Differences in Sweet Taste Perception and Its Association with the Streptococcus mutans Cariogenic Profile in Preschool Children with Caries

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group and Study Design
2.2. Data Collection
2.3. General Data about Children
2.4. Analysis of Eating Behavior
2.5. Assessment of Sweet and Bitter Taste
2.6. Clinical Evaluation of Caries
2.7. Collection of Samples and Microbiological Analysis
2.8. Statistical Analysis
3. Results
3.1. Study Group
3.2. Body Weight Results
3.3. Assessment of Eating Behavior
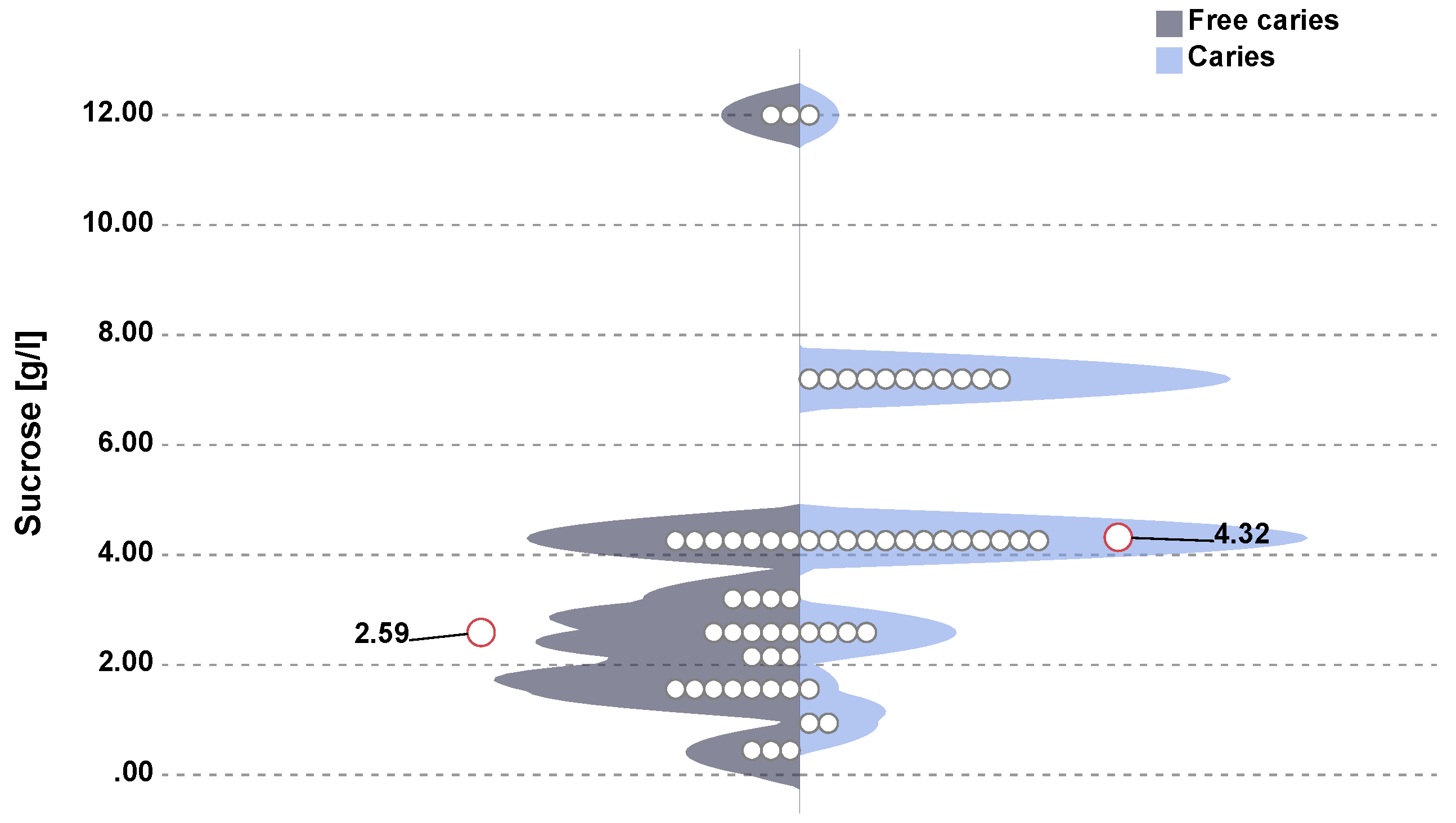
3.4. Evaluation of Sweet Taste
3.5. Clinical Examination
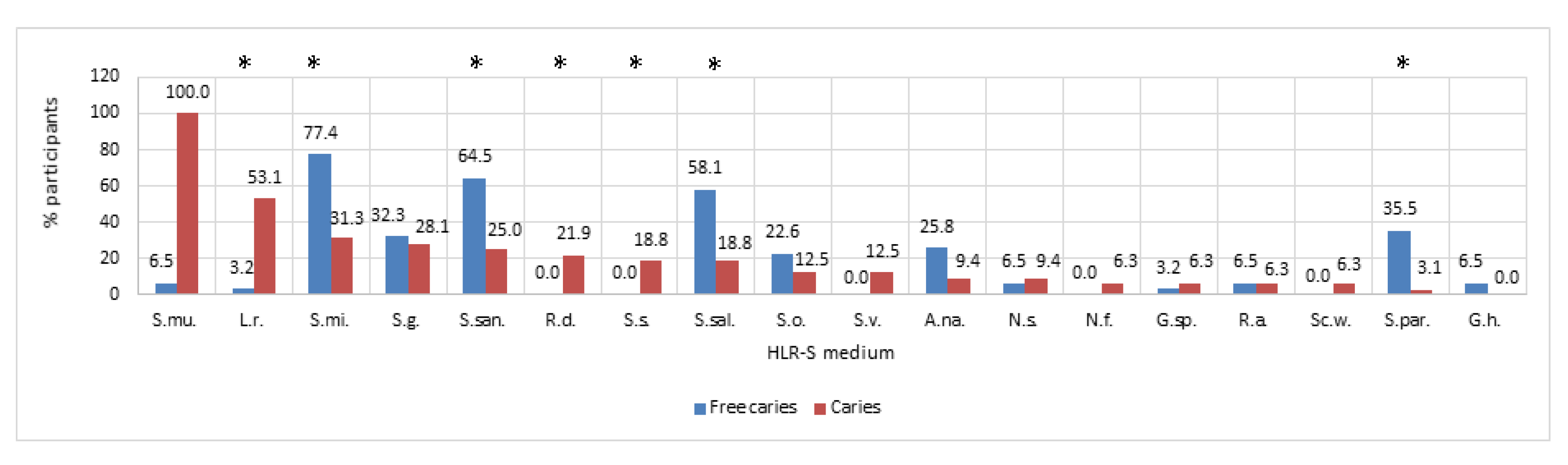
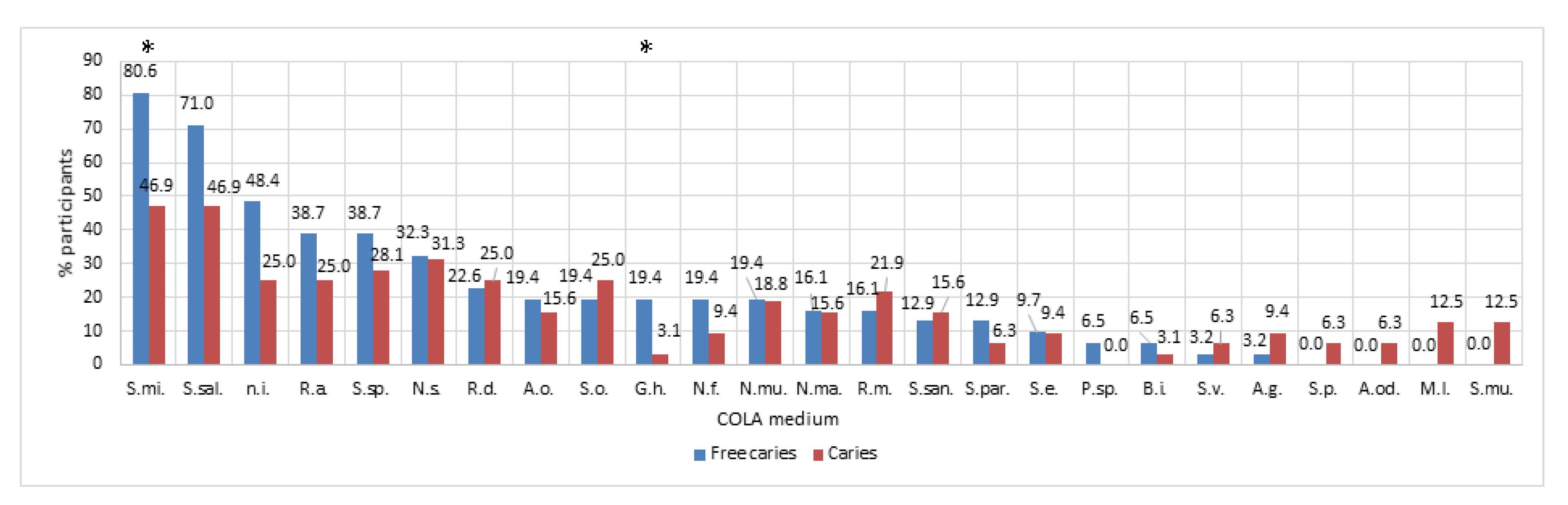
3.6. Microbiology
3.7. Odds Ratio
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
- What meals and at what times during the day does your child eat? Please enter in the table below the time when the child normally eats a given meal. If the meal is not consumed, please leave the field blank.
Meal Breakfast Lunch Dinner Tea-time Supper II supper/snack Time - Does your child eat between meals?
- □
- Yes
- □
- No
- How often does your child eat sweets (candies, chocolates, cookies, sweetened milk products) during the day?
- □
- Not at all
- □
- Sweets do not appear every day
- □
- Once a day
- □
- Several times a day
- Does your child eat in the evening or at night after brushing their teeth?
- □
- Yes
- □
- No
- Does your child consume any beverages other than plain water during the day?
- □
- Yes
- □
- No
- Does your child consume any beverages other than plain water in the evening or at night after brushing their teeth?
- □
- Yes
- □
- No
- Is your child on a vegetarian/vegan diet?
- □
- Yes
- □
- No
- Does the child receive any dietary supplements?
- □
- Yes
- □
- No
- 9.
- Please complete the anthropometric parameters of your child:
Age: Sex: Body mass: Height:
References
- Lemos, J.A.; Palmer, S.R.; Zeng, L.; Wen, Z.T.; Kajfasz, J.K.; Freires, I.A.; Abranches, J.; Brady, L.J. The Biology of Streptococcus mutans. Microbiol. Spectr. 2019, 7, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Chamoun, E.; Carroll, N.A.; Duizer, L.M.; Qi, W.; Feng, Z.; Darlington, G.; Duncan, A.M.; Haines, J.; Ma, D.W.L. The Relationship between Single Nucleotide Polymorphisms in Taste Receptor Genes, Taste Function and Dietary Intake in Preschool-Aged Children and Adults in the Guelph Family Health Study. Nutrients 2018, 10, 990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koletzko, B.; Brands, B.; Grote, V.; Kirchberg, F.F.; Prell, C.; Rzehak, P.; Uhl, O.; Weber, M. Long-Term Health Impact of Early Nutrition: The Power of Programming. Ann. Nutr. Metab. 2017, 70, 161–169. [Google Scholar] [CrossRef]
- Sobek, G.; Łuszczki, E.; Dąbrowski, M.; Dereń, K.; Baran, J.; Weres, A.; Mazur, A. Preferences for Sweet and Fatty Taste in Children and Their Mothers in Association with Weight Status. Int. J. Environ. Res. Public Health 2020, 17, 538. [Google Scholar] [CrossRef] [Green Version]
- Mennella, J.A.; Jagnow, C.P.; Beauchamp, G.K. Prenatal and postnatal flavor learning by human infants. Pediatrics 2001, 107, E88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benton, D.; Nabb, S. Carbohydrate, Memory, and Mood. Nutr. Rev. 2003, 61, S61–S67. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, C.; Issanchou, S.; Nicklaus, S. Developmental changes in the acceptance of the five basic tastes in the first year of life. Br. J. Nutr. 2009, 102, 1375–1385. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, C.; Chabanet, C.; Laval, C.; Issanchou, S.; Nicklaus, S. Breast-feeding duration: Influence on taste acceptance over the first year of life. Br. J. Nutr. 2013, 109, 1154–1161. [Google Scholar] [CrossRef] [Green Version]
- Ventura, A.K. Does Breastfeeding Shape Food Preferences? Links to Obesity. Ann. Nutr. Metab. 2017, 70 (Suppl. 3), 8–15. [Google Scholar] [CrossRef] [PubMed]
- Hausner, H.; Nicklaus, S.; Issanchou, S.; Mølgaard, C.; Møller, P. Breastfeeding facilitates acceptance of a novel dietary flavour compound. Clin. Nutr. 2010, 29, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Forestell, C.A. Flavor Perception and Preference Development in Human Infants. Ann. Nutr. Metab. 2017, 70, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchamp, G.K.; Mennella, J.A. Early flavor learning and its impact on later feeding behavior. J. Pediatr. Gastroenterol. Nutr. 2009, 48, S25–S30. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. The Role of Dietary Experience in the Development of Eating Behavior during the First Years of Life. Ann. Nutr. Metab. 2017, 70, 241–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicklaus, S.; Schwartz, C.; Monnery-Patris, S.; Issanchou, S. Early Development of Taste and Flavor Preferences and Consequences on Eating Behavior. Nestle Nutr. Inst. Workshop Ser. 2019, 91, 1–10. [Google Scholar] [PubMed]
- Paglia, L. The sweet danger of added sugars. Eur. J. Paediatr. Dent. 2019, 20, 89. [Google Scholar]
- Birch, L.L.; Doub, A.E. Learning to eat: Birth to age 2 y. Am. J. Clin. Nutr. 2014, 99, 723S–728S. [Google Scholar] [CrossRef] [Green Version]
- Wudy, S.A.; Hagemann, S.; Dempfle, A.; Ringler, G.; Blum, W.F.; Berthold, L.D.; Alzen, G.; Gortner, L.; Hebebrand, J. Children with idiopathic short stature are poor eaters and have decreased body mass index. Pediatrics 2005, 116, e52–e57. [Google Scholar] [CrossRef] [Green Version]
- Michels, N.; Sioen, I.; Ruige, J.; De Henauw, S. Children’s psychosocial stress and emotional eating: A role for leptin? Int. J. Eat. Disord. 2017, 50, 471–480. [Google Scholar] [CrossRef]
- Feldens, C.A.; Rodrigues, P.H.; de Anastácio, G.; Vítolo, M.R.; Chaffee, B.W. Feeding frequency in infancy and dental caries in childhood: A prospective cohort study. Int. Dent. J. 2018, 68, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Freitas, A.; Albuquerque, G.; Silva, C.; Oliveira, A. Appetite-Related Eating Behaviours: An Overview of Assessment Methods, Determinants and Effects on Children’s Weight. Ann. Nutr. Metab. 2018, 73, 19–29. [Google Scholar] [CrossRef]
- Prieto-Patron, A.; Van der Horst, K.; Hutton, Z.V.; Detzel, P. Association between Anaemia in Children 6 to 23 Months Old and Child, Mother, Household and Feeding Indicators. Nutrients 2018, 10, 1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costacurta, M.; DiRenzo, L.; Sicuro, L.; Gratteri, S.; De Lorenzo, A.; Docimo, R. Dental caries and childhood obesity: Analysis of food intakes, lifestyle. Eur. J. Paediatr. Dent. 2014, 15, 343–348. [Google Scholar] [PubMed]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paglia, L.; Scaglioni, S.; Torchia, V.; De Cosmi, V.; Moretti, M.; Marzo, G.; Giuca, M.R. Familial and dietary risk factors in Early Childhood Caries. Eur. J. Paediatr. Dent. 2016, 17, 93–99. [Google Scholar] [PubMed]
- Paglia, L. WHO: Healthy diet to prevent chronic diseases and caries. Eur. J. Paediatr. Dent. 2018, 19, 5. [Google Scholar]
- Krzyściak, W.; Jurczak, A.; Kościelniak, D.; Bystrowska, B.; Skalniak, A. The virulence of Streptococcus mutans and the ability to form biofilms. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 499–515. [Google Scholar] [CrossRef] [Green Version]
- Jurczak, A.; Kościelniak, D.; Skalniak, A.; Papież, M.; Vyhouskaya, P.; Krzyściak, W. The role of the saliva antioxidant barrier to reactive oxygen species with regard to caries development. Redox Rep. 2017, 22, 524–533. [Google Scholar] [CrossRef] [Green Version]
- Mosaddad, S.A.; Tahmasebi, E.; Yazdanian, A.; Rezvani, M.B.; Seifalian, A.; Yazdanian, M.; Tebyanian, H. Oral microbial biofilms: An update. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2005–2019. [Google Scholar] [CrossRef]
- Ciandrini, E.; Campana, R.; Federici, S.; Manti, A.; Battistelli, M.; Falcieri, E.; Papa, S.; Baffone, W. In vitro activity of Carvacrol against titanium-adherent oral biofilms and planktonic cultures. Clin. Oral Investig. 2014, 18, 2001–2013. [Google Scholar] [CrossRef]
- Koo, H.; Allan, R.N.; Howlin, R.P.; Stoodley, P.; Hall-Stoodley, L. Targeting microbial biofilms: Current and prospective therapeutic strategies. Nat. Rev. Microbiol. 2017, 15, 740–755. [Google Scholar] [CrossRef]
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral Biofilms: Pathogens, Matrix, and Polymicrobial Interactions in Microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Begzati, A.; Berisha, M.; Meqa, K. Early childhood caries in preschool children of Kosovo—A serious public health problem. BMC Public Health 2010, 10, 788. [Google Scholar] [CrossRef] [Green Version]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Rosier, B.T.; Marsh, P.D.; Mira, A. Resilience of the Oral Microbiota in Health: Mechanisms That Prevent Dysbiosis. J. Dent. Res. 2018, 97, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Kressirer, C.A.; Smith, D.J.; King, W.F.; Dobeck, J.M.; Starr, J.R.; Tanner, A.C.R. Scardovia wiggsiae and its potential role as a caries pathogen. J. Oral Biosci. 2017, 59, 135–141. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Kressirer, C.A.; Rothmiller, S.; Johansson, I.; Chalmers, N.I. The Caries Microbiome: Implications for Reversing Dysbiosis. Adv. Dent. Res. 2018, 29, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of dental caries in primary and permanent teeth in children and young adults. J. Clin. Microbiol. 2008, 46, 1407–1417. [Google Scholar] [CrossRef] [Green Version]
- NIH Human Microbiome Project—Core Microbiome Sampling Protocol A (HMP-A). Available online: https://www.ncbi.nlm.nih.gov/projects/gap/cgibin/document.cgi?study_id=phs000228.v3.p1&phd=3190#sec70 (accessed on 29 March 2010).
- Esberg, A.; Haworth, S.; Hasslöf, P.; Lif Holgerson, P.; Johansson, I. Oral Microbiota Profile Associates with Sugar Intake and Taste Preference Genes. Nutrients 2020, 12, 681. [Google Scholar] [CrossRef] [Green Version]
- Krisdapong, S.; Prasertsom, P.; Rattanarangsima, K.; Sheiham, A. Sociodemographic differences in oral health-related quality of life related to dental caries in thai school children. Community Dent. Health 2013, 30, 112–118. [Google Scholar]
- Samaranayake, L.; Matsubara, V.H. Normal Oral Flora and the Oral Ecosystem. Dent. Clin. N. Am. 2017, 61, 199–215. [Google Scholar] [CrossRef]
- Klein-Jöbstl, D.; Quijada, N.M.; Dzieciol, M.; Feldbacher, B.; Wagner, M.; Drillich, M.; Schmitz-Esser, S.; Mann, E. Microbiota of newborn calves and their mothers reveals possible transfer routes for newborn calves’ gastrointestinal microbiota. PLoS ONE 2019, 14, e0220554. [Google Scholar] [CrossRef] [Green Version]
- Sampaio-Maia, B.; Monteiro-Silva, F. Acquisition and maturation of oral microbiome throughout childhood: An update. Dent. Res. J. 2014, 11, 291–301. [Google Scholar]
- Dominguez-Bello, M.G.; Costello, E.K.; Contreras, M.; Magris, M.; Hidalgo, G.; Fierer, N.; Knight, R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc. Natl. Acad. Sci. USA 2010, 107, 11971–11975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagg, J.; MacFarlane, T.; Poxton, I.; Smith, A. Essentials of Microbiology for Dental Students; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Di, K.; Yuqing, L.; Xuedong, Z. Construction of a low-pH-sensing system in Streptococcus mutans. Hua xi kou qiang yi xue za zhi = Huaxi kouqiang yixue zazhi = West China J. Stomatol. 2017, 35, 239–244. [Google Scholar]
- Xu, H.; Hao, W.; Zhou, Q.; Wang, W.; Xia, Z.; Liu, C.; Chen, X.; Qin, M.; Chen, F. Plaque bacterial microbiome diversity in children younger than 30 months with or without caries prior to eruption of second primary molars. PLoS ONE 2014, 9, e89269. [Google Scholar] [CrossRef] [PubMed]
- Cephas, K.D.; Kim, J.; Mathai, R.A.; Barry, K.A.; Dowd, S.E.; Meline, B.S.; Swanson, K.S. Comparative analysis of salivary bacterial microbiome diversity in edentulous infants and their mothers or primary care givers using pyrosequencing. PLoS ONE 2011, 6, e23503. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.F.; Evans, M.; Fitzsimmons, S.; Johnson, J.; Pearce, C.; Sheridan, M.J.; Wientzen, R.; Bowden, G. Pioneer oral streptococci produce immunoglobulin A1 protease. Infect. Immun. 1994, 62, 2165–2168. [Google Scholar] [CrossRef] [Green Version]
- Caufield, P.W.; Cutter, G.R.; Dasanayake, A.P. Initial acquisition of mutans streptococci by infants: Evidence for a discrete window of infectivity. J. Dent. Res. 1993, 72, 37–45. [Google Scholar] [CrossRef]
- Crielaard, W.; Zaura, E.; Schuller, A.A.; Huse, S.M.; Montijn, R.C.; Keijser, B.J.F. Exploring the oral microbiota of children at various developmental stages of their dentition in the relation to their oral health. BMC Med. Genom. 2011, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Krzyściak, W.; Jurczak, A.; Piątkowski, J. The Role of Human Oral Microbiome in Dental Biofilm Formation. In Microbial Biofilms—Importance and Applications; Intech Open: London, UK, 2016; pp. 329–382. [Google Scholar]
- Van Houte, J.; Lopman, J.; Kent, R. The predominant cultivable flora of sound and carious human root surfaces. J. Dent. Res. 1994, 73, 1727–1734. [Google Scholar] [CrossRef]
- Jurczak, A.; Kościelniak, D.; Papież, M.; Vyhouskaya, P.; Krzyściak, W. A study on β-defensin-2 and histatin-5 as a diagnostic marker of early childhood caries progression. Biol. Res. 2015, 48, 61. [Google Scholar] [CrossRef] [Green Version]
- Gross, E.L.; Leys, E.J.; Gasparovich, S.R.; Firestone, N.D.; Schwartzbaum, J.A.; Janies, D.A.; Asnani, K.; Griffen, A.L. Bacterial 16S sequence analysis of severe caries in young permanent teeth. J. Clin. Microbiol. 2010, 48, 4121–4128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, A.C.R.; Mathney, J.M.J.; Kent, R.L.; Chalmers, N.I.; Hughes, C.V.; Loo, C.Y.; Pradhan, N.; Kanasi, E.; Hwang, J.; Dahlan, M.A.; et al. Cultivable anaerobic microbiota of severe early childhood caries. J. Clin. Microbiol. 2011, 49, 1464–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brady, L.J.; Maddocks, S.E.; Larson, M.R.; Forsgren, N.; Persson, K.; Deivanayagam, C.C.; Jenkinson, H.F. The changing faces of Streptococcus antigen I/II polypeptide family adhesins. Mol. Microbiol. 2010, 77, 276–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mombelli, A.; Gusberti, F.A.; van Oosten, M.A.; Lang, N.P. Gingival health and gingivitis development during puberty. A 4-year longitudinal study. J. Clin. Periodontol. 1989, 16, 451–456. [Google Scholar] [CrossRef]
- Lee, H.-C.; Yu, S.-C.; Lo, Y.-C.; Lin, I.-H.; Tung, T.-H.; Huang, S.-Y. A high linoleic acid diet exacerbates metabolic responses and gut microbiota dysbiosis in obese rats with diabetes mellitus. Food Funct. 2019, 10, 786–798. [Google Scholar] [CrossRef]
- Hsu, T.M.; Konanur, V.R.; Taing, L.; Usui, R.; Kayser, B.D.; Goran, M.I.; Kanoski, S.E. Effects of sucrose and high fructose corn syrup consumption on spatial memory function and hippocampal neuroinflammation in adolescent rats. Hippocampus 2015, 25, 227–239. [Google Scholar] [CrossRef]
- Hetherington, M.M.; Cecil, J.E.; Jackson, D.M.; Schwartz, C. Feeding infants and young children. From guidelines to practice. Appetite 2011, 57, 791–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Sugar in Infants, Children and Adolescents: A Position Paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, A.; Christian, B.; Masood, M.; Calache, H.; Carpenter, L.; Gibbs, L.; Gussy, M. Natural history of dental caries: Baseline characteristics of the VicGen birth cohort study. Int. J. Paediatr. Dent. 2020, 30, 334–341. [Google Scholar] [CrossRef] [Green Version]
- Giacaman, R.A. Sugars and beyond. The role of sugars and the other nutrients and their potential impact on caries. Oral Dis. 2018, 24, 1185–1197. [Google Scholar] [CrossRef] [PubMed]
- Janket, S.-J.; Benwait, J.; Isaac, P.; Ackerson, L.K.; Meurman, J.H. Oral and Systemic Effects of Xylitol Consumption. Caries Res. 2019, 53, 491–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rafeek, R.; Carrington, C.V.F.; Gomez, A.; Harkins, D.; Torralba, M.; Kuelbs, C.; Addae, J.; Moustafa, A.; Nelson, K.E. Xylitol and sorbitol effects on the microbiome of saliva and plaque. J. Oral Microbiol. 2019, 11, 1536181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Štšepetova, J.; Truu, J.; Runnel, R.; Nõmmela, R.; Saag, M.; Olak, J.; Nõlvak, H.; Preem, J.-K.; Oopkaup, K.; Krjutškov, K.; et al. Impact of polyols on Oral microbiome of Estonian schoolchildren. BMC Oral Health 2019, 19, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, P.; Moore, D.; Ahmed, F.; Sharif, M.O.; Worthington, H. V Xylitol-containing products for preventing dental caries in children and adults. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Lohner, S.; Toews, I.; Meerpohl, J.J. Health outcomes of non-nutritive sweeteners: Analysis of the research landscape. Nutr. J. 2017, 16, 55. [Google Scholar] [CrossRef] [Green Version]
- Kułaga, Z.; Różdżyńska-Świątkowska, A.; Grajda, A.; Gurzkowska, B.; Wojtyło, M.; Góźdź, M.; Świąder-Leśniak, A.; Litwin, M. Siatki centylowe dla oceny wzrastania i stanu odżywienia polskich dzieci i młodzieży od urodzenia do 18 roku życia. Stand. Med. 2015, 12, 119–135. [Google Scholar]
- Sheiham, A.; James, W.P.T. Diet and Dental Caries: The Pivotal Role of Free Sugars Reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef]
- Zeng, L.; Zeng, Y.; Zhou, Y.; Wen, J.; Wan, L.; Ou, X.; Zhou, X. Diet and lifestyle habits associated with caries in deciduous teeth among 3- to 5-year-old preschool children in Jiangxi province, China. BMC Oral Health 2018, 18, 224. [Google Scholar] [CrossRef] [Green Version]
- ISO 3972: 2011: Sensory Analysis—Methodology—Method of Investigating Sensitivity of Taste, 3rd ed.; ISO: Geneva, Switzerland, 2011.
- WHO. Oral Health Surveys: Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Petersen, P.; Bourgeois, D.; Bratthall, D.; Ogawa, H.; World Health Organization. Oral Health Surveys—Basic Methods; WHO: Geneva, Switzerland, 2005; Volume 83, pp. 686–693. [Google Scholar]
- Struzycka, I. The oral microbiome in dental caries. Polish J. Microbiol. 2014, 63, 127–135. [Google Scholar] [CrossRef]
- Feron, G. Unstimulated saliva: Background noise in taste molecules. J. Texture Stud. 2019, 50, 6–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forssten, S.D.; Björklund, M.; Ouwehand, A.C. Streptococcus mutans, caries and simulation models. Nutrients 2010, 2, 290–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciel, S.M.; Marcenes, W.; Sheiham, A. The relationship between sweetness preference, levels of salivary mutans streptococci and caries experience in Brazilian pre-school children. Int. J. Paediatr. Dent. 2001, 11, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.; So, P.W.; Carpenter, G.H. Intraoral Microbial Metabolism and Association with Host Taste Perception. J. Dent. Res. 2020, 99, 739–745. [Google Scholar] [CrossRef]
- Pidamale, R.; Sowmya, B.; Thomas, A.; Jose, T.; Madhusudan, K.K.; Prasad, G. Association between early childhood caries, streptococcus mutans level and genetic sensitivity levels to the bitter taste of, 6-N propylthiouracil among the children below 71 months of age. Dent. Res. J. 2012, 9, 730–734. [Google Scholar]
- Dashper, S.G.; Mitchell, H.L.; Lê Cao, K.-A.; Carpenter, L.; Gussy, M.G.; Calache, H.; Gladman, S.L.; Bulach, D.M.; Hoffmann, B.; Catmull, D.V.; et al. Temporal development of the oral microbiome and prediction of early childhood caries. Sci. Rep. 2019, 9, 19732. [Google Scholar] [CrossRef]
- Cattaneo, C.; Gargari, G.; Koirala, R.; Laureati, M.; Riso, P.; Guglielmetti, S.; Pagliarini, E. New insights into the relationship between taste perception and oral microbiota composition. Sci. Rep. 2019, 9, 3549. [Google Scholar] [CrossRef] [Green Version]
- Szczeklik, K.; Owczarek, D.; Cibor, D.; Cześnikiewicz-Guzik, M.; Krzyściak, P.; Krawczyk, A.; Mach, T.; Karczewska, E.; Krzyściak, W. Relative homogeneity of oral bacterial oral in Crohn’s disease compared to ulcerative colitis and its connections with antioxidant defense—Preliminary report. Folia Med. Cracov. 2019, 59, 15–35. [Google Scholar]
- Krzyściak, W.; Pluskwa, K.K.; Piątkowski, J.; Krzyściak, P.; Jurczak, A.; Kościelniak, D.; Skalniak, A. The usefulness of biotyping in the determination of selected pathogenicity determinants in Streptococcus mutans. BMC Microbiol. 2014, 14, 194. [Google Scholar] [CrossRef] [Green Version]
- Arid, J.; Antunes, L.A.A.; de Koch, L.F.A.; Evangelista, S.S.; Vasconcelos, K.R.F.; Brancher, J.A.; Gabardo, M.C.L.; Milani, A.J.; Dutra, A.L.T.; Antunes, L.S.; et al. Association of taste receptor gene polymorphisms with dental caries. Braz. Oral Res. 2020, 34, e055. [Google Scholar] [CrossRef]
- Izakovicova Holla, L.; Borilova Linhartova, P.; Lucanova, S.; Kastovsky, J.; Musilova, K.; Bartosova, M.; Kukletova, M.; Kukla, L.; Dusek, L. GLUT2 and TAS1R2 Polymorphisms and Susceptibility to Dental Caries. Caries Res. 2015, 49, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Esberg, A.; Haworth, S.; Holgerson, P.L.; Johansson, I. Allelic Variation in Taste Genes Is Associated with Taste and Diet Preferences and Dental Caries. Nutrients 2019, 11, 1491. [Google Scholar] [CrossRef] [Green Version]
- Chi, D.L.; Scott, J.M. Added Sugar and Dental Caries in Children: A Scientific Update and Future Steps. Dent. Clin. N. Am. 2019, 63, 17–33. [Google Scholar] [CrossRef]
- Abdel Rahman, A.; Jomaa, L.; Kahale, L.A.; Adair, P.; Pine, C. Effectiveness of behavioral interventions to reduce the intake of sugar-sweetened beverages in children and adolescents: A systematic review and meta-analysis. Nutr. Rev. 2018, 76, 88–107. [Google Scholar] [CrossRef] [PubMed]
- Nezami, B.T.; Lytle, L.A.; Ward, D.S.; Ennett, S.T.; Tate, D.F. Effect of the Smart Moms intervention on targeted mediators of change in child sugar-sweetened beverage intake. Public Health 2020, 182, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Martin-Kerry, J.; Gussy, M.; Gold, L.; Calache, H.; Boak, R.; Smith, M.; de Silva, A. Are Australian parents following feeding guidelines that will reduce their child’s risk of dental caries? Child. Care. Health Dev. 2020, 46, 495–505. [Google Scholar] [CrossRef]
- Slabsinskiene, E.; Milciuviene, S.; Narbutaite, J.; Vasiliauskiene, I.; Andruskeviciene, V.; Bendoraitiene, E.A.; Saldūnaite, K. Severe early childhood caries and behavioral risk factors among 3-year-old children in Lithuania. Medicina 2010, 46, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Costa, E.L.; Costa, J.F.; Santos, M.P.; Ladeira, L.L.C.; Silva, R.A.; Ribeiro, C.C.C. Streptococcus mutans in Mother-Child Dyads and Early Childhood Caries: Examining Factors Underlying Bacterial Colonization. Caries Res. 2018, 51, 582–589. [Google Scholar] [CrossRef]
- Jamel, H.A.; Sheiham, A.; Watt, R.G.; Cowell, C.R. Sweet preference, consumption of sweet tea and dental caries; studies in urban and rural Iraqi populations. Int. Dent. J. 1997, 47, 213–217. [Google Scholar] [CrossRef]
- Furquim, T.R.D.; Poli-Frederico, R.C.; Maciel, S.M.; Gonini-Júnior, A.; Walter, L.R.F. Sensitivity to bitter and sweet taste perception in schoolchildren and their relation to dental caries. Oral Health Prev. Dent. 2010, 8, 253–259. [Google Scholar]
- Ashi, H.; Campus, G.; Klingberg, G.; Forslund, H.B.; Lingström, P. Childhood obesity in relation to sweet taste perception and dental caries—A cross-sectional multicenter study. Food Nutr. Res. 2019, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bretz, W.A.; Corby, P.M.A.; Melo, M.R.; Coelho, M.Q.; Costa, S.M.; Robinson, M.; Schork, N.J.; Drewnowski, A.; Hart, T.C. Heritability estimates for dental caries and sucrose sweetness preference. Arch. Oral Biol. 2006, 51, 1156–1160. [Google Scholar] [CrossRef]
- World Health Organization. Ending Childhood Dental Caries; WHO implementation manual: Geneva, Switzerland, 2019. [Google Scholar]
- Iatridi, V.; Hayes, J.E.; Yeomans, M.R. Quantifying Sweet Taste Liker Phenotypes: Time for Some Consistency in the Classification Criteria. Nutrients 2019, 11, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feeney, E.; O’Brien, S.; Scannell, A.; Markey, A.; Gibney, E.R. Genetic variation in taste perception: Does it have a role in healthy eating? Proc. Nutr. Soc. 2011, 70, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Basil, M.; Maibach, E.; Goldberg, J.; Snyder, D. Why Americans eat what they do: Taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. J. Am. Diet. Assoc. 1998, 98, 1118–1126. [Google Scholar] [CrossRef]
- Jamar, G.; Ribeiro, D.A.; Pisani, L.P. High-fat or high-sugar diets as trigger inflammation in the microbiota-gut-brain axis. Crit. Rev. Food Sci. Nutr. 2020, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Jayasinghe, S.N.; Kruger, R.; Walsh, D.C.I.; Cao, G.; Rivers, S.; Richter, M.; Breier, B.H. Is Sweet Taste Perception Associated with Sweet Food Liking and Intake? Nutrients 2017, 9, 750. [Google Scholar] [CrossRef] [Green Version]
- Wise, P.M.; Nattress, L.; Flammer, L.J.; Beauchamp, G.K. Reduced dietary intake of simple sugars alters perceived sweet taste intensity but not perceived pleasantness. Am. J. Clin. Nutr. 2016, 103, 50–60. [Google Scholar] [CrossRef]
- Cicerale, S.; Riddell, L.J.; Keast, R.S.J. The association between perceived sweetness intensity and dietary intake in young adults. J. Food Sci. 2012, 77, H31–H35. [Google Scholar] [CrossRef]
- Tan, S.-Y.; Tucker, R.M. Sweet Taste as a Predictor of Dietary Intake: A Systematic Review. Nutrients 2019, 11, 94. [Google Scholar] [CrossRef] [Green Version]
- Paes Leme, A.F.; Koo, H.; Bellato, C.M.; Bedi, G.; Cury, J.A. The role of sucrose in cariogenic dental biofilm formation—New insight. J. Dent. Res. 2006, 85, 878–887. [Google Scholar] [CrossRef]
- Zhao, W.; Li, W.; Lin, J.; Chen, Z.; Yu, D. Effect of sucrose concentration on sucrose-dependent adhesion and glucosyltransferase expression of S. mutans in children with severe early-childhood caries (S-ECC). Nutrients 2014, 6, 3572–3586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, J.-N.; Jung, J.-E.; Lee, M.-H.; Choi, H.-M.; Jeon, J.-G. Sucrose challenges to Streptococcus mutans biofilms and the curve fitting for the biofilm changes. FEMS Microbiol. Ecol. 2018, 94, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.; Scoffield, J.; Wu, R.; Deivanayagam, C.; Zou, J.; Wu, H. Antigen I/II mediates interactions between Streptococcus mutans and Candida albicans. Mol. Oral Microbiol. 2018, 33, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Zhan, L. Rebalancing the Caries Microbiome Dysbiosis: Targeted Treatment and Sugar Alcohols. Adv. Dent. Res. 2018, 29, 110–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blander, J.M.; Longman, R.S.; Iliev, I.D.; Sonnenberg, G.F.; Artis, D. Regulation of inflammation by microbiota interactions with the host. Nat. Immunol. 2017, 18, 851–860. [Google Scholar] [CrossRef]
- Shang, L.; Deng, D.; Buskermolen, J.K.; Roffel, S.; Janus, M.M.; Krom, B.P.; Crielaard, W.; Gibbs, S. Commensal and Pathogenic Biofilms Alter Toll-Like Receptor Signaling in Reconstructed Human Gingiva. Front. Cell. Infect. Microbiol. 2019, 9, 282. [Google Scholar] [CrossRef] [Green Version]
- Belibasakis, G.N.; Bostanci, N.; Marsh, P.D.; Zaura, E. Applications of the oral microbiome in personalized dentistry. Arch. Oral Biol. 2019, 104, 7–12. [Google Scholar] [CrossRef]
- Johansson, I.; Witkowska, E.; Kaveh, B.; Lif Holgerson, P.; Tanner, A.C.R. The Microbiome in Populations with a Low and High Prevalence of Caries. J. Dent. Res. 2016, 95, 80–86. [Google Scholar] [CrossRef]
- Harth-Chu, E.N.; Alves, L.A.; Theobaldo, J.D.; Salomão, M.F.; Höfling, J.F.; King, W.F.; Smith, D.J.; Mattos-Graner, R.O. PcsB Expression Diversity Influences on Streptococcus mitis Phenotypes Associated With Host Persistence and Virulence. Front. Microbiol. 2019, 10, 2567. [Google Scholar] [CrossRef] [Green Version]
- Banas, J.A.; Zhu, M.; Dawson, D.V.; Blanchette, D.R.; Drake, D.R.; Gu, H.; Frost, R.; McCaulley, G.; Levy, S.M. Acidogenicity and acid tolerance of Streptococcus oralis and Streptococcus mitis isolated from plaque of healthy and incipient caries teeth. J. Oral Microbiol. 2016, 8, 32940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, Y.Q.; Lacy, K.; Keast, R. The role of sweet taste in satiation and satiety. Nutrients 2014, 6, 3431–3450. [Google Scholar] [CrossRef] [Green Version]
- Ashi, H.; Campus, G.; Bertéus Forslund, H.; Hafiz, W.; Ahmed, N.; Lingström, P. The Influence of Sweet Taste Perception on Dietary Intake in Relation to Dental Caries and BMI in Saudi Arabian Schoolchildren. Int. J. Dent. 2017, 2017, 4262053. [Google Scholar] [CrossRef] [PubMed]
- Lanfer, A.; Knof, K.; Barba, G.; Veidebaum, T.; Papoutsou, S.; de Henauw, S.; Soós, T.; Moreno, L.A.; Ahrens, W.; Lissner, L. Taste preferences in association with dietary habits and weight status in European children: Results from the IDEFICS study. Int. J. Obes. 2012, 36, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quadri, F.A.; Hendriyani, H.; Pramono, A.; Jafer, M. Knowledge, attitudes and practices of sweet food and beverage consumption and its association with dental caries among schoolchildren in Jazan, Saudi Arabia. East. Mediterr. Health J. 2015, 21, 403–411. [Google Scholar] [CrossRef]
- Deo, P.N.; Deshmukh, R. Oral microbiome: Unveiling the fundamentals. J. Oral Maxillofac. Pathol. 2019, 23, 122–128. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Sucrose (g/L) |
|---|
| 0.34 |
| 0.55 |
| 0.94 |
| 1.56 |
| 2.59 |
| 4.32 |
| 7.20 |
| 12.00 |
| Total N = 63. | Controls n = 31 | With Caries n = 32 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| X | SD | Me | X | SD | Me | X | SD | Me | p | |
| Age | 4.76 | 1.18 | 5.00 | 4.79 | 1.28 | 5.00 | 4.73 | 1.09 | 5.00 | 0.831 A |
| Body mass (kg) | 18.84 | 4.58 | 18.00 | 19.47 | 5.39 | 19.00 | 18.23 | 3.62 | 17.75 | 0.491 B |
| Height (cm) | 111.11 | 12.16 | 110.00 | 110.10 | 13.67 | 109.00 | 112.09 | 10.63 | 110.00 | 0.519 A |
| Total | Controls | With Caries | Chi-Square Test | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BMI | n | % | Cumulative % | n | % | Cumulative % | n | % | Cumulative % | |
| Underweight | 20 | 31.7 | 31.7 | 8 | 25.8 | 25.8 | 12 | 37.5 | 37.5 | |
| Normal weight | 33 | 52.4 | 84.1 | 15 | 48.4 | 74.2 | 18 | 56.3 | 93.8 | 0.0575 |
| Overweight | 9 | 14.3 | 98.4 | 8 | 25.8 | 74.2 | 1 | 3.1 | 96.9 | |
| Obesity | 1 | 1.6 | 100.0 | 0 | 0.00 | 100.0 | 1 | 3.1 | 100.0 | |
| Total | 63 | 100.0 | 31 | 100.0 | 32 | 100.0 | ||||
| Total | Controls | With Caries | Chi-Square Test | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sweets intake | n | % | Cumulative % | n | % | Cumulative % | n | % | Cumulative % | |
| No | 9 | 14.3 | 14.3 | 9 | 29.0 | 29.0 | 0 | 0 | 0.0 | |
| Daily | 18 | 28.6 | 42.9 | 17 | 54.8 | 83.9 | 1 | 3.1 | 3.1 | <0.0001 |
| Once a day | 21 | 33.3 | 76.2 | 3 | 9.7 | 93.5 | 18 | 56.3 | 59.4 | |
| Several times a day | 15 | 23.8 | 100.0 | 2 | 6.5 | 100.0 | 13 | 40.6 | 100.0 | |
| Total | 63 | 100.0 | 31 | 100.0 | 32 | 100.0 | ||||
| Variables | Category | % | |
|---|---|---|---|
| Sucrose | Sucrose | ||
| <4 mg/L | >4 mg/L | ||
| Caries | no | 75.9 | 26.5 |
| yes | 24.1 | 73.5 | |
| OR | 1 | 8.73 | |
| 95% CI | 2.72–27.99 | ||
| BMI (overweight or obesity) | no | 79.3 | 88.2 |
| yes | 20.7 | 11.8 | |
| OR | 1 | 0.51 | |
| 95% CI | 0.12-2.08 | ||
| S. mutans presence | no | 75.9 | 23.5 |
| yes | 24.1 | 76.5 | |
| OR | 1 | 10.21 | |
| 95% CI | 3.11–33.44 | ||
| Consumption of sweets | no | 69 | 20.6 |
| (once a day or several times a day) | yes | 31 | 79.4 |
| OR | 1 | 8.57 | |
| 95% CI | 2.67–27.56 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurczak, A.; Jamka-Kasprzyk, M.; Bębenek, Z.; Staszczyk, M.; Jagielski, P.; Kościelniak, D.; Gregorczyk-Maga, I.; Kołodziej, I.; Kępisty, M.; Kukurba-Setkowicz, M.; et al. Differences in Sweet Taste Perception and Its Association with the Streptococcus mutans Cariogenic Profile in Preschool Children with Caries. Nutrients 2020, 12, 2592. https://doi.org/10.3390/nu12092592
Jurczak A, Jamka-Kasprzyk M, Bębenek Z, Staszczyk M, Jagielski P, Kościelniak D, Gregorczyk-Maga I, Kołodziej I, Kępisty M, Kukurba-Setkowicz M, et al. Differences in Sweet Taste Perception and Its Association with the Streptococcus mutans Cariogenic Profile in Preschool Children with Caries. Nutrients. 2020; 12(9):2592. https://doi.org/10.3390/nu12092592
Chicago/Turabian StyleJurczak, Anna, Małgorzata Jamka-Kasprzyk, Zuzanna Bębenek, Małgorzata Staszczyk, Paweł Jagielski, Dorota Kościelniak, Iwona Gregorczyk-Maga, Iwona Kołodziej, Magdalena Kępisty, Magdalena Kukurba-Setkowicz, and et al. 2020. "Differences in Sweet Taste Perception and Its Association with the Streptococcus mutans Cariogenic Profile in Preschool Children with Caries" Nutrients 12, no. 9: 2592. https://doi.org/10.3390/nu12092592
APA StyleJurczak, A., Jamka-Kasprzyk, M., Bębenek, Z., Staszczyk, M., Jagielski, P., Kościelniak, D., Gregorczyk-Maga, I., Kołodziej, I., Kępisty, M., Kukurba-Setkowicz, M., Bryll, A., & Krzyściak, W. (2020). Differences in Sweet Taste Perception and Its Association with the Streptococcus mutans Cariogenic Profile in Preschool Children with Caries. Nutrients, 12(9), 2592. https://doi.org/10.3390/nu12092592