Are the Results of a Combined Behavioural and Surgical Treatment of Morbid Obesity Satisfactory and Predictable?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Inclusion Criteria
2.3. Interventions
2.4. Variables
- Demographic and anthropometric data: age (years), gender (male/female), height (m), body weight (kg), and body mass index (BMI; kg/m2);
- Weight loss was measured as reduction in BMI and relative loss of excess BMI above 25 km/m2 (%EBMIL). Treatment success was defined as %EBMIL ≥ 50%;
- Social factors: cohabitation (yes/no); education (number of years); employed (yes/no); smoking (daily/not daily);
- Dietary habits: The diet was assessed with a validated food frequency questionnaire, and the daily intake was based on the Norwegian food composition table [16]. Use of coffee was measured as number of cups per day. Alcohol intake was measured as more/less frequently than once a month;
- The physical activity score was calculated as the sum of two scores and classified as follows: easy activity (not sweaty/breathless)—none; <1 h/week, 1–2 h/week, and >3 h/week (scores 0–3); strenuous activity (sweaty/breathless)—none; <1 h/week, 1–2 h/week, and >3 h/week (scores 0, 3, 4, and 5). The total sum of the scores for physical activity was 0–8;
- Comorbidities: The participants were asked about the presence of 12 current or previous disorders (yes/no; scores: 0–12);
- Musculoskeletal pain from six parts of the body (scores 0–12);
- The World Health Organisation – Five Well-Being Index (WHO-5) (scores 0–100; scores ≤50 indicate low mood and scores ≤28 indicate likely depression) [17];
- Hopkins Symptom Checklist 10 to measure psychological distress (scores 1–4; scores ≥ 1.85 indicate mental distress) [18];
- Fatigue Severity Scale: A validated Norwegian translation of the Fatigue Severity Scale was used (scores 9–63; scores ≥ 36 indicate further evaluation) [19];
- Epworth Sleepiness Scale: A validated Norwegian translation was used (scores 0–24; normal 0–10; mild 11–14; moderate 15–18; severe 19–25) [22];
- Sense of Humour Questionnaire: A Norwegian version of the short form SHQ-6: “Attitudes toward humour” was used (scores 6–24) [23];
- Suter’s food tolerance questionnaire (scores 1–27; high score = good food tolerance) [24].
2.5. Statistics
2.6. Ethics
3. Results
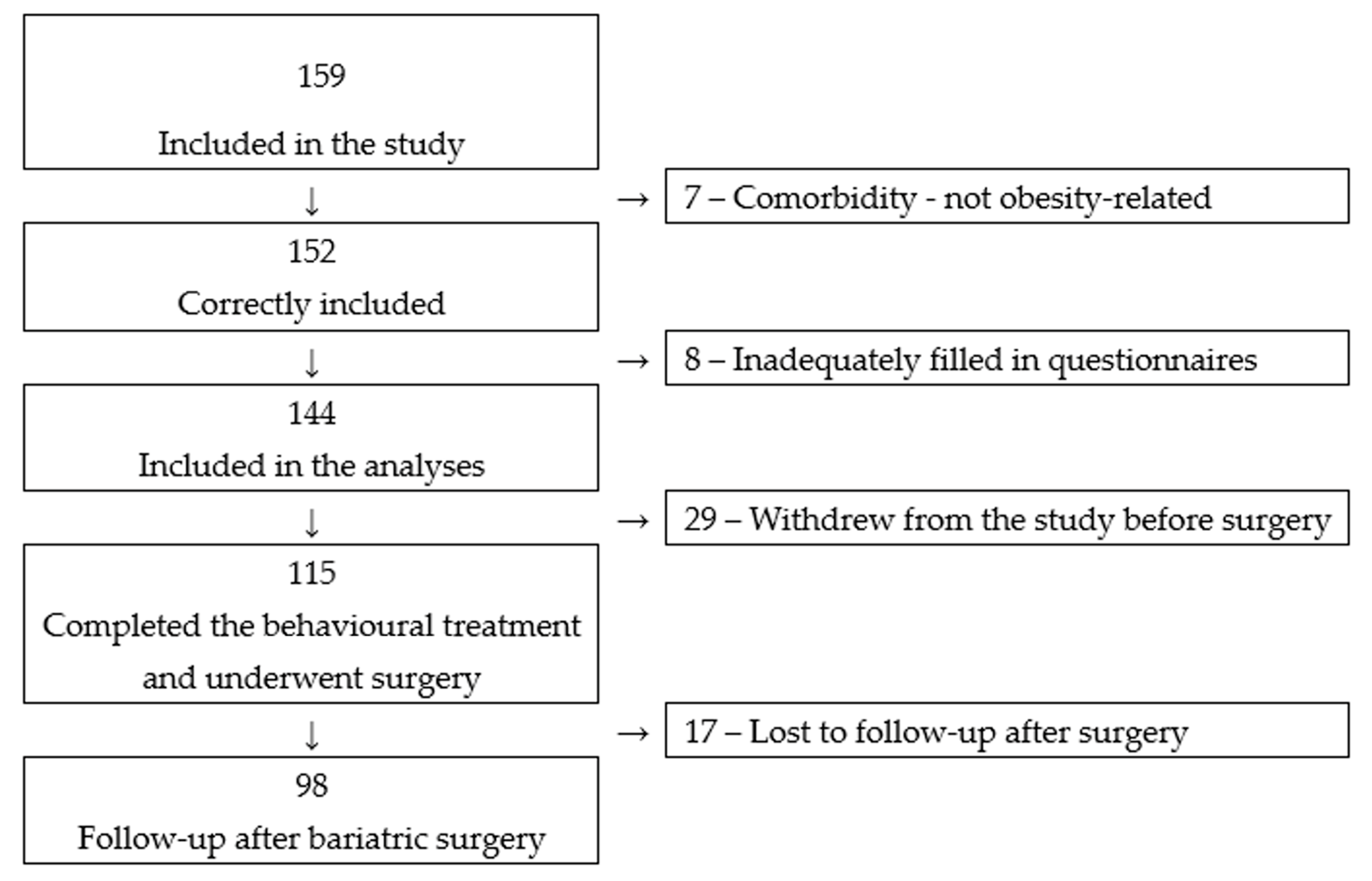
3.1. Participants
3.2. Participants’ Characteristics at Inclusion
3.3. Weight Loss during the Two Treatment Periods
3.4. Associations between Weight Loss after the Two Treatment Periods
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- WHO. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 5 June 2020).
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for weight loss in adults. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Gloy, V.L.; Briel, M.; Bhatt, D.L.; Kashyap, S.R.; Schauer, P.R.; Mingrone, G.; Bucher, H.C.; Nordmann, A.J. Bariatric surgery versus non-surgical treatment for obesity: A systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 347, f5934. [Google Scholar] [CrossRef] [Green Version]
- Hall, K.D.; Kahan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef]
- Sima, E.; Webb, D.L.; Hellstrom, P.M.; Sundbom, M. Non-responders After Gastric Bypass Surgery for Morbid Obesity: Peptide Hormones and Glucose Homeostasis. Obes. Surg. 2019, 29, 4008–4017. [Google Scholar] [CrossRef] [Green Version]
- Van de Laar, A.W.; van Rijswijk, A.S.; Kakar, H.; Bruin, S.C. Sensitivity and Specificity of 50% Excess Weight Loss (50%EWL) and Twelve Other Bariatric Criteria for Weight Loss Success. Obes. Surg. 2018, 28, 2297–2304. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Allison, K.C.; Wadden, T.A.; Ashare, R.; Spitzer, J.C.; McCuen-Wurst, C.; LaGrotte, C.; Williams, N.N.; Edwards, M.; Tewksbury, C.; et al. Psychopathology, disordered eating, and impulsivity as predictors of outcomes of bariatric surgery. Surg. Obes. Relat. Dis. 2019, 15, 650–655. [Google Scholar] [CrossRef]
- Livhits, M.; Mercado, C.; Yermilov, I.; Parikh, J.A.; Dutson, E.; Mehran, A.; Ko, C.Y.; Gibbons, M.M. Preoperative predictors of weight loss following bariatric surgery: Systematic review. Obes. Surg. 2012, 22, 70–89. [Google Scholar] [CrossRef]
- Aasbrenn, M.; Farup, P.G.; Videm, V. Changes in C-reactive protein, neopterin and lactoferrin differ after conservative and surgical weight loss in individuals with morbid obesity. Sci. Rep. 2019, 9, 17695. [Google Scholar] [CrossRef]
- Farup, P.G.; Aasbrenn, M.; Valeur, J. Separating “good” from “bad” faecal dysbiosis-evidence from two cross-sectional studies. BMC Obes. 2018, 5, 30. [Google Scholar] [CrossRef]
- Farup, P.G.; Valeur, J. Changes in Faecal Short-Chain Fatty Acids after Weight-Loss Interventions in Subjects with Morbid Obesity. Nutrients 2020, 12, 802. [Google Scholar] [CrossRef] [Green Version]
- Kvehaugen, A.S.; Farup, P.G. Changes in gastrointestinal symptoms and food tolerance 6 months following weight loss surgery: Associations with dietary changes, weight loss and the surgical procedure. BMC Obes. 2018, 5, 29. [Google Scholar] [CrossRef]
- Schauer, P.R.; Ikramuddin, S.; Hamad, G.; Eid, G.M.; Mattar, S.; Cottam, D.; Ramanathan, R.; Gourash, W. Laparoscopic gastric bypass surgery: Current technique. J. Laparoendosc Adv. Surg. Tech. A 2003, 13, 229–239. [Google Scholar] [CrossRef]
- Roa, P.E.; Kaidar-Person, O.; Pinto, D.; Cho, M.; Szomstein, S.; Rosenthal, R.J. Laparoscopic sleeve gastrectomy as treatment for morbid obesity: Technique and short-term outcome. Obes. Surg. 2006, 16, 1323–1326. [Google Scholar] [CrossRef]
- Norwegian Food Safety Authority. Food Database. Available online: http://www.matvaretabellen.no/?language=en (accessed on 5 June 2020).
- Topp, C.W.; Ostergaard, S.D.; Sondergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Søgaard, A.J.; Bjelland, I.; Tell, G.S.; Røysamb, E. A comparison of the CONOR Mental Health Index to the HSCL-10 and HADS. Norsk. Epidemiologi. 2003, 13, 279–284. [Google Scholar]
- Lerdal, A.; Wahl, A.; Rustoen, T.; Hanestad, B.R.; Moum, T. Fatigue in the general population: A translation and test of the psychometric properties of the Norwegian version of the fatigue severity scale. Scand. J. Public Health 2005, 33, 123–130. [Google Scholar] [CrossRef]
- Alessandri, G.; Vecchione, M.; Eisenberg, N.; Laguna, M. On the factor structure of the Rosenberg (1965) General Self-Esteem Scale. Psychol. Assess 2015, 27, 621–635. [Google Scholar] [CrossRef] [Green Version]
- Von Soest, T. Rosenbergs selfølelsesskala: Validering av en norsk oversettelse. Tidsskr. Nor. Psykologforen 2005, 42, 226–228. [Google Scholar]
- Beiske, K.K.; Kjelsberg, F.N.; Ruud, E.A.; Stavem, K. Reliability and validity of a Norwegian version of the Epworth sleepiness scale. Sleep Breath. 2009, 13, 65–72. [Google Scholar] [CrossRef]
- Svebak, S. The development of the Sense of Humor Questionnaire: From SHQ to SHQ-6. Humor-Int. J. Humor Res. 1996, 9, 341–362. [Google Scholar] [CrossRef]
- Suter, M.; Calmes, J.M.; Paroz, A.; Giusti, V. A new questionnaire for quick assessment of food tolerance after bariatric surgery. Obes. Surg. 2007, 17, 2–8. [Google Scholar] [CrossRef]
- Tan, S.Y.T.; Loi, P.L.; Lim, C.H.; Ganguly, S.; Syn, N.; Tham, K.W.; Tan, H.C.; Chan, W.H.; Wong, H.M.; Lee, P.C. Preoperative Weight Loss via Very Low Caloric Diet (VLCD) and Its Effect on Outcomes After Bariatric Surgery. Obes. Surg. 2020, 30, 2099–2107. [Google Scholar] [CrossRef]
- SOReg. Scandinavian Obesity Surgery Registry. Årsrapport SOReg 2015. Available online: https://www.ucr.uu.se/soreg/component/edocman/2016-10-19-arsrapport-2015-del-2/viewdocument/362?Itemid= (accessed on 5 June 2020).
- Livhits, M.; Mercado, C.; Yermilov, I.; Parikh, J.A.; Dutson, E.; Mehran, A.; Ko, C.Y.; Gibbons, M.M. Does weight loss immediately before bariatric surgery improve outcomes: A systematic review. Surg. Obes. Relat. Dis. 2009, 5, 713–721. [Google Scholar] [CrossRef]
- Stefura, T.; Dros, J.; Kacprzyk, A.; Wierdak, M.; Proczko-Stepaniak, M.; Szymanski, M.; Pisarska, M.; Malczak, P.; Rubinkiewicz, M.; Wysocki, M.; et al. Influence of Preoperative Weight Loss on Outcomes of Bariatric Surgery for Patients Under the Enhanced Recovery After Surgery Protocol. Obes. Surg. 2019, 29, 1134–1141. [Google Scholar] [CrossRef] [Green Version]
- LeBlanc, E.L.; Patnode, C.D.; Webber, E.M.; Redmond, N.; Rushkin, M.; O’Connor, E.A. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews. In Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018. [Google Scholar]
- Menezes, M.C.; Duarte, C.K.; Costa, D.V.P.; Lopes, M.S.; Freitas, P.P.; Campos, S.F.; Lopes, A.C.S. A systematic review of effects, potentialities, and limitations of nutritional interventions aimed at managing obesity in primary and secondary health care. Nutrition 2020, 75–76, 110784. [Google Scholar] [CrossRef]
- Nickel, F.; de la Garza, J.R.; Werthmann, F.S.; Benner, L.; Tapking, C.; Karadza, E.; Wekerle, A.L.; Billeter, A.T.; Kenngott, H.G.; Fischer, L.; et al. Predictors of Risk and Success of Obesity Surgery. Obes. Facts. 2019, 12, 427–439. [Google Scholar] [CrossRef]
- Paulsen, J.S.; Miller, A.C.; Hayes, T.; Shaw, E. Cognitive and behavioral changes in Huntington disease before diagnosis. Handb. Clin. Neurol. 2017, 144, 69–91. [Google Scholar] [CrossRef]
- Wimmelmann, C.L.; Dela, F.; Mortensen, E.L. Psychological predictors of weight loss after bariatric surgery: A review of the recent research. Obes. Res. Clin. Pract. 2014, 8, e299–e313. [Google Scholar] [CrossRef]
- Marek, R.J.; Ben-Porath, Y.S.; Heinberg, L.J. Understanding the role of psychopathology in bariatric surgery outcomes. Obes. Rev. 2016, 17, 126–141. [Google Scholar] [CrossRef]
- Carden, A.; Blum, K.; Arbaugh, C.J.; Trickey, A.; Eisenberg, D. Low socioeconomic status is associated with lower weight-loss outcomes 10-years after Roux-en-Y gastric bypass. Surg. Endosc. 2019, 33, 454–459. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Bariatric Surgery | Statistics | |
|---|---|---|---|
| Yes (No 115) | No (No 29) | (p-Value) | |
| Gender (men/women) | 24 (21%)/91 (79%) | 7 (24%)/22 (76%) | 0.801 |
| Age (years) | 42.8 (8.7) | 44.1 (9.0) | 0.484 |
| BMI at inclusion | 41.9 (3.9) | 43.0 (3.4) | 0.202 |
| BMI reduction after behavioural therapy 1 | 3.1 (1.7) | 1.8 (1.8) | 0.181 |
| %EBMIL 2 after behavioural therapy (%) 1 | 19.3 (10.8) | 8.7 (7.6) | 0.094 |
| Cohabitation (yes/no) | 89 (77%)/26 (23%) | 16 (55%)/13 (45%) | 0.021 |
| Education (years) | 12.6 (3.6) | 12.3 (4.3) | 0.737 |
| Employed (yes/no) | 90 (78%)/25 (22%) | 20 (71%)/8 (29%) | 0.459 |
| Coffee (cups/day) | 3.1 (2.5) | 2.4 (2.4) | 0.216 |
| Smoker (daily/not daily) | 23 (20%)/92 (80%) | 2 (7%)/27 (93%) | 0.109 |
| Alcohol 3 | 56 (49%)/59 (51%) | 12 (41%)/17 (59%) | 0.536 |
| Physical activity (scores 0–8) | 4.5 (2.2) | 4.5 (2.2) | 0.980 |
| Burden of comorbidity (scores 0–12) 4 | 1.7 (1.3) | 2.2 (1.6) | 0.100 |
| Musculoskeletal pain (scores 0–12) | 4.4 (3.0) | 3.8 (2.7) | 0.338 |
| WHO-5 (The World Health Organisation – Five) Well-Being Index (scores 0–100) | 59 (18) | 61 (16) | 0.621 |
| Hopkins symptom checklist 10 (scores 1–4) | 1.56 (0.50) | 1.68 (0.67) | 0.296 |
| Fatigue severity score (scores 1–7) | 4.0 (1.6) | 3.8 (1.7) | 0.628 |
| Rosenberg self-esteem scale (scores 0–30) | 18.2 (5.1) | 18.0 (5.7) | 0.839 |
| Epworth sleepiness scale (scores 0–24) | 8.2 (4.7) | 7.8 (4.8) | 0.354 |
| Sense of humour questionnaire (scores 6–24) | 19.3 (2.3) | 18.6 (3.8) | 0.171 |
| Food tolerance (Suter questionnaire) (scores 1–27) | 24.1 (2.3) | 23.8 (3.1) | 0.643 |
| Treatment Period | BMI (kg/m2) Reduction | %EBMIL |
|---|---|---|
| 1st period: Inclusion to Surgery | 3.2 (1.7) | 19.0 (10.9) |
| 2nd period: Surgery to 6-month follow-up | 8.6 (2.3) | 52.1 (14.7) |
| Overall: Inclusion to 6-month follow-up | 11.7 (2.7) | 71.2 (18.5) |
| Independent Variables 1 | Dependent Variables | |||
|---|---|---|---|---|
| BMI Reduction | %EBMIL | |||
| B (95% CI) | p-Value | B (95% CI) | p-Value | |
| Gender (women/men) | 0.21 (−1.15; 1.58) | 0.756 | −4.47 (−13.6; 4.7) | 0.335 |
| Age (years) | −0.02 (−0.09; 0.04) | 0.479 | 0.42 (−0.02; 0.87) | 0.062 |
| Type of operation (sleeve/bypass) | 0.62 (−0.80; 2.04) | 0.389 | −6.27 (−15.8; 3.3) | 0.194 |
| BMI at inclusion | 0.28 (0.12; 0.43) | 0.001 | −2.29 (−3.30; −1.28) | <0.001 |
| Cohabitation (yes) | −0.52 (−2.05; 1.01) | 0.502 | −3.70 (−13.96; 6.57) | 0.477 |
| Education (years) | −0.02 (−0.18; 0.13) | 0.767 | −0.27 (−1.30; 0.76) | 0.602 |
| Employed (yes) | 0.94 (−0.34; 2.22) | 0.148 | −3.42 (−12.07; 5.23) | 0.435 |
| Coffee (cups/day) | 0.02 (−0.22; 0.26) | 0.849 | −0.54 (−2.14; 1.06) | 0.506 |
| Smoker (daily) | 0.18 (−1.26; 1.62) | 0.809 | 1.37 (−8.31; 11.04) | 0.780 |
| Alcohol 2 | 0.152 (−0.97; 1.27) | 0.788 | −3.54 (−11.00; 3.93) | 0.350 |
| Physical activity (scores 0–8) | −0.11 (−0.36; 0.14) | 0.385 | −0.48 (−2.15; 1.19) | 0.569 |
| Burden of comorbidity (scores 0–12) 3 | −0.28 (−0.65; 0.16) | 0.228 | 0.11 (−2.63; 2.84) | 0.940 |
| Musculoskeletal pain (scores 0–12) | 0.09 (−0.10; 0.27) | 0.354 | 0.78 (−0.46; 2.03) | 0.215 |
| WHO-5 Well-Being Index (scores 0–100) | −0.03 (−0.06; 0.002) | 0.064 | −0.17 (−0.37; 0.03) | 0.091 |
| Hopkins symptom checklist 10 (scores 1–4) | 0.70 (−0.39; 1.80) | 0.205 | 4.17 (−3.2; 11.54) | 0.264 |
| Fatigue severity score (scores 1–7) | 0.17 (−0.17; 0.50) | 0.322 | 0.14 (−2.11; 2.38) | 0.904 |
| Rosenberg self-esteem scale (scale 0–30) | −0.01 (−0.12; 0.10 | 0.854 | −0.19 (−0.94; 0.56) | 0.620 |
| Epworth sleepiness scale (scores 0–24 | 0.05 (−0.07; 0.17) | 0.381 | 0.63 (−0.15; 1.41) | 0.114 |
| Sense of humour questionnaire (scores 6–24) | 0.31 (0.07; 0.55) | 0.010 | 0.32 (−1.32; 1.96) | 0.701 |
| Food tolerance (Suter questionnaire) (scores 1–27) | 0.04 (−0.20; 0.28) | 0.737 | 0.16 (−1.47; 1.76) | 0.858 |
| Independent Variables 1 | Dependent Variables | |||
|---|---|---|---|---|
| BMI Reduction 2nd Period | %EBMIL 2nd Period | |||
| B (95% CI) | p-Value | B (95% CI) | p-Value | |
| Gender (women/men) | −0.13 (−1.27; 1.00) | 0.815 | −5.0 (−12.5; 2.4) | 0.185 |
| Age (years) | −0.07 (−0.12; −0.01) | 0.022 | −0.06 (−0.45; 0.33) | 0.751 |
| Type of operation (sleeve/bypass) | 0.40 (−0.78; 1.58) | 0.503 | −4.1 (−11.9; 3.8) | 0.305 |
| BMI reduction 1st period | −0.03 (−0.32; 0.26) | 0.840 | --- | |
| %EBMIL 1st period | --- | 0.07 (−0.24; 0.37) | 0.664 | |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farup, P.G. Are the Results of a Combined Behavioural and Surgical Treatment of Morbid Obesity Satisfactory and Predictable? Nutrients 2020, 12, 1997. https://doi.org/10.3390/nu12071997
Farup PG. Are the Results of a Combined Behavioural and Surgical Treatment of Morbid Obesity Satisfactory and Predictable? Nutrients. 2020; 12(7):1997. https://doi.org/10.3390/nu12071997
Chicago/Turabian StyleFarup, Per G. 2020. "Are the Results of a Combined Behavioural and Surgical Treatment of Morbid Obesity Satisfactory and Predictable?" Nutrients 12, no. 7: 1997. https://doi.org/10.3390/nu12071997
APA StyleFarup, P. G. (2020). Are the Results of a Combined Behavioural and Surgical Treatment of Morbid Obesity Satisfactory and Predictable? Nutrients, 12(7), 1997. https://doi.org/10.3390/nu12071997