A Low-FODMAP Diet for Irritable Bowel Syndrome: Some Answers to the Doubts from a Long-Term Follow-Up

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Nutritional Assessment and Anthropometrical Measurements
2.2. BIVA (Bioelectrical Impedance Vector Analysis)
2.3. Questionnaires
- 1.
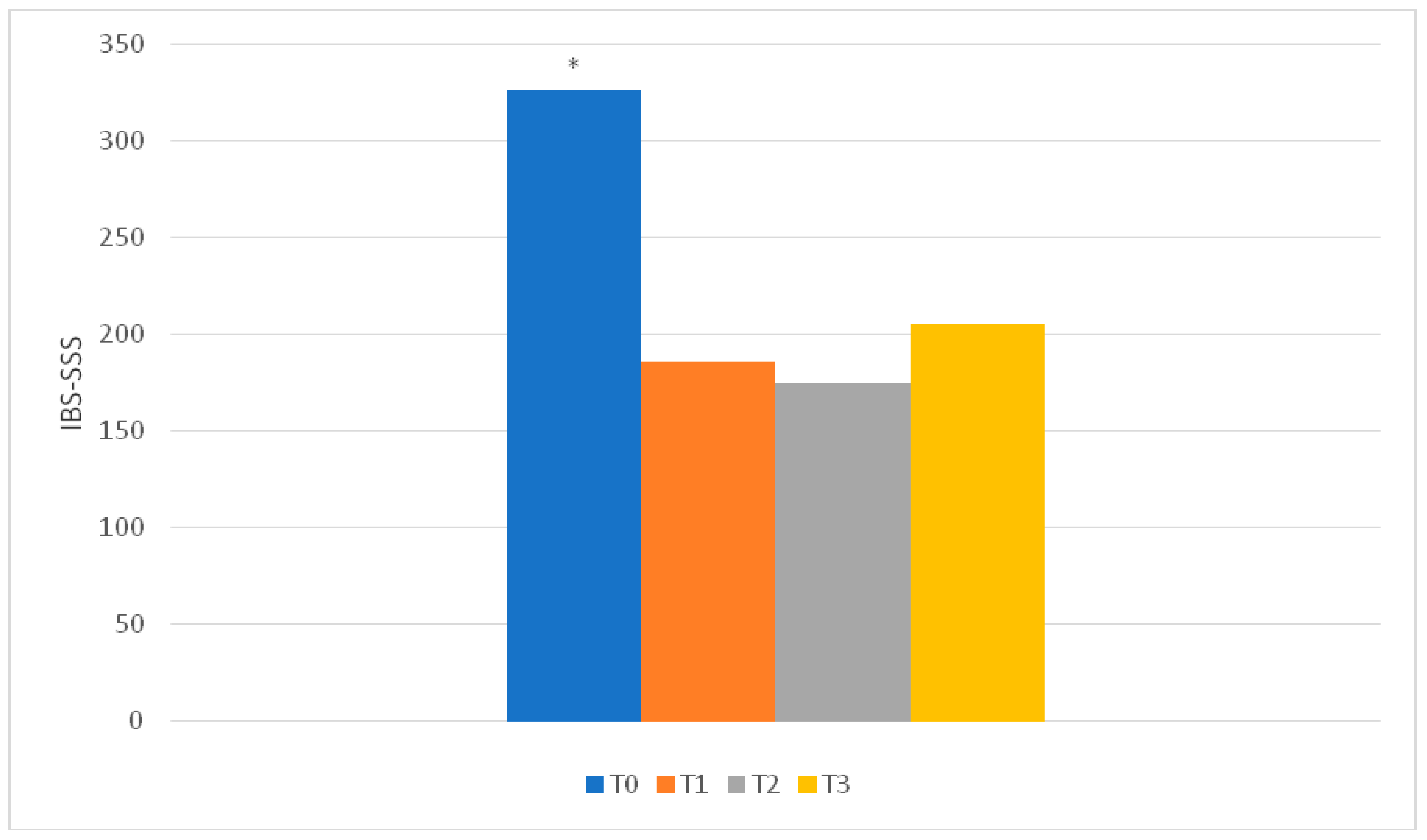
- IBS—Symptom Severity Score (IBS-SSS): this evaluates the severity of abdominal symptoms [22]. It consists of 5 questions that investigate the presence and severity of abdominal pain or discomfort, frequency of abdominal pain, presence and severity of abdominal distension, degree of dissatisfaction with defecatory function and degree of interference of IBS symptoms in work and life habits [3]. Each question is answered by indicating the percentage of the symptomatology on a visual analogue scale (VAS), which generates a score from 0 to 100, where 0 indicates “not at all/absent”, 50 indicates “quite important” and 100 indicates “very important”. The maximum final score, obtained from the sum of the individual values, is 500. A score higher than 300 is a sign of severe symptoms, from 175 to 300 indicates moderate symptoms and between 75 and 175 is a sign of mild symptoms.
- 2.
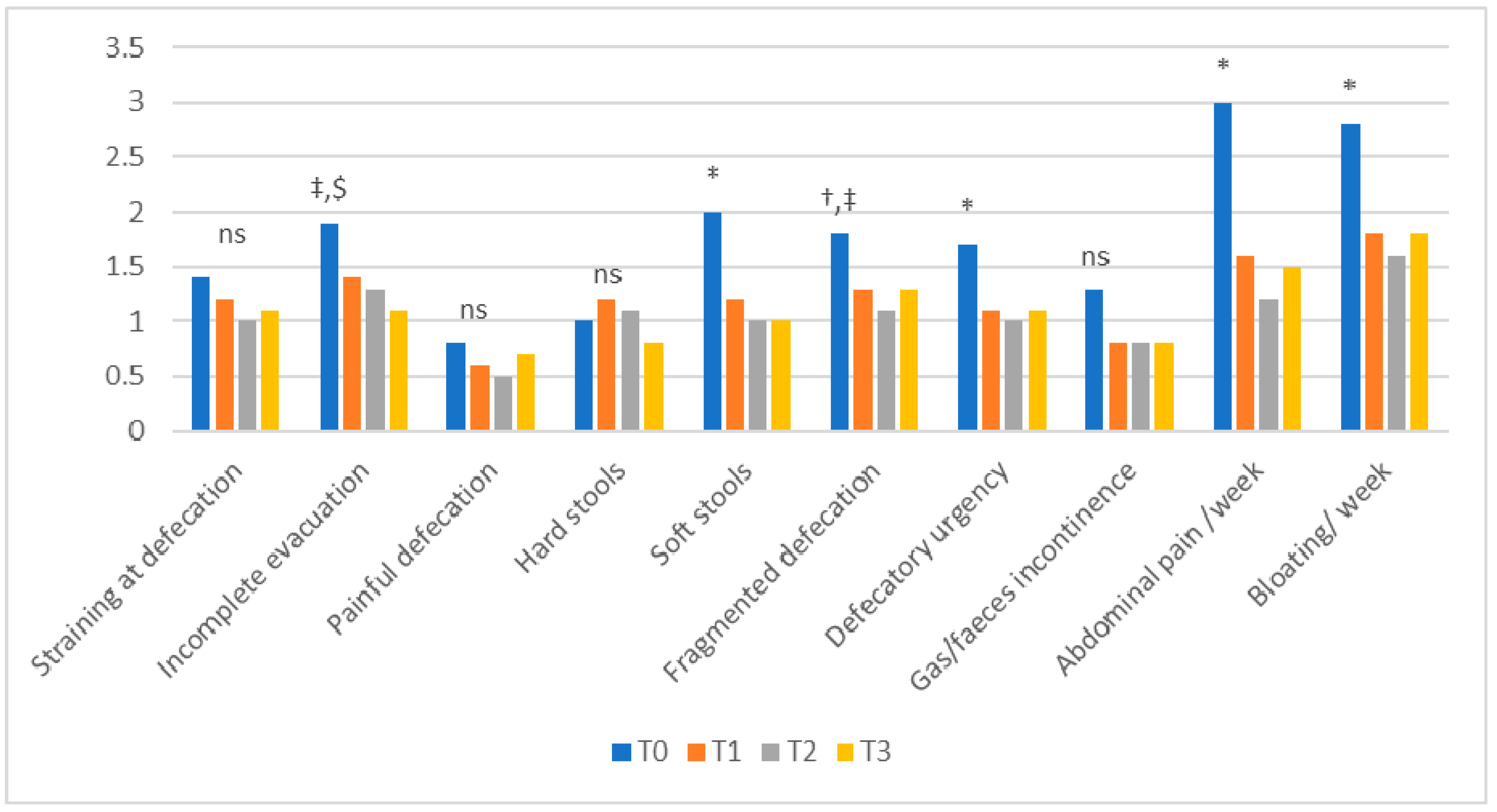
- Bowel habits questionnaire: a ‘‘homemade’’ bowel habits questionnaire evaluating the frequency of (a) straining at defecation, (b) incomplete evacuation, (c) painful defecation, (d) hard stools (Bristol Stool Scale 1–2), (e) watery stools (Bristol Stool Scale 6–7), (f) fragmented defecation, (g) defecatory urgency, (h) incontinence for gas and/or feces, (i) abdominal pain and (j) abdominal bloating, using a scale ranging from 0 (no symptoms) to 4 (symptoms present during >75% of bowel movements or days) [23].
- 3.
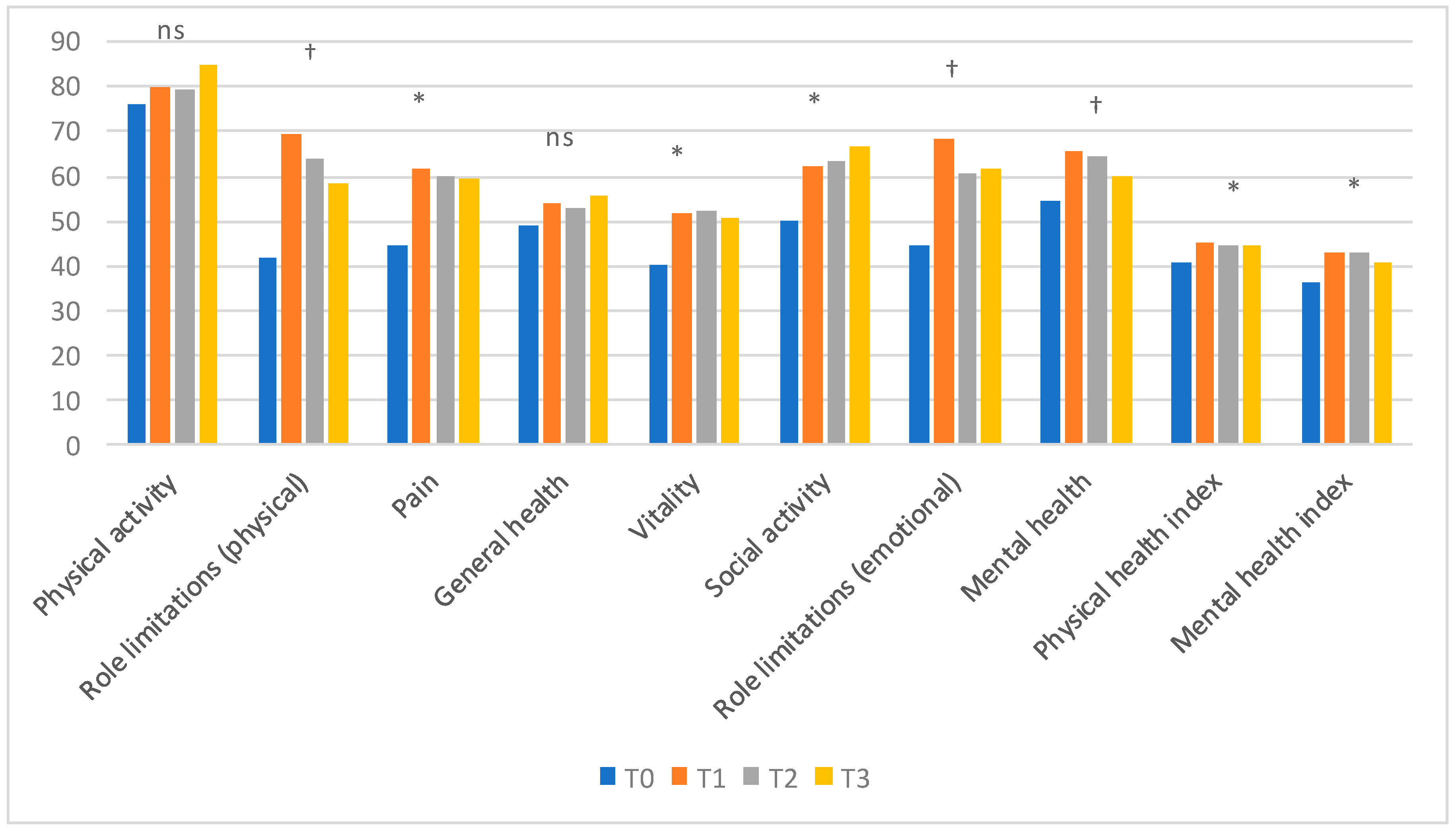
- SF–36 (Italian version): a questionnaire able to measure the health-related quality of life in the general population [24,25]. It consists of 36 questions divided into 8 sections, each investigating a different aspect of health:
- -
- Physical functioning (10 questions)
- -
- Social functioning (2 questions)
- -
- Role limitations (physical problems) (4 questions)
- -
- Role limitations (emotional problems) (3 questions)
- -
- Mental health (5 questions)
- -
- Vitality (4 questions)
- -
- Pain (2 questions)
- -
- General health (5 questions)
- -
- Health change (1 question)
From each section, a score on a scale from 0 to 100 is obtained, where 0 is the worst possible health state measured by the questionnaire and 100 is the best possible health state. It is also possible to calculate two summary indexes: one for physical function (PFI) and the other for mental function (MFI), standardized versus a normal value of 50 ± 10. - 4.
- Hospital Anxiety and Depression Scale (HADS): used to investigate the presence and severity of anxiety and depression with a good sensitivity and specificity [26]. It includes 14 questions divided into two groups: 7 questions investigate anxiety symptoms (HADS-A) and 7 assess symptoms of depression (HADS-D). Each question is given a score from 0 to 3, with a possible total score ranging from 0 to 42.
- 5.
- Pittsburgh Sleep Quality Index (PSQI): this investigates the quality of sleep and possible sleep disorders over a period of one month. It consists of 19 questions from which 7 overall scores are obtained, each representing a particular aspect of sleep: subjective quality, latency, duration, habitual sleep efficacy, sleep disturbances, use of sleeping medication and daytime dysfunctions. The sum of the scores of these seven components, to which a value from 0 to 3 is attributed, produces the overall result of the PSQI. It can vary from 0 to 21, where a score higher than 5 is considered indicative of sleep disorders [27,28].
- Degree of relief: this estimates the symptom improvement perceived by the patient compared to T0. The answer is indicated on a 7-point visual analogue scale, where 7 means that the patient feels much worse than at the beginning of the treatment, 4 means nothing has changed and 1 indicates that the patient feels completely relieved, with a remission of symptoms [29,30].
- Degree of treatment satisfaction: a single question that estimates patient satisfaction with the LFD or AdLFD. The patient is asked to mark the answer on a 10-point visual analogue scale, where 0 indicates that the patient is totally dissatisfied with the diet and 10 indicates completely satisfied [29,30].
- FODMAP Adherence Report Scale (FARS): this evaluates how much the patient adhered to the diet. It consists of 5 questions, each offering five possible answers (always, often, sometimes, rarely and never) to which a score is assigned respectively from 1 to 5, with a maximum score of 25. A total score of at least 20 points (≥80%) is considered as adherence to the diet [31].
- LFD acceptability questionnaire: composed of 13 items adapted from the nutrition-related QOL (Quality of Life) questionnaire [32]. This investigates the impact of the diet on everyday life. The answers are categorized using 3 possible answers (agree, neutral and disagree) [33] (Table S1 in the Supplementary Materials).
- Food-related QOL questionnaire: a seven-item questionnaire, based on a 3-point Likert scale (agree, neutral and disagree), investigating the relationship with food and meals [34] (Table S2 in the Supplementary Materials).
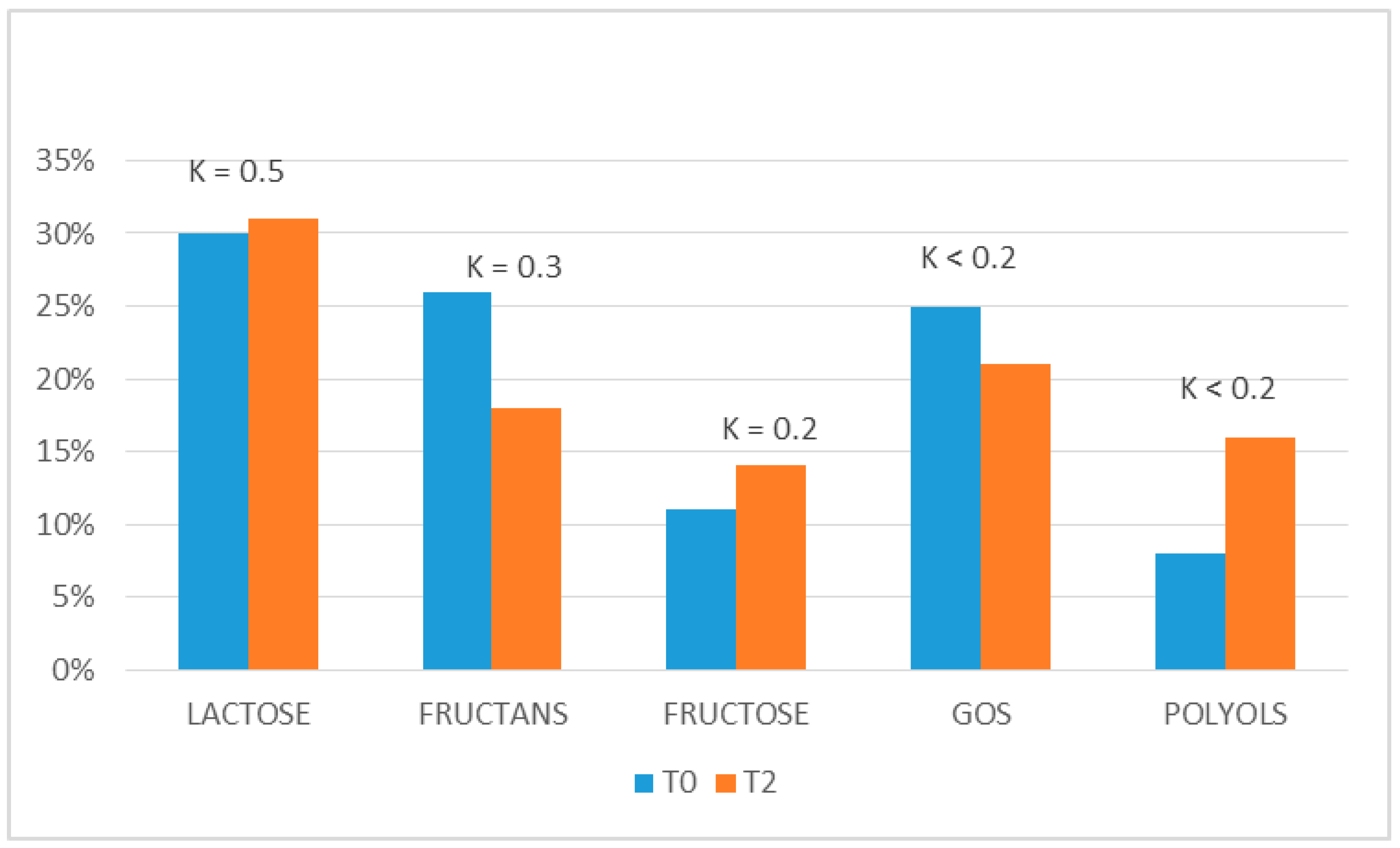
- Perception of “trigger” foods: at T0, the patients were asked if there were some FODMAP groups that they could identify as trigger food, e.g., causing bloating, pain and/or impairing the quality of their defecation (bowel movements and stool consistency). Data were compared with the results obtained at the end of the reintroduction period (T2) to evaluate the concordance in detecting the FODMAP foods able to provoke their symptoms.
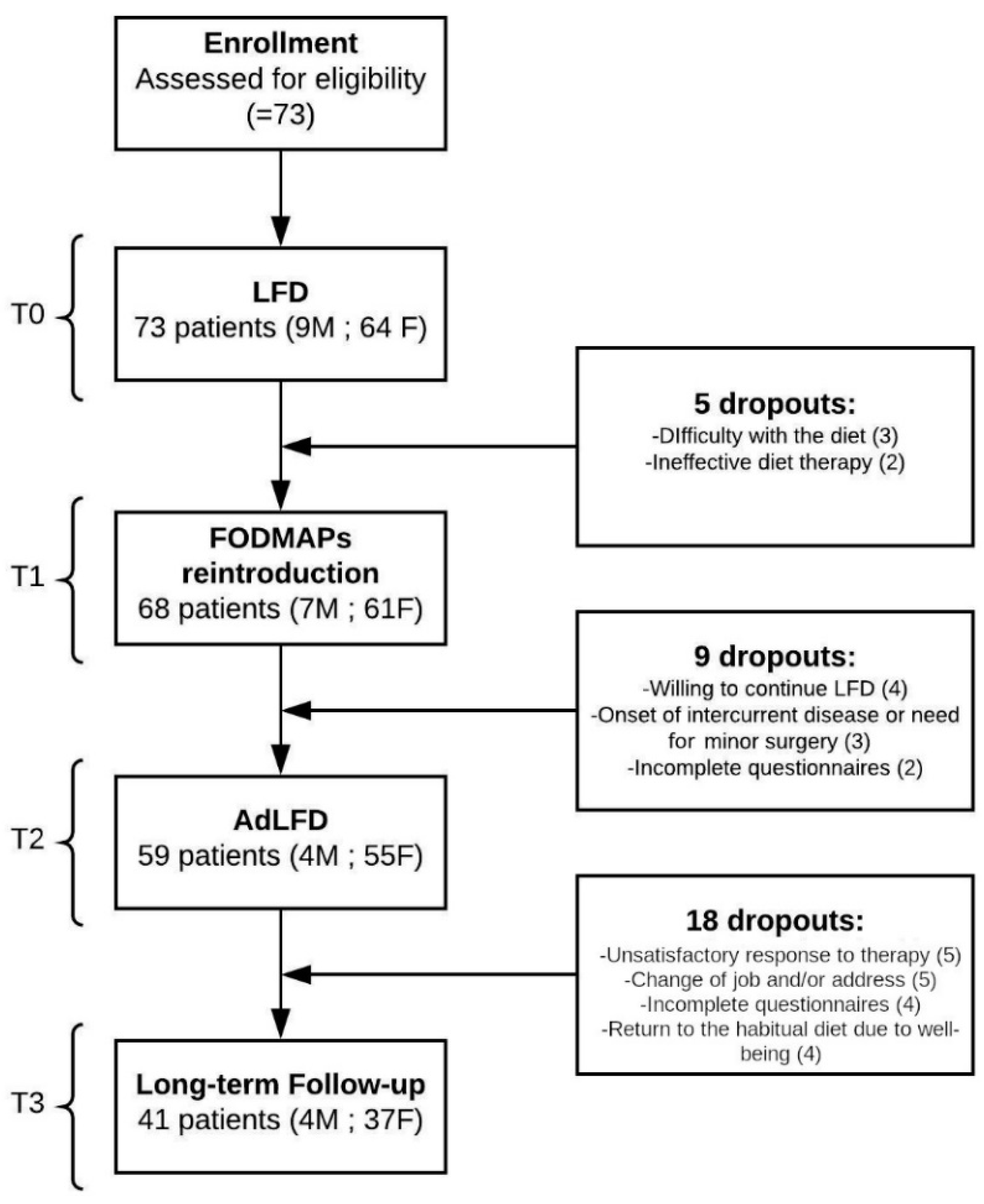
2.4. Enrollment (T0)
2.5. First Check-Up (T1)
2.6. Second Check-Up (T2)
2.7. Third Check-Up (T3)
2.8. Data Analysis and Statistical Tests
3. Results
3.1. BIVA and Anthropometrical Measurements
3.2. IBS-SSS
3.3. Bowel Habits
3.4. SF–36
3.5. Hospital Anxiety and Depression Scale (HADS)
3.6. Pittsburgh Sleep Quality Index (PSQI)
3.7. Evaluation of the Degree of Relief and Degree of Treatment Satisfaction
3.8. FODMAP Adherence Report Scale (FARS)
3.9. Acceptability of the Diet
3.10. Food-Related QOL
3.11. Perception of Trigger Foods
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weaver, K.R.; Melkus, G.D.; Henderson, W.A. Irritable bowel syndrome. Am. J. Nurs. 2017, 117, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.; Gambaccini, D.; Stasi, C.; Urbano, M.T.; Marchi, S.; Usai-Satta, P. Irritable bowel syndrome: A disease still searching for pathogenesis, diagnosis and therapy. World J. Gastroenterol. 2014, 20, 8807–8820. [Google Scholar] [CrossRef] [PubMed]
- Soncini, M.; Stasi, C.; Usai Satta, P.; Milazzo, G.; Bianco, M.; Leandro, G.; Montalbano, L.M.; Muscatiello, N.; Monica, F.; Galeazzi, F.; et al. IBS clinical management in Italy: The AIGO survey. Dig. Liver Dis. 2019, 51, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Spiegel, B.M. The effect of irritable bowel syndrome on health-related quality of life and health care expenditures. Gastroenterol. Clin. N. Am. 2011, 40, 11–19. [Google Scholar] [CrossRef]
- Basilisco, G. Italian Society of Neurogastroenterology Motility (SINGEM). Study Group. Patient dissatisfaction with medical therapy for chronic constipation or irritable bowel syndrome with constipation: Analysis of N-of-1 prospective trials in 81 patients. Aliment. Pharmacol. Ther. 2020, 51, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef] [Green Version]
- De Giorgio, R.; Volta, U.; Gibson, P.R. Sensitivity to wheat, gluten and FODMAPs in IBS: Facts or fiction? Gut 2016, 65, 169–178. [Google Scholar] [CrossRef]
- Bellini, M.; Tonarelli, S.; Nagy, A.G.; Pancetti, A.; Costa, F.; Ricchiuti, A.; de Bortoli, N.; Mosca, M.; Marchi, S.; Rossi, A. Low FODMAP diet: Evidence, doubts, and hopes. Nutrients 2020, 12, 148. [Google Scholar] [CrossRef] [Green Version]
- Gibson, P.R.; Shepherd, S.J. Personal view: Food for thought—Western lifestyle and susceptibility to Crohn’s disease―The FODMAP hypothesis. Aliment Pharmacol Ther. 2005, 21, 1399–1409. [Google Scholar] [CrossRef]
- Bellini, M.; Rossi, A. Is a low FODMAP diet dangerous? Tech. Coloproctol. 2018, 22, 569–571. [Google Scholar] [CrossRef] [Green Version]
- O’Keeffe, M.; Lomer, M.C. Who should deliver the low FODMAP diet and what educational methods are optimal: A review. J. Gastroenterol. Hepatol. 2017, 32, 23–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dionne, J.; Ford, A.C.; Yuan, Y.; Chey, W.D.; Lacy, B.E.; Saito, Y.A.; Quigley, E.M.M.; Moayyedi, P. A systematic review and meta-analysis evaluating the efficacy of a gluten-free diet and a low FODMAPs diet in treating symptoms of irritable bowel syndrome. Am. J. Gastroenterol. 2018, 113, 1290–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gomez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Composition of the EWG: Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, A.; Nigrelli, S.; Caberlotto, A.; Bottazzo, S.; Rossi, B.; Pillon, L.; Maggiore, Q. Bivariate normal values of the bioelectrical impedance vector in adult and elderly populations. Am. J. Clin. Nutr. 1995, 61, 269–270. [Google Scholar] [CrossRef]
- Piccoli, A.; Rossi, B.; Pillon, L.; Bucciante, G. A new method for monitoring body fluid variation by bioimpedance analysis: The RXc graph. Kidney Int. 1994, 6, 534–539. [Google Scholar] [CrossRef] [Green Version]
- Bosy-Westphal, A.; Danielzik, S.; Dörhöfer, R.P.; Piccoli, A.; Müller, M.J. Patterns of bioelectrical impedance vector distribution by body mass index and age: Implications for body-composition analysis. Am. J. Clin. Nutr. 2005, 82, 60–68. [Google Scholar] [CrossRef]
- Walter-Kroker, A.; Kroker, A.; Mattiucci-Guehlke, M.; Glaab, T. A practical guide to bioelectrical impedance analysis using the example of chronic obstructive pulmonary disease. Nutr. J. 2011, 10, 35. [Google Scholar] [CrossRef] [Green Version]
- Buffa, R.; Mereu, E.; Comandini, O.; Ibanez, M.E.; Marini, E. Bioelectrical impedance vector analysis (BIVA) for the assessment of two-compartment body composition. Eur. J. Clin. Nutr. 2014, 68, 1234–1240. [Google Scholar] [CrossRef]
- Alves, F.D.; Souza, G.C.; Aliti, G.B.; Rabelo-Silva, E.R.; Clausell, N.; Biolo, A. Dynamic changes in bioelectrical impedance vector analysis and phase angle in acute decompensated heartfailure. Nutrition 2015, 31, 84–89. [Google Scholar] [CrossRef]
- Buffa, R.; Saragat, B.; Cabras, S.; Rinaldi, A.C.; Marini, E. Accuracy of specific BIVA for the assessment of body composition in the United States population. PLoS ONE 2013, 8, e58533. [Google Scholar] [CrossRef]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bellini, M.; Gemignani, A.; Gambaccini, D.; Toti, S.; Menicucci, D.; Stasi, C.; Costa, F.; Mumolo, M.G.; Ricchiuti, A.; Bedini, R.; et al. Evaluation of latent links between irritable bowel syndrome and sleep quality. World J. Gastroenterol. 2011, 17, 5089–5096. [Google Scholar] [CrossRef]
- Camilleri, M.; Lembo, A.J.; Lavins, B.J.; MacDougall, J.E.; Carson, R.T.; Williams, V.S.; Nelson, L.M.; Shiff, S.J.; Currie, M.G.; Kurtz, C.B.; et al. Comparison of adequate relief with symptom, global, and responder endpoints in linaclotide phase 3 trials in IBS-C. United Eur. Gastroenterol. J. 2015, 3, 53–62. [Google Scholar] [CrossRef]
- Cremon, C.; Guglielmetti, S.; Gargari, G.; Taverniti, V.; Castellazzi, A.M.; Valsecchi, C.; Tagliacarne, C.; Fiore, W.; Bellini, M.; Bertani, L.; et al. Effect of Lactobacillus paracasei CNCM I-1572 on symptoms, gut microbiota, short chain fatty acids, and immune activation in patients with irritable bowel syndrome: A pilot randomized clinical trial. United Eur. Gastroenterol. J. 2018, 6, 604–613. [Google Scholar] [CrossRef] [Green Version]
- Maagaard, L.; Ankersen, D.V.; Végh, Z.; Burisch, J.; Jensen, L.; Pedersen, N.; Munkholm, P. Follow-up of patients with functional bowel symptoms treated with a low FODMAP diet. World J. Gastroenterol. 2016, 22, 4009–4019. [Google Scholar] [CrossRef]
- O’Keeffe, M.; Jansen, C.; Martin, L.; Williams, M.; Seamark, L.; Staudacher, H.M.; Irving, P.M.; Whelan, K.; Lomer, M.C. Long-term impact of the low-FODMAP diet on gastrointestinal symptoms, dietary intake, patient acceptability, and healthcare utilization in irritable bowel syndrome. Neurogastroenterol. Motil. 2018, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, J.; Schumacher, G. Using focus groups to determine what constitutes quality of life in clients receiving medical nutrition therapy: First steps in the development of a nutrition quality-of- life survey. J. Am. Diet. Assoc. 2003, 103, 844–851. [Google Scholar] [CrossRef]
- Grunert, K.G.; Dean, M.; Raats, M.M.; Nielsen, N.A.; Lumbers, M. Food in later life team: A measure of satisfaction with food-related Life. Appetite 2007, 49, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Shepard, S.; Gibson, P.; Chey, W.D. The Complete Low-FODMAP Diet: A Revolutionary Plan for Managing IBS and Other Digestive Disorders, 1st ed.; The Experiment LLC: New York, NY, USA, 2013. [Google Scholar]
- Varney, J.; Barrett, J.; Scarlata, K.; Catsos, P.; Gibson, P.R.; Muir, J.G. FODMAPs: Food composition, defining cutoff values and international application. J. Gastroenterol. Hepatol. 2017, 32, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Muir, J.G.; Shepherd, S.J.; Rosella, O.; Rose, R.; Barrett, J.S.; Gibson, P.R. Fructan and free fructose content of common Australian vegetables and fruit. J. Agric. Food Chem. 2007, 55, 6619–6627. [Google Scholar] [CrossRef]
- Muir, J.G.; Rose, R.; Rosella, O.; Liels, K.; Barrett, J.S.; Shepherd, S.J.; Gibson, P.R. Measurement of short-chain carbohydrates in common Australian vegetables and fruits by high-performance liquid chromatography (HPLC). J. Agric. Food Chem. 2009, 57, 554–565. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Rosella, O.; Rose, R.; Liels, K.; Barrett, J.S.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. Quantification of fructans, galacto-oligosaccharides and other short-chain carbohydrates in processed grains and cereals. J. Hum. Nutr. Diet. 2011, 24, 154–176. [Google Scholar] [CrossRef]
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- Gravina, A.G.; Dallio, M.; Romeo, M.; Di Somma, A.; Cotticelli, G.; Loguercio, C.; Federico, A. Adherence and effects derived from FODMAP diet on irritable bowel syndrome: A real life evaluation of a large follow-up observation. Nutrients 2020, 12, 928. [Google Scholar] [CrossRef] [Green Version]
- Staudacher, H.M.; Whelan, K. The low FODMAP diet: Recent advances in understanding its mechanisms and efficacy in IBS. Gut 2017, 66, 1517–1527. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.C.; Lacy, B.E.; Talley, N.J. Irritable Bowel Syndrome. N. Engl. J. Med. 2017, 376, 2566–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caccialanza, R.; Cereda, E.; Klersy, C.; Bonardi, C.; Cappello, S.; Quarleri, L.; Turri, A.; Montagna, E.; Iacona, I.; Valentino, F.; et al. Phase angle and handgrip strength are sensitive early markers of energy intake in hypophagic, non-surgical patients at nutritional risk, with contraindications to enteral nutrition. Nutrients 2015, 7, 1828–1840. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.; Gambaccini, D.; Bazzichi, L.; Bassotti, G.; Mumolo, M.G.; Fani, B.; Costa, F.; Ricchiuti, A.; De Bortoli, N.; Mosca, M.; et al. Bioelectrical impedance vector analysis in patients with irritable bowel syndrome on a low FODMAP diet: A pilot study. Tech. Coloproctol. 2017, 21, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Burkhart, P.V.; Sabaté, E. Adherence to long-term therapies: Evidence for action. J. Nurs. Scholarsh. 2003, 35, 207. [Google Scholar] [PubMed]
- Harvie, R.M.; Chisholm, A.W.; Bisanz, J.E.; Burton, J.P.; Herbison, P.; Schultz, K.; Schultz, M. Long-term irritable bowel syndrome symptom control with reintroduction of selected FODMAPs. World J. Gastroenterol. 2017, 23, 4632–4643. [Google Scholar] [CrossRef]
- De Roest, R.H.; Dobbs, B.R.; Chapman, B.A.; Batman, B.; O’Brien, L.A.; Leeper, J.A.; Hebblethwaite, C.R.; Gearry, R.B. The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: A prospective study. Int. J. Clin. Pract. 2013, 67, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M.; Lomer, M.C.; Anderson, J.L.; Barrett, J.S.; Muir, J.G.; Irving, P.M.; Whelan, K. Fermentable carbohydrate restriction reduces luminal bifidobacteria and gastrointestinal symptoms in patients with irritable bowel syndrome. J. Nutr. 2012, 142, 1510–1518. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recurrent abdominal pain, at least 1 day per week in the last 3 months, associated with 2 or more of the following characteristics:
|
| Criteria fulfilled with symptom onset in the last 3 months with an onset at least 6 months prior to diagnosis [6]. |
| Habitual Diet | LFD | AdLFD | p-Value | |
|---|---|---|---|---|
| Energy (kcal) | 1996 ± 541 | 1957 ± 459 | 1972 ± 510 | ns |
| Proteins (g) | 90.3 ± 43.3 | 88.4 ± 47.2 | 91.4 ± 44.7 | ns |
| Fats (g) | 72.2 ± 24.1 | 69.5 ± 18.2 | 71.5 ± 20.3 | ns |
| Carbohydrates (g) | 249 ± 41 | 254 ± 59 | 252 ± 60 | ns |
| Dietary fibers (g) | 19.8 ± 8.3 | 18.4 ± 7.2 | 20.3 ± 9.1 | ns |
| Calcium (mg/day) | 910 ± 550 | 870 ± 520 | 970 ± 580 | ns |
| Iron (mg/day) | 8.7 ± 4.2 | 8.6 ± 4.1 | 9.1 ± 4.5 | ns |
| Zinc (mg/day) | 11.3 ± 4.4 | 11.1 ± 4.5 | 11.3 ± 4.5 | ns |
| Magnesium (mg/day) | 420 ± 90 | 390 ± 110 | 430 ± 107 | ns |
| Sodium (g/day) | 2.5 ± 1.8 | 2.3 ± 1.7 | 2.3 ± 1.8 | ns |
| Potassium (g/day) | 4.1 ± 1.9 | 3.9 ± 1.8 | 3.9 ± 1.8 | ns |
| Phosphorus (mg/day) | 1863 ± 630 | 1932 ± 710 | 1879 ± 693 | ns |
| Fructans | 50 g of wheat bread or pasta or 1 clove of garlic or ¼ onion |
| Lactose | 125 mL of milk |
| Fructose | 2 teaspoons of honey |
| Polyols | mushrooms (100 g fresh or 10 g dried) or 2 dried apricots |
| Galactans | lentils or legumes (100 g cooked or 30 g dried) |
| BIVA | T0 | T1 | T2 | T3 | p-Value |
|---|---|---|---|---|---|
| TBW (L/m) | 20.9 ± 2.6 | 20.8 ± 2.7 | 20.9 ± 2.6 | 20.7 ± 2.6 | ns |
| ECW (%) | 0.5 ± 0.0 | 0.5 ± 0.0 | 0.5 ± 0.0 | 0.5 ± 0.0 | ns |
| ICW (%) | 0.5 ± 0.0 | 0.5 ± 0.0 | 0.5 ± 0.0 | 0.5 ± 0.0 | ns |
| FFM (kg/m) | 28.5 ± 3.6 | 28.4 ± 3.6 | 28.6 ± 3.6 | 28.5 ± 3.2 | ns |
| FM (kg/m) | 13.0 ± 5.8 | 12.8 ± 5.9 | 12.8 ± 6.6 | 12.9 ± 6.6 | ns |
| BCM (kg/m) | 14.4 ± 2.6 | 14.5 ± 3.2 | 13.9 ± 2.0 | 13.9 ± 2.7 | ns |
| PhA (°) | 5.2 ± 0.6 | 5.2 ± 0.6 | 5.1 ± 0.5 | 5.3 ± 0.4 | ns |
| BMR (kcal) | 1425.6 ± 119.0 | 1420.1 ± 118.9 | 1416.7 ± 117.5 | 1417.7 ± 117.9 | ns |
| BMI (kg/m2) | 25.0 ± 4.2 | 24.8 ± 4.8 | 24.8 ± 4.9 | 24.8 ± 4.8 | ns |
| HADS | T0 | T1 | T2 | T3 | p-Value |
|---|---|---|---|---|---|
| HADS-A | 9.5 ± 4.4 | 6.4 ± 4.0 | 6.8 ± 4.4 | 7.1 ± 4.4 | T0 vs others: p < 0.001 |
| HADS-D | 6.8 ± 4.3 | 5.2 ± 3.9 | 5.3 ± 4.2 | 5.2 ± 3.8 | T0 vs others: p < 0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, M.; Tonarelli, S.; Barracca, F.; Morganti, R.; Pancetti, A.; Bertani, L.; de Bortoli, N.; Costa, F.; Mosca, M.; Marchi, S.; et al. A Low-FODMAP Diet for Irritable Bowel Syndrome: Some Answers to the Doubts from a Long-Term Follow-Up. Nutrients 2020, 12, 2360. https://doi.org/10.3390/nu12082360
Bellini M, Tonarelli S, Barracca F, Morganti R, Pancetti A, Bertani L, de Bortoli N, Costa F, Mosca M, Marchi S, et al. A Low-FODMAP Diet for Irritable Bowel Syndrome: Some Answers to the Doubts from a Long-Term Follow-Up. Nutrients. 2020; 12(8):2360. https://doi.org/10.3390/nu12082360
Chicago/Turabian StyleBellini, Massimo, Sara Tonarelli, Federico Barracca, Riccardo Morganti, Andrea Pancetti, Lorenzo Bertani, Nicola de Bortoli, Francesco Costa, Marta Mosca, Santino Marchi, and et al. 2020. "A Low-FODMAP Diet for Irritable Bowel Syndrome: Some Answers to the Doubts from a Long-Term Follow-Up" Nutrients 12, no. 8: 2360. https://doi.org/10.3390/nu12082360
APA StyleBellini, M., Tonarelli, S., Barracca, F., Morganti, R., Pancetti, A., Bertani, L., de Bortoli, N., Costa, F., Mosca, M., Marchi, S., & Rossi, A. (2020). A Low-FODMAP Diet for Irritable Bowel Syndrome: Some Answers to the Doubts from a Long-Term Follow-Up. Nutrients, 12(8), 2360. https://doi.org/10.3390/nu12082360