Recovery of Saccharomyces cerevisiae CNCM I-3856 in Vaginal Samples of Healthy Women after Oral Administration

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim of the Study
2.2. Population and Ethical Considerations
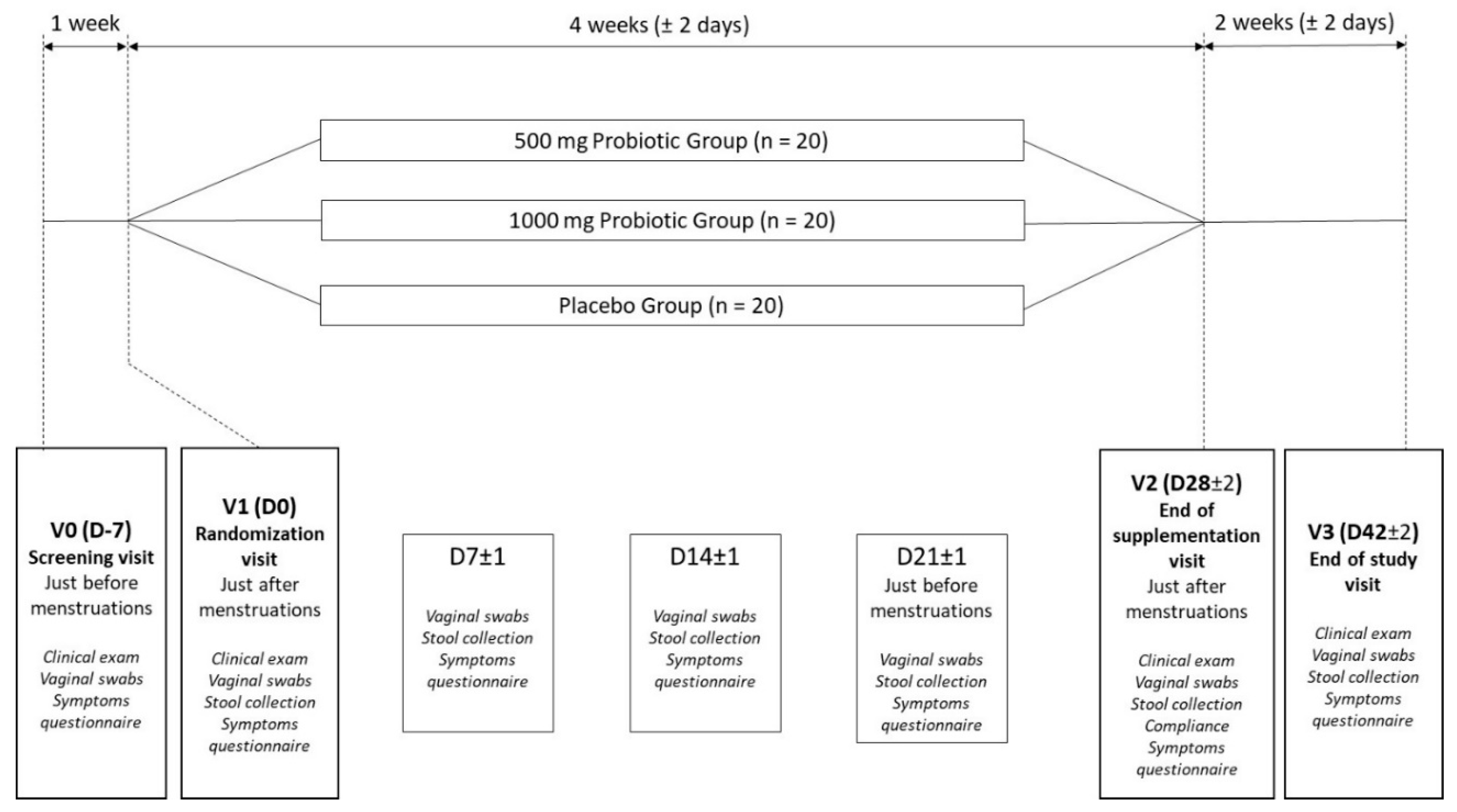
2.3. Design
2.4. Intervention
- -
- 2.5 × 109 colony forming units (CFU) daily in the 500 mg Probiotic group;
- -
- 5 × 109 CFU daily in the 1000 mg Probiotic group.
2.5. Assesment
2.5.1. Study Endpoints
2.5.2. Laboratory Assessments
2.5.3. Safety and Compliance Assessment
2.5.4. Sample Size, Randomization Procedure and Statistical Analysis
- -
- : Value of the parameter at Day Dn;
- -
- Product: Placebo, 500 mg or 1000 mg of S. cerevisiae CNCM I-3856;
- -
- Day Dn (D0 D7 D14 D21 D28 or D 42);
- -
- ε Residuals with covariance structure considering the repeated measurements on the same subject.
- -
- : 1 if the CNCM I 3856 at day Dn in the sphere Sph is present, 0 if absent;
- -
- Dose: 500 mg or 1000 mg of S. cerevisiae CNCM I-3856;
- -
- Day: Day of the study (D7, D14, D21, D28, D42);
- -
- Sphere: Anatomical Sphere Sph (vaginal or intestinal).
3. Results
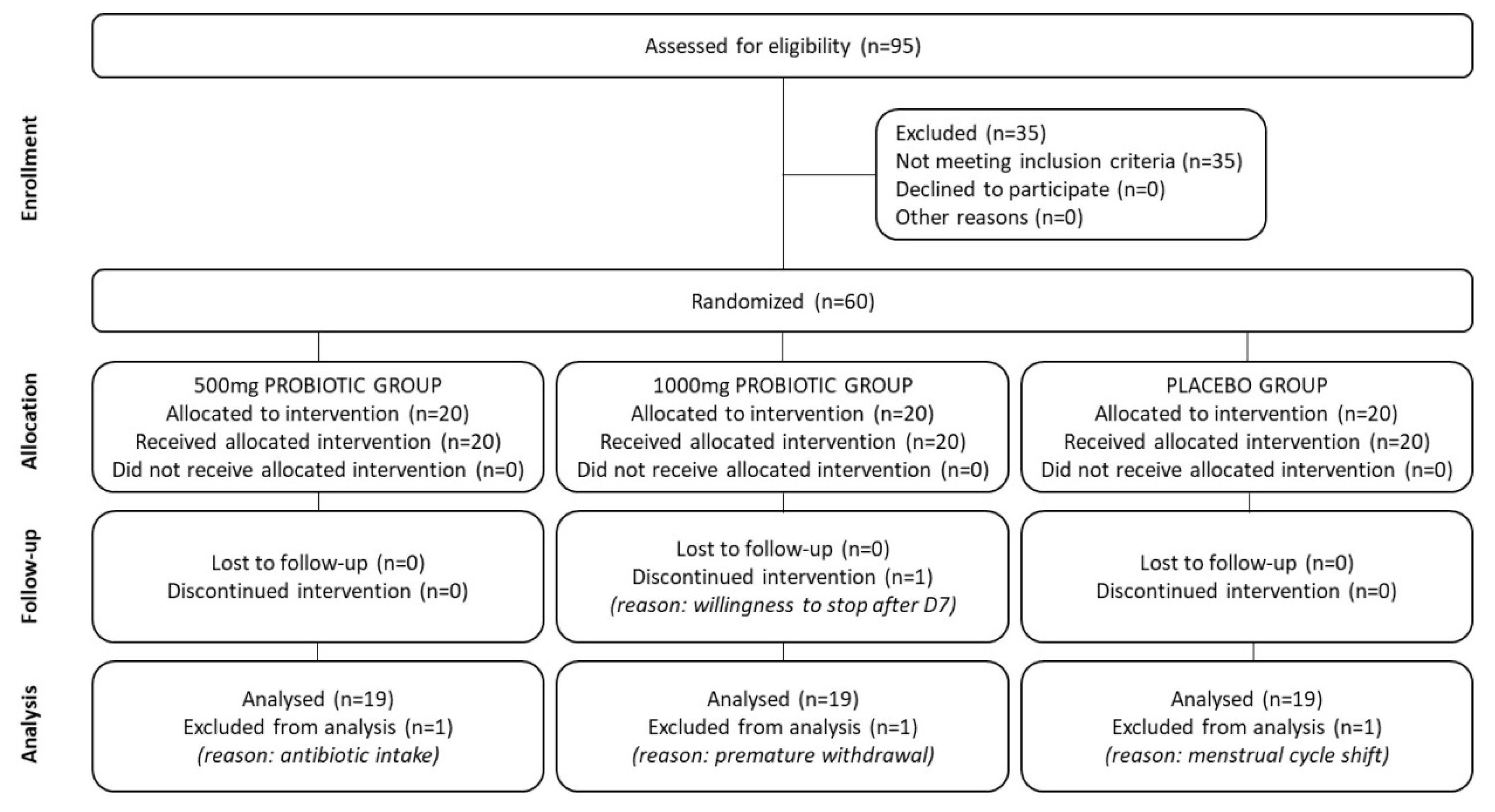
3.1. Study Flowchart and Baseline Characteristics of the Population
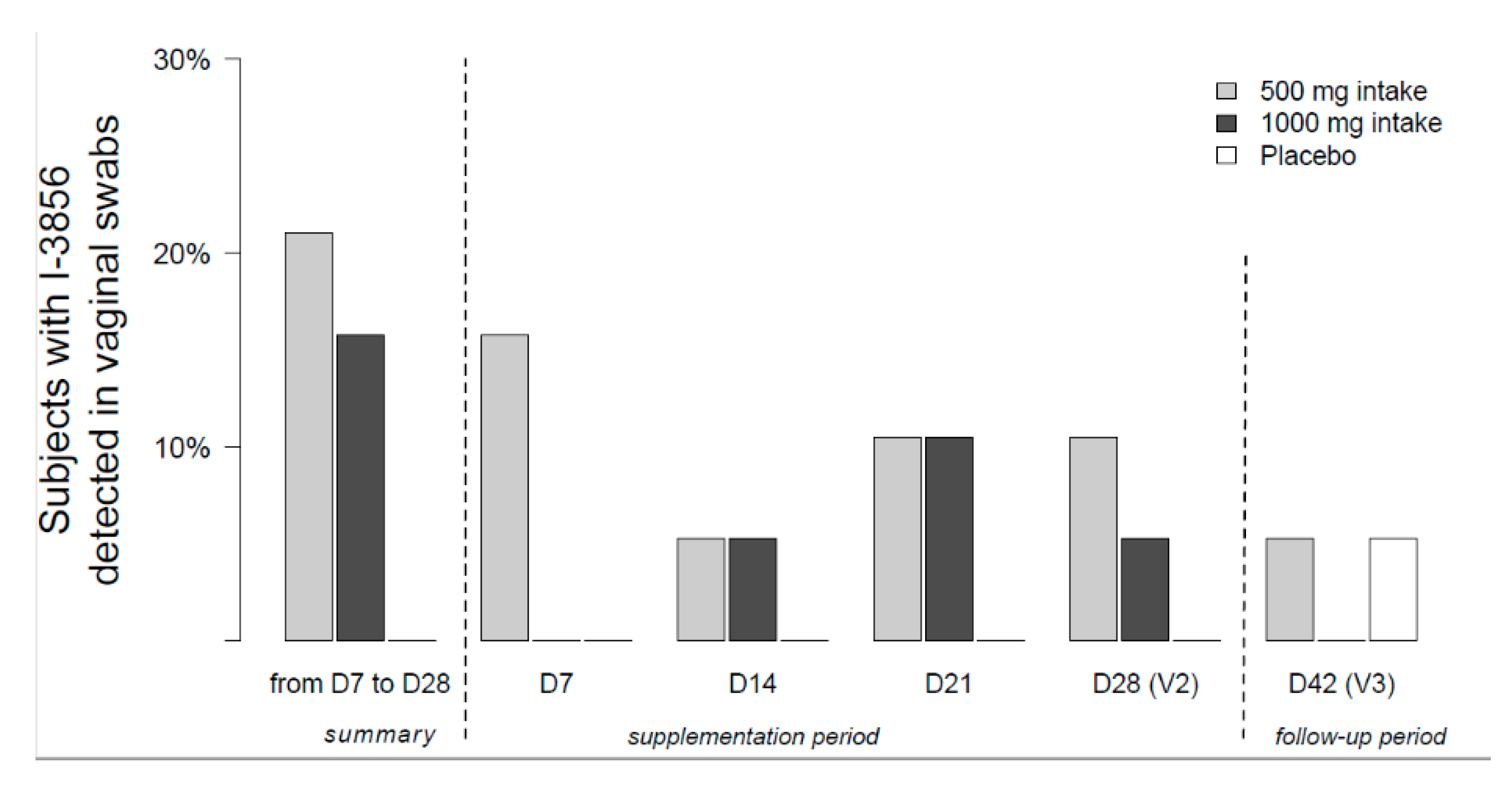
3.2. The Migration of S. cerevisiae CNCM I-3856 from Intestine to Vagina Was Demonstrated
- 500 mg Probiotic group (n = 19): 15.8% at day 7, 5.3% at day 14, 10.5% at day 21 and 10.5% at day 28.
- 1000 mg Probiotic group (n = 19): 0% at day 7, 5.3% at day 14, 10.5% at day 21 and 5.3% at day 28.
3.3. No Significant Impact of S. cerevisiae CNCM I-3856 on the Döderlein Flora Was Found
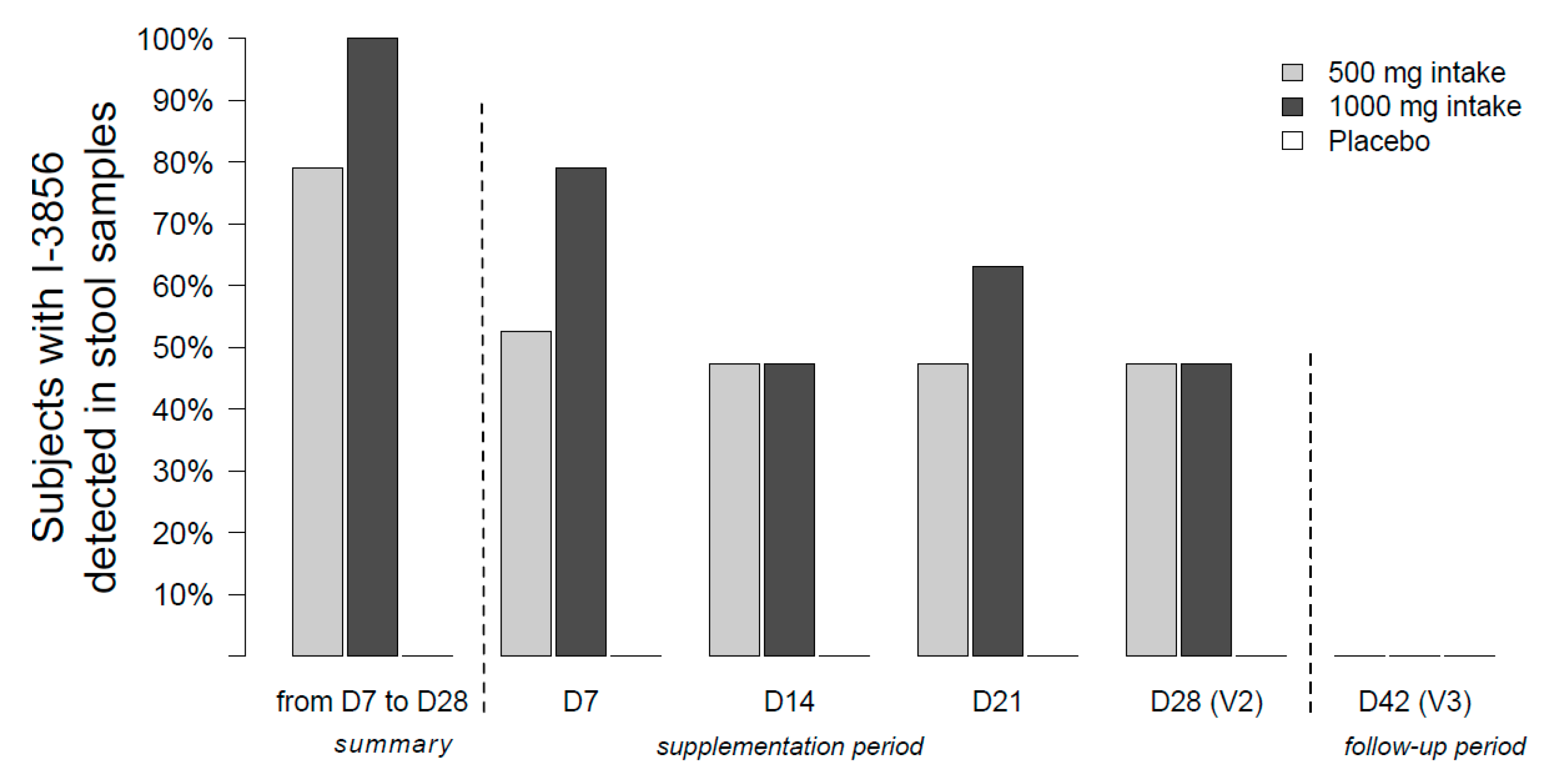
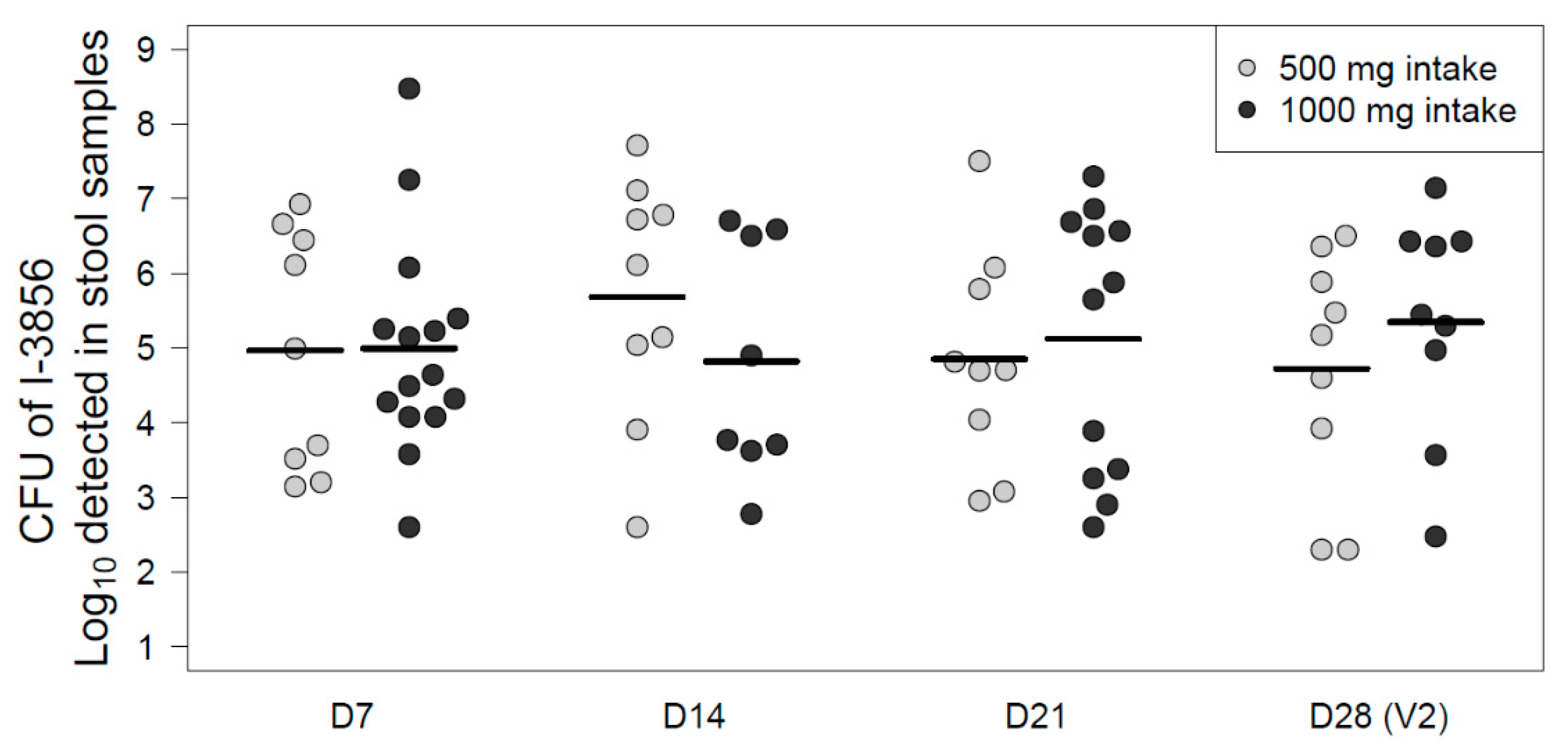
3.4. S. cerevisiae CNCM I-3856 Survived through the Gastrointestinal Tract
3.5. C. albicans Did Not Show Significant Variations in Vaginal Samples
3.6. S. cerevisiae CNCM I-3856 Was Safe and Well Tolerated
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Falagas, M.E.; Betsi, G.I.; Athanasiou, S. Probiotics for prevention of recurrent vulvovaginal candidiasis. J. Antimicrob. Chemother. 2006, 58, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amabebe, E.; Anumba, D.O.C. The Vaginal Microenvironment: The Physiologic Role of Lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, S.; Fredricks, D.N. The human vaginal bacterial biota and bacterial vaginosis. Interdiscip. Perspect. Infect. Dis. 2008, 2008, 750479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Aila, N.A.; Tency, I.; Saerens, B.; de Backer, E.; Cools, P.; Santiago, G.L.d.S.; Verstraelen, H.; Verhelst, R.; Temmerman, M.; Vaneechoutte, M. Strong correspondence in bacterial loads between the vagina and rectum of pregnant women. Res. Microbiol. 2011, 162, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Antonio, M.A.D.; Rabe, L.K.; Hillier, S.L. Colonization of the rectum by Lactobacillus species and decreased risk of bacterial vaginosis. J. Infect. Dis. 2005, 192, 394–398. [Google Scholar] [CrossRef] [Green Version]
- Tempera, G. Vaginal infections: Epidemiology and risk factors. Giornale Italiano di ostetricia e ginecologia 2005, 27, 263–266. [Google Scholar]
- Truter, I. Bacterial vaginosis: Literature review of treatment options with specific emphasis on non-antibiotic treatment. Afr. J. Pharm. Pharmacol. 2013, 7, 3060–3067. [Google Scholar] [CrossRef] [Green Version]
- Guaschino, S.; de Seta, F.; Piccoli, M.; Maso, G.; Alberico, S. Aetiology of preterm labour: Bacterial vaginosis. BJOG 2006, 113 (Suppl. 3), 46–51. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4680–4687. [Google Scholar] [CrossRef] [Green Version]
- Cribby, S.; Taylor, M.; Reid, G. Vaginal microbiota and the use of probiotics. Interdiscip. Perspect. Infect. Dis. 2008, 2008, 256490. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murina, F.; Graziottin, A.; Vicariotto, F.; Seta, F. Can Lactobacillus fermentum LF10 and Lactobacillus acidophilus LA02 in a slow-release vaginal product be useful for prevention of recurrent vulvovaginal candidiasis? A clinical study. J. Clin. Gastroenterol. 2014, 48 (Suppl. 1), S102–S105. [Google Scholar] [CrossRef] [Green Version]
- Kovachev, S.; Dobrevski-Vacheva, R. Effect of Lactobacillus casei var rhamnosus (Gynophilus) in restoring the vaginal flora by female patients with bacterial vaginosis--randomized, open clinical trial. Akush Ginekol 2013, 52 (Suppl. 1), 48–53. [Google Scholar]
- Bohbot, J.M.; Cardot, J.M. Vaginal impact of the oral administration of total freeze-dried culture of LCR 35 in healthy women. Infect. Dis. Obstet. Gynecol. 2012, 2012, 503648. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Bruce, A.W.; Fraser, N.; Heinemann, C.; Owen, J.; Henning, B. Oral probiotics can resolve urogenital infections. FEMS Immunol. Med. Microbiol. 2001, 30, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Yefet, E.; Colodner, R.; Strauss, M.; Letova, Y.G.Z.; Nachum, Z. A Randomized Controlled Open Label Crossover Trial to Study Vaginal Colonization of Orally Administered Lactobacillus Reuteri RC-14 and Rhamnosus GR-1 in Pregnant Women at High Risk for Preterm Labor. Nutrients 2020, 12, 1141. [Google Scholar] [CrossRef] [Green Version]
- Nystatin Multicenter Study Group. Therapy of candida vaginitis: The effect of eliminating intestinal Candida. Am. J. Obstet. Gynecol. 1986, 155, 651–655. [Google Scholar] [CrossRef]
- Barrientos-Durán, A.; Fuentes-López, A.; de Salazar, A.; Plaza-Díaz, J.; García, F. Reviewing the Composition of Vaginal Microbiota: Inclusion of Nutrition and Probiotic Factors in the Maintenance of Eubiosis. Nutrients 2020, 12, 419. [Google Scholar] [CrossRef] [Green Version]
- Lewis, F.M.T.; Bernstein, K.T.; Aral, S.O. Vaginal microbiome and its relationship to behavior, sexual health, and sexually transmitted diseases. Obstet. Gynecol. 2017, 129, 643–654. [Google Scholar] [CrossRef]
- Ma, B.; Forney, L.J.; Ravel, J. Vaginal microbiome: Rethinking health and disease. Annu. Rev. Microbiol. 2012, 66, 371–389. [Google Scholar] [CrossRef] [Green Version]
- O’Hanlon, D.E.; Moench, T.R.; Cone, R.A. In vaginal fluid, bacteria associated with bacterial vaginosis can be suppressed with lactic acid but not hydrogen peroxide. BMC Infect. Dis. 2011, 11, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrielli, E.; Pericolini, E.; Ballet, N.; Roselletti, E.; Sabbatini, S.; Mosci, P.; Decherf, A.C.; Pélerin, F.; Perito, S.; Jüsten, P.; et al. Saccharomyces cerevisiae-based probiotic as novel anti-fungal and anti-inflammatory agent for therapy of vaginal candidiasis. Benef. Microbes 2018, 9, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Pericolini, E.; Gabrielli, E.; Ballet, N.; Sabbatini, S.; Roselletti, E.; Decherf, A.C.; Pélerin, F.; Luciano, E.; Perito, S.; Jüsten, P.; et al. Therapeutic activity of a Saccharomyces cerevisiae-based probiotic and inactivated whole yeast on vaginal candidiasis. Virulence 2017, 8, 74–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabbatini, S.; Monari, C.; Ballet, N.; Mosci, P.; Decherf, A.C.; Pélerin, F.; Perito, S.; Scarpelli, P.; Vecchiarelli, A. Saccharomyces cerevisiae-based probiotic as novel anti-microbial agent for therapy of bacterial vaginosis. Virulence 2018, 9, 954–966. [Google Scholar] [CrossRef] [Green Version]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Nikita, L.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The composition and stability of the vaginal microbiota of normal pregnant women is different from that of non-pregnant women. Microbiome 2014, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Kurtzman, C.P.; Robnett, C.J. Identification of clinically important ascomycetous yeasts based on nucleotide divergence in the 5 end of the large-subunit (26S) ribosomal DNA gene. J. Clin. Microbiol. 1997, 35, 1216–1223. [Google Scholar] [CrossRef] [Green Version]
- Kurtzman, C.P.; Robnett, C.J. Identification and phylogeny of ascomycetous yeasts from analysis of nuclear large subunit (26S) ribosomal DNA partial sequences. Antonie Van Leeuwenhoek 1998, 73, 331–371. [Google Scholar] [CrossRef]
- European Committee for Standardization. Animal Feeding Stuffs, PCR Typing of Probiotic Strains of Saccharomyces cerevisiae (Yeast); CEN/TS 15790: 2008; European Committee for Standardization: Brussels, Berlgium, 2009. [Google Scholar]
- Kusters, J.G.; Reuland, E.A.; Bouter, S.; Koenig, P.; Dorigo-Zetsma, J.W. A multiplex real-time PCR assay for routine diagnosis of bacterial vaginosis. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1779–1785. [Google Scholar] [CrossRef] [Green Version]
- Standardization ECF. Animal Feeding Stuffs: PCR Typing of Probiotic; European Committee for Standardization: Brussels, Berlgium, 2009. [Google Scholar]
- Sim, J.; Lewis, M. The size of a pilot study for a clinical trial should be calculated in relation to considerations of precision and efficiency. J. Clin. Epidemiol. 2012, 65, 301–308. [Google Scholar] [CrossRef]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharmaceut. Statist. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Mezzasalma, V.; Manfrini, E.; Ferri, E.; Boccarusso, M.; Di Gennaro, P.; Schiano, I.; Michelotti, A.; Labra, M. Orally administered multispecies probiotic formulations to prevent uro-genital infections: A randomized placebo-controlled pilot study. Arch. Gynecol. Obstet. 2017, 295, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Russo, R.; Edu, A.; Seta, F. Study on the effects of an oral lactobacilli and lactoferrin complex in women with intermediate vaginal microbiota. Arch. Gynecol. Obstet. 2018, 298, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Morelli, L.; Zonenenschain, D.; Del Piano, M.; Cognein, P. Utilization of the intestinal tract as a delivery system for urogenital probiotics. J. Clin. Gastroenterol. 2004, 38, S107–S110. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Charbonneau, D.; Erb, J.; Kochanowski, B.; Beuerman, D.; Poehner, R.; Bruce, A.W. Oral use of Lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora. FEMS Immunol. Med. Microbiol. 2003, 35, 131–134. [Google Scholar] [CrossRef] [Green Version]
- de Alberti, D.; Russo, R.; Terruzzi, F.; Nobile, V.; Ouwehand, A.C. Lactobacilli vaginal colonisation after oral consumption of Respecta(®) complex: A randomised controlled pilot study. Arch. Gynecol. Obstet. 2015, 292, 861–867. [Google Scholar] [CrossRef]
- Anukam, K.C.; Duru, M.U.; Eze, C.C.; Egharevba, J.; Aiyebelehin, A.; Bruce, A.; Reid, G. Oral use of probiotics as an adjunctive therapy to fluconazole in the treatment of yeast vaginitis: A study of Nigerian women in an outdoor clinic. Microb. Ecol. Health Dis. 2009, 21, 72–77. [Google Scholar]
- Strus, M.; Chmielarczyk, A.; Kochan, P.; Adamski, P.; Chełmicki, Z.; Chełmicki, A.; Pałucha, A.; Heczko, P.B. Studies on the effects of probiotic Lactobacillus mixture given orally on vaginal and rectal colonization and on parameters of vaginal health in women with intermediate vaginal flora. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 163, 210–215. [Google Scholar] [CrossRef]
- Reid, G.; Beuerman, D.; Heinemann, C.; Bruce, A.W. Probiotic Lactobacillus dose required to restore and maintain a normal vaginal flora. FEMS Immunol. Med. Microbiol. 2001, 32, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouwehand, A.C. A review of dose-responses of probiotics in human studies. Benef. Microbes 2017, 8, 143–151. [Google Scholar] [CrossRef]
- Selle, K.; Klaenhammer, T.R. Genomic and phenotypic evidence for probiotic influences of Lactobacillus gasseri on human health. FEMS Microbiol. Rev. 2013, 37, 915–935. [Google Scholar] [CrossRef] [Green Version]
- Elmer, G.W.; McFarland, L.V.; Surawicz, C.M.; Danko, L.; Greenberg, R.N. Behaviour of Saccharomyces boulardii in recurrent Clostridium difficile disease patients. Aliment. Pharmacol. Ther. 1999, 13, 1663–1668. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.M.; Elmer, G.W.; McFarland, L.V.; Surawicz, C.M.; Levy, R.H. Recovery and elimination of the biotherapeutic agent, Saccharomyces boulardii, in healthy human volunteers. Pharm. Res. 1993, 10, 1615–1619. [Google Scholar] [CrossRef] [PubMed]
- Blehaut, H.; Massot, J.; Elmer, G.W.; Levy, R.H. Disposition kinetics of Saccharomyces boulardii in man and rat. Biopharm. Drug Dispos. 1989, 10, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, C.; Thévenot, J.; Etienne-Mesmin, L.; Denis, S.; Alric, M.; Livrelli, V.; Blanquet-Diot, S. Dynamic In Vitro Models of the Human Gastrointestinal Tract as Relevant Tools to Assess the Survival of Probiotic Strains and Their Interactions with Gut Microbiota. Microorganisms 2015, 3, 725–745. [Google Scholar] [CrossRef]
- Jeavons, H.S. Prevention and treatment of vulvovaginal candidiasis using exogenous Lactobacillus. J. Obstet. Gynecol. Neonatal Nurs. 2003, 32, 287–296. [Google Scholar] [CrossRef]
- Marrazzo, J.M.; Fiedler, T.L.; Srinivasan, S.; Thomas, K.K.; Liu, C.; Ko, D.; Xie, H.; Saracino, M.; Fredricks, D.N. Extravaginal Reservoirs of Vaginal Bacteria as Risk Factors for Incident Bacterial Vaginosis. J. Infect. Dis. 2012, 205, 1580–1588. [Google Scholar] [CrossRef] [Green Version]
- Cayzeele-Decherf, A.; Pélerin, F.; Leuillet, S.; Douillard, B.; Housez, B.; Cazaubiel, M.; Jacobson, G.K.; Jüsten, P.; Desreumaux, P. Saccharomyces cerevisiae CNCM I-3856 in irritable bowel syndrome. World J. Gastroenterol. 2017, 23, 336–344. [Google Scholar] [CrossRef] [Green Version]
- Sobel, J.D. Vulvovaginal candidosis. Lancet 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Martin Lopez, J.E. Candidiasis (vulvovaginal). BMJ Clin. Evid. 2015, 2015, 0815. [Google Scholar]
- Decherf, A.C.; Pelerin, F.; Justen, P. Saccharomyces cerevisiae CNCM I-3856 as a natural breakthrough for vaginal health: A clinical study. Med. J. Obstet. Gynecol. 2017, 5, 1112. [Google Scholar]
- Leyva-Gómez, G.; Prado-Audelo, M.L.D.; Ortega-Peña, S.; Mendoza-Muñoz, N.; Urbán-Morlán, Z.; González-Torres, M.; González-Del Carmen, M.; Figueroa-González, G.; Reyes-Hernández, O.D.; Cortés, H. Modifications in Vaginal Microbiota and Their Influence on Drug Release: Challenges and Opportunities. Pharmaceutics 2019, 11, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Products | S. cerevisiae CNCM I-3856 | Maize Starch + Magnesium Stearate | Total |
|---|---|---|---|
| 500 mg Probiotic Group | 1 capsule (500 mg) 2.5 × 109 CFU | 1 capsule (500 mg) | 2 capsules (2 × 500 mg) |
| 1000 mg Probiotic Group | 2 capsules (2 × 500 mg) 5 × 109 CFU | - | 2 capsules (2 × 500 mg) |
| Placebo Group | - | 2 capsules (2 × 500 mg) | 2 capsules (2 × 500 mg) |
| Total Included Subjects (n = 60) | Placebo Group (n = 20) | 500 mg Probiotic Group (n = 20) | 1000 mg Probiotic Group (n = 20) | |
|---|---|---|---|---|
| Age (years) | 31.2 (7.19) | 32.2 (7.67) | 32.7 (7.57) | 28.7 (5.83) |
| Body mass index (BMI) (Kg/m2) (V1) | 23.8 (4.90) | 23.5 (4.16) | 24.6 (6.22) | 23.3 (4.19) |
| Ethnicity | 60 (100%) | 20 (100%) | 20 (100%) | 20 (100.0) |
| Caucasian | 60 (100%) | 20 (100%) | 20 (100%) | 20 (100.0) |
| Contraceptive method | 60 (100%) | 20 (100%) | 20 (100%) | 20 (100.0) |
| Estroprogestative pill (21 days/month) | 38 (63.3%) | 13 (65.0%) | 13 (65.0%) | 12 (60.0%) |
| Simple intra-uterine device | 19 (31.7%) | 5 (25.0%) | 7 (35.0%) | 7 (35.0%) |
| Oestroprogestative patch with a stop of 7 days at each cycle | 1 (1.7%) | 0 (0.0%) | 0 (0.0%) | 1 (5.0%) |
| Tubal ligation | 1 (1.7%) | 1 (5.0%) | 0 (0.0%) | 0 (0.0%) |
| Essure system | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Condom + spermicidal gel | 1 (1.7%) | 1 (5.0%) | 0 (0.0%) | 0 (0.0%) |
| Vaginal pH (V0) | 4.10 (0.303) | 4.15 (0.366) | 4.03 (0.112) | 4.13 (0.358) |
| Nugent score (V0) | 0.52 (0.676) | 0.40 (0.681) | 0.4 (0.598) | 0.75 (0.716) |
| Presence of C. albicans in vaginal samples (V1) | 2 (3.3) | 1 (5.0) | 0 (0.0) | 1 (5.0) |
| Presence of S. cerevisiae I-3856 in stool samples (V1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Presence of S. cerevisiae I-3856 in vaginal samples (V1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Timepoints | 500 mg Probiotic Group | 1000 mg Probiotic Group | ||
|---|---|---|---|---|
| Randomization Number | Log/Sample | Randomization Number | Log/Sample | |
| D7 | 26 | 1.0 | - | - |
| 60 | 2.0 | - | - | |
| 67 | 1.8 | - | - | |
| D14 | 67 | 3.9 | 84 | 5.0 |
| D21 | 4 | 1.6 | 41 | 4.5 |
| 67 | 4.5 | 84 | 1.0 | |
| D28 | 4 | 1.0 | 74 | 1.3 |
| 67 | 4.9 | - | - | |
| Timepoints | 500 mg Probiotic Group | 1000 mg Probiotic Group | Placebo Group | |||
|---|---|---|---|---|---|---|
| Randomization Number | Log/sample | Randomization Number | Log/Sample | Randomization Number | Log/Sample | |
| D0 | - | - | 17 | 2.4 | 45 | 4.2 |
| D7 | - | - | 17 | 3.5 | 05 | 2.2 |
| - | - | - | - | 43 | 3.0 | |
| - | - | - | - | 45 | 2.7 | |
| D14 | 01 | 1.0 | 17 | 2.8 | 05 | 3.3 |
| - | - | - | - | 43 | 4.5 | |
| D21 | 32 | 3.3 | 17 | 3.7 | 39 | 1.0 |
| - | - | - | - | 43 | 3.6 | |
| - | - | - | - | 45 | 3.0 | |
| D28 | 70 | 2.1 | 17 | 2.0 | 05 | 1.9 |
| - | - | - | - | 45 | 1.6 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Decherf, A.; Dehay, E.; Boyer, M.; Clément-Ziza, M.; Rodriguez, B.; Legrain-Raspaud, S. Recovery of Saccharomyces cerevisiae CNCM I-3856 in Vaginal Samples of Healthy Women after Oral Administration. Nutrients 2020, 12, 2211. https://doi.org/10.3390/nu12082211
Decherf A, Dehay E, Boyer M, Clément-Ziza M, Rodriguez B, Legrain-Raspaud S. Recovery of Saccharomyces cerevisiae CNCM I-3856 in Vaginal Samples of Healthy Women after Oral Administration. Nutrients. 2020; 12(8):2211. https://doi.org/10.3390/nu12082211
Chicago/Turabian StyleDecherf, Amelie, Elodie Dehay, Mickaël Boyer, Mathieu Clément-Ziza, Bertrand Rodriguez, and Sophie Legrain-Raspaud. 2020. "Recovery of Saccharomyces cerevisiae CNCM I-3856 in Vaginal Samples of Healthy Women after Oral Administration" Nutrients 12, no. 8: 2211. https://doi.org/10.3390/nu12082211
APA StyleDecherf, A., Dehay, E., Boyer, M., Clément-Ziza, M., Rodriguez, B., & Legrain-Raspaud, S. (2020). Recovery of Saccharomyces cerevisiae CNCM I-3856 in Vaginal Samples of Healthy Women after Oral Administration. Nutrients, 12(8), 2211. https://doi.org/10.3390/nu12082211