To Wean or Not to Wean: The Role of Autologous Reconstructive Surgery in the Natural History of Pediatric Short Bowel Syndrome on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP)

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
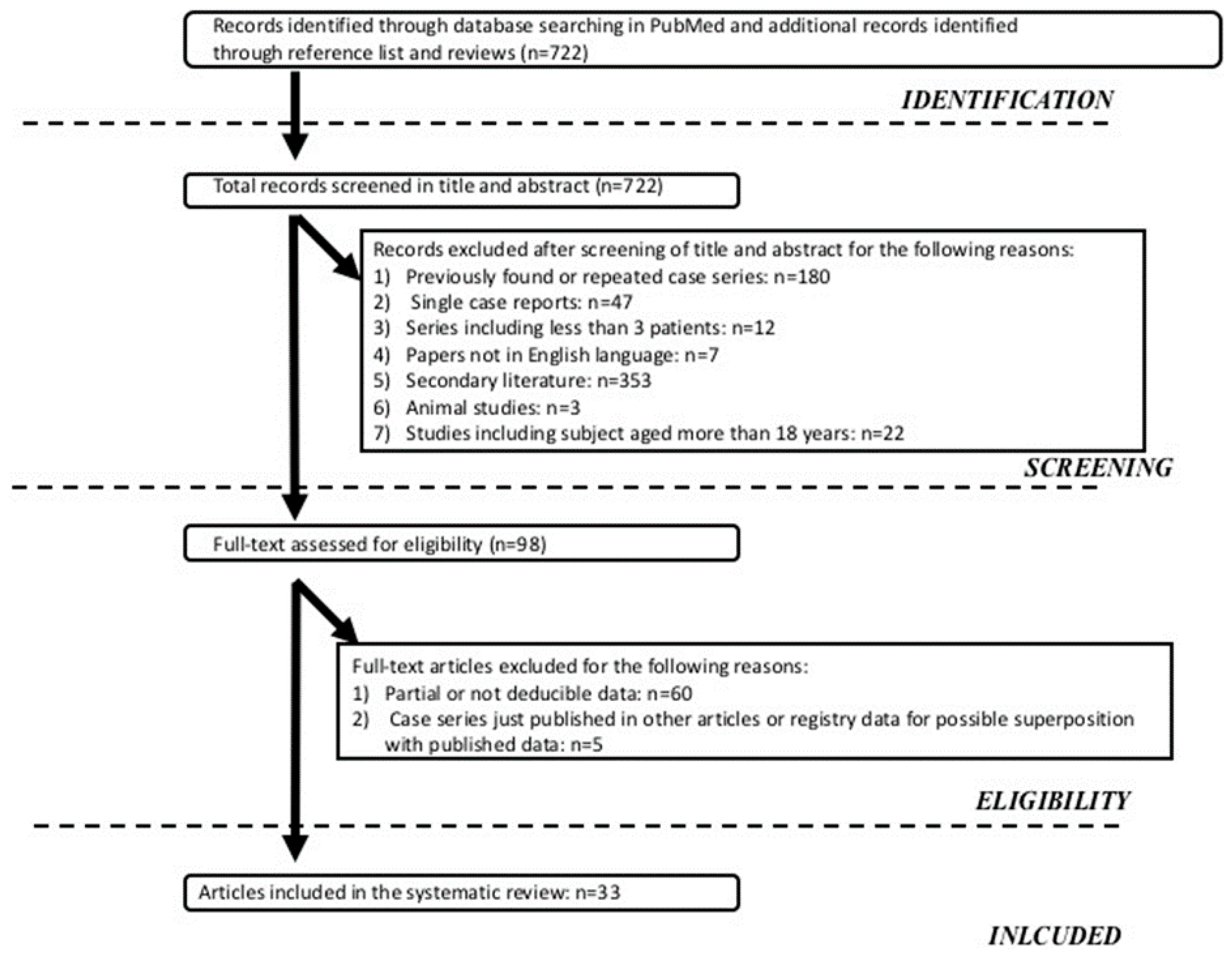
2.1. Literature Search Strategy
2.2. Eligibility Criteria and Study Selection
- SBS acquired at neonatal age;
- SBS patients PN-dependent at inclusion;
- Follow-up length: 1–5 years;
- Follow up beginning before 2000;
- Lack of reference to the weaning off PN trend.
- Single cases or case series with less than three patients;
- Patients treated with known intestinal growth factors, such as Glucagon-like peptide 2, Glucagon-like peptide 1, insulin, glutamine and Growth hormone;
- Secondary literature (review, editorial, position paper, guidelines).
- The primary outcome was the prevalence of weaning off PN, compared between Groups 1 and 2 and between a subset of patients in Groups 1 and 2, aged <24 months and ≥24 months
- Secondary outcomes were survival, Tx and LD.
2.3. Data Extraction, Synthesis and Analysis
3. Results
3.1. Summary of the Series Including Patients Treated with PN + AGIR
3.2. Summary of the Series Including Patients Treated with PN Alone
3.3. Summary of the Patients Characteristics
3.3.1. Univariate Analysis
3.3.2. Logistic Binary for PN Alone/AGIR and PN Alone/STEP
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Diamanti, A.; Capriati, T.; Gandullia, P.; Di Leo, G.; Lezo, A.; Lacitignola, L.; Spagnuolo, M.I.; Gatti, S.; D’Antiga, L.; Verlato, G.; et al. Pediatric Chronic Intestinal Failure in Italy: Report from the 2016 Survey on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients 2017, 9, 1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goulet, O.; Ruemmele, F.; Lacaille, F.; Colomb, V. Irreversible intestinal failure. J. Pediatric Gastroenterol. Nutr. 2004, 38, 250–269. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.; Floyd, T.F.; Ross, A.J., III; Bishop, H.C.; Templeton, J.M., Jr.; Ziegler, M.M. Morbidity and mortality of short bowel syndrome acquired in infancy: An update. J. Pediatric Surg. 1984, 19, 711–717. [Google Scholar] [CrossRef]
- Tappenden, K.A. Mechanisms of enteral nutrient-enhanced intestinal adaptation. Gastroenterology 2006, 130, S93–S99. [Google Scholar] [CrossRef]
- Thompson, J.S.; Quigley, E.M.; Adrian, T.E. Factors affecting outcome following proximal and distal intestinal resection in the dog: An examination of the relative roles of mucosal adaptation, motility, luminal factors, and enteric peptides. Dig. Dis. Sci. 1999, 44, 63–74. [Google Scholar] [CrossRef]
- Schmidt, T.; Pfeiffer, A.; Hackelsberger, N.; Widmer, R.; Meisel, C.; Kaess, H. Effect of intestinal resection on human small bowel motility. Gut 1996, 38, 859–863. [Google Scholar] [CrossRef]
- Dowling, R.H. Intestinal adaptation. N. Engl. J. Med. 1973, 288, 520–521. [Google Scholar] [CrossRef]
- Weaver, L.T.; Austin, S.; Cole, T.J. Small intestinal length: A factor essential for gut adaptation. Gut 1991, 32, 1321–1323. [Google Scholar] [CrossRef]
- DiBaise, J.K.; Young, R.J.; Vanderhoof, J.A. Intestinal rehabilitation and the short bowel syndrome: Part 2. Am. J. Gastroenterol. 2004, 99, 1823–1832. [Google Scholar] [CrossRef]
- Husebye, E. The patterns of small bowel dismotility: Physiology and implication in organic disease and functional desorders. Neurogastroenterol. Motil. 1999, 11, 141–161. [Google Scholar] [CrossRef]
- Cole, C.R.; Zigler, T.R. Small bowel bacterial overgrowth: A negative factor in gut adaptation in pediatric SBS. Curr. Gastroenterol. Rep. 2007, 9, 456–462. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, S.J. Bacterial overgrowth and liver complications in short bowel intestinal failure patients. Gastroenterology 2006, 130, S67–S69. [Google Scholar] [CrossRef]
- Willis, T.C.; Carter, B.A.; Rogers, S.P.; Hawthorne, K.M.; Hicks, P.D.; Abrahms, S.A. High rates of mortality and morbidity occur in infants with parenteral nutrition- associated cholestasis. JPEN 2010, 34, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; De Silva, N.T.; Stanojevic, S.; Avitzur, Y.; Bayoumi, A.M.; Ungar, W.J.; Hoch, J.S.; Wales, P.W. Change of Outcomes in Pediatric Intestinal Failure: Use of Time-Series Analysis to Assess the Evolution of an Intestinal Rehabilitation Program. J. Am. Coll. Surg. 2016, 222, 1180–1188. [Google Scholar] [CrossRef] [PubMed]
- Billiauws, L.; Joly, F. Emerging treatments for short bowel syndrome in adult patients. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Diamond, I.R.; de Silva, N.; Pencharz, P.B.; Kim, J.H.; Wales, P.W. Neonatal short bowel syndrome outcomes after the establishment of the first Canadian multidisciplinary intestinal rehabilitation program: Preliminary experience. J. Pediatric Surg. 2007, 42, 806–811. [Google Scholar] [CrossRef]
- Pakarinen, M.P.; Pakkasjärvi, N.; Merras-Salmio, L.; Koivusalo, A.; Rintala, R. Intestinal rehabilitation of infantile onset very short bowel syndrome. J. Pediatric Surg. 2015, 50, 289–292. [Google Scholar] [CrossRef]
- Infantino, B.J.; Mercer, D.F.; Hobson, B.D.; Fischer, R.T.; Gerhardt, B.K.; Grant, W.J.; Langnas, A.N.; Quiros-Tejeira, R.E. Successful Rehabilitation in Pediatric Ultrashort Small Bowel Syndrome. J. Pediatric 2013, 163, 1361–1366. [Google Scholar] [CrossRef]
- Stanger, J.D.; Oliveira, C.; Blackmore, C.; Avitzur, Y.; Wales, P.W. The impact of multi-disciplinary intestinal rehabilitation programs on the outcome of pediatric patients with intestinal failure: A systematic review and meta-analysis. J. Pediatric Surg. 2013, 48, 983–992. [Google Scholar] [CrossRef]
- Spencer, A.U.; Kovacevich, D.; McKinney-Barnett, M.; Hair, D.; Canham, J.; Maksym, C.; Teitelbaum, D.H. Pediatric short-bowel syndrome: The cost of comprehensive care. Am. J. Clin. Nutr. 2008, 88, 1552–1559. [Google Scholar] [CrossRef] [Green Version]
- Sigalet, D.; Boctor, D.; Robertson, M.; Lam, V.; Brindle, M.; Sarkhosh, K.; Driedger, L.; Sajedi, M. Improved outcomes in pediatric intestinal failure with aggressive prevention of liver disease. Eur. J. Pediatric Surg. 2009, 19, 348–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti, A.; Capriati, T.; Elia, D. Recent Advances in Nutritional Care of Patients with Intestinal Failure. In Current Concepts of Intestinal Failure; Springer: Cham, Switzerland, 2016; pp. 63–77. [Google Scholar]
- Wilmore, D.W.; Byrne, T.A.; Persinger, R.L. Short bowel syndrome: New therapeutic approaches. Curr. Probl. Surg. 1997, 34, 389–444. [Google Scholar] [CrossRef]
- Bianchi, A. From the cradle to enteral autonomy: The role of autologous gastrointestinal reconstruction. Gastroenterology 2006, 130, S138–S146. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A. Intestinal loop lengthening a technique for increasing small intestinal length. J. Ped. Surg. 1980, 15, 145–151. [Google Scholar] [CrossRef]
- Kim, H.B.; Fauza, D.; Garza, J.; Oh, J.T.; Nurko, S.; Jaksic, T. Serial transverse enteroplasty (STEP): A novel bowel lengthening procedure. J. Pediatric Surg. 2003, 38, 425–429. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.; Sudan, D. Intestinal lengthening for short bowel syndrome. Adv. Surg. 2008, 42, 49–61. [Google Scholar] [CrossRef]
- Cserni, T.; Biszku, B.; Guthy, I.; Dicso, F.; Szaloki, L.; Folaranmi, S.; Murphy, F.; Rakoczy, G.; Bianchi, A.; Morabito, A. The First Clinical Application of the Spiral Intestinal Lengthening and Tailoring (Silt) in Extreme Short Bowel Syndrome. J. Gastrointest. Surg. 2014, 18, 1852–1857. [Google Scholar] [CrossRef]
- Beyer-Berjot, L.; Joly, F.; Maggiori, L.; Corcos, O.; Bouhnik, Y.; Bretagnol, F.; Panis, Y. Segmental reversal of the small bowel can end permanent parenteral nutrition dependency: An experience of 38 adults with short bowel syndrome. Ann. Surg. 2012, 256, 739–745. [Google Scholar] [CrossRef]
- Belza, C.; Fitzgerald, K.; de Silva, N.; Avitzur, Y.; Steinberg, K.; Courtney-Martin, G.; Wales, P.W. Predicting Intestinal Adaptation in Pediatric Intestinal Failure A Retrospective Cohort Study. Ann. Surg. 2019, 269, 988–993. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 62, 1006–1012. [Google Scholar]
- Capriati, T.; Giorgio, D.; Fusaro, F.; Candusso, M.; Schingo, P.; Caldaro, T.; Laureti, F.; Elia, D.; Diamanti, A. Pediatric Short Bowel Syndrome: Predicting Four-Year Outcome after Massive Neonatal Resection. Eur. J. Pediatric Surg. 2018, 28, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.K.; Davies, N.; Smyth, E.; Heather, N.; Cole, C.; Keys, S.C.; Beattie, R.M.; Batra, A. Intestinal failure: The evolving demographic and patient outcomes on home parenteral nutrition. Acta Paediatr. 2018, 107, 2207–2211. [Google Scholar] [CrossRef]
- Lakananurak, N. Risk factors for parenteral nutrition-dependence and mortality with the short bowel syndrome: A 10-year retrospective study in Thailand. Asia Pac. J. Clin. Nutr. 2018, 27, 770–776. [Google Scholar]
- Chiba, M.; Sanada, Y.; Toki, A. Markers of enteral adaptation in pediatric short bowel syndrome. Pediatrics Int. 2017, 59, 911–916. [Google Scholar] [CrossRef]
- Hukkinen, M.; Kivisaari, R.; Merras-Salmio, L.; Koivusalo, A.; Pakarinen, M.P. Small Bowel Dilatation Predicts Prolonged Parenteral Nutrition and Decreased Survival in Pediatric Short Bowel Syndrome. Ann. Surg. 2017, 266, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Nader, E.A.; Lambe, C.; Talbotec, C.; Pigneur, B.; Lacaille, F.; Garnier-Lengliné, H.; Petit, L.M.; Poisson, C.; Rocha, A.; Corriol, O.; et al. Outcome of home parenteral nutrition in 251 children over a 14-y period: Report of a single center. Am. J. Clin. Nutr. 2016, 103, 1327–1336. [Google Scholar] [CrossRef] [Green Version]
- Ives, G.C.; Demehri, F.R.; Sanchez, R.; Barrett, M.; Gadepalli, S.; Teitelbaum, D.H. Small Bowel Diameter in Short Bowel Syndrome as a Predictive Factor for Achieving Enteral Autonomy. J. Pediatric 2016, 178, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Petit, L.M.; Girard, D.; Ganousse-Mazeron, S.; Talbotec, C.; Pigneur, B.; Elie, C.; Corriol, O.; Poisson, C.; Goulet, O.; Colomb, V. Weaning Off Prognosis Factors of Home Parenteral Nutrition for Children With Primary Digestive Disease. JPGN 2016, 62, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Schurink, M.; Hulscher, J.B.F.; Nieuwenhuijs, V.B.; Heineman, E.; Rings, E.H.H.M. A Surgical Perspective of the Outcome of a Multidisciplinary Intestinal Rehabilitation Program for Children with Short Bowel Syndrome in the Netherlands. Transplant. Proc. 2014, 46, 2102–2108. [Google Scholar] [CrossRef]
- Nusinovich, Y.; Revenis, M.; Torres, C. Long-term Outcomes for Infants with Intestinal Atresia Studied at Children’s National Medical Center. JPGN 2013, 57, 324–329. [Google Scholar]
- Bailly-Botuha, C.; Colomb, V.; Thioulouse, E.; Berthe, M.C.; Garcette, K.; Dubern, B.; Goulet, O.; Couderc, R.; Girardet, J.P. Plasma Citrulline Concentration Reflects Enterocyte Mass in Children With Short Bowel Syndrome. Pediatric Res. 2009, 65, 559–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvia, G.; Guarino, A.; Terrin, G.; Cascioli, C.; Paludetto, R.; Indrio, F.; Lega, L.; Fanaro, S.; Stronati, M.; Corvaglia, L.; et al. For The Working Group on Neonatal Gastroenterology of the Italian Society of Pediatric Gastroenterology, HepatologyAnd Nutrition (Sigenp). Neonatal Onset Intestinal Failure: An Italian Multicenter Study. J. Pediatric 2008, 153, 674–676. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, K.; Muto, M.; Belza, C.; De Silva, N.; Avitzur, Y.; Wales, P.W. The evolution of the serial transverse enteroplasty for pediatric short bowel syndrome at a single institution. J. Pediatric Surg. 2019, 54, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.A.; Petrosyan, M.; Franklin, A.L.; Chahine, A.A.; Torres, C.; Sandler, A.D. Autologous intestinal reconstruction: A single institution study of the serial transverse enteroplasty (STEP) and the longitudinal intestinal lengthening and tailoring (LILT). Pediatric Surg. Int. 2019, 35, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Mutanen, A.; Barrett, M.; Feng, Y.; Lohi, J.; Rabah, R.; Teitelbaum, D.H.; Pakarinen, M.P. Short bowel mucosalmorphology, proliferation and inflammation at first hand repeat STEP procedures. J. Pediatric Surg. 2019, 54, 511–516. [Google Scholar] [CrossRef] [Green Version]
- Pederiva, F.; Sgrò, A.; Coletta, R.; Khalil, B.; Morabito, A. Outcomes in patients with short bowel syndrome after autologous intestinal reconstruction: Does etiology matter? J. Pediatric Surg. 2018, 53, 1345–1350. [Google Scholar] [CrossRef]
- Coletta, R.; Aldeiri, B.; Morabito, A. Institutional Experience with Spiral Intestinal Lengthening and Tailoring. Eur. J. Pediatric Surg. 2019, 29, 412–416. [Google Scholar] [CrossRef]
- Barrett, M.; Demehri, F.R.; Ives, G.C.; Schaedig, K.; Arnold, M.A.; Teitelbaum, D.H. Taking a STEP back: Assessing the outcomes of multiple STEP procedures. J. Pediatric Surg. 2017, 53, 69–73. [Google Scholar] [CrossRef]
- Wester, T.; Lilja, H.E.; Stenström, P.; Pakarinen, M. Absent ileocecal valve predicts the need for repeated step in children. Surgery 2017, 161, 818–822. [Google Scholar] [CrossRef] [Green Version]
- Bueno, J.; Redecillas, S.; GarcÍa, L.; Lara, A.; Giné, C.; Molino, J.A.; Broto, J.; Segarra, O. Duodenal lengthening in short bowel with dilated duodenum. J. Pediatric Surg. 2015, 50, 493–496. [Google Scholar] [CrossRef]
- Oh, P.S.; Fingeret, A.L.; Shah, M.Y.; Ventura, K.A.; Brodlie, S.; Ovchinsky, N.; Martinez, M.; Lobritto, S.J.; Cowles, R.A. Improved tolerance for enteral nutrition after serial transverse enteroplasty (STEP) in infants and children with short bowel syndrome—A seven-year single-center experience. J. Pediatric Surg. 2014, 49, 1589–1592. [Google Scholar] [CrossRef] [PubMed]
- Mercer, D.F.; Hobson, B.D.; Gerhardt, B.K.; Grant, W.J.; Vargas, L.M.; Langnas, A.N.; Quiros-Tejeira, R.E. Serial Transverse Enteroplasty Allows Children with Short Bowel to Wean from Parenteral Nutrition. J. Pediatric 2014, 164, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Javid, P.J.; Sanchez, S.E.; Horslen, S.P.; Healey, P.J. Intestinal lengthening and nutritional outcomes in children with short bowel syndrome. Am. J. Surg. 2013, 205, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Wales, P.W.; Jancelewicz, T.; Romao, R.L.; Piper, H.G.; De Silva, N.T.; Avitzur, Y. Delayed primary serial transverse enteroplasty as a novel management strategy for infants with congenital ultra-short bowel syndrome. J. Pediatric Surg. 2013, 48, 993–999. [Google Scholar] [CrossRef]
- Almond, S.L.; Haveliwala, Z.; Khalil, B.; Morabito, A. Autologous Intestinal Reconstructive Surgery to Reduce Bowel Dilatation Improves Intestinal Adaptation in Children With Short Bowel Syndrome. JPGN 2013, 56, 631–634. [Google Scholar] [CrossRef]
- Kang, K.H.J.; Gutierrez, I.M.; Zurakowski, D.; DiPerna, S.; Buonomo, C.; Kim, H.B.; Jaksic, T. Bowel re-dilation following serial transverse enteroplasty (STEP). Pediatric Surg. Int. 2012, 28, 1189–1193. [Google Scholar] [CrossRef]
- Leung, M.W.; Chan, I.H.; Chao, N.S.; Wong, B.P.; Liu, K.K. Serial transverse enteroplasty for short bowel syndrome: Hong Kong experience. Hong Kong Med. J. 2012, 18, 35–39. [Google Scholar]
- Lourenço, L.; Campos, M.; Monteiro, J.; Trindade, E.; Dias, J.A.; Guerra, A.; Guerra, P.; Correia-Pinto, J.; Estevão-Costa, J. Serial transverse enteroplasty (STEP): Intermediate outcomes in children with short bowel syndrome. Eur. J. Pediatric 2012, 171, 1265–1268. [Google Scholar] [CrossRef]
- Ching, Y.A.; Fitzgibbons, S.; Valim, C.; Zhou, J.; Duggan, C.; Jaksic, T.; Kim, H.B. Long-term nutritional and clinical outcomes after serial transverse enteroplasty at a single institution. J. Pediatric Surg. 2009, 44, 939–943. [Google Scholar] [CrossRef] [Green Version]
- Wales, P.W.; de Silva, N.; Langer, J.C.; Fecteau, A. Intermediate outcomes after serial transverse enteroplasty in children with short bowel syndrome. J. Pediatric Surg. 2007, 42, 1804–1810. [Google Scholar] [CrossRef]
- Duggan, C.; Piper, H.; Javid, P.J.; Valim, C.; Collier, S.; Kim, H.B.; Jaksic, T. Growth and Nutritional Status in Infants With Short-Bowel Syndrome After the Serial Transverse Enteroplasty Procedure. Clin. Gastroenterol. Hepatol. 2006, 4, 1237–1241. [Google Scholar] [CrossRef]
- Phillips, J.D.; Raval, M.V.; Redden, C.; Weiner, T.M. Gastroschisis, atresia, dysmotility: Surgical treatment strategies for a distinct clinical entity. J. Pediatric Surg. 2008, 43, 2208. [Google Scholar] [CrossRef] [PubMed]
- Srinathan, S.K.; Langer, J.C.; Blennerhassett, M.G.; Harrison, M.R.; Pelletier, G.J.; Lagunoff, D. Etiology of intestinal damage in gastroschisis. III: Morphometric analysis of the smooth muscle and submucosa. J. Pediatric Surg. 1995, 30, 379–383. [Google Scholar] [CrossRef]
- Gabella, G. Hypertrophy of intestinal smooth muscle. Cell Tissue Res. 1975, 163, 199–214. [Google Scholar] [CrossRef]
- Auber, F.; Danzer, E.; Noché-Monnery, M.E.; Sarnacki, S.; Trugnan, G.; Boudjemaa, S.; Audry, G. Enteric nervous system impairment in gastroschisis. Eur. J. Pediatric Surg. 2013, 23, 29–38. [Google Scholar] [PubMed] [Green Version]
- Jones, B.A.; Hull, M.A.; Potanos, K.M.; Zurakowski, D.; Fitzgibbons, S.C.; Ching, Y.A.; Duggan, C.; Jaksic, T.; Kim, H.B.; Registry, I.S.D. Report of 111 consecutive patients enrolled in the International Serial Transverse Enteroplasty (STEP) Data Registry: A retrospectiveobservational study. J. Am. Coll. Surg. 2013, 216, 438–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacaille, F.; Gupte, G.; Colomb, V.; D’Antiga, L.; Hartman, C.; Hojsak, I.; Kolacek, S.; Puntis, J.; Shamir, R. Paper of the ESPGHAN Working Group of Intestinal Failure and Intestinal Transplantation. JPGN 2015, 60, 272–283. [Google Scholar] [PubMed] [Green Version]
- Norsa, L.; Nicastro, E.; Di Giorgio, A.; Lacaille, F.; D’Antiga, L. Prevention and treatment of intestinal failure-associated liver disease in children. Nutrients 2018, 10, 664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celik, N.; Stanley, K.; Rudolph, J.; Al-Issa, F.; Kosmach, B.; Ashokkumar, C.; Sun, Q.; Brown-Bakewell, R.; Zecca, D.; Soltys, K.; et al. Seminar in ped. Improvements in intestinal transplantation. Surgery 2018, 27, 267–272. [Google Scholar]
- Walker, S.R.; Nucci, A.; Yaworski, J.A.; Barksdale, E.M., Jr. The Bianchi procedure: A 20-year single institution experience. J. Pediatric Surg. 2006, 41, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Khalil, B.A.; Ba’ath, M.E.; Aziz, A.; Forsythe, L.; Gozzini, S.; Murphy, F.; Carlson, G.; Bianchi, A.; Morabito, A. Intestinal rehabilitation and bowel reconstructive surgery: Improved outcomes in children with short bowel syndrome. J. Pediatric Gastroenterol. Nutr. 2012, 54, 505–550. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author(Year) | Country | Study-Period | Study Population * | Number of Patients Weaned from PN |
|---|---|---|---|---|
| Belza (2019) | Canada | 2006–2013 | 120 | 84 |
| Capriati (2018) | Italy | 2008–2016 | 19 | 7 |
| Brown (2018) | UK | 2001–2016 | 15 | 4 |
| Lakananurak (2018) | Thailand | 2005–2015 | 19 | 9 |
| Chiba (2017) | Japan | 2000–2015 | 7 | 5 |
| Hukkinen (2017) | Finland | 2002–2015 | 61 | 49 |
| AbiNader (2016) | France | 2000–2013 | 148 | 91 |
| Chester Ives (2016) | USA | 2000–2015 | 29 | 16 |
| Petit (2016) | France | 2000–2009 | 98 | 57 |
| Schurink (2014) | Netherlands | 2001–2009 | 19 | 16 |
| Nusinovich (2012) | USA | 2000–2010 | 20 | 11 |
| Sigalet (2009) | Canada | 2006–2009 | 22 | 18 |
| Bailly-Bouta (2008) | France | 2001–2004 | 31 | 9 |
| Salvia (2008) | Italy | 2003–2004 | 19 | 10 |
| Author (Year) | Country | Period of Study | Study Population | Number of Patients Weaning of PN |
|---|---|---|---|---|
| Fitzgerald (2019) | Canada | 2003–2016 | 36 | 15 |
| Shah (2019) | USA | 2004–2014 | 22 | 11 |
| Mutanen (2019) | Finland | 2003–2014 | 15 | 1 |
| Pederiva (2018) | UK | 2002–2012 | 43 | 25 |
| Coletta (2017) | UK | 2012–2017 | 5 | 0 |
| Barrett 2017) | USA | 2003–2014 | 17 | 6 |
| Wester (2016) | Finland | 2004–2015 | 27 | 16 |
| Bueno (2015) | Spain | 2005–2013 | 3 | 1 |
| Oh (2014) | USA | 2004–2011 | 15 | 5 |
| Mercer (2014) | USA | 2006–2011 | 51 | 24 |
| Javid (2013) | USA | 2004–2011 | 16 | 9 |
| Wales (2013) | Canada | 2009–2011 | 5 | 2 |
| Almond (2013) | UK | 2004–2011 | 8 | 7 |
| Kang (2012) | USA | 2002–2011 | 16 | 8 |
| Leung (2012) | Hong Kong | 2007–2010 | 4 | 1 |
| Lourenco (2012) | Portugal | 2006–2008 | 3 | 2 |
| Ching (2009) | USA | 2002–2008 | 16 | 6 |
| Wales (2007) | Canada | 2003–2006 | 14 | 7 |
| Duggan (2006) | USA | 2002–2014 | 4 | 2 |
| INDICATIONS |
|---|
| Nutritional [52,60,62] Failure to progress EN |
| Digestive [45,49,60,61] At least 10 cm of small bowel+>50% of the colon, dysmotility, vomiting, bacterial overgrowth, obstructive symptoms, increased secretions, IFALD |
| Extra-digestive [49] Fluid and electrolyte problems, D-lactic acidosis, vascular access problems |
| Biochemistry/Imaging based [45] Small bowel > 35 cm + increased bilirubin level + normal INR; small bowel ≥50 cm of bowel+portal hypertension+ hypersplenism ± thrombocytopenia + normal INR |
| Imaging based [48,52,58,61] Gut dilatation, as shown by upper gastrointestinal contrast study with diameter >3.5 cm or >2 vertebral bodies |
| TYPE OF SURGERY |
| STEP [44,45,46,47,49,50,51,52,53,54,55,56,57,58,59,60,61,62], LILT [44,47,57], SILT [48], reverse segment [47], colonic interposition [47], tapering enteroplasty [47,51,56] |
| COMPLICATIONS (in 64/320 Patients) |
| Staple leak [44,61], stricture/obstruction [44,47,52,53,55,58,59,60], bleeding, abdominal adhesions [44,47,54,60], entero-cutaneous fistula [47,52], bowel wall hematoma [52], infections [44,47,48,53,59], intra-abdominal abscess [55], ulcers [54,61], D-lactic acidosis and abdominal distension [48,49,50,51,52,53,54,55,56,57,58,59] |
| PN | PN + AGIR | PN + STEP | p PN vs. Surgery | p PN vs. STEP | |
|---|---|---|---|---|---|
| General Data | |||||
| N° Pts | 627 | 320 | 242 | 0.09 | 0.04 |
| N° studies | 13 | 19 | 15 | / | / |
| Male/Female | 242/176 | 155/126 | 120/91 | 0.06 | 0.06 |
| Follow up (mo) | 53.3 ± 41.3 | 36.2 ± 15.9 | 28.4 ± 11.8 | 0.06 | 0.03 |
| GA | 34.3 ± 0.8 | 34.5 ± 0.9 | 34.1 ± 3.8 | 0.66 | 0.87 |
| <24 mo/≥24 mo | 59/41 | 67/33 | 81/19 | 0.001 | 0.0001 |
| Etiology (%) | |||||
| NEC | 29.5 | 15 | 15 | 0.06 | 0.12 |
| Gastroschisis | 17 | 32.5 | 33 | 0.04 | 0.02 |
| Volvulus | 16.7 | 11.8 | 9 | 0.64 | 0.55 |
| Multiple atresias | 17.3 | 24.6 | 26 | 0.29 | 0.24 |
| Hirshprung | 6.2 | 2.5 | 2.4 | 0.66 | 0.56 |
| Combined | 1.6 | 6.8 | 6.6 | 0.18 | 0.27 |
| Other | 3.9 | 0.3 | 0.4 | 0.04 | 0.04 |
| Residual Bowel Anatomy (%) | |||||
| Length BS | 45.7 ± 20.9 | 50.8 ± 22.6 | 57.2 ± 22.0 | 0.74 | 0.68 |
| Length AS | NA | 80.3 ± 33.5 | 90.3 ± 32.5 | UV | UV |
| ICV+ | 48.5 | 16.5 | 26 | 0.003 | 0.10 |
| Colon>50% | 43.8 | 62.5 | 96.2 | 0.007 | 0.001 |
| Age at surgery | 39.4 ± 56.6 | 22.7 ± 21.3 | UV | UV | |
| Outcomes (%) | |||||
| Weaning off PN | 61.6 | 46.2 | 43 | 0.03 | 0.01 |
| Survival | 91.5 | 95 | 94.2 | 0.72 | 0.82 |
| Tx | 5.4 | 7.5 | 9.5 | 0.24 | 0.045 |
| LD | 30.4 | 12 | 14.3 | 0.001 | 0.001 |
| IFALD | 23.2 | 12 | 14.3 | 0.01 | 0.06 |
| Abnormal LFTs | 33/461 (7.1) | NA | NA | UV | UV |
| <24 Months | ≥24 Months | p NP | p Surgery | |||
|---|---|---|---|---|---|---|
| PN | AGIR | NP | AGIR | |||
| General Data | ||||||
| N° Pts | 284 | 214 | 198 | 106 | / | / |
| N° studies | 8 | 12 | 3 | 7 | / | / |
| M/F | 56/44 | 55/45 | 48/52 | 55/45 | 0.74 | 0.38 |
| Follow up | 41.7 ± 27.4 | 32.1 ± 12.2 | 59.7 ± 23.1 | 36.9 ± 13.2 | 0.06 | 0.09 |
| Age at surgery | 13.6 ± 4.3 | 43.8 ± 28.7 | 0.02 | |||
| Etiology (%) | ||||||
| NEC | 50 | 15 | 22.7 | 14 | 0.004 | 0.42 |
| Gastroschisis | 20 | 38 | 19.1 | 22 | 0.84 | 0.23 |
| Volvulus | 23.1 | 8 | 23.7 | 19 | 0.85 | 0.90 |
| Atresias | 20.4 | 27 | 34 (17.1) | 22 (21) | 0.95 | 0.79 |
| Hirshprung | 33/284 (11.6) | 6 (3) | 25 (12.6) | 2 (2) | 0.77 | 0.15 |
| Combined etiologies | 25/186 (13.4) | 16 (7) | 0 (0) | 6 (6) | / | 0.38 |
| Other | 14/186 (7.5) | 1 (0.4) | 9 (4.5) | 0 (0) | 0.55 | / |
| Residual Bowel Anatomy | ||||||
| Length BS | 51.6 ± 18.6 | 55.8 ± 17.6 | 51.8 ± 2.5 | 45.2 ± 29.9 | 0.87 | 0.45 |
| Length AS | 84.5 ± 33.3 | 76.9 ± 36.9 | / | 0.37 | ||
| ICV+ | 54.8 | 30 | 47.9 | 24 | 0.36 | 0.96 |
| Outcomes | ||||||
| Weaning off PN | 59.5 | 44 | 55.5 | 84 | 0.59 | 0.01 |
| Survival | 79.9 | 95 | 98.5 | 94 | 0.03 | 0.79 |
| Tx | 7.2 | 9 | 5.9 | 4 | 0.48 | 0.50 |
| LD | 1 | 6 | 17.3 | 19 | 0.35 | 0.75 |
| PN vs. AGIR | PN vs. STEP | |||
|---|---|---|---|---|
| Odds Ratio (95% CIs) | p | Odds Ratio (95% CIs) | p | |
| Weaning off PN | 1.1 (1.00–1.17) | 0.03 | 1.13 (1.01, 1.31) | 0.045 |
| Survival | 1.05 (1.01–1.09) | 0.01 | 1.06 (0.99, 1.15) | 0.051 |
| Tx | 1.14 (0.91, 1.44) | 0.27 | 1.17 (0.86, 1.59) | 0.31 |
| LD | 0.40 (0.11, 1.46) | 0.21 | 1.19 (0.90, 1.58) | 0.20 |
| Model 1 * | ||||
| Weaning off PN | 1.08 (1.01, 1.16) | 0.03 | 1.12 (1.01,1.29) | 0.048 |
| Survival | 1.15(0.9, 1.45) | 0.11 | 1.64 (0.64, 2.39) | 0.26 |
| Tx | 1.07 (0.80, 1.44) | 0.51 | 1.01 (0.57, 1.9) | 0.71 |
| LD | 1.24 (0.93, 1,63) | 0.13 | 1.68 (0.61, 3.1) | 0.28 |
| Model 2 ** | ||||
| Weaning off PN | 1.18 (0.82, 1.13) | 0.052 | 1.26 (0.97, 1.64) | 0.07 |
| Survival | 1.04 (0.99, 1.11) | 0.06 | 1.10 (0.98, 1.28) | 0.09 |
| Tx | 0.78 (0.49, 1.21) | 0.26 | 1.21 (0.41, 3.1) | 0.78 |
| LD | 1.31 (0.95, 1.83) | 0.10 | 1.23 (0.89,1.71) | 0.39 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capriati, T.; Mosca, A.; Alterio, T.; Spagnuolo, M.I.; Gandullia, P.; Lezo, A.; Lionetti, P.; D’Antiga, L.; Fusaro, F.; Diamanti, A. To Wean or Not to Wean: The Role of Autologous Reconstructive Surgery in the Natural History of Pediatric Short Bowel Syndrome on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients 2020, 12, 2136. https://doi.org/10.3390/nu12072136
Capriati T, Mosca A, Alterio T, Spagnuolo MI, Gandullia P, Lezo A, Lionetti P, D’Antiga L, Fusaro F, Diamanti A. To Wean or Not to Wean: The Role of Autologous Reconstructive Surgery in the Natural History of Pediatric Short Bowel Syndrome on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients. 2020; 12(7):2136. https://doi.org/10.3390/nu12072136
Chicago/Turabian StyleCapriati, Teresa, Antonella Mosca, Tommaso Alterio, Maria Immacolata Spagnuolo, Paolo Gandullia, Antonella Lezo, Paolo Lionetti, Lorenzo D’Antiga, Fabio Fusaro, and Antonella Diamanti. 2020. "To Wean or Not to Wean: The Role of Autologous Reconstructive Surgery in the Natural History of Pediatric Short Bowel Syndrome on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP)" Nutrients 12, no. 7: 2136. https://doi.org/10.3390/nu12072136
APA StyleCapriati, T., Mosca, A., Alterio, T., Spagnuolo, M. I., Gandullia, P., Lezo, A., Lionetti, P., D’Antiga, L., Fusaro, F., & Diamanti, A. (2020). To Wean or Not to Wean: The Role of Autologous Reconstructive Surgery in the Natural History of Pediatric Short Bowel Syndrome on Behalf of Italian Society for Gastroenterology, Hepatology and Nutrition (SIGENP). Nutrients, 12(7), 2136. https://doi.org/10.3390/nu12072136