Clustering of Sedentary Behaviours, Physical Activity, and Energy-Dense Food Intake in Six-Year-Old Children: Associations with Family Socioeconomic Status



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Socioeconomic Status
2.3. Lifestyle Behaviours
2.3.1. Screen Time
2.3.2. Physical Activity
2.3.3. Calorie-Rich Snack
2.3.4. Sugar-Sweetened Beverages
2.4. Potential Confounders
2.5. Statistical Analyses
2.6. Non-Response Analyses
3. Results
3.1. Description of the Clusters
3.2. Cluster Distribution according to Child Characteristics and Socioeconomic Status
3.3. Associations of SES Indicators with the Cluster Distribution
4. Discussion
Methodological Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Adolescent Obesity and Relatedbehaviours: Trends and Inequalities in the WHO European Region, 2002–2014; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Pérez-Rodrigo, C.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2015, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netherlands Bureau for Economic Policy Analysis. Available online: http://www.cpb.nl (accessed on 9 May 2017).
- Santaliestra-Pasías, A.M.; Mouratidou, T.; Reisch, L.; Pigeot, I.; Ahrens, W.; Mårild, S.; Molnár, D.; Siani, A.; Sieri, S.; Tornatiris, M.; et al. Clustering of lifestyle behaviours and relation to body composition in European children. The IDEFICS study. Eur. J. Clin. Nutr. 2015, 69, 811–816. [Google Scholar]
- Gubbels, J.; Kremers, S.P.J.; Stafleu, A.; Goldbohm, R.A.; de Vries, N.K.; Thijs, C. Clustering of energy balance-related behaviors in 5-year-old children: Lifestyle patterns and their longitudinal association with weight status development in early childhood. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 77. [Google Scholar] [CrossRef] [Green Version]
- Seghers, J.; Rutten, C. Clustering of multiple lifestyle behaviours and its relationship with weight status and cardiorespiratory fitness in a sample of Flemish 11- to 12-year-olds. Public Health Nutr. 2010, 13, 1838–1846. [Google Scholar] [CrossRef] [Green Version]
- Bel-Serrat, S.; Ojeda-Rodríguez, A.; Heinen, M.; Buoncristiano, M.; Abdrakhmanova, S.; Duleva, V.; Sant’Angelo, V.F.; Fijalkowska, A.; Hejgaard, T.; Huidumac, C.; et al. Clustering of Multiple Energy Balance-Related Behaviors in School Children and its Association with Overweight and Obesity-WHO European Childhood Obesity Surveillance Initiative (COSI 2015–2017). Nutrients 2019, 11, 511. [Google Scholar] [CrossRef] [Green Version]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. Clustering of children’s obesity-related behaviours: Associations with sociodemographic indicators. Eur. J. Clin. Nutr. 2014, 68, 623–628. [Google Scholar] [CrossRef]
- Matias, T.S.; Silva, K.S.; da Silva, J.A.; de Mello, G.T.; Salmon, J. Clustering of diet, physical activity and sedentary behavior among Brazilian adolescents in the national school-Based health survey (PeNSE 2015). BMC Public Health 2018, 18, 1283. [Google Scholar] [CrossRef]
- Huh, J.; Riggs, N.R.; Spruijt-Metz, N.; Chou, C.-P.; Huang, Z.; Pentz, M. Identifying patterns of eating and physical activity in children: A latent class analysis of obesity risk. Obesity 2010, 19, 652–658. [Google Scholar] [CrossRef] [Green Version]
- Ottevaere, C.; Huybrechts, I.; Benser, J.; De Bourdeaudhuij, I.; Cuenca-García, M.; Dallongeville, J.; Zaccaria, M.; Gottrand, F.; Kersting, M.; Rey-López, J.; et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Health 2011, 11, 328. [Google Scholar] [CrossRef]
- Miguel-Berges, M.L.; Zachari, K.; Santaliestra-Pasias, A.M.; Mouratidou, T.; Androutsos, O.; Iotova, V.; Galcheva, S.; De Craemer, M.; Cardon, G.; Koletzko, B.; et al. Clustering of energy balance-related behaviours and parental education in European preschool children: The ToyBox study. Br. J. Nutr. 2017, 118, 1089–1096. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.; Kremers, S.P.; Stafleu, A.; Dagnelie, P.C.; De Vries, S.I.; De Vries, N.; Thijs, C. Clustering of Dietary Intake and Sedentary Behavior in 2-Year-Old Children. J. Pediatr. 2009, 155, 194–198. [Google Scholar] [CrossRef]
- Craigie, A.M.; Lake, A.; Kelly, S.; Adamson, A.J.; Mathers, J. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [Green Version]
- Northstone, K.; Emmett, P. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Kim, J.; Colabianchi, N.; Ortaglia, A.; Pate, R.R. Co-varying Patterns of Physical Activity and Sedentary Behaviors and Their Long-Term Maintenance Among Adolescents. J. Phys. Act. Health 2010, 7, 465–474. [Google Scholar] [CrossRef]
- Mistry, R.; McCarthy, W.J.; Yancey, A.K.; Lu, Y.; Patel, M. Resilience and patterns of health risk behaviors in California adolescents. Prev. Med. 2008, 48, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Galobardes, B.; Shaw, M.; Lawlor, D.; Lynch, J.W. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Jaddoe, V.W.; Van Duijn, C.M.; Franco, O.H.; Van Der Heijden, A.J.; Van Iizendoorn, M.H.; De Jongste, J.C.; Van Der Lugt, A.; MacKenbach, J.P.; Moll, H.A.; Raat, H.; et al. The Generation R Study: Design and cohort update 2012. Eur. J. Epidemiol. 2012, 27, 739–756. [Google Scholar] [CrossRef] [Green Version]
- Statistics Netherlands. Standaard Onderwijsindeling 2003; Statistics Netherlands: Voorburg/Heerlen, The Netherlands, 2004.
- Fernández-Alvira, J.M.; De Bourdeaudhuij, I.; Singh, A.S.; Vik, F.N.; Manios, Y.; Kovács, É.; Jan, N.; Brug, J.; Moreno, L.A. Clustering of energy balance-related behaviors and parental education in European children: The ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 5. [Google Scholar]
- Statistics Netherlands. Annual Report on Integration 2012 Summary. Available online: https://www.cbs.nl/en-gb/publication/2012/51/annual-report-on-integration-2012-summary (accessed on 8 June 2020).
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [Green Version]
- Everitt, B.S.; Leese, M. Cluster Analysis, 4th ed.; Oxford University Press, Inc.: New York, NY, USA, 2001. [Google Scholar]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 37. [Google Scholar]
- Physical Activity and Young People. Recommended Levels of Physical Activity for Children Aged 5–17 Years. Available online: https://www.who.int/dietphysicalactivity/factsheet_young_people/en/ (accessed on 8 June 2020).
- Department of Health. Australia’s Physical Activity and Sedentary Behaviour Guidelines; Department of Health: Canberra, Australia, 2014.
- Bel-Serrat, S.; Mouratidou, T.; Santaliestra-Pasías, A.M.; Iacoviello, L.; A Kourides, Y.; Mårild, S.; Molnár, D.; Reisch, L.; Siani, A.; Stomfai, S.; et al. Clustering of multiple lifestyle behaviours and its association to cardiovascular risk factors in children: The IDEFICS study. Eur. J. Clin. Nutr. 2013, 67, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Farooq, M.A.; Parkinson, K.N.; Adamson, A.; Pearce, M.; Reilly, J.K.; Hughes, A.R.; Janssen, X.; Basterfield, L.; Reilly, J.J. Timing of the decline in physical activity in childhood and adolescence: Gateshead Millennium Cohort Study. Br. J. Sports Med. 2017, 52, 1002–1006. [Google Scholar] [CrossRef] [Green Version]
- Rey-López, J.; Vicente-Rodriguez, G.; Ortega, F.B.; Ruiz, J.R.; Martínez-Gómez, D.; De Henauw, S.; Manios, Y.; Molnár, D.; Polito, A.; Verloigne, M.; et al. Sedentary patterns and media availability in European adolescents: The HELENA study. Prev. Med. 2010, 51, 50–55. [Google Scholar] [CrossRef]
- Westerterp, K.R. Physical activity, food intake, and body weight regulation: Insights from doubly labeled water studies. Nutr. Rev. 2010, 68, 148–154. [Google Scholar] [CrossRef]
- Hao, G.; Pollock, N.K.; Harris, R.A.; Gutin, B.; Su, S.; Wang, X. Associations between muscle mass, physical activity and dietary behaviour in adolescents. Pediatr. Obes. 2018, 14, e12471. [Google Scholar] [CrossRef]
- Yang-Huang, J.; Van Grieken, A.; Moll, H.A.; Jaddoe, V.W.; Wijtzes, A.I.; Raat, H. Socioeconomic differences in children’s television viewing trajectory: A population-based prospective cohort study. PLoS ONE 2017, 12, e0188363. [Google Scholar] [CrossRef]
- Wijtzes, A.I.; Jansen, W.; Bouthoorn, S.H.; Pot, N.; Hofman, A.; Jaddoe, V.W.; Raat, H. Social inequalities in young children’s sports participation and outdoor play. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 155. [Google Scholar] [CrossRef] [Green Version]
- Trigwell, J.; Murphy, R.C.; Cable, N.T.; Stratton, G.; Watson, P.M. Parental views of children’s physical activity: A qualitative study with parents from multi-ethnic backgrounds living in England. BMC Public Health 2015, 15, 1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Rodrigo, C.; Gianzo, M.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Lifestyle Patterns and Weight Status in Spanish Adults: The ANIBES Study. Nutrients 2017, 9, 606. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Finding | Missing | |
|---|---|---|---|
| n (%) | n (%) | ||
| Social characteristics | |||
| Maternal educational level | Low | 420 (10.4) | 25 (0.6) |
| Mid-low | 1215 (30.1) | ||
| Mid-high | 1162 (28.8) | ||
| High | 1237 (30.7) | ||
| Net household income | Low | 727 (18.9) | 211 (5.2) |
| Middle | 1036 (26.9) | ||
| High | 2085 (54.2) | ||
| Maternal age at child birth, years, mean (SD) | 31.1 (4.8) | 0 | |
| Children’s characteristics | |||
| Sex | Boy | 2057 (50.7) | 0 |
| Girl | 2002 (49.3) | ||
| Age, years (SD) | 6.0 (0.4) | 0 | |
| Ethnic background | Western | 3040 (74.9) | 2 (0.05) |
| Non-western | 1017 (25.1) | ||
| Weight status | Overweight/obesity | 536 (14.5) | 373 (9.2) |
| Normal weight | 3150 (85.5) |
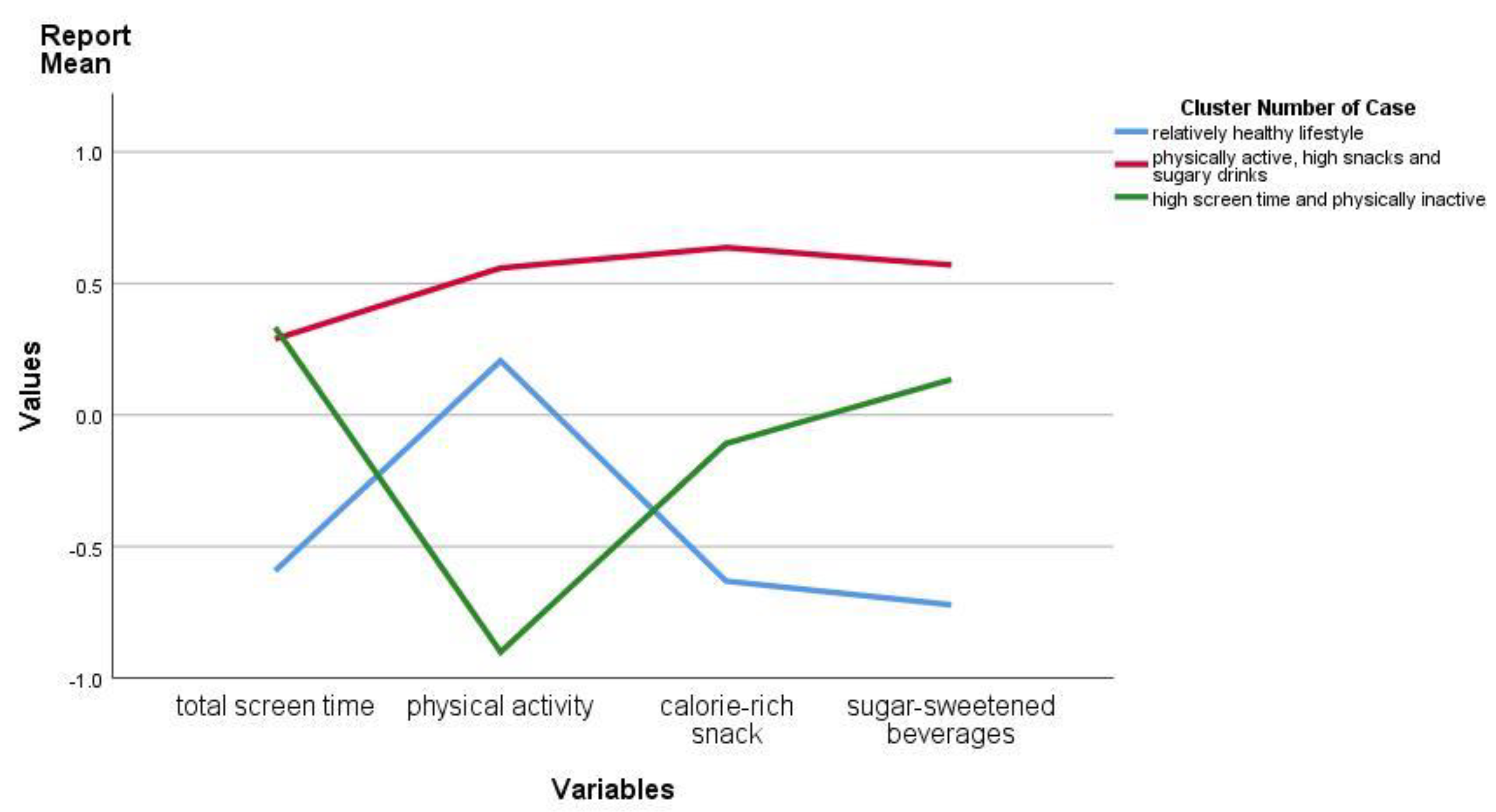
| Cluster 1 “Relatively Healthy Lifestyle” | Cluster 2 “High Screen Time and Physically Inactive” | Cluster 3 “Physically Active, High Snacks and Sugary Drinks” | |
|---|---|---|---|
| n = 1444 (35.6%) | n = 1217 (30.0%) | n = 1398 (34.4%) | |
| Screen time, mean (SD) | 0.99 (0.64) | 1.96 (1.10) | 1.91 (1.04) |
| z-score (SE) | −0.59 (0.61) | 0.33 (1.05) | 0.29 (0.99) |
| Physical activity, mean (SD) | 1.87 (0.96) | 0.67 (0.37) | 2.26 (1.05) |
| z-score (SE) | 0.21 (0.88) | −0.90 (0.34) | 0.56 (0.96) |
| Calorie-rich snacks, mean (SD) | 0.76 (0.60) | 1.25 (0.79) | 1.95 (0.72) |
| z-score (SE) | −0.63 (0.64) | −0.11 (0.84) | 0.64 (0.77) |
| Sugary drinks, mean (SD) | 1.33 (0.96) | 2.48 (1.13) | 3.06 (1.16) |
| z-score (SE) | −0.72 (0.71) | 0.13 (0.84) | 0.57 (0.86) |
| Cluster 1 “Relatively Healthy Lifestyle” | Cluster 2 “High Screen Time and Physically Inactive” | Cluster 3 “Physically Active, High Snacks and Sugary Drinks” | p-Value * | ||
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Sex | Boy | 676 (46.8) | 624 (51.3) | 757 (54.1) | <0.001 |
| Girl | 768 (53.2) | 593 (48.7) | 641 (45.9) | ||
| Weight status | Overweight/obesity | 181 (14.0) | 178 (15.9) | 177 (13.9) | <0.001 |
| Normal weight | 1114 (86.0) | 938 (84.1) | 1098 (86.1) | ||
| Maternal educational level | Low | 73 (5.1) | 165 (13.7) | 182 (13.7) | <0.001 |
| Mid-low | 329 (22.9) | 420 (34.9) | 466 (33.5) | ||
| Mid-high | 459 (31.9) | 321 (26.6) | 382 (27.4) | ||
| High | 576 (40.1) | 299 (24.8) | 362 (26.0) | ||
| Net household income | Low | 178 (13.1) | 314 (27.0) | 235 (17.7) | <0.001 |
| Middle | 327 (24.0) | 323 (27.8) | 386 (29.2) | ||
| High | 857 (62.9) | 525 (45.2) | 703 (53.1) |
| Cluster 1 “Relatively Healthy Lifestyle” | Cluster 2 “High Screen Time and Physically Inactive” | Cluster 3 “Physically Active, High Snacks and Sugary Drinks” | ||
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Maternal educational level | Low | 0.28 (0.21, 0.37) | 1.45 (1.13, 1.86) | 2.28 (1.79, 2.90) |
| Mid-low | 0.46 (0.39, 0.55) | 1.37 (1.14, 1.64) | 1.69 (1.42, 2.01) | |
| Mid-high | 0.77 (0.66, 0.91) | 1.11 (0.92, 1.34) | 1.23 (1.04, 1.47) | |
| High | Ref | Ref | Ref | |
| Net household income | Low | 0.59 (0.48, 0.74) | 1.57 (1.27, 1.94) | 1.07 (0.87, 1.31) |
| Middle | 0.72 (0.61, 0.84) | 1.18 (0.99, 1.40) | 1.22 (1.05, 1.43) | |
| High | Ref | Ref | Ref |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang-Huang, J.; van Grieken, A.; Wang, L.; Jansen, W.; Raat, H. Clustering of Sedentary Behaviours, Physical Activity, and Energy-Dense Food Intake in Six-Year-Old Children: Associations with Family Socioeconomic Status. Nutrients 2020, 12, 1722. https://doi.org/10.3390/nu12061722
Yang-Huang J, van Grieken A, Wang L, Jansen W, Raat H. Clustering of Sedentary Behaviours, Physical Activity, and Energy-Dense Food Intake in Six-Year-Old Children: Associations with Family Socioeconomic Status. Nutrients. 2020; 12(6):1722. https://doi.org/10.3390/nu12061722
Chicago/Turabian StyleYang-Huang, Junwen, Amy van Grieken, Lu Wang, Wilma Jansen, and Hein Raat. 2020. "Clustering of Sedentary Behaviours, Physical Activity, and Energy-Dense Food Intake in Six-Year-Old Children: Associations with Family Socioeconomic Status" Nutrients 12, no. 6: 1722. https://doi.org/10.3390/nu12061722
APA StyleYang-Huang, J., van Grieken, A., Wang, L., Jansen, W., & Raat, H. (2020). Clustering of Sedentary Behaviours, Physical Activity, and Energy-Dense Food Intake in Six-Year-Old Children: Associations with Family Socioeconomic Status. Nutrients, 12(6), 1722. https://doi.org/10.3390/nu12061722