaching discharge from the NICU. In Proceedings of the Pediatric Academic Societies’ Meeting, Boston, MA, USA, May 2012. [Google Scholar]
- Tonkin, E.L.; Collins, C.T.; Miller, J. Protein Intake and Growth in Preterm Infants: A Systematic Review. Glob. Pediatr. Health 2014, 1, 2333794X14554698. [Google Scholar] [CrossRef] [Green Version]
- Piemontese, P.; Liotto, N.; Mallardi, D.; Roggero, P.; Puricelli, V.; Giannì, M.L.; Morniroli, D.; Tabasso, C.; Perrone, M.; Menis, C.; et al. The Effect of Human Milk on Modulating the Quality of Growth in Preterm Infants. Front. Pediatr. 2018, 6, 291. [Google Scholar] [CrossRef]
- Pencharz, P.; Ball, R. Amino acid needs for early growth and development. J. Nutr. 2004, 134, 1566S–1568S. [Google Scholar] [CrossRef] [Green Version]
- Lonnerdal, B. Infant formula and infant nutrition: Bioactive proteins of human milk and implications for composition of infant formulas. Am. J. Clin. Nutr. 2014, 99, 712S–717S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, M.; Wang, D.; Gou, L.; Sun, Z.; Ma, J.; Zhang, L.; Wang, C.; Schibler, K.; Li, Z. Individualized Human Milk Fortification to Improve the Growth of Hospitalized Preterm Infants. Nutr. Clin. Pract. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ramel, S.E.; Gray, H.L.; Christiansen, E.; Boys, C.; Georgieff, M.K.; Demerath, E.W. Greater Early Gains in Fat-Free Mass, but Not Fat Mass, Are Associated with Improved Neurodevelopment at 1 Year Corrected Age for Prematurity in Very Low Birth Weight Preterm Infants. J. Pediatr. 2016, 173, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Scheurer, J.M.; Zhang, L.; Plummer, E.A.; Hultgren, S.A.; Demerath, E.W.; Ramel, S.E. Body Composition Changes from Infancy to 4 Years and Associations with Early Childhood Cognition in Preterm and Full-Term Children. Neonatology 2018, 114, 169–176. [Google Scholar] [CrossRef]
- Frondas-Chauty, A.; Simon, L.; Flamant, C.; Hanf, M.; Darmaun, D.; Roze, J.C. Deficit of Fat Free Mass in Very Preterm Infants at Discharge is Associated with Neurological Impairment at Age 2 Years. J. Pediatr. 2018, 196, 301–304. [Google Scholar] [CrossRef]
- Josefson, J.L.; Nodzenski, M.; Talbot, O.; Scholtens, D.M.; Catalano, P. Fat mass estimation in neonates: Anthropometric models compared with air displacement plethysmography. Brit. J. Nutr. 2018, 121, 285–290. [Google Scholar] [CrossRef]
- Nagel, E.; Hickey, M.; Teigen, L.; Kuchnia, A.; Curran, K.; Soumekh, L.; Earthman, C.; Demerath, E.; Ramel, S. Clinical Application of Body Composition Methods in Premature Infants. J. Parenter. Enteral Nutr. 2020. [Google Scholar] [CrossRef]
- Giuliani, F.; Prandi, G.; Coscia, A.; Cresi, F.; Di Nicola, P.; Raia, M.; Sabatino, G.; Occhi, L.; Bertino, E. Donor human milk versus mother’s own milk in preterm VLBWIs: A case control study. J. Biol. Regul. Homeost Agents 2012, 26 (Suppl. 3), 19–24. [Google Scholar]


{kind=link}
| Standard Group (n = 19) | Targeted Group (n = 17) | p-value * | |
|---|---|---|---|
| Female, n (%) | 8/19 (42.3%) | 7/17 (41.2%) | 0.955 |
| African American, n (%) | 10/19 (52.6%) | 9/17 (52.9%) | 0.179 |
| Multiple births, n (%) | 4/19 (21.1%) | 4/17 (23.5%) | 1.000 |
| Small for Gestational age, n (%) | 6/19 (31.6%) | 6/17 (35.3%) | 0.965 |
| Gestational age at birth (weeks) | 28.6 ± 3.6 | 28.7 ± 2.9 | 0.874 |
| Birth Weight (grams) | 1016 ±326 | 1069 ± 346 | 0.641 |
| Birth Length (cm) | 36.1 ± 4.1 | 36.0 ± 4.8 | 0.958 |
| Birth Head Circumference (cm) | 25.6 ± 3.5 | 25.3 ± 3.0 | 0.759 |
| Day of life at intervention | 35.4 ± 23.4 | 32.7 ± 19.2 | 0.713 |
| Gestational age at intervention (weeks) | 33.7 ± 2.1 | 33.4 ± 2.2 | 0.675 |
| Weight at intervention (grams) | 1447 ±275 | 1551 ± 272 | 0.263 |
| Length at intervention (cm) | 39.6 ± 3.1 | 40.3 ± 2.8 | 0.436 |
| Head circumference at intervention (cm) | 27.5 ± 2.2 | 28.5 ± 2.0 | 0.176 |
| Standard Group (n = 19) | Targeted Group (n = 17) | p-Value | |
|---|---|---|---|
| Postmenstrual age (weeks) at body composition assessment | 37.5 ± 1.74 | 37.9 ± 2.21 | 0.633 |
| Days of Intervention | 26.5 ± 12.4 | 31.4 ± 16.7 | 0.324 |
| Protein intake (gram/kg/day) | 3.09 ± 0.33 | 4.07 ± 0.27 | <0.001 ** |
| Calorie intake (kcal/kg/day) | 116.7 ± 8.3 | 107.4 ± 9.2 | 0.003 ** |
| Weight (grams) | 2217 ±422 | 2368 ± 379 | 0.268 |
| Length (cm) | 43.6 ± 2.0 | 45.0 ± 2.2 | 0.065 * |
| Head circumference (cm) | 31.8 ± 1.3 | 31.9 ± 1.5 | 0.805 |
| Mid arm circumference (cm) | 8.34 ± 0.72 | 8.61 ± 0.90 | 0.315 |
| Triceps skin fold thickness (mm) | 4.1 ± 0.9 | 4.0 ± 0.9 | 0.980 |
| Subscapular skin fold thickness (mm) | 4.1 ± 1.0 | 4.1 ± 1.3 | 0.922 |
| Flank skin fold thickness (mm) | 3.3 ± 1.2 | 4.4 ± 1.5 | 0.022 ** |
| Fat free mass (%) | 82.8 ± 4.8 | 83.6 ± 3.2 | 0.557 |
| Fat mass (grams) | 381 ± 142 | 397 ± 130 | 0.730 |
| Fat free mass (grams) | 1784 ± 230 | 1940 ± 264 | 0.066 * |
| Standard Group (n = 8) | Targeted Group (n = 8) | p-Value | |
|---|---|---|---|
| Triceps skin fold thickness (mm) | 4.68 ± 0.74 | 4.41 ± 0.97 | 0.528 |
| Subscapular skin fold thickness (mm) | 4.62 ± 0.92 | 4.55 ± 1.56 | 0.875 |
| Flank skin fold thickness (mm) | 3.53 ± 1.54 | 5.00 ± 1.46 | 0.036 ** |
| Fat Mass (%) | 22.0 ± 3.1 | 18.2 ± 2.9 | 0.046 ** |
| Fat Free Mass (%) | 78.1 ± 3.0 | 81.8 ± 2.9 | 0.046 ** |
| Fat Mass (grams) | 520 ± 87 | 473 ± 138 | 0.600 |
| Fat Free Mass (grams) | 1856 ± 232 | 2067 ± 316 | 0.093 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parat, S.; Raza, P.; Kamleh, M.; Super, D.; Groh-Wargo, S. Targeted Breast Milk Fortification for Very Low Birth Weight (VLBW) Infants: Nutritional Intake, Growth Outcome and Body Composition. Nutrients 2020, 12, 1156. https://doi.org/10.3390/nu12041156
Parat S, Raza P, Kamleh M, Super D, Groh-Wargo S. Targeted Breast Milk Fortification for Very Low Birth Weight (VLBW) Infants: Nutritional Intake, Growth Outcome and Body Composition. Nutrients. 2020; 12(4):1156. https://doi.org/10.3390/nu12041156
Chicago/Turabian StyleParat, Sumesh, Praneeta Raza, May Kamleh, Dennis Super, and Sharon Groh-Wargo. 2020. "Targeted Breast Milk Fortification for Very Low Birth Weight (VLBW) Infants: Nutritional Intake, Growth Outcome and Body Composition" Nutrients 12, no. 4: 1156. https://doi.org/10.3390/nu12041156
APA StyleParat, S., Raza, P., Kamleh, M., Super, D., & Groh-Wargo, S. (2020). Targeted Breast Milk Fortification for Very Low Birth Weight (VLBW) Infants: Nutritional Intake, Growth Outcome and Body Composition. Nutrients, 12(4), 1156. https://doi.org/10.3390/nu12041156