Potato Preload Mitigated Postprandial Glycemic Excursion in Healthy Subjects: An Acute Randomized Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects Recruitment
2.2. Study Design
2.3. Meal Preparation
2.4. Measurements of Blood Glucose and Satiety
2.5. Data Processing and Statistical Analysis
3. Results
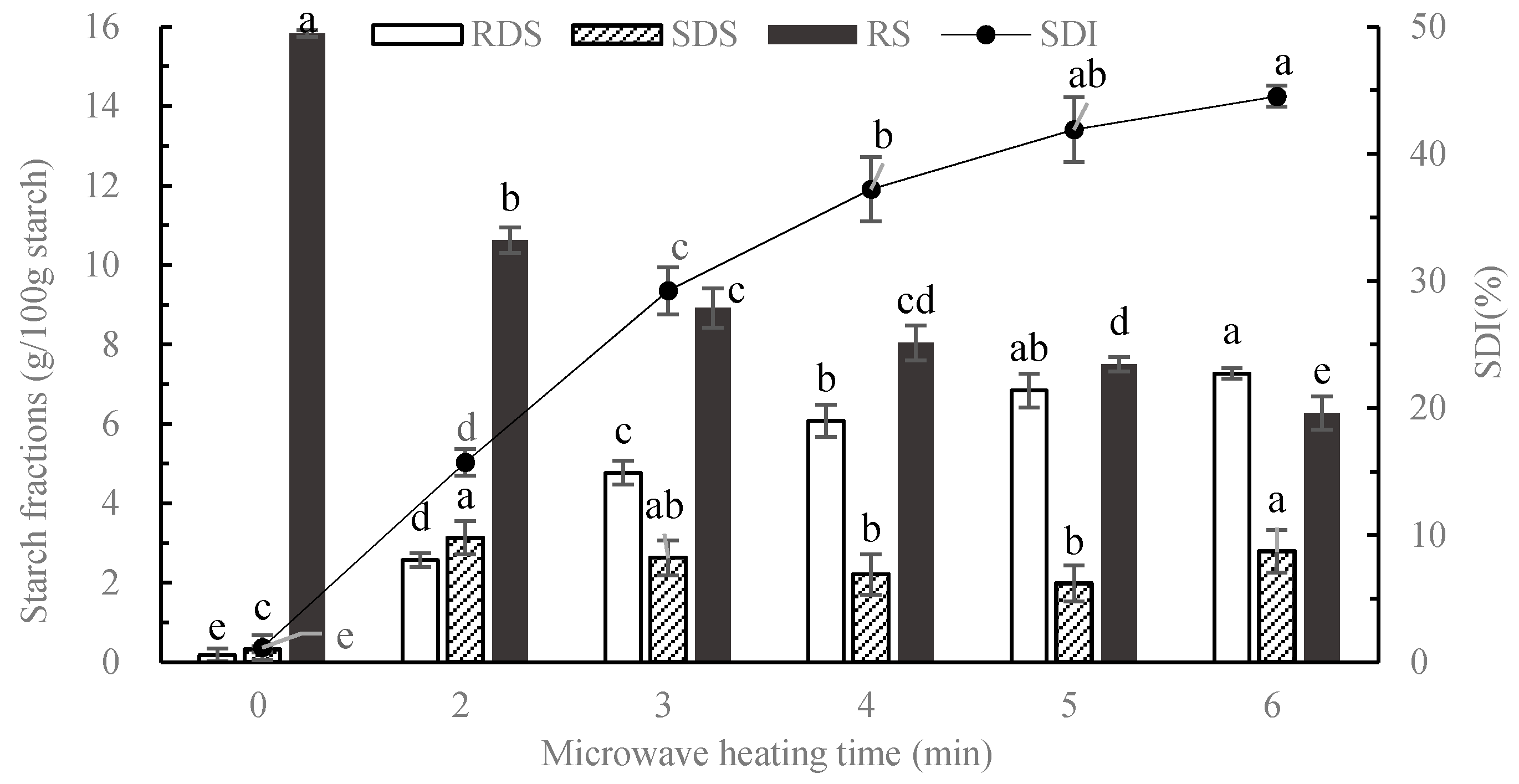
3.1. In Vitro Starch Digestion of Cooked Potato
3.2. Glycemic Responses
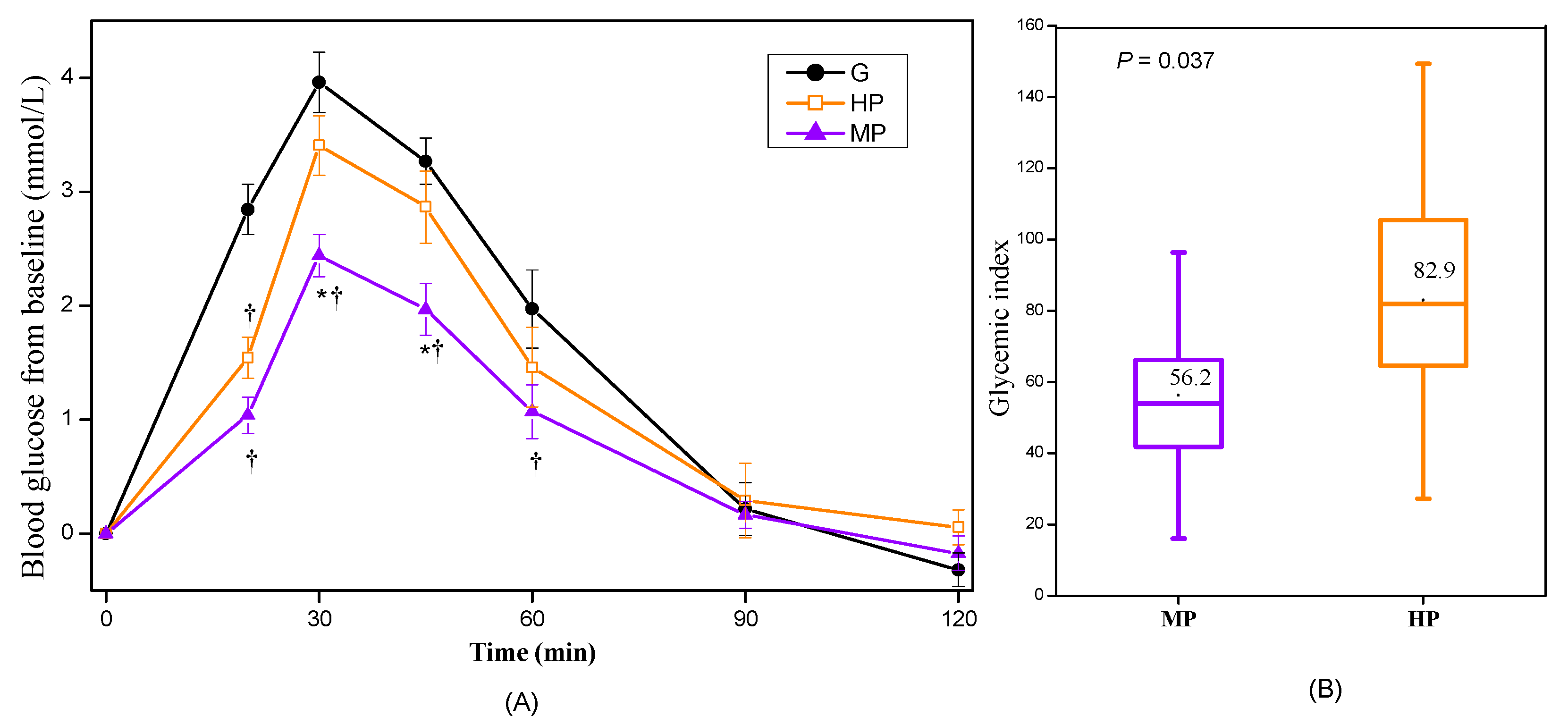
3.2.1. Glycemic Responses of Cooked Potatoes
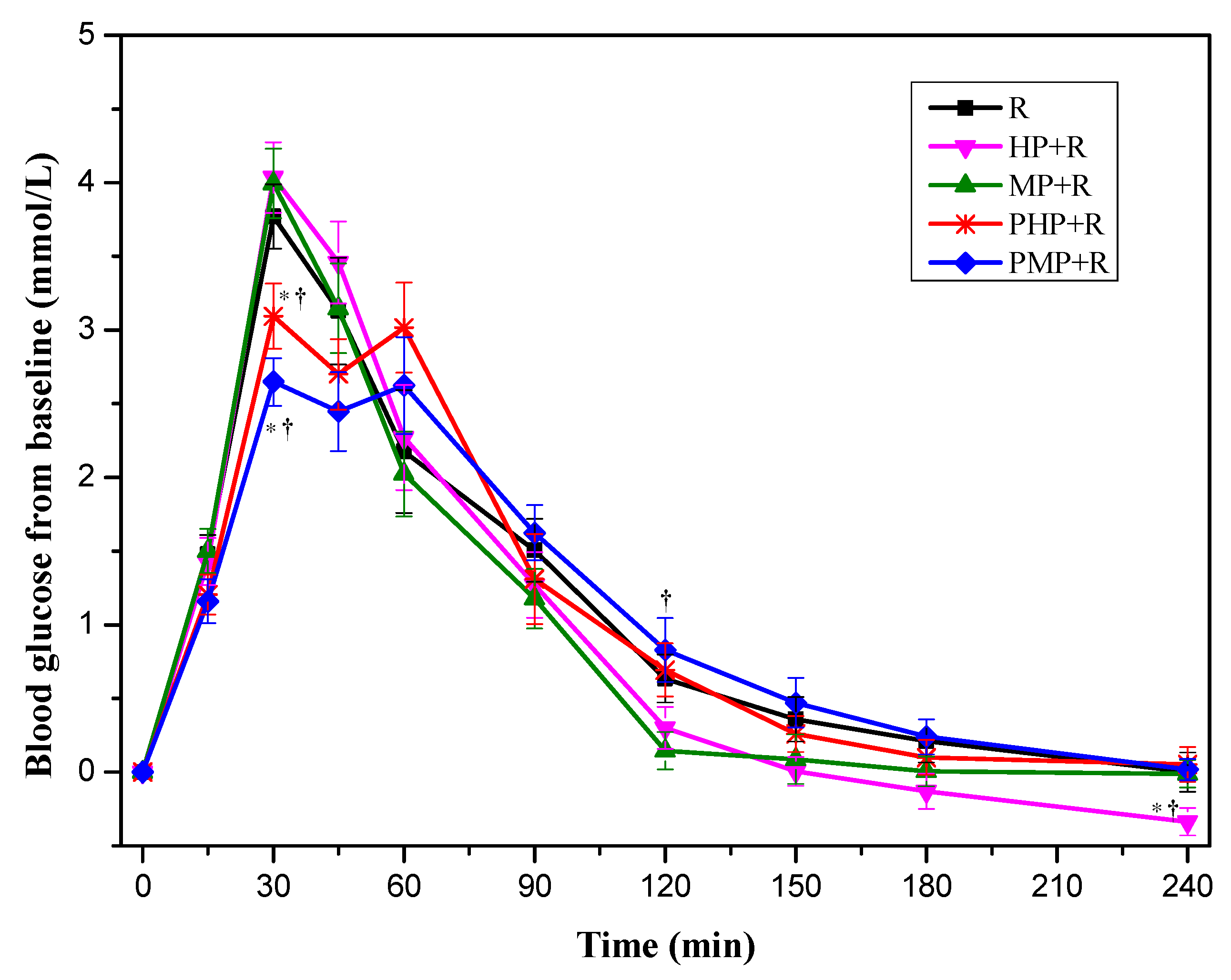
3.2.2. Glycemic Response of Mixed Meals Containing Potatoes and Rice
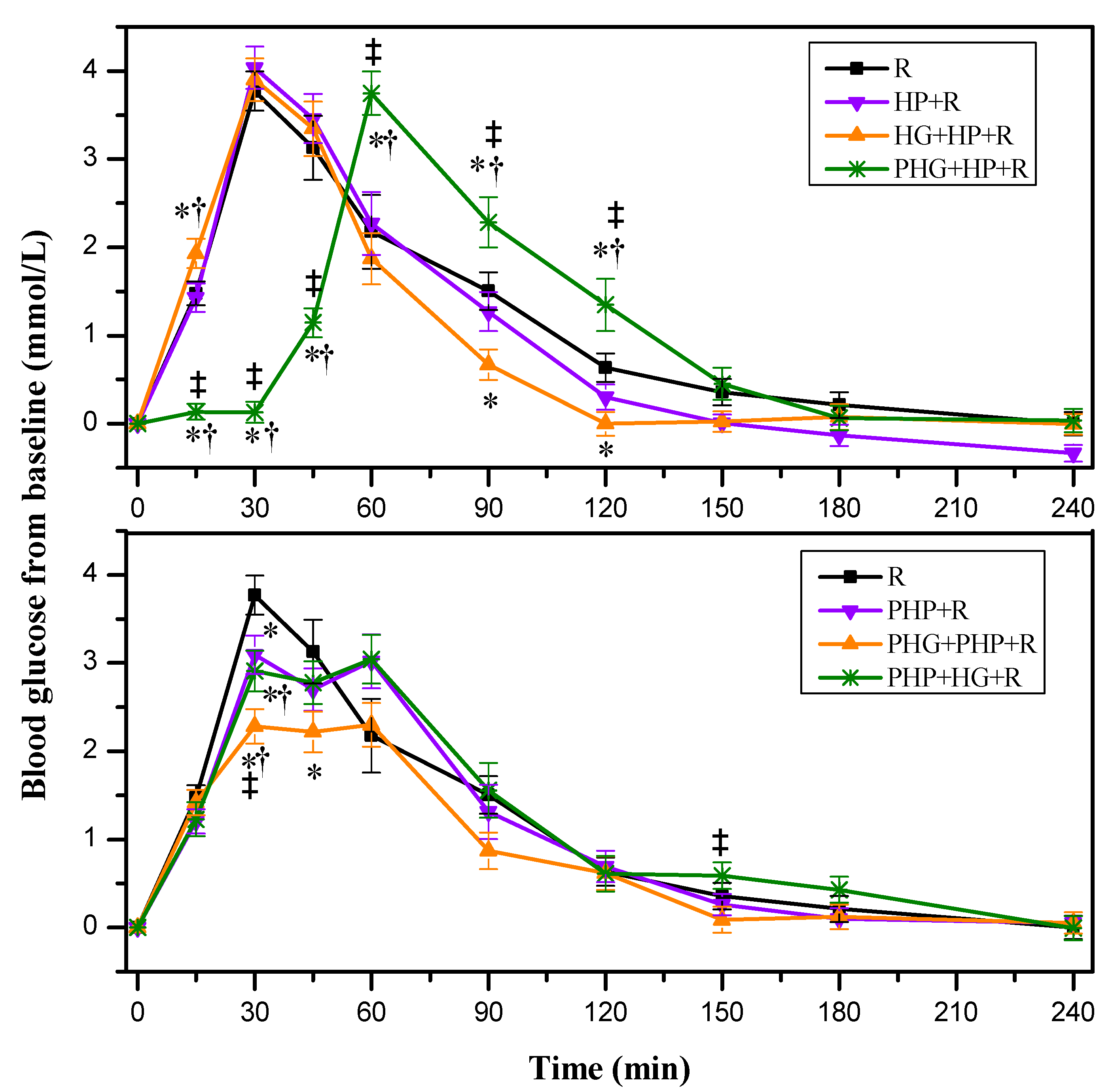
3.2.3. Glycemic Response of Mixed Meals Containing HG, Potatoes and Rice
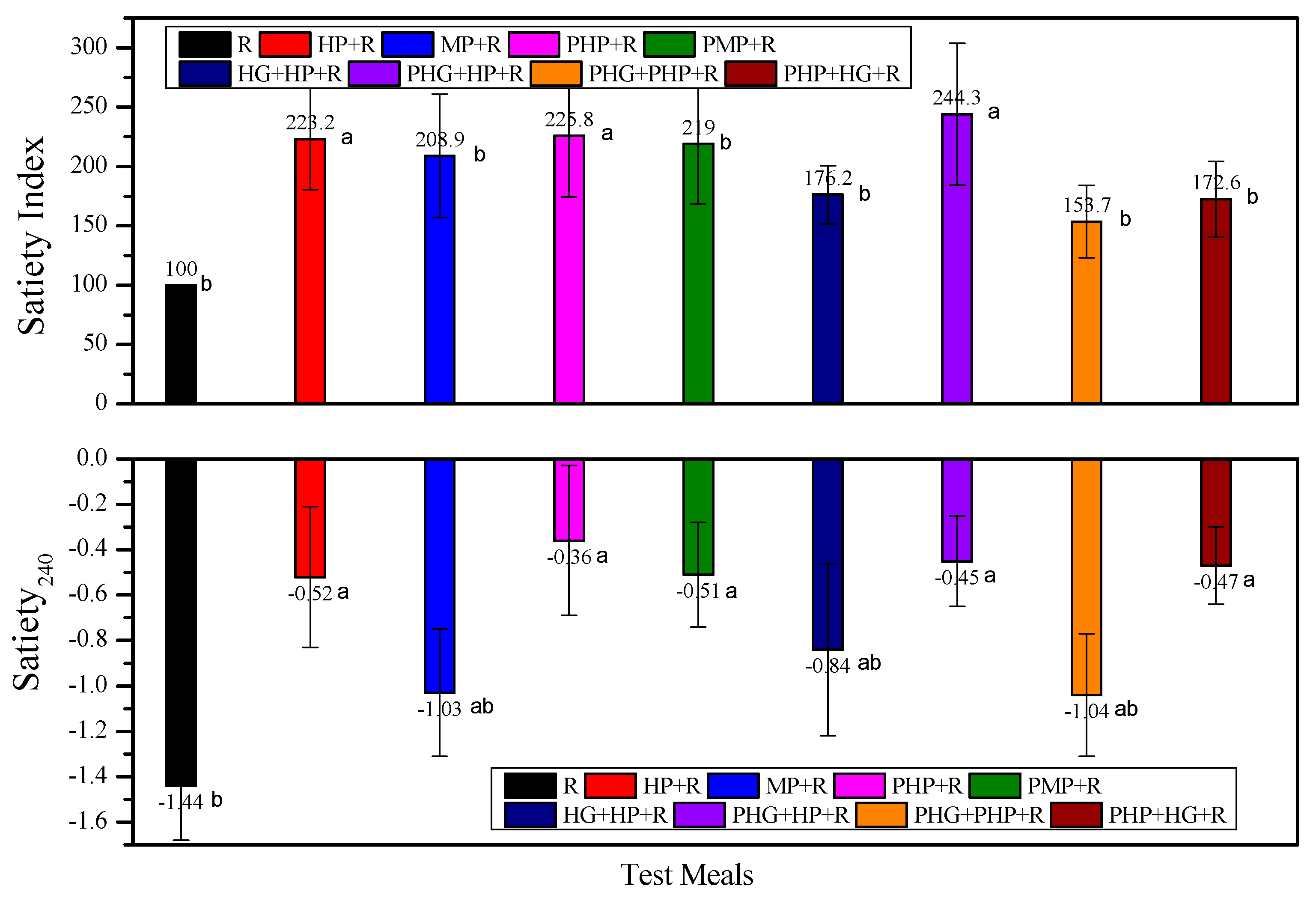
3.3. Subjective Appetite
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Ch’Ng, L.Z.; Barakatun-Nisak, M.Y.; Wan, Z.W.; Abas, F.; Wahab, N.A. Nutritional strategies in managing postmeal glucose for type 2 diabetes: A narrative review. Diabetes Metab. Syndr. 2019, 13, 2339–2345. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.E.; Phillips, L.K.; Wu, T.; Bound, M.J.; Rayner, C.K. A whey/guar “preload” improves postprandial glycaemia and HbA1c in type 2 diabetes—A 12-week, single-blind, randomized, placebo-controlled trial. Diabetes Obes. Metab. 2018, 21, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Stevens, J.E.; Cukier, K.; Maddox, A.F.; Wishart, J.M.; Jones, K.L.; Clifton, P.M.; Horowitz, M.; Rayner, C.K. Effects of a protein preload on gastric emptying, glycemia, and gut hormones after a carbohydrate meal in diet-controlled type 2 diabetes. Diabetes Care 2009, 32, 1600–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubransky, A.; Monro, J.; Mishra, S.; Yu, H.; Haszard, J.J.; Venn, B.J. Postprandial glycaemic, hormonal and satiety responses to rice and kiwifruit preloads in Chinese adults: A randomised controlled crossover trial. Nutrients 2018, 10, 1110. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Zhao, W.; Wang, L.; Fan, Z.; Zhu, R.; Wu, Y.; Zhou, Y. Apple preload halved the postprandial glycaemic response of rice meal in healthy subjects. Nutrients 2019, 11, 2912. [Google Scholar] [CrossRef] [Green Version]
- Brand-Miller, J.C.; Astrup, A.; Buyken, A.E. Low vs. high glycemic index diet. Jama J. Am. Med. Assoc. 2015, 313, 1371–1372. [Google Scholar] [CrossRef]
- Augustin, L.S.A.; Kendall, C.W.C.; Jenkins, D.J.A.; Willett, W.C.; Astrup, A.; Barclay, A.W.; Bjorck, I.; Brand-Miller, J.C.; Brighenti, F.; Buyken, A.E.; et al. Glycemic index, glycemic load and glycemic response: An International Scientific Consensus Summit from the International Carbohydrate Quality Consortium (ICQC). Nutr. Metab. Cardiovasc. 2015, 25, 795–815. [Google Scholar] [CrossRef] [Green Version]
- Beals, K.A. Potatoes, Nutrition and Health. Am. J. Potato Res. 2019, 96, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; You, D.; Lu, N.; Duan, D.; Feng, X.; Astell-Burt, T.; Zhu, P.; Han, L.; Duan, S.; Zou, Z. Potatoes consumption and risk of type 2 diabetes: A meta-analysis. Iran. J. Public Health 2018, 47, 1627–1635. [Google Scholar]
- Ek, K.L.; Wang, S.; Copeland, L.; Brand-Miller, J.C. Discovery of a low-glycaemic index potato and relationship with starch digestion in vitro. Br. J. Nutr. 2014, 111, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leeman, M.; Ostman, E.; Bjorck, I. Glycaemic and satiating properties of potato products. Eur. J. Clin. Nutr. 2008, 62, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.; Monro, J.; Hedderley, D. Effect of processing on slowly digestible starch and resistant starch in potato. Starch-Stärke 2008, 60, 500–507. [Google Scholar] [CrossRef]
- Chen, X.; Jiao, J.; Zhuang, P.; Wu, F.; Zhang, Y. Current intake levels of potatoes and all-cause mortality in China: A population-based nationwide study. Nutrition 2020, 81, 110902. [Google Scholar] [CrossRef] [PubMed]
- Johnston, E.A.; Petersen, K.S. and Kris-Etherton, P.M. Daily intake of non-fried potato does not affect markers of glycaemia and is associated with better diet quality compared with refined grains: A randomised, crossover study in healthy adults. Br. J. Nutr. 2020, 123, 1032–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez Pineda, M.A.; Artacho Martin-Lagos, R.; Lopez Garcia De La Serrana, H.; Lopez Martinez, M.C. Microwave ovens: Influence on the nutritional value of foods. Alimentaria 1994, 31, 41–44. [Google Scholar]
- Tian, J.; Chen, J.; Ye, X.; Chen, S. Health benefits of the potato affected by domestic cooking: A review. Food Chem. 2016, 202, 165–175. [Google Scholar] [CrossRef]
- Huang, J.; Hess, W.M.; Weber, D.J.; Purcell, A.E.; Huber, C.S. Scanning electron microscopy: Tissue characteristics and starch granule variations of potatoes after microwave and conductive heating. Food Struct. 1990, 9, 113–122. [Google Scholar]
- Nott, K.P.; Shaarani, S.M.; Hall, L.D. The effect of microwave heating on potato texture studied with magnetic resonance imaging. R. Soc. Chem. Spec. Publ. 2003, 286, 38–45. [Google Scholar]
- Wood, P.J.; Braaten, J.T.; Scott, F.W.; Riedel, D.; Poste, L.M. Comparisons of viscous properties of oat and guar gum and the effects of these and oat bran on glycemic index. J. Agric. Food Chem. 1990, 38, 753–757. [Google Scholar] [CrossRef]
- Reider, S.J.; Moosmang, S.; Tragust, J.; Trgovec-Greif, L.; Tragust, S.; Perschy, L.; Przysiecki, N.; Sturm, S.; Tilg, H.; Stuppner, H.; et al. Prebiotic effects of partially hydrolyzed guar gum on the composition and function of the human microbiota-Results from the PAGODA Trial. Nutrients 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Finley, J.W.; Soto-Vaca, A.; Heimbach, J.; Rao, T.P.; Juneja, L.R.; Slavin, J.; Fahey, G.C. Safety assessment and caloric value of partially hydrolyzed guar gum. J. Agric. Food Chem. 2013, 61, 1756–1771. [Google Scholar] [CrossRef] [PubMed]
- Yasukawa, Z.; Inoue, R.; Ozeki, M.; Okubo, T.; Takagi, T.; Honda, A.; Naito, Y. Effect of repeated consumption of partially hydrolyzed guar gum on fecal characteristics and gut microbiota: A randomized, double-blind, placebo-controlled, and parallel-group clinical trial. Nutrients 2019, 11, 2170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapoor, M.P.; Ishihara, N.; Okubo, T. Soluble dietary fibre partially hydrolysed guar gum markedly impacts on postprandial hyperglycaemia, hyperlipidaemia and incretins metabolic hormones over time in healthy and glucose intolerant subjects. J. Funct. Foods 2016, 24, 207–220. [Google Scholar] [CrossRef]
- Englyst, K.N.; Englyst, H.N.; Hudson, G.J.; Cole, T.J.; Cummings, J.H. Rapidly available glucose in foods: An in vitro measurement that reflects the glycemic response. Am. J. Clin. Nutr. 1999, 69, 448–454. [Google Scholar] [CrossRef]
- Flint, A.; Raben, A.; Blundell, J.E.; Astrup, A. Reproducibility, power and validity of visual analogue scares in assessment of appetite sensations in single test meal studies. Int. J. Obes. 2000, 24, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Blundell, J.; de Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; van der Knaap, H.; et al. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. 2010, 11, 251–270. [Google Scholar] [CrossRef] [Green Version]
- Englyst, H.N.; Kingman, S.M.; Cummings, J.H. Classification and measurement of nutritionally important starch fractions. Eur. J. Clin. Nutr. 1992, 46 (Suppl. S2), S33–S50. [Google Scholar]
- Service, F.J.; Nelson, R.L. Characteristics of Glycemic Stability. Diabetes Care 1980, 3, 58–62. [Google Scholar] [CrossRef]
- McDonnell, C.M.; Donath, S.M.; Vidmar, S.I.; Werther, G.A.; Cameron, F.J. A novel approach to continuous glucose analysis utilizing glycemic variation. Diabetes Technol. Ther. 2005, 7, 253–263. [Google Scholar] [CrossRef]
- Wolever, T.M. Effect of blood sampling schedule and method of calculating the area under the curve on validity and precision of glycaemic index values. Br. J. Nutr. 2004, 91, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institution, B.S. Food Products—Determination of the Glycaemic Index (GI) and Recommendation for Food Classification; ISO: Geneva, Switzerland, 2010. [Google Scholar]
- Wolever, T.M. Effect of macronutrients on the glycemic index. Am. J. Clin. Nutr. 2017, 106, 704–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, H.; Matthan, N.R.; Lichtenstein, A.H. Effect of macronutrients on the glycemic index Reply. Am. J. Clin. Nutr. 2017, 106, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Ramdath, D.D.; Padhi, E.; Hawke, A.; Sivaramalingam, T.; Tsao, R. The glycemic index of pigmented potatoes is related to their polyphenol content. Food Funct. 2014, 5, 909–915. [Google Scholar] [CrossRef]
- Karhunen, L.J.; Juvonen, K.R.; Huotari, A.; Purhonen, A.K.; Herzig, K.H. Effect of protein, fat, carbohydrate and fibre on gastrointestinal peptide release in humans. Regul. Pept. 2008, 149, 70–78. [Google Scholar] [CrossRef]
- Bindels, L.B.; Walter, J.; Ramer-Tait, A.E. Resistant starches for the management of metabolic diseases. Curr. Opin. Clin. Nutr. 2015, 18, 559–565. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Zhao, B.R.; Bound, M.J.; Checklin, H.L.; Bellon, M.; Little, T.J.; Young, R.L.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Effects of different sweet preloads on incretin hormone secretion, gastric emptying, and postprandial glycemia in healthy humans. Am. J. Clin. Nutr. 2012, 95, 78–83. [Google Scholar] [CrossRef]
- Akhavan, T.; Luhovyy, B.L.; Panahi, S.; Kubant, R.; Brown, P.H.; Anderson, G.H. Mechanism of action of pre-meal consumption of whey protein on glycemic control in young adults. J. Nutr. Biochem. 2014, 25, 36–43. [Google Scholar] [CrossRef]
- Raben, A.; Tagliabue, A.; Christensen, N.J.; Madsen, J.; Holst, J.J.; Astrup, A. Resistant starch: The effect on postprandial glycemia, hormonal response, and satiety. Am. J. Clin. Nutr. 1994, 60, 544–551. [Google Scholar] [CrossRef]
- Bodinham, C.L.; Al-Mana, N.M.; Smith, L.; Robertson, M.D. Endogenous plasma glucagon-like peptide-1 following acute dietary fibre consumption. Br. J. Nutr. 2013, 110, 1429–1433. [Google Scholar] [CrossRef] [Green Version]
- Liljeberg, H.; Bjorck, I. Effects of a low-glycaemic index spaghetti meal on glucose tolerance and lipaemia at a subsequent meal in healthy subjects. Eur. J. Clin. Nutr. 2000, 54, 24–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacNeil, S.; Rebry, R.M.; Tetlow, I.J.; Emes, M.J.; McKeown, B.; Graham, T.E. Resistant starch intake at breakfast affects postprandial responses in type 2 diabetics and enhances the glucose-dependent insulinotropic polypeptide—Insulin relationship following a second meal. Appl. Physiol. Nutr. Metab. 2013, 38, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Keenan, M.J.; Zhou, J.; Hegsted, M.; Pelkman, C.; Durham, H.A.; Coulon, D.B.; Martin, R.J. Role of resistant starch in improving gut health, adiposity, and insulin resistance. Adv. Nutr. 2015, 6, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bindels, L.B.; Segura Munoz, R.R.; Gomes-Neto, J.O.C.; Mutemberezi, V.; Martínez, I.; Salazar, N.; Cody, E.A.; Quintero-Villegas, M.I.; Kittana, H.; De, L.R.C.G. Resistant starch can improve insulin sensitivity independently of the gut microbiota. Microbiome 2017, 5, 12. [Google Scholar] [CrossRef] [Green Version]
- Vilsboll, T.; Krarup, T.; Sonne, J.; Madsbad, S.; Vølund, A.; Juul, A.G.; Holst, J.J. Incretin secretion in relation to meal size and body weight in healthy subjects and people with type 1 and type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. 2003, 88, 2706–2713. [Google Scholar] [CrossRef] [Green Version]
- Steinert, R.E.; Raederstorff, D.; Wolever, T.M.S. Effect of consuming oat bran mixed in water before a meal on glycemic responses in healthy humans-A pilot study. Nutrients 2016, 8, 524. [Google Scholar] [CrossRef] [Green Version]
- Anders, F.; Andrea, T.; Giovanni, P.; Martin, R.L. Effect of oral pre-meal administration of betaglucans on glycaemic control and variability in subjects with type 1 diabetes. Nutrients 2017, 9, 1004. [Google Scholar]
- Fabek, H.; Messerschmidt, S.; Brulport, V.; Goff, H.D. The effect of in vitro digestive processes on the viscosity of dietary fibres and their influence on glucose diffusion. Food Hydrocoll. 2014, 35, 718–726. [Google Scholar] [CrossRef]
- Yoon, S.; Chu, D.; Juneja, L.R. Physiological functions of partially hydrolyzed guar gum. J. Clin. Biochem. Nutr. 2006, 39, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Wolf, B.W.; Wolever, T.; Cai, C.S.; Bolognesi, C.; Radmard, R.; Maharry, K.S.; Garleb, K.A.; Hertzler, S.R.; Firkins, J.L. Effects of a beverage containing an enzymatically induced-viscosity dietary fiber, with or without fructose, on the postprandial glycemic response to a high glycemic index food in humans. Eur. J. Clin. Nutr. 2003, 57, 1120–1127. [Google Scholar] [CrossRef] [Green Version]
- Klosterbuer, A.S.; Greaves, K.A.; Slavin, J. Fiber intake inconsistently alters gut hormone levels in humans following acute or chronic intake. J. Food Res. 2012, 1, 255–273. [Google Scholar] [CrossRef] [Green Version]
- Holt, S.; Brand, J.; Soveny, C.; Hansky, J. Relationship of satiety to postprandial glycemic, insulin and cholecystokinin responses. Appetite 1992, 18, 129–141. [Google Scholar] [CrossRef]
- Kenda, C.W.C.; Esfahani, A.; Sanders, L.M.; Potter, S.M.; Vidgen, E. The effect of a preload meal containing resistant starch on spontaneous food intake and glucose and insulin responses. J. Food Technol. 2010, 8, 67–73. [Google Scholar]
- Reader, D.; Johnson, M.L.; Hollander, P.; Franz, M. The glycemic and insulinemic response of resistant starch in a food bar vs. two commercially available food bars in persons with type II diabetes mellitus. Diabetes 1997, 461, 975. [Google Scholar]
- Andersen, S.S.H.; Heller, J.M.F.; Hansen, T.T.; Raben, A. Comparison of low glycaemic index and high glycaemic index potatoes in relation to satiety: A single-blinded, randomised crossover study in humans. Nutrients 2018, 10, 1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, U.; Peterson, C.M.; Beyl, R.A.; Martin, C.K.; Ravussin, E. Resistant starch has no effect on appetite and food intake in individuals with prediabetes. J. Acad. Nutr. Diet. 2020, 120, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Al-Mana, N.; Robertson, M. Acute effect of resistant starch on food intake, appetite and satiety in overweight/obese males. Nutrients 2018, 10, 1993. [Google Scholar] [CrossRef] [Green Version]
- Ble-Castillo, J.L.; Juarez-Rojop, I.E.; Tovilla-Zarate, C.A.; Garcia-Vazquez, C.; Servin-Cruz, M.Z.; Rodriguez-Hernandez, A.; Araiza-Saldana, C.I.; Nolasco-Coleman, A.M.; Diaz-Zagoya, J.C. Acute consumption of resistant starch reduces food intake but has no effect on appetite ratings in healthy subjects. Nutrients 2017, 9, 696. [Google Scholar] [CrossRef] [Green Version]
- Boey, D.; Sainsbury, A.; Herzog, H. The role of peptide YY in regulating glucose homeostasis. Peptides 2007, 28, 395. [Google Scholar] [CrossRef] [Green Version]
- Rao, T.P. Role of guar fiber in appetite control. Physiol. Behav. 2016, 164, 277–283. [Google Scholar] [CrossRef]
- Willis, H.J.; Thomas, W.; Eldridge, A.L.; Harkness, L.; Green, H.; Slavin, J.L. Increasing doses of fiber do not influence short-term satiety or food intake and are inconsistently linked to gut hormone levels. Food Nutr. Res. 2010, 54, 5135. [Google Scholar] [CrossRef] [PubMed]
- Giuntini, E.B.; Sarda, F.A.H.; Lui, M.C.Y.; Tadini, C.C.; Lajolo, F.M.; Menezes, E.W. Gastrointestinal hormone modulation after a double-blind interventional study with unavailable carbohydrates. Food Res. Int. 2015, 77, 17–23. [Google Scholar] [CrossRef]
- Bhupathiraju, S.N.; Tobias, D.K.; Malik, V.S.; Pan, A.; Hruby, A.; Manson, J.E.; Willett, W.C.; Hu, F.B. Glycemic index, glycemic load, and risk of type 2 diabetes: Results from 3 large US cohorts and an updated meta-analysis. Am. J. Clin. Nutr. 2014, 100, 218–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Meals | Rice (g) | Potatoes (g) | HG (g) | Weight (g) | Protein (g) | Fat (g) | Soluble Fiber (g) | Insoluble Fiber (g) | Available CHO (g) | Energy (kcal) |
|---|---|---|---|---|---|---|---|---|---|---|
| Glucose (25 g AC) | - | - | - | 355.56 | - | - | - | - | 25.0 | 100.0 |
| HP | - | 110.0 | - | 355.56 | 3.4 | 0.1 | 0.9 | 1.6 | 25.0 | 114.5 |
| MP | - | 152.0 | - | 355.56 | 3.4 | 0.1 | 0.9 | 1.6 | 25.0 | 114.5 |
| Glucose (50 g AC) | - | - | - | 355.56 | - | - | - | - | 50.0 | 200.0 |
| Rice | 143.1 | - | - | 355.56 | 6.2 | 0.5 | 0.0 | 0.7 | 50.0 | 229.3 |
| HP + R | 100.2 | 66.0 | - | 355.56 | 6.4 | 0.4 | 0.5 | 1.4 | 50.0 | 229.2 |
| MP + R | 100.2 | 91.2 | - | 355.56 | 6.4 | 0.4 | 0.5 | 1.4 | 50.0 | 229.2 |
| PHP + R | 100.2 | 66.0 | - | 355.56 | 6.4 | 0.4 | 0.5 | 1.4 | 50.0 | 229.2 |
| PMP + R | 100.2 | 91.2 | - | 355.56 | 6.4 | 0.4 | 0.5 | 1.4 | 50.0 | 229.2 |
| HG + HP + R | 100.2 | 66.0 | 11.8 | 355.56 | 6.5 | 0.4 | 10.5 | 1.4 | 50.0 | 229.6 |
| PHG + HP + R | 100.2 | 66.0 | 11.8 | 355.56 | 6.5 | 0.4 | 10.5 | 1.4 | 50.0 | 229.6 |
| PHP + HG + R | 100.2 | 66.0 | 11.8 | 355.56 | 6.5 | 0.4 | 10.5 | 1.4 | 50.0 | 229.6 |
| PHG + PHP + R | 100.2 | 66.0 | 11.8 | 355.56 | 6.5 | 0.4 | 10.5 | 1.4 | 50.0 | 229.6 |
| R | HP + R | MP + R | PHP + R | PMP + R | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| ∆Peak (mmol/L) | 4.1 a | 0.2 | 4.3 a | 0.2 | 4.2 a | 0.2 | 3.7 a,b | 0.2 | 3.2 b | 0.2 |
| ∆Low (mmol/L) | −0.3a | 0.1 | −0.6 b | 0.1 | 0.3 a,b | 0.1 | −0.3 a | 0.1 | −0.2 a | 0.1 |
| MAGE (mmol/L) | 4.4 a,b | 0.2 | 4.9 a | 0.2 | 4.5 a,b | 0.2 | 3.9 b,c | 0.2 | 3.4 c | 0.2 |
| −∆G/∆G (%) | 67.5 a,b | 3.8 | 74.5 a,b | 5.2 | 79.6 a | 4.4 | 77.5 a | 5.4 | 61.1 b | 4.7 |
| CONGA1 | 1.8 a | 0.2 | 2.0 a | 0.2 | 1.9 a | 0.2 | 2.2 a | 0.2 | 1.7 a | 0.2 |
| iAUC0–30 | 50.4 a | 2.9 | 51.7 a | 3.5 | 52.5 a | 3.7 | 41.3 a,b | 2.9 | 37.2 b | 3.4 |
| iAUC0–60 | 142.3 a | 11.3 | 150.9 a | 9.4 | 144.8 a | 9.9 | 127.6 a,b | 6.7 | 113.5 b | 9.0 |
| iAUC0–120 | 230.4 a | 23.1 | 229.3 a | 18.4 | 213.5 a | 17.7 | 223.4 a | 19.0 | 214.0 a | 18.1 |
| iAUC120–240 | 46.2 a | 10.0 | 15.6 b | 4.2 | 24.7 a,b | 8.3 | 36.6 a,b | 7.8 | 44.3 a | 9.7 |
| iAUC0–240 | 276.7 a | 28.9 | 244.9 a | 20.2 | 238.2 a | 20.8 | 260.0 a | 21.8 | 258.3 a | 22.8 |
| R | HP + R | HG + HP + R | PHG + HP + R | PHP + R | PHP + HG + R | PHG + PHP + R | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| ∆Peak (mmol/L) | 4.1 a | 0.2 | 4.3 a | 0.2 | 4.1 a | 0.3 | 3.7 a | 0.2 | 3.7 a | 0.2 | 3.6 a | 0.2 | 2.9 b | 0.2 |
| ∆Low (mmol/L) | −0.3 a,b | 0.1 | −0.6 b | 0.1 | −0.4 a,b | 0.1 | −0.3 a,b | 0.1 | −0.3 a,b | 0.1 | −0.3 a,b | 0.1 | −0.2 a | 0.1 |
| MAGE (mmol/L) | 4.4 a,b,c | 0.2 | 4.9 a | 0.2 | 4.5 a,b | 0.3 | 4.0 b,c | 0.3 | 3.9 c | 0.2 | 3.9 c | 0.2 | 3.1 d | 0.2 |
| −∆G/∆G (%) | 67.5 b | 3.8 | 74.5 a,b | 5.2 | 85.6 a | 4.2 | 68.8 a,b | 7.2 | 77.5 a,b | 5.4 | 71.7 a,b | 6.2 | 81.5 a,b | 5..4 |
| CONGA1 | 1.8 b | 0.2 | 2.0 b | 0.2 | 1.9 b | 0.2 | 2.6 a | 0.2 | 2.2 a,b | 0.2 | 2.2 a,b | 0.2 | 1.7 b | 0.1 |
| iAUC0–30 | 50.4 a | 2.9 | 51.7 a | 3.5 | 57.5 a | 3.8 | 5.5 c | 1.4 | 41.3 b | 2.9 | 40.3 b | 3.8 | 38.4 b | 3.2 |
| iAUC0–60 | 142.3 a | 11.3 | 150.9 a | 9.4 | 151.7 a | 8.5 | 52.0 c | 4.6 | 127.6 a,b | 6.7 | 126.6 a,b | 7.6 | 106.0 b | 6.4 |
| iAUC0–120 | 230.4 a | 23.1 | 229.3 a | 18.4 | 203.5 a | 13.5 | 197.3 a | 16.2 | 223.4 a | 19.0 | 228.9 a | 17.2 | 176.8 a | 15.2 |
| iAUC120–240 | 46.2 a,b | 10.0 | 15.6 c | 4.2 | 23.8 b,c | 6.3 | 53.7 a | 8.9 | 36.6 a,b,c | 7.8 | 56.5 a | 11.0 | 36.6 a,b,c | 9.5 |
| iAUC0–240 | 276.7 a,b | 28.9 | 244.9 a,b | 20.2 | 227.2 a,b | 16.0 | 251.0 a,b | 20.0 | 260.0 a,b | 21.8 | 285.3 a | 25.0 | 213.3b | 21.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, W.; Zhou, Y.; Yuan, Y.; Fan, Z.; Wu, Y.; Liu, A.; Lu, X. Potato Preload Mitigated Postprandial Glycemic Excursion in Healthy Subjects: An Acute Randomized Trial. Nutrients 2020, 12, 2759. https://doi.org/10.3390/nu12092759
Zhao W, Zhou Y, Yuan Y, Fan Z, Wu Y, Liu A, Lu X. Potato Preload Mitigated Postprandial Glycemic Excursion in Healthy Subjects: An Acute Randomized Trial. Nutrients. 2020; 12(9):2759. https://doi.org/10.3390/nu12092759
Chicago/Turabian StyleZhao, Wenqi, Ying Zhou, Yuqing Yuan, Zhihong Fan, Yixue Wu, Anshu Liu, and Xuejiao Lu. 2020. "Potato Preload Mitigated Postprandial Glycemic Excursion in Healthy Subjects: An Acute Randomized Trial" Nutrients 12, no. 9: 2759. https://doi.org/10.3390/nu12092759
APA StyleZhao, W., Zhou, Y., Yuan, Y., Fan, Z., Wu, Y., Liu, A., & Lu, X. (2020). Potato Preload Mitigated Postprandial Glycemic Excursion in Healthy Subjects: An Acute Randomized Trial. Nutrients, 12(9), 2759. https://doi.org/10.3390/nu12092759