Zonulin-Dependent Intestinal Permeability in Children Diagnosed with Mental Disorders: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Management
2.4. Selection and Data Collection Process
2.5. Quality Assessment and Risk of Bias Tool
2.6. Meta-Analysis
3. Results
3.1. Identification and Description of the Studies
3.2. Description of Excluded Studies
3.3. Summary of Main Results and Description of the Studies
- ADHD:
- ∘
- “Increased zonulin is associated with hyperactivity and social dysfunctions in children with attention deficit hyperactivity disorder” [5].
- ASD:
- ∘
- “Increased serum zonulin levels as an intestinal permeability marker in autistic subjects” [6].
- ∘
- “The occurrence of antibodies against gluten in children with autism spectrum disorders does not correlate with serological markers of impaired intestinal permeability” [7].
- ∘
- “Differential immune responses and microbiota profiles in children with autism spectrum disorders and co-morbid gastro-intestinal symptoms” [8].
- OCD:
- ∘
- “Serum zonulin and claudin-5 levels in children with obsessive–compulsive disorder” [9].
3.4. Study Quality
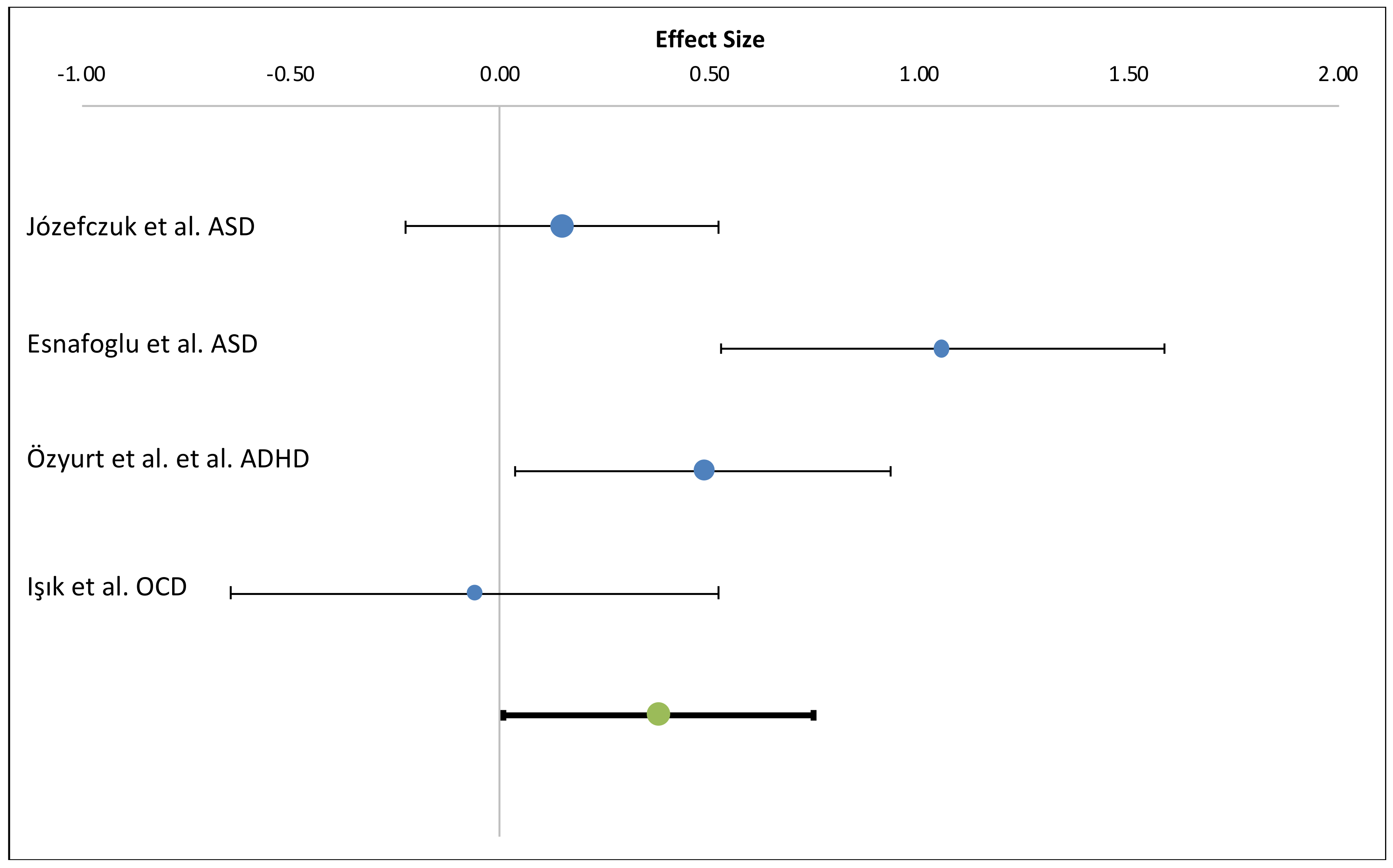
3.5. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AD | Anxiety Disorders |
| ADD | Attention Deficit Disorder |
| ADHD | Attention Deficit and Hyperactivity Disorder |
| BD | Bipolar Disorder |
| CNS | Central Nervous System |
| CARS | Childhood Autism Rating Scale |
| CD | Coeliac Disease |
| CRP | C-Reactive Protein |
| DAO | Diamine Oxidase |
| GI | Gastro-Intestinal |
| GALT | Gut-Associated Lymphoid Tissue |
| GBA | Gut-Brain Axis |
| HPA | Hypothalamic Pituitary Adrenal Axis |
| IL-6 | Interleukin 6 |
| IP | Intestinal Permeability |
| LPS | Lipopolysaccharide |
| LBP | Lipopolysaccharide Binding Protein |
| MDD | Major Depressive Disorder |
| NOS | Newcastle-Ottawa Scale |
| NCGS | Non-Coeliac Gluten Sensitivity |
| OCD | Obsessive–Compulsive Disorder |
| PANS | Pediatric Acute-onset Neuropsychiatric Syndrome |
| PANDAS | Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| PICO | Participants, Interventions, Comparisons, Outcomes |
| SCZ | Schizophrenia |
| sIgA | Secretory IgA |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| TG6 | Transglutaminase 6 |
| TG2 | Type 2 Tissue Transglutaminase |
| ZTM | Zonulin Transgenic Mouse Model |
Appendix A

{kind=link}
{kind=link}
| Checklist Item | Reported on Page | ||
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 3/4 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | 1 |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 4 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 3/4 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 4 |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 4/5 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 4/5 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 4/5 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 5 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | N/A |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 8/9 |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | 11 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | N/A |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 6/7 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 7/8 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 10/11 |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | 11 |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | 11 |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | 11 |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | N/A |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 12/15 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias) and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 12/15 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence and implications for future research. | 15 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 15 |
Appendix B. Detailed Search String (PubMed)
Appendix C
| Data Extraction Form |
|---|
| Reviewer ID: |
| Date of data extraction: |
| 1 General information |
|
|
|
|
|
| 2 Study characteristics |
|
|
|
|
|
|
| 3 Quality assessment of the study |
|
|
|
| 4 Participant Characteristics |
|
|
|
|
|
| 5 Exposures/comparison |
| 5.1 Exposures (biomarkers, intrinsic, exotoxins etc.) |
| 5.2 Comparison (describe) |
|
|
| 5.3 Number and type of clinical settings (in which the exposure/comarison is performed/tested): |
| 6 Outcome Data/results |
| 6.1 Main outcomes and effects addressed in the study |
|
| 6.2 Outcomes for which data were reported: |
|
| 6.3 Total number of participants included in the study: |
| 7 Statistical techniques used in the study: |
| 8 Number of participants included in analysis in the study - |
| 9 Summary outcome data |
|
|
|
|
|
|
|
|
|
| 10 Other comments - |
Appendix D. The Nos Criteria
- (1)
- Is the case definition adequate?
- (a)
- yes, with independent validation Ø
- (b)
- yes, eg record linkage or based on self reports
- (c)
- no description
- (2)
- Representativeness of the cases
- (a)
- consecutive or obviously representative series of cases Ø
- (b)
- potential for selection biases or not stated
- (3)
- Selection of Controls
- (a)
- community controls Ø
- (b)
- hospital controls
- (c)
- no description
- (4)
- Definition of Controls
- (a)
- no history of disease (endpoint) Ø
- (b)
- no description of source
- (1)
- Comparability of cases and controls on the basis of the design or analysis
- (a)
- study controls for _______________ (Select the most important factor.) Ø
- (b)
- study controls for any additional factor Ø (This criteria could be modified to indicate specific control for a second important factor.)
- (1)
- Ascertainment of exposure
- (a)
- secure record (eg surgical records) Ø
- (b)
- structured interview where blind to case/control status Ø
- (c)
- interview not blinded to case/control status
- (d)
- written self report or medical record only
- (e)
- no description
- (2)
- Same method of ascertainment for cases and controls
- (a)
- yes Ø
- (b)
- no
- (3)
- Non-Response rate
- (a)
- same rate for both groups Ø
- (b)
- non respondents described
- (c)
- rate different and no designation
References
- Hansen, B.H.; Oerbeck, B.; Skirbekk, B.; Petrovski, B.É.; Kristensen, H. Neurodevelopmental disorders: Prevalence and comorbidity in children referred to mental health services. Nord. J. Psychiatry 2018, 72, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Szatmari, P.; Gaebel, W.; Berk, M.; Vieta, E.; Maj, M.; Anna De Vries, Y.; Roest, A.M.; De Jonge, P.; Maercker, A.; et al. Mental, behavioral and neurodevelopmental disorders in the ICD-11: An international perspective on key changes and controversies. BMC Med. 2020, 18, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thapar, A.; Cooper, M.; Eyre, O.; Langley, K. What have we learnt about the causes of ADHD? J. Child Psychol. Psychiatry 2013, 54, 3–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesch, K.-P. Editorial: Illuminating the dark matter of developmental neuropsychiatric genetics - strategic focus for future research in child psychology and psychiatry. J. Child Psychol. Psychiatry 2014, 55, 201–203. [Google Scholar] [CrossRef]
- Özyurt, G.; Öztürk, Y.; Appak, Y.Ç.; Arslan, F.D.; Baran, M.; Karakoyun, İ.; Tufan, A.E.; Pekcanlar, A.A. Increased zonulin is associated with hyperactivity and social dysfunctions in children with attention deficit hyperactivity disorder. Compr. Psychiatry 2018, 87, 138–142. [Google Scholar] [CrossRef]
- Esnafoglu, E.; Cırrık, S.; Ayyıldız, S.N.; Erdil, A.; Ertürk, E.Y.; Daglı, A.; Noyan, T. Increased serum zonulin levels as an intestinal permeability marker in autistic subjects. J. Pediatr. 2017, 188, 240–244. [Google Scholar] [CrossRef]
- Józefczuk, J.; Konopka, E.; Bierła, J.B.; Trojanowska, I.; Sowińska, A.; Czarnecki, R.; Sobol, L.; Józefczuk, P.; Surdy, W.; Cukrowska, B. The occurrence of antibodies against gluten in children with autism spectrum disorders does not correlate with serological markers of impaired intestinal permeability. J. Med. Food 2018, 21, 181–187. [Google Scholar] [CrossRef]
- Rose, D.R.; Yang, H.; Serena, G.; Sturgeon, C.; Ma, B.; Careaga, M.; Hughes, H.K.; Angkustsiri, K.; Rose, M.; Hertz-Picciotto, I.; et al. Differential immune responses and microbiota profiles in children with autism spectrum disorders and co-morbid gastrointestinal symptoms. Brain Behav. Immun. 2018, 70, 354–368. [Google Scholar] [CrossRef]
- Işık, Ü.; Avşar, A.; Aktepe, E.; Doğuç, K.; Kılıç, F.; Büyükbayram, H.İ. Serum zonulin and claudin-5 levels in children with obsessive-compulsive disorder. Nord. J. Psychiatry 2020, 74, 346–351. [Google Scholar] [CrossRef]
- Greene, C.; Kealy, J.; Humphries, M.M.; Gong, Y.; Hou, J.; Hudson, N.; Cassidy, L.M.; Martiniano, R.; Shashi, V.; Hooper, S.R.; et al. Dose-dependent expression of claudin-5 is a modifying factor in schizophrenia. Mol. Psychiatry 2018, 23, 2156–2166. [Google Scholar] [CrossRef]
- Fiorentino, M.; Sapone, A.; Senger, S.; Camhi, S.S.; Kadzielski, S.M.; Buie, T.M.; Kelly, D.L.; Cascella, N.; Fasano, A. Blood–brain barrier and intestinal epithelial barrier alterations in autism spectrum disorders. Mol. Autism 2016, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, G.S.; Sturgeon, C.; Fasano, A.; Cascella, N.G.; Eaton, W.W.; McMahon, R.P.; Kelly, D.L. Elevated zonulin, a measure of tight-junction permeability, may be implicated in schizophrenia. Schizophr. Res. 2019, 211, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, L.; Gustafsson, A.; Lavant, E.; Suneson, K.; Brundin, L.; Westrin, Å.; Ljunggren, L.; Lindqvist, D. Leaky gut biomarkers in depression and suicidal behavior. Acta Psychiatr. Scand. 2019, 139, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Mental Health NIMH » Treatment of Children with Mental Illness. Available online: https://www.nimh.nih.gov/health/publications/treatment-of-children-with-mental-illness-fact-sheet/index.shtml (accessed on 4 May 2017).
- König, J.; Wells, J.; Cani, P.D.; García-Ródenas, C.L.; MacDonald, T.; Mercenier, A.; Whyte, J.; Troost, F.; Brummer, R.-J. Human intestinal barrier function in health and disease. Clin. Transl. Gastroenterol. 2016, 7, e196. [Google Scholar] [CrossRef]
- David Gulbransen, B.; Tellez, G.; MacNaughton, W.; Clarke, G.; Kelly, J.R.; Kennedy, P.J.; Cryan, J.F.; Dinan, T.G.; Hyland, N.P. Breaking down the barriers: The gut microbiome, intestinal permeability and stress-related psychiatric disorders. Front. Cell. Neurosci. 2015, 9. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A. Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity, and cancer. Physiol. Rev. 2011, 91, 151–175. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Uzzau, S.; Goldblum, S.; Fasano, A. Human zonulin, a potential modulator of intestinal tight junctions. J. Cell Sci. 2000, 113, 4435–4440. [Google Scholar]
- Sturgeon, C.; Lan, J.; Fasano, A. Zonulin transgenic mice show altered gut permeability and increased morbidity/mortality in the DSS colitis model. Ann. N. Y. Acad. Sci. 2017, 1397, 130–142. [Google Scholar] [CrossRef]
- Vanuytsel, T.; Vermeire, S.; Cleynen, I. The role of Haptoglobin and its related protein, Zonulin, in inflammatory bowel disease. Tissue Barriers 2013, 1, e27321. [Google Scholar] [CrossRef] [Green Version]
- De Magistris, L.; Familiari, V.; Pascotto, A.; Sapone, A.; Frolli, A.; Iardino, P.; Carteni, M.; De Rosa, M.; Francavilla, R.; Riegler, G.; et al. Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 418–424. [Google Scholar] [CrossRef] [Green Version]
- Galiatsatos, P.; Gologan, A.; Lamoureux, E. Autistic enterocolitis: Fact or fiction? Can. J. Gastroenterol. 2009, 23, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Jyonouchi, H.; Geng, L.; Davidow, A.L. Cytokine profiles by peripheral blood monocytes are associated with changes in behavioral symptoms following immune insults in a subset of ASD subjects: An inflammatory subtype? J. Neuroinflammation 2014, 11, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakefield, A.J.; Ashwood, P.; Limb, K.; Anthony, A. The significance of ileo-colonic lymphoid nodular hyperplasia in children with autistic spectrum disorder. Eur. J. Gastroenterol. Hepatol. 2005, 17, 827–836. [Google Scholar] [CrossRef]
- Siniscalco, D.; Sapone, A.; Giordano, C.; Cirillo, A.; de Novellis, V.; de Magistris, L.; Rossi, F.; Fasano, A.; Maione, S.; Antonucci, N. The expression of caspases is enhanced in peripheral blood mononuclear cells of autism spectrum disorder patients. J. Autism Dev. Disord. 2012, 42, 1403–1410. [Google Scholar] [CrossRef]
- Severance, E.G.; Yolken, R.H.; Eaton, W.W. Autoimmune diseases, gastrointestinal disorders and the microbiome in schizophrenia: More than a gut feeling. Schizophr. Res. 2016, 176, 23–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasano, A. Zonulin, regulation of tight junctions, and autoimmune diseases. Ann. N. Y. Acad. Sci. 2012. [Google Scholar] [CrossRef] [Green Version]
- Sellin, J.H.; Odenwald, M.A.; Turner, J.R. Advances in translational science intestinal permeability defects: Is it time to treat? YJCGH 2013, 11, 1075–1083. [Google Scholar] [CrossRef]
- Fasano, A. Intestinal permeability and its regulation by zonulin: Diagnostic and therapeutic implications. Clin. Gastroenterol. Hepatol. 2012. [Google Scholar] [CrossRef] [Green Version]
- Bressan, P.; Kramer, P. Bread and other edible agents of mental disease. Front. Hum. Neurosci. 2016, 10, 130. [Google Scholar] [CrossRef] [Green Version]
- Clapp, M.; Aurora, N.; Herrera, L.; Bhatia, M.; Wilen, E.; Wakefield, S. Gut microbiota’s effect on mental health: The gut-brain axis. Clin. Pract. 2017, 7, 987. [Google Scholar] [CrossRef]
- Sturgeon, C.; Fasano, A. Zonulin, a regulator of epithelial and endothelial barrier functions, and its involvement in chronic inflammatory diseases. Tissue Barriers 2016, 4, e1251384. [Google Scholar] [CrossRef] [Green Version]
- Kiecolt-Glaser, J.K.; Derry, H.M.; Fagundes, C.P. Inflammation: Depression fans the flames and feasts on the heat. Am. J. Psychiatry 2015, 172, 1075–1091. [Google Scholar] [CrossRef]
- Kim, J.-W.; Szigethy, E.M.; Melhem, N.M.; Saghafi, E.M.; Brent, D.A. Inflammatory markers and the pathogenesis of pediatric depression and suicide. J. Clin. Psychiatry 2014, 75, 1242–1253. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.M.; Pearson, R.M.; Zammit, S.; Lewis, G.; Jones, P.B. Association of serum interleukin 6 and C-reactive protein in childhood with depression and psychosis in young adult life: A population-based longitudinal study. JAMA Psychiatry 2014, 71, 1121–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szondy, Z.; Korponay-Szabó, I.; Király, R.; Sarang, Z.; Tsay, G.J. Transglutaminase 2 in human diseases. BioMedicine 2017, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadoth, A.; Nefussy, B.; Bleiberg, M.; Klein, T.; Artman, I.; Drory, V.E. Transglutaminase 6 antibodies in the serum of patients with amyotrophic lateral sclerosis. JAMA Neurol. 2015, 72, 676. [Google Scholar] [CrossRef] [Green Version]
- Sekirov, I.; Russell, S.L.; Antunes, L.C.M.; Finlay, B.B. Gut microbiota in health and disease. Physiol. Rev. 2010, 90, 859–904. [Google Scholar] [CrossRef] [Green Version]
- Yano, J.M.; Yu, K.; Donaldson, G.P.; Shastri, G.G.; Ann, P.; Ma, L.; Nagler, C.R.; Ismagilov, R.F.; Mazmanian, S.K.; Hsiao, E.Y. Indigenous bacteria from the gut microbiota regulate host serotonin biosynthesis. Cell 2015, 161, 264–276. [Google Scholar] [CrossRef] [Green Version]
- Rogers, G.B.; Keating, D.J.; Young, R.L.; Wong, M.-L.; Licinio, J.; Wesselingh, S. From gut dysbiosis to altered brain function and mental illness: Mechanisms and pathways. Mol. Psychiatry 2016, 21, 738–748. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Zhu, G. Gut–brain axis and mood disorder. Front. Psychiatry 2018, 9, 223. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Shin, C. The microbiota-gut-brain axis in neuropsychiatric disorders: Patho-physiological mechanisms and novel treatments. Curr. Neuropharmacol. 2018, 16, 559. [Google Scholar] [CrossRef] [PubMed]
- Appleton, J. The gut-brain axis: Influence of microbiota on mood and mental health. Integr. Med. A Clin. J. 2018, 17, 28. [Google Scholar]
- Dam, S.A.; Mostert, J.C.; Szopinska-Tokov, J.W.; Bloemendaal, M.; Amato, M.; Arias-Vasquez, A. The role of the gut-brain axis in attention-deficit/hyperactivity disorder. Gastroenterol. Clin. North Am. 2019, 48, 407–431. [Google Scholar] [CrossRef] [PubMed]
- Budziszewska, B.; Basta-Kaim, A.; Kubera, M.; Lasoń, W. Immunological and endocrinological pattern in ADHD etiopathogenesis. Przegl. Lek. 2010, 67, 1200–1204. [Google Scholar] [PubMed]
- Julio-Pieper, M.; Bravo, J.A.; Aliaga, E.; Gotteland, M. Review article: Intestinal barrier dysfunction and central nervous system disorders—A controversial association. Aliment. Pharmacol. Ther. 2014, 40, 1187–1201. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 27 April 2020).
- Calarge, C.A.; Devaraj, S.; Shulman, R.J. Gut permeability and depressive symptom severity in unmedicated adolescents. J. Affect. Disord. 2019, 246, 586–594. [Google Scholar] [CrossRef]
- Dalton, N.; Chandler, S.; Turner, C.; Charman, T.; Pickles, A.; Loucas, T.; Simonoff, E.; Sullivan, P.; Baird, G. Gut permeability in autism spectrum disorders. Autism Res. 2014, 7, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaney, S.; Fallon, B.; Alaedini, A.; Yolken, R.; Indart, A.; Feng, T.; Wang, Y.; Javitt, D. Inflammatory biomarkers in psychosis and clinical high risk populations. Schizophr. Res. 2019, 206, 440–443. [Google Scholar] [CrossRef]
- De Santis, B.; Brera, C.; Mezzelani, A.; Soricelli, S.; Ciceri, F.; Moretti, G.; Debegnach, F.; Bonaglia, M.C.; Villa, L.; Molteni, M.; et al. Role of mycotoxins in the pathobiology of autism: A first evidence. Nutr. Neurosci. 2019, 22, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Gabriele, S.; Sacco, R.; Altieri, L.; Neri, C.; Urbani, A.; Bravaccio, C.; Riccio, M.P.; Iovene, M.R.; Bombace, F.; De Magistris, L.; et al. Slow intestinal transit contributes to elevate urinary p -cresol level in Italian autistic children. Autism Res. 2016, 9, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Iovene, M.R.; Bombace, F.; Maresca, R.; Sapone, A.; Iardino, P.; Picardi, A.; Marotta, R.; Schiraldi, C.; Siniscalco, D.; Serra, N.; et al. Intestinal dysbiosis and yeast isolation in stool of subjects with autism spectrum disorders. Mycopathologia 2017, 182, 349–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jyonouchi, H.; Sun, S.; Itokazu, N. Innate immunity associated with inflammatory responses and cytokine production against common dietary proteins in patients with autism spectrum disorder. Neuropsychobiology 2002, 46, 76–84. [Google Scholar] [CrossRef]
- Lau, N.M.; Green, P.H.R.; Taylor, A.K.; Hellberg, D.; Ajamian, M.; Tan, C.Z.; Kosofsky, B.E.; Higgins, J.J.; Rajadhyaksha, A.M.; Alaedini, A. Markers of celiac disease and gluten sensitivity in children with autism. PLoS ONE 2013, 8, e66155. [Google Scholar] [CrossRef] [Green Version]
- Pusponegoro, H.D.; Ismael, S.; Sastroasmoro, S.; Firmansyah, A.; Vandenplas, Y. Maladaptive behavior and gastrointestinal disorders in children with autism spectrum disorder. Pediatr. Gastroenterol. Hepatol. Nutr. 2015, 18, 230. [Google Scholar] [CrossRef] [Green Version]
- Suurmond, R.; van Rhee, H.; Hak, T. Introduction, comparison, and validation of Meta-Essentials: A free and simple tool for meta-analysis. Res. Synth. Methods 2017, 8, 537–553. [Google Scholar] [CrossRef] [Green Version]
- Seide, S.E.; Röver, C.; Friede, T. Likelihood-based random-effects meta-analysis with few studies: Empirical and simulation studies. BMC Med. Res. Methodol. 2019, 19, 16. [Google Scholar] [CrossRef]
- Ajamian, M.; Steer, D.; Rosella, G.; Gibson, P.R. Serum zonulin as a marker of intestinal mucosal barrier function: May not be what it seems. PLoS ONE 2019, 14, e0210728. [Google Scholar] [CrossRef] [PubMed]
- Swanson, J.; Sergeant, J.; Taylor, E.; Sonuga-Barke, E.; Jensen, P.; Cantwell, D. Attention-deficit hyperactivity disorder and hyperkinetic disorder. Lancet 1998, 351, 429–433. [Google Scholar] [CrossRef]
- Van der Plas, E.; Dupuis, A.; Arnold, P.; Crosbie, J.; Schachar, R. Association of autism spectrum disorder with obsessive-compulsive and attention-deficit/hyperactivity traits and response inhibition in a community sample. J. Autism Dev. Disord. 2016, 46, 3115–3125. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.J.; Charman, T.; Robinson, E.B.; Plomin, R.; Happé, F.; Asherson, P.; Ronald, A. Developmental associations between traits of autism spectrum disorder and attention deficit hyperactivity disorder: A genetically informative, longitudinal twin study. Psychol. Med. 2013, 43, 1735–1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau-Zhu, A.; Fritz, A.; McLoughlin, G. Overlaps and distinctions between attention deficit/hyperactivity disorder and autism spectrum disorder in young adulthood: Systematic review and guiding framework for EEG-imaging research. Neurosci. Biobehav. Rev. 2019, 96, 93. [Google Scholar] [CrossRef] [PubMed]
- Halpern, M.D.; Denning, P.W. The role of intestinal epithelial barrier function in the development of NEC. Tissue Barriers 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Wasilewska, J.; Klukowski, M. Gastrointestinal symptoms and autism spectrum disorder: Links and risks—A possible new overlap syndrome. Pediatr. Health Med. Ther. 2015, 6, 153–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horvath, K.; Perman, J.A. Autistic disorder and gastrointestinal disease. Curr. Opin. Pediatr. 2002, 14, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S.; et al. Nutritional and metabolic status of children with autism vs. neurotypical children, and the association with autism severity. Nutr. Metab. (Lond.) 2011, 8, 34. [Google Scholar] [CrossRef] [Green Version]
- Chaidez, V.; Hansen, R.L.; Hertz-Picciotto, I. Gastrointestinal problems in children with autism, developmental delays or typical development. J. Autism Dev. Disord. 2014, 44, 1117. [Google Scholar] [CrossRef] [Green Version]
- Miranda-Ribera, A.; Ennamorati, M.; Serena, G.; Cetinbas, M.; Lan, J.; Sadreyev, R.I.; Jain, N.; Fasano, A.; Fiorentino, M. Exploiting the zonulin mouse model to establish the role of primary impaired gut barrier function on microbiota composition and immune profiles. Front. Immunol. 2019, 10, 2233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fattorusso, A.; Di Genova, L.; Dell’isola, G.B.; Mencaroni, E.; Esposito, S. Autism spectrum disorders and the gut microbiota. Nutrients 2019, 11, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjivassiliou, M.; Mäki, M.; Sanders, D.S.; Williamson, C.A.; Grünewald, R.A.; Woodroofe, N.M.; Korponay-Szabó, I.R. Autoantibody Targeting of Brain and Intestinal Transglutaminase in Gluten Ataxia. Neurology 2006, 66, 373–377. [Google Scholar] [CrossRef]
- Adzic, M.; Brkic, Z.; Mitic, M.; Francija, E.; Jovicic, M.J.; Radulovic, J.; Maric, N.P. Therapeutic strategies for treatment of inflammation-related depression. Curr. Neuropharmacol. 2018, 16, 176. [Google Scholar] [CrossRef] [PubMed]
- Rea, K.; Dinan, T.G.; Cryan, J.F. Gut microbiota: A perspective for psychiatrists. Neuropsychobiology 2019. [Google Scholar] [CrossRef] [PubMed]
- Graziani, C.; Talocco, C.; De Sire, R.; Petito, V.; Lopetuso, L.R.; Gervasoni, J.; Persichilli, S.; Franceschi, F.; Ojetti, V.; Gasbarrini, A.; et al. Intestinal permeability in physiological and pathological conditions: Major determinants and assessment modalities. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 795–810. [Google Scholar] [PubMed]
- Zimomra, Z.R.; Porterfield, V.M.; Camp, R.M.; Johnson, J.D. Time-dependent mediators of HPA axis activation following live Escherichia coli. Am. J. Physiol. Integr. Comp. Physiol. 2011, 301, R1648–R1657. [Google Scholar] [CrossRef]
- Rees, J.C. Obsessive–compulsive disorder and gut microbiota dysregulation. Med. Hypotheses 2014, 82, 163–166. [Google Scholar] [CrossRef]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef]
- Finegold, S.M.; Summanen, P.H.; Downes, J.; Corbett, K.; Komoriya, T. Detection of clostridium perfringens toxin genes in the gut microbiota of autistic children. Anaerobe 2017, 45, 133–137. [Google Scholar] [CrossRef]
- Mccartney, A.L.; Parracho, H.M.R.T.; Bingham, M.O.; Gibson, G.R. Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children. J. Med. Microbiol. 2005, 54, 987–991. [Google Scholar] [CrossRef]
- Wang, L.; Angley, M.T.; Gerber, J.P.; Young, R.L.; Abarno, D.V.; McKinnon, R.A.; Sorich, M.J. Is urinary indolyl-3-acryloylglycine a biomarker for autism with gastrointestinal symptoms? Biomarkers 2009, 14, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Critchfield, J.W.; van Hemert, S.; Ash, M.; Mulder, L.; Ashwood, P. The potential role of probiotics in the management of childhood autism spectrum disorders. Gastroenterol. Res. Pract. 2011, 2011, 161358. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Conlon, M.A.; Christophersen, C.T.; Sorich, M.J.; Angley, M.T. Gastrointestinal microbiota and metabolite biomarkers in children with autism spectrum disorders. Biomark. Med. 2014, 8, 331–344. [Google Scholar] [CrossRef]
- Cenit, M.C.; Nuevo, I.C.; Codoñer-Franch, P.; Dinan, T.G.; Sanz, Y. Gut microbiota and attention deficit hyperactivity disorder: New perspectives for a challenging condition. Eur. Child Adolesc. Psychiatry 2017, 26, 1081–1092. [Google Scholar] [CrossRef]
- Flowers, S.A.; Evans, S.J.; Ward, K.M.; McInnis, M.G.; Ellingrod, V.L. Interaction between atypical antipsychotics and the gut microbiome in a bipolar disease cohort. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 261–267. [Google Scholar] [CrossRef]
- Bengesser, S.A.; Mörkl, S.; Painold, A.; Dalkner, N.; Birner, A.; Fellendorf, F.T.; Platzer, M.; Queissner, R.; Hamm, C.; Maget, A.; et al. Epigenetics of the molecular clock and bacterial diversity in bipolar disorder. Psychoneuroendocrinology 2019, 101, 160–166. [Google Scholar] [CrossRef]
- Lv, F.; Chen, S.; Wang, L.; Jiang, R.; Tian, H.; Li, J.; Yao, Y.; Zhuo, C. The role of microbiota in the pathogenesis of schizophrenia and major depressive disorder and the possibility of targeting microbiota as a treatment option. Oncotarget 2017, 8, 100899–100907. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Ling, Z.; Zhang, Y.; Mao, H.; Ma, Z.; Yin, Y.; Wang, W.; Tang, W.; Tan, Z.; Shi, J.; et al. Altered fecal microbiota composition in patients with major depressive disorder. Brain Behav. Immun. 2015, 48, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhang, L.; Wang, X.; Wang, Z.; Zhang, J.; Jiang, R.; Wang, X.; Wang, K.; Liu, Z.; Xia, Z.; et al. Similar fecal microbiota signatures in patients with diarrhea-predominant irritable bowel syndrome and patients with depression. Clin. Gastroenterol. Hepatol. 2016, 14, 1602–1611.e5. [Google Scholar] [CrossRef]
- Aizawa, E.; Tsuji, H.; Asahara, T.; Takahashi, T.; Teraishi, T.; Yoshida, S.; Ota, M.; Koga, N.; Hattori, K.; Kunugi, H. Possible association of Bifidobacterium and Lactobacillus in the gut microbiota of patients with major depressive disorder. J. Affect. Disord. 2016, 202, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Naseribafrouei, A.; Hestad, K.; Avershina, E.; Sekelja, M.; Linløkken, A.; Wilson, R.; Rudi, K. Correlation between the human fecal microbiota and depression. Neurogastroenterol. Motil. 2014, 26, 1155–1162. [Google Scholar] [CrossRef]
- Hemmings, S.M.J.; Malan-Müller, S.; van den Heuvel, L.L.; Demmitt, B.A.; Stanislawski, M.A.; Smith, D.G.; Bohr, A.D.; Stamper, C.E.; Hyde, E.R.; Morton, J.T.; et al. The microbiome in posttraumatic stress disorder and trauma-exposed controls. Psychosom. Med. 2017, 79, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, A.; Totino, V.; Cacciotti, F.; Iebba, V.; Neroni, B.; Bonfiglio, G.; Trancassini, M.; Passariello, C.; Pantanella, F.; Schippa, S. Rebuilding the gut microbiota ecosystem. Int. J. Environ. Res. Public Health 2018, 15, 1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; et al. Microbiota modulate behavioral and physiological abnormalities associated with neurodevelopmental disorders. Cell 2013, 155, 1451–1463. [Google Scholar] [CrossRef] [Green Version]
- Ashwood, P.; Krakowiak, P.; Hertz-Picciotto, I.; Hansen, R.; Pessah, I.; Van de Water, J. Elevated plasma cytokines in autism spectrum disorders provide evidence of immune dysfunction and are associated with impaired behavioral outcome. Brain Behav. Immun. 2011, 25, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A. Regulation of intercellular tight junctions by zonula occludens toxin and its eukaryotic analogue zonulin. Ann. N. Y. Acad. Sci. 2006, 915, 214–222. [Google Scholar] [CrossRef]
- Fasano, A.; Not, T.; Wang, W.; Uzzau, S.; Berti, I.; Tommasini, A.; Goldblum, S.E. Zonulin, a newly discovered modulator of intestinal permeability, and its expression in coeliac disease. Lancet 2000, 355, 1518–1519. [Google Scholar] [CrossRef]


| Population | Children (0–18 years) diagnosed with one or more of the following according to validated criteria; anxiety disorders (AD), autism spectrum disorder (ASD), attention deficit disorder (ADD), attention deficit and hyperactivity disorder (ADHD), bipolar disorder (BD), major depressive disorder (MDD), manic-depressive disorder, obsessive–compulsive disorder (OCD), and schizophrenia. Mental disorders should be diagnosed by a standard procedure such as experts’ diagnoses involving dimensional and multi-informant assessments, including recognized and validated rating scales. To be eligible for inclusion, the study also needed to address intestinal permeability. |
| Exposures | Biomarkers (intrinsic or endotoxins) for intestinal permeability such as zonulin, diamine oxidase (DAO), lipopolysaccharide (LPS), and lipopolysaccharide binding protein (LBP) in individuals diagnosed with one or more of the mental illnesses according to the validated criteria. |
| Comparison | Biomarkers (intrinsic or endotoxins) for intestinal permeability such as zonulin, diamine oxidase (DAO), lipopolysaccharide (LPS), and lipopolysaccharide binding protein (LBP) in controls. |
| Outcome | Comparing intestinal permeability values (serum zonulin, stool zonulin, serum diamine oxidase, serum LPS, or serum LPB) between children diagnosed with mental, behavioral, or neurodevelopment disorders and controls. |
| Reference ID | Study Characteristics | Reason for Exclusion |
|---|---|---|
| Calarger et al., 2019 [52] | Intervention study, major depressive disorder, children (age: 12–17), n = 41, analyzed urine; lactulose/mannitol recovery ratio. | Did not fulfill a priori inclusion criteria for biomarkers (zonulin, intestinal permeability). |
| Dalton et al., 2014 [53] | Intervention study, ASD, children (age: 10–14), n = 103, analyzed urine; lactulose/mannitol recovery ratio. | Did not fulfill a priori inclusion criteria for study type (observational) and participants (children 0–18 years). |
| Delaney et al., 2019 [54] | Observation cross-sectional study, Schizophrenia, children, adolescents, young adults (age: 8–35), n = 97, analyzed serum; 25 (OH) D, anti-LPS antibodies, CRP, IL-6 levels). | Did not fulfill a priori inclusion criteria for participants (children 0–18 years). |
| De Santis et al., 2019 [55] | Observational pilot study, ASD, children (age: 2–9), n = 110, analyzed mycotoxins. | Did not fulfill a priori inclusion criteria for biomarkers (zonulin, intestinal permeability). |
| Gabriele et al., 2016 [56] | Research study, ASD, children (age: 0–8), n = 53, analyzed urine; p-cresol levels. | Did not fulfill a priori inclusion criteria for study type, no controls. |
| Iovene et al., 2017 [57] | Intervention study, ASD, children (age: 3–9 approx.), n = 80, analyzed urine; lactulose/mannitol recovery ratio. | Did not fulfill a priori inclusion criteria for biomarkers (zonulin, intestinal permeability). |
| Jyonouchi et al., 2002 [58] | Intervention study, ASD, and DPI children, young adults, adults (age: 1–20), n = 209, analyzed; response to an elimination diet. | Did not fulfill a priori inclusion criteria for study type. |
| Lau et al., 2013 [59] | Cohort study, ASD, children (age: 4–12) n = 140, analyzed serum; IgG and IgA antibodies to gliadin. | Did not fulfill a priori inclusion criteria for biomarkers. |
| Pusponegoro et al., 2015 [60] | Observational cross-sectional study, ASD, children (age: 2–10), n = 268, analyzed urine; lactulose/mannitol recovery ratio. | Did not fulfill a priori inclusion criteria for study type. |
| References | Country | Participants | Mean Age | Measurement/Diagnosis | ||
|---|---|---|---|---|---|---|
| ASD | ADHD | OCD | ||||
| Özyurt et al., 2018 [5] | Turkey | Total Blood (81). 40 ADHD/41 HC | ADHD: 7.9/HC: 7.8 | N/A | Blood: Serum Zonulin/DuPaul ADHD-RS-IV Inventory | N/A |
| Esnafoglu et al., 2017 [6] | Turkey | Total Blood (65). 32 ASD/33 HC | ASD: 7.5/HC: 7.0 | Blood: Serum Zonulin and BMI/CARS | N/A | N/A |
| Józefczuk et al., 2017 [7] | Poland | Total Blood (121). 75 ASD/46 HC | ASD: 8.1/HC: N/A | Blood: Serum Zonulin and CSA, AGA, I-FABP, /ADI-R, ADOS Scale | N/A | N/A |
| Rose et al., 2018 [8] | U.S.A. California | Total Blood (87). 46 ASD (NoGI: 26, GI: 20), 41 TD (NoGI: 35, GI:6; Total Stool (91). 50 ASD (NoGI: 29, GI: 21), 41 TD (NoGI: 34, GI: 7) | Blood: ASD- NoGI: 7.8/TD-NoGI: 6.8; ASD-GI: 5.7/TD-GI: 5.2; Stool: ASD- NoGI: 7.8/TD-NoGI: 7.1; ASD-GI: 6.6/TD-GI: 5.1 | Blood: Plasma Haptoglobin and Stool: Microbiome/ADI-R, ADOS | N/A | N/A |
| Işık et al., 2020 [9] | Turkey | Total Blood (48). 24 OCD/24 HC | OCD: 14.3/HC: 13.7 | N/A | N/A | Blood: Serum Zonulin and serum Claudin-5 and BMI/K-SADS-PL, DSM-5 and CY-BOCS, M.O.C.I., RCADS-CV |
| First Author, Year of Publication, Country | Participants Included in the Study Based on Serum Zonulin and Plasma Haptoglobin | Main Study Findings | Authors Conclusions |
|---|---|---|---|
| Özyurt et al., 2018, Turkey [5] | 81 | Children with ADHD had significantly elevated levels of zonulin compared to controls. Children with hyperactive/impulsive presentations had significantly elevated zonulin compared to other presentations. ADHD symptoms and social communication problems correlated significantly with zonulin levels, and hyperactive/impulsive and social communication symptoms were important predictors of zonulin levels. | “Regardless of its limitations, the results of our study suggest that zonulin levels may be elevated in children with ADHD (especially the hyperactive/impulsive presentation) and that this elevation correlated with social deficits. Symptoms of hyperactivity/impulsivity and social deficits independently predict zonulin levels in children with ADHD although the changes in adjusted R2 suggest that the majority of the predictive value lies with symptoms of hyperactivity/impulsivity.” |
| Esnafoglu et al., 2017, Turkey [6] | 65 | There was an increase in serum zonulin levels in the group with ASD compared with the healthy control group. Additionally, for all subjects, there was a positive correlation identified between the CARS score, indicating severity of autism, and zonulin. | “Increased zonulin levels in patients with ASD may play a role in the development of ASD symptoms. However, zonulin upregulation and subsequent increase in intestinal permeability may be necessary but not sufficient to develop ASD, because other factors are likely at play.” |
| Józefczuk et al., 2017, Poland [7] | 121 | Concentrations of zonulin were the highest in the youngest children (5 years). The mean level of zonulin in this group was significantly higher compared with patients aged 6–11 years. The occurrence of anti-TG6 antibodies in ASD patients with normal mucosa was not associated with CD. | “There is a subgroup of ASD patients whichrespond to gluten with increased production of antibodies against native gluten and neural TG6, but not of typical celiac-specific antibodies, and this production is not related to serological markers of an impaired intestinal barrier.” |
| Rose et al., 2018, California [8] | 87 | Children with ASD who experience GI symptoms have an imbalance in their immune response, possibly influenced by or influencing metagenomic changes, and may have a propensity to impaired gut barrier function, which may contribute to their symptoms and clinical outcome. | “We found several differences when comparing children with ASD who exhibit GI symptoms vs. those that did not. The most notable of these was the reduced regulatory TGFb1 response of the ASDGI groups following stimulation. We also noted an increase in the production of cytokines linked to mucosal inflammation after TLR-4 stimulation in children with ASDGI symptoms relative to children with ASDNoGI. Our analysis of the microbiome underscores the relationship between the presence of GI symptoms and the host microflora and suggest a possible role of dysbiosis in the co-morbidity of GI issues in ASD” |
| Işık et al., 2020, Turkey [9] | 48 | There was an increase in serum claudin-5 levels in the group with OCD compared with the healthy control group. There was no significant difference between the study and control group in the serum zonulin concentrations. | “Regardless of the limitations, taken together with our results, dysregulation of the BBB, especially claudin-5, may be involved in the etiology of OCD. Further detailed and more comprehensive studies designed on a longitudinal basis are greatly needed to find out exactly whether increased claudin- 5 levels are the cause or consequence of the disease process in OCD” |
| Study | Serum Zonulin Levels (ng/mL) in Patients and Control Groups | |||||||
|---|---|---|---|---|---|---|---|---|
| Patient Group | Control Group | |||||||
| n | Mean Zonulin | S.D. | n | Mean Zonulin | SD | p-Value | ||
| Özyurt et al., ADHD (n)/(ng/mL), mean ± SD | 40 | 105.36 | 98.38 | 41 | 63.34 | 73.4 | 0.031 | |
| Esnafoglu et al., ASD (n)/(ng/mL), mean ± SD | 32 | 122.3 | 98.46 | 33 | 41.89 | 45.83 | <0.001 | |
| Józefczuk et al., ASD (n)/(ng/mL), mean ± SD | 75 | 17.2 | 15.7 | 46 | 15.3 | 5.9 | >0.05 | |
| Işık et al., OCD (n)/(ng/mL), mean ± SD | 24 | 98.93 | 83.06 | 24 | 103.7 | 73.53 | 0.834 | |
| Study | Selection of Controls | Definition of Controls | Non- Response Rate | Final Score |
|---|---|---|---|---|
| Özyurt et al., ADHD [5] | 0 | * | * | 8/9 (strong) |
| Esnafoglu et al., ASD [6] | 0 | * | * | 8/9 (strong) |
| Józefczuk et al., ASD [7] | 0 | 0 | 0 | 6/9 (moderate) |
| Rose et al., ASD [8] | * | * | 0 | 8/9 (strong) |
| Işık et al., OCD [9] | 0 | * | 0 | 7/9 (strong) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asbjornsdottir, B.; Snorradottir, H.; Andresdottir, E.; Fasano, A.; Lauth, B.; Gudmundsson, L.S.; Gottfredsson, M.; Halldorsson, T.I.; Birgisdottir, B.E. Zonulin-Dependent Intestinal Permeability in Children Diagnosed with Mental Disorders: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1982. https://doi.org/10.3390/nu12071982
Asbjornsdottir B, Snorradottir H, Andresdottir E, Fasano A, Lauth B, Gudmundsson LS, Gottfredsson M, Halldorsson TI, Birgisdottir BE. Zonulin-Dependent Intestinal Permeability in Children Diagnosed with Mental Disorders: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(7):1982. https://doi.org/10.3390/nu12071982
Chicago/Turabian StyleAsbjornsdottir, Birna, Heiddis Snorradottir, Edda Andresdottir, Alessio Fasano, Bertrand Lauth, Larus S. Gudmundsson, Magnus Gottfredsson, Thorhallur Ingi Halldorsson, and Bryndis Eva Birgisdottir. 2020. "Zonulin-Dependent Intestinal Permeability in Children Diagnosed with Mental Disorders: A Systematic Review and Meta-Analysis" Nutrients 12, no. 7: 1982. https://doi.org/10.3390/nu12071982
APA StyleAsbjornsdottir, B., Snorradottir, H., Andresdottir, E., Fasano, A., Lauth, B., Gudmundsson, L. S., Gottfredsson, M., Halldorsson, T. I., & Birgisdottir, B. E. (2020). Zonulin-Dependent Intestinal Permeability in Children Diagnosed with Mental Disorders: A Systematic Review and Meta-Analysis. Nutrients, 12(7), 1982. https://doi.org/10.3390/nu12071982