Magnesium Sulfate-Rich Natural Mineral Waters in the Treatment of Functional Constipation–A Review

Abstract
:1. Functional Constipation
2. Current Treatments
2.1. First-Line Recommendations
2.2. Drug Treatments
2.2.1. Bulk Laxatives
2.2.2. Lubricants and Emollients
2.2.3. Stimulant Laxatives
2.2.4. Osmotic Laxatives
Saccharides
Polyethylene Glycols (PEG)
Magnesium Oxide
2.3. Probiotics
3. Magnesium Sulfate-Rich Natural Mineral Waters
3.1. Hépar
3.2. Ensinger Schiller Quelle
3.3. Donat Mg
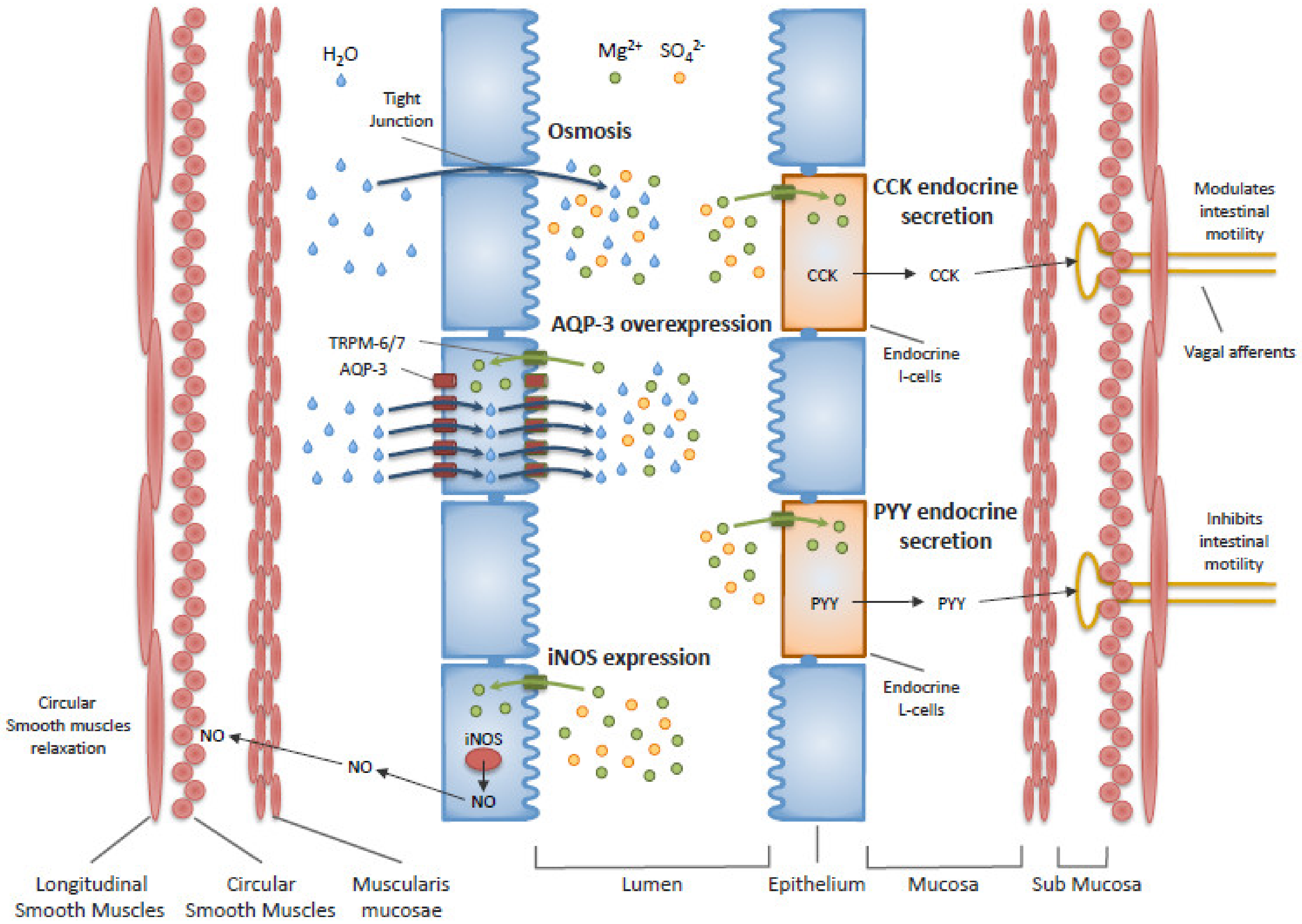
3.4. Mechanisms of Action
3.5. Overview
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mugie, S.M.; Benninga, M.A.; Di Lorenzo, C. Epidemiology of constipation in children and adults: A systematic review. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; Kellow, J.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Suares, N.C.; Ford, A.C. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: Systematic review and meta-analysis. Am. J. Gastroenterol. 2011, 106, 1582–1591. [Google Scholar] [CrossRef]
- Wald, A.; Scarpignato, C.; Mueller-Lissner, S.; Kamm, M.A.; Hinkel, U.; Helfrich, I.; Schuijt, C.; Mandel, K.G. A multinational survey of prevalence and patterns of laxative use among adults with self-defined constipation. Aliment. Pharmacol. Ther. 2008, 28, 917–930. [Google Scholar] [CrossRef] [PubMed]
- Zeitoun, J.D.; de Parades, V. Chronic constipation in adults. Presse Med. 2013, 42, 1176–1185. [Google Scholar] [CrossRef] [PubMed]
- Markland, A.D.; Palsson, O.; Goode, P.S.; Burgio, K.L.; Busby-Whitehead, J.; Whitehead, W.E. Association of low dietary intake of fiber and liquids with constipation: Evidence from the national health and nutrition examination survey. Am. J. Gastroenterol. 2013, 108, 796–803. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Sasaki, S.; Okubo, H.; Takahashi, Y.; Hosoi, Y.; Itabashi, M. Association between dietary fiber, water and magnesium intake and functional constipation among young Japanese women. Eur. J. Clin. Nutr. 2006, 61, 616–622. [Google Scholar] [CrossRef] [Green Version]
- Maxion-Bergemann, S.; Thielecke, F.; Abel, F.; Bergemann, R. Costs of irritable bowel syndrome in the UK and US. Pharmacoeconomics 2006, 24, 21–37. [Google Scholar] [CrossRef]
- Wald, A.; Scarpignato, C.; Kamm, M.A.; Helfrich, I.; Schuijt, C.; Bubeck, J.; Limoni, C.; Petrini, O.; Mueller-Lissner, S. The burden of constipation on quality of life: Results of a multinational survey. Aliment. Pharmacol. Ther. 2007, 26, 227–236. [Google Scholar] [CrossRef]
- Piche, T.; Dapoigny, M.; Bouteloup, C.; Chassagne, P.; Coffin, B.; Desfourneaux, V.; Fabiani, P.; Fatton, B.; Flammenbaum, M.; Jacquet, A.; et al. Recommendations for the clinical management and treatment of chronic constipation in adults. Gastroentérologie Clinique et Biologique 2007, 31, 125–135. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paré, P.; Fedorak, R. Systematic review of stimulant and nonstimulant laxatives for the treatment of functional constipation. Can. J. Gastroenterol. Hepatol. 2014, 28, 549–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alison, L.H.; Bulugahapitiya, D. Laxative induced magnesium poisoning in a 6 week old infant. BMJ 1990, 300, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelbaum, A.R.; Donofrio, P.D.; Walker, F.; Troost, B.T. Laxative abuse causing hypermagnesemia, quadriparesis, and neuromuscular junction defect. Neurology 1989, 39, 746. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, H.; Nakamura, K.; Nishida, A.; Kubo, K.; Nakagawa, R.; Sumida, Y. A case of hypermagnesemia accompanied by hypercalcemia induced by a magnesium laxative in a hemodialysis patient. Nephron 1995, 71, 477–478. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Suzuki, H.; Hirai, Y.; Okuzawa, A.; Kayashima, A.; Kubosawa, Y.; Kinoshita, S.; Fujimoto, A.; Nakazato, Y.; Nishizawa, T.; et al. Clinical features of hypermagnesemia in patients with functional constipation taking daily magnesium oxide. J. Clin. Biochem. Nutr. 2019, 65, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Tatsuki, M.; Miyazawa, R.; Tomomasa, T.; Ishige, T.; Nakazawa, T.; Arakawa, H. Serum magnesium concentration in children with functional constipation treated with magnesium oxide. World J. Gastroenterol. 2011, 17, 779–783. [Google Scholar] [CrossRef]
- Zaman, F.; Abreo, K. Severe Hypermagnesemia as a Result of Laxative Use in Renal Insufficiency. South Med. J. 2003, 96, 102–103. [Google Scholar] [CrossRef]
- Bokhari, S.R.; Siriki, R.; Teran, F.J.; Batuman, V. Fatal Hypermagnesemia Due to Laxative Use. Am. J. Med Sci. 2018, 355, 390–395. [Google Scholar] [CrossRef]
- Corbi, G.; Acanfora, D.; Iannuzzi, G.L.; Longobardi, G.; Cacciatore, F.; Furgi, G.; Filippelli, A.; Rengo, G.; Leosco, D.; Ferrara, N. Hypermagnesemia Predicts Mortality in Elderly with Congestive Heart Disease: Relationship with Laxative and Antacid Use. Rejuvenation Res. 2008, 11, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Quigley, E.M.M.; Lacy, B.E.; Lembo, A.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.R.; Moayyedi, P. Efficacy of Prebiotics, Probiotics, and Synbiotics in Irritable Bowel Syndrome and Chronic Idiopathic Constipation: Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2014, 109, 1547–1561. [Google Scholar] [CrossRef] [PubMed]
- Kubota, M.; Ito, K.; Tomimoto, K.; Kanazaki, M.; Tsukiyama, K.; Kubota, A.; Kuroki, H.; Fujita, M.; Vandenplas, Y. Kubota Lactobacillus reuteri DSM 17938 and Magnesium Oxide in Children with Functional Chronic Constipation: A Double-Blind and Randomized Clinical Trial. Nutrition 2020, 12, 225. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Martínez, M.I.; Calabuig-Tolsá, R.; Cauli, O. The effect of probiotics as a treatment for constipation in elderly people: A systematic review. Arch. Gerontol. Geriatr. 2017, 71, 142–149. [Google Scholar] [CrossRef]
- Barbara, G.; Stanghellini, V.; Brandi, G.; Cremon, C.; Di Nardo, G.; De Giorgio, R.; Corinaldesi, R. Interactions Between Commensal Bacteria and Gut Sensorimotor Function in Health and Disease. Am. J. Gastroenterol. 2005, 100, 2560–2568. [Google Scholar] [CrossRef]
- Gerritsen, J.; Timmerman, H.M.; Fuentes, S.; Van Minnen, L.P.; Panneman, H.; Konstantinov, S.R.; Rombouts, F.M.; Gooszen, H.G.; Akkermans, L.M.A.; Smidt, H.; et al. Correlation between Protection against Sepsis by Probiotic Therapy and Stimulation of a Novel Bacterial Phylotype. Appl. Environ. Microbiol. 2011, 77, 7749–7756. [Google Scholar] [CrossRef] [Green Version]
- Parthasarathy, G.; Chen, J.; Chen, X.; Chia, N.; O’Connor, H.M.; Wolf, P.G.; Gaskins, H.R.; Bharucha, A.E. Faculty Opinions recommendation of Relationship between microbiota of the colonic mucosa vs feces and symptoms, colonic transit, and methane production in female patients with chronic constipation. Gastroenterology 2016, 150, 367–379. [Google Scholar] [CrossRef] [Green Version]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.-Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking Long-Term Dietary Patterns with Gut Microbial Enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef] [Green Version]
- Callen, J. Inventor. Magnesia, Medicated, Liquid. USA patent X2952, 4 May 1818. [Google Scholar]
- Wood, H.C. Catharctics. Therapeutics. Its Principles and Practice; Lippincott: New York, NY, USA, 1908. [Google Scholar]
- Constant, F.; Morali, A.; Arnaud, M.J.; Delabroise, A.M.; Thirion, F.; Matisse, N.; Wagner, M.; Dohm, J.P.; Vuillemin, J.L.; Gay, G. Treatment of idiopathic constipation in infants: Comparative and randomized study of two mineral waters (60 cases). J. Pediatr. Gastroenterol. Nutr. 1999, 28, 551. [Google Scholar] [CrossRef]
- Dupont, C.; Campagne, A.; Constant, F. Efficacy and safety of a magnesium sulfate-rich natural mineral water for patients with functional constipation. Clin. Gastroenterol. Hepatol. 2014, 12, 1280–1287. [Google Scholar] [CrossRef] [Green Version]
- Dupont, C.; Constant, F.; Imbert, A.; Hébert, G.; Zourabichvili, O.; Kapel, N. Time to treatment response of a magnesium- and sulphate-rich natural mineral water in functional constipation. Nutrition 2019, 65, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Naumann, J.; Sadaghiani, C.D.; Alt, F.; Huber, R. Effects of Sulfate-Rich Mineral Water on Functional Constipation: A Double-Blind, Randomized, Placebo-Controlled Study. Complement. Med. Res. 2016, 23, 356–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bothe, G.; Coh, A.; Auinger, A. Efficacy and safety of a natural mineral water rich in magnesium and sulphate for bowel function: A double-blind, randomized, placebo-controlled study. Eur. J. Nutr. 2015, 56, 491–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chevallier, M. Sur la source salée de Vittel (Vosges). Bull. Acad. Natl. Med. 1875, 4, 263–264. [Google Scholar]
- Meillière, M.G. Sur les demandes de changement de nom de sources hydro-minérales autorisées, au nom de la Commission de Eaux minérales. Bull. Acad. Natl. Med. 1919, 82, 499. [Google Scholar]
- Heizer, W.D.; Sandler, R.S.; Seal, E.; Murray, S.C.; Busby, M.G.; Schliebe, B.G.; Pusek, S.N. Intestinal effects of sulfate in drinking water on normal human subjects. Dig. Dis. Sci. 1997, 42, 1055–1061. [Google Scholar] [CrossRef]
- WHO. Sulfate in Drinking Water. Background Document for Development of WHO Guidelines for Drinking-water Quality; WHO/SDE/WSH/0304/114; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Florin, T.; Neale, G.; Gibson, G.R.; Christl, S.U.; Cummings, J.H. Metabolism of dietary sulphate: Absorption and excretion in humans. Gut 1991, 32, 766–773. [Google Scholar] [CrossRef] [Green Version]
- Kashyap, P.K.; Peled, R. Polyethylene glycol plus an oral sulfate solution as a bowel cleansing regimen for colon capsule endoscopy: A prospective, single-arm study in healthy volunteers. Ther. Adv. Gastroenterol. 2015, 8, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Sabatier, M.; Grandvuillemin, A.; Kastenmayer, P.; Aeschliman, J.-M.; Bouisset, F.; Arnaud, M.J.; Dumoulin, G.; Berthelot, A. Influence of the consumption pattern of magnesium from magnesium-rich mineral water on magnesium bioavailability. Br. J. Nutr. 2011, 106, 331–334. [Google Scholar] [CrossRef]
- Schuchardt, J.P.; Hahn, A. Intestinal Absorption and Factors Influencing Bioavailability of Magnesium-An Update. Curr. Nutr. Food Sci. 2017, 13, 260–278. [Google Scholar] [CrossRef]
- Lium, R.; Florey, H.W. The action of magnesium sulphate on the intestine of cat. Q. J. Exp. Physiol. Cogn. Med. Sci. 1939, 29, 303–319. [Google Scholar] [CrossRef] [Green Version]
- Harvey, R.; Read, A. Saline purgatives act by releasing cholecystokinin. Lancet 1973, 302, 185–187. [Google Scholar] [CrossRef]
- Izzo, A.A.; Gaginella, T.S.; Mascolo, N.; Capasso, F. Nitric oxide as a mediator of the laxative action of magnesium sulphate. Br. J. Pharmacol. 1994, 113, 228–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikarashi, N.; Mochiduki, T.; Takasaki, A.; Ushiki, T.; Baba, K.; Ishii, M.; Kudo, T.; Ito, K.; Toda, T.; Ochiai, W.; et al. A mechanism by which the osmotic laxative magnesium sulphate increases the intestinal aquaporin 3 expression in HT-29 cells. Life Sci. 2011, 88, 194–200. [Google Scholar] [CrossRef]
- Ikarashi, N.; Kon, R.; Sugiyama, K. Aquaporins in the Colon as a New Therapeutic Target in Diarrhea and Constipation. Int. J. Mol. Sci. 2016, 17, 1172. [Google Scholar] [CrossRef]
- Vu, M.K.; Nouwens, M.A.; Biemond, I.; Lamers, C.B.; Masclee, A.A. The osmotic laxative magnesium sulphate activates the ileal brake. Aliment. Pharmacol. Ther. 2000, 14, 587–595. [Google Scholar] [CrossRef] [Green Version]
- Adewoye, E.O.; Ige, A.O. Effect of magnesium on gastrointestinal transit time in normal and diabetic rats: Possible mechanism of action. Afr. J. Med. Med Sci. 2012, 41, 373–378. [Google Scholar]
- Uberti, F.; Morsanuto, V.; Ruga, S.; Galla, R.; Farghali, M.; Notte, F.; Bozzo, C.; Magnani, C.; Nardone, A.; Molinari, C. Study of Magnesium Formulations on Intestinal Cells to Influence Myometrium Cell Relaxation. Nutrition 2020, 12, 573. [Google Scholar] [CrossRef] [Green Version]
- Cuomo, R.; Grasso, R.; Sarnelli, G.; Capuano, G.; Nicolai, E.; Nardone, G.; Pomponi, D.; Budillon, G.; Ierardi, E. Effects of carbonated water on functional dyspepsia and constipation. Eur. J. Gastroenterol. Hepatol. 2002, 14, 991–999. [Google Scholar] [CrossRef]
- Mun, J.-H.; Jun, S.S. Effects of Carbonated Water Intake on Constipation in Elderly Patients Following a Cerebrovascular Accident. J. Korean Acad. Nurs. 2011, 41, 269. [Google Scholar] [CrossRef] [Green Version]
- Spiller, R.C. Problems and challenges in the design of irritable bowel syndrome clinical trials: Experience from published trials. Am. J. Med. 1999, 107, 91–97. [Google Scholar] [CrossRef]
- WHO. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]


{kind=link}
| Criteria |
|---|
| 1. Must include 2 or more of the following: |
| a. Straining during more than 25% of defecations |
| b. Lumpy or hard stools (Bristol Scale 1–2) more than 25% of defecations |
| c. Sensation of incomplete evacuation more than 25% of defecations |
| d. Sensation of anorectal obstruction/blockage more than 25% of defecations |
| e. Manual maneuvers to facilitate more than 25% of defecations (e.g., digital evacuation, support of the pelvic floor) |
| f. Fewer than 3 spontaneous bowel movements per week |
| 2. Loose stools are rarely present without the use of laxatives |
| 3. Insufficient criteria for irritable bowel syndrome |
| Active Compound | Mechanisms of Action | Major Undesirable Effects | |
|---|---|---|---|
| First line recommendations | / | - Lifestyle changes and nutritional-hygienic measures | / |
| Drug treatments | |||
| Bulk laxatives | e.g., psyllium, calcium polycarbophil, bran, methylcellulose | - Increase stool volume due to their high hydrophilic power | - Flatulence and abdominal distension |
| Lubricants | Mineral oils (e.g., paraffin oils) | - Lubricate the intestinal wall | - Anal irritation, lipoid pneumonia if inhaled |
| Emollients | Surfactants (e.g., docusate) | - Increase the stool content in water and lipids | - Nausea, abdominal cramps |
| Stimulant laxatives | e.g., bisacodyl, senna and sodium picosulfate | - Stimulate intestinal motility and increase water secretion | - Abdominal discomfort, nausea, cramps |
| Osmotic laxatives | |||
| Saccharides | Non-digested fermentable sugars (e.g., lactitol, lactulose, mannitol, pentaerythritol and sorbitol) | - Transformed into short chain fatty acids exerting an osmotic effect and acting as prebiotics | - Flatulence, abdominal pain, nausea, vomiting, bloating |
| Polyethylene glycols | 3350, 4000 or 6000 g/mol PEGs | - Do not cross the intestinal barrier and retain water in the intestine | - Nausea, abdominal distension, cramps |
| Magnesium oxide | MgO | - Low intestinal absorption, osmotic effect | - Hypermagnesemia |
| Probiotics | e.g., lactobacilli, bifidobacteria | - Probably modification of the gut microbiota and production of short chain fatty acids | Not reported |
| Author, Year (Ref) | Design | Treatment | Comparator | Primary Endpoint | Outcome |
|---|---|---|---|---|---|
| Dupont et al. 2014 [32] | RCT, 244 participants (100% females), Rome III criteria | Hépar 0.5 or 1 L/day | Low mineral natural water (400 mg/L) | Response to the treatment: ≥4 stools/week or an increase of ≥2 stools per week AND <25% lumpy or hard stools | - Increased response rate with 1 L/day Hépar vs. placebo: +16.4% at week 2 (p = 0.013) +14.7% at week 4 (p = 0.028) |
| Naumann et al. 2016 [34] | RCT, 100 participants (85% female), Rome III criteria with 2–4 bowel movements/week and ≥ 1 L/day water | Ensinger Schiller Quelle 4 × 0.25 L/day | Tap water (108 mg/L) + 2650 mg/L CO2 | Difference in stool frequency | - Increased weekly number of stools at 3 weeks vs. placebo (4.80 vs. 3.82, p = 0.036) |
| Bothe et al. 2017 [35] | RCT, 75 participants (84% females), Rome III criteria with 2–4 bowel movements/week and ≥ 0.3 L/day water | Donat MG 0.5 L/day | Low mineral natural water (<1000 mg/L) + 3500 mg/L CO2 | Difference in complete spontaneous bowel movement | - Increased weekly bowel movements vs. placebo: at 3 weeks 6.14 vs. 4.45, p = 0.006 at 6 weeks 6.62 vs. 4.47, p = 0.001. |
| Dupont et al. 2019 [33] | RCT, 226 participants (100% females), Rome III criteria | Hépar 1 L/day | Low mineral natural water (400 mg/L) | Response to the treatment: ≥4 stools/week or an increase of ≥2 stools per week AND <25% lumpy or hard stools | - Increased response rate vs. placebo at 2 weeks: +21.1% responders (p = 0.001) Response reached in a mean of 6.4 ± 0.6 days (p = 0.013 vs. placebo) |
| Hépar [32,33] | ESQ [34] | Donat Mg [35] | |
|---|---|---|---|
| Minerals | 2513 | 2666 | 13000 |
| Magnesium (Mg2+) | 119 | 105 | 1000 |
| Sulfate (SO42-) | 1530 | 1535 | 2000 |
| Calcium (Ca2+) | 549 | 573 | 370 |
| Carbonates (HCO3-) | 383.7 | 347 | 7600 |
| Sodium (Na+) | 14.2 | 28.9 | 1600 |
| Potassium (K+) | 4.1 | 7.34 | / |
| Nitrates (NO3-) | 4.3 | 2.7 | / |
| Chloride (Cl-) | 18.8 | 31.4 | / |
| Carbon dioxide (CO2) | / | 2650 | 3800 |
| Molar Mass | 0.5 L Hépar [32] | 0.3 L Donat Mg [35] | 1 L ESQ [34] | 1 L Hépar [32,33] | 0.5 L Donat Mg [35] | |
|---|---|---|---|---|---|---|
| Mg2+ | 24 g/Mol | 2.48 | 12.50 | 4.38 | 4.96 | 20.83 |
| SO42− | 96 g/Mol | 7.97 | 6.25 | 15.99 | 15.94 | 10.42 |
| Total | 10.45 | 18.75 | 20.37 | 20.90 | 31.25 | |
| Efficacy * | - | - | + | + | + |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dupont, C.; Hébert, G. Magnesium Sulfate-Rich Natural Mineral Waters in the Treatment of Functional Constipation–A Review. Nutrients 2020, 12, 2052. https://doi.org/10.3390/nu12072052
Dupont C, Hébert G. Magnesium Sulfate-Rich Natural Mineral Waters in the Treatment of Functional Constipation–A Review. Nutrients. 2020; 12(7):2052. https://doi.org/10.3390/nu12072052
Chicago/Turabian StyleDupont, Christophe, and Guillaume Hébert. 2020. "Magnesium Sulfate-Rich Natural Mineral Waters in the Treatment of Functional Constipation–A Review" Nutrients 12, no. 7: 2052. https://doi.org/10.3390/nu12072052
APA StyleDupont, C., & Hébert, G. (2020). Magnesium Sulfate-Rich Natural Mineral Waters in the Treatment of Functional Constipation–A Review. Nutrients, 12(7), 2052. https://doi.org/10.3390/nu12072052