Oral Vitamin D Therapy in Patients with Psoriasis




Abstract
:1. Introduction
2. Materials and Methods
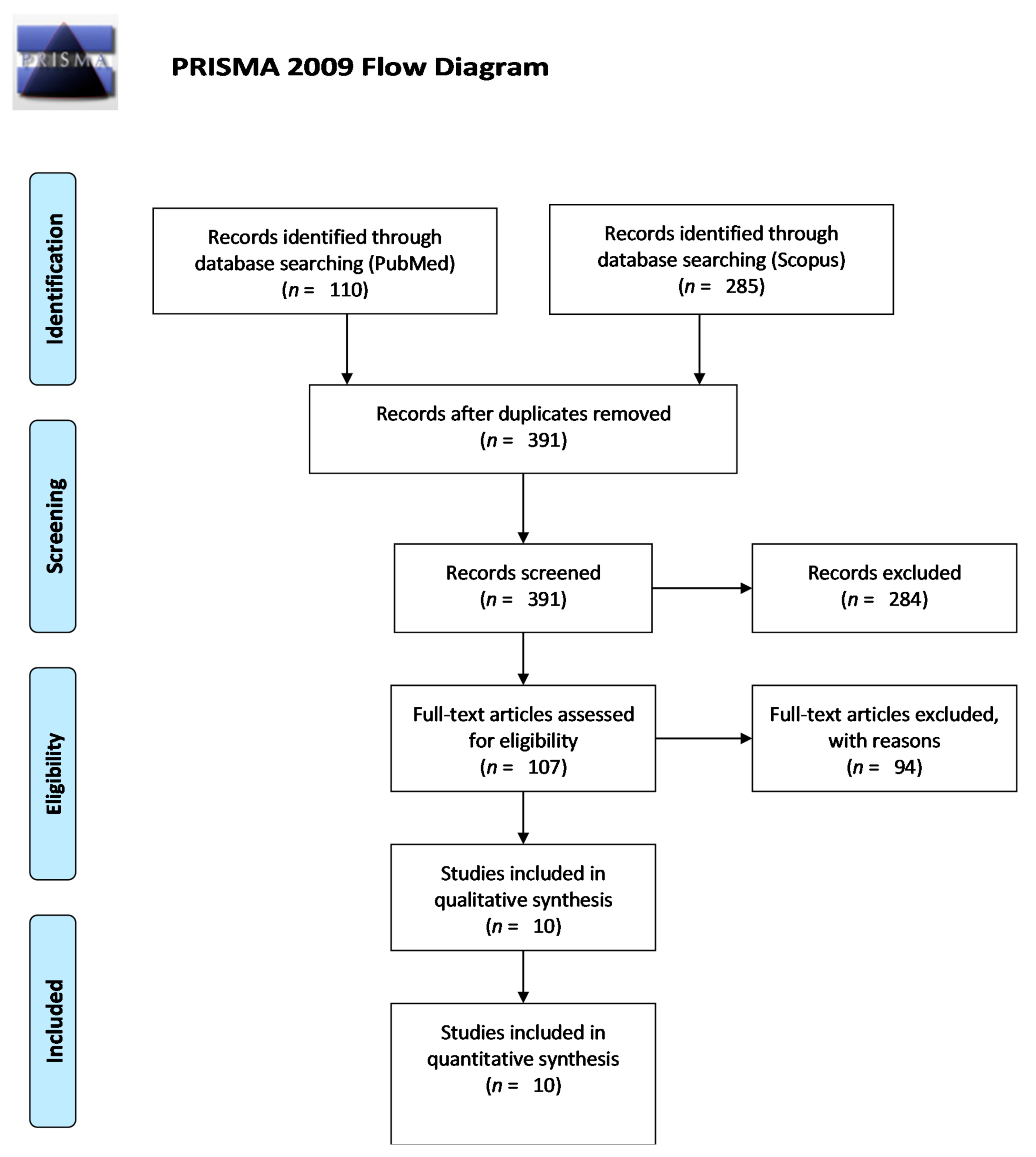
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Martens, P.J.; Gysemans, C.; Verstuyf, A.; Mathieu, A.C. Vitamin D’s effect on immune function. Nutrients 2020, 12, 1248. [Google Scholar] [CrossRef]
- Windaus, A.; Linsert, O.; Luttringhaus, A.; Weidlich, G. Über das krystallisierte Vitamin D2. Ann. Chem. Liebigs 1932, 492, 226–241. [Google Scholar] [CrossRef]
- Windaus, A.; Schenck, F.; von Werder, F. Über das antirachitisch wirksame bestrahlungs-produkt aus 7-dehydrocholesterin. Z Physiol. Chem. Hoppe Seylers 1936, 241, 100–103. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic effects of vitamin D on human health and disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Brandão-Lima, P.N.; Santos, B.D.C.; Aguilera, C.M.; Freire, A.R.S.; Martins-Filho, P.R.S.; Pires, L.V. Vitamin D food fortification and nutritional status in children: A systematic review of randomized controlled trials. Nutrients 2019, 11, 2766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Misra, M.; Pacaud, D.; Petryk, A.; Collett-Solberg, P.F.; Kappy, M. Drug and therapeutics committee of the Lawson Wilkins pediatric endocrine society. Vitamin D deficiency in children and its management: Review of current knowledge and recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.W.; Lee, H.C. Vitamin u8h brD and health—The missing vitamin in humans. Pediatrics Neonatol. 2019, 60, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Rendon, A.; Schäkel, K. Psoriasis pathogenesis and treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [Green Version]
- Slominski, A.; Kim, T.K.; Zmijewski, M.A.; Janjetovic, Z.; Li, W.; Chen, J.; Kusniatsova, E.I.; Semak, I.; Postlethwaite, A.; Miller, D.D.; et al. Novel vitamin D photoproducts and their precursors in the skin. Dermatoendocrinology 2013, 5, 7–19. [Google Scholar] [CrossRef] [Green Version]
- Stanescu, A.M.A.; Grajdeanu, I.V.; Iancu, M.A.; Pantea Stoian, A.; Bratu, O.G.; Socea, B.; Socea, L.I.; Diaconu, C.C. Correlation of oral vitamin D administration with the severity of psoriasis and the presence of metabolic syndrome. Rev. Chim. 2018, 69, 1668–1672. [Google Scholar] [CrossRef]
- Burfield, L.; Burden, A.D. Psoriasis. J. R. Coll. Physicians Edinb. 2013, 43, 334–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, A.; Slatopolsky, E. Vitamin D analogs: Therapeutic applications and mechanisms for selectivity. Mol. Asp. Med. 2008, 29, 433–452. [Google Scholar] [CrossRef] [PubMed]
- Piotrowska, A.; Wierzbicka, J.; Żmijewski, M.A. Vitamin D in the skin physiology and pathology. Acta Biochim. Pol. 2016, 63, 17–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penna, G.; Adorini, L. 1 Alpha,25-dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J. Immunol. 2000, 164, 2405–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morimoto, S.; Yoshikawa, K.; Kozyka, T.; Kitano, Y.; Imanaka, S.; Fukuo, K.; Koh, E.; Kumahara, Y. An open study of vitamin D3 treatment in psoriasis vulgaris. Br. J. Dermatol. 1986, 115, 421–429. [Google Scholar] [CrossRef]
- Kamangar, F.; Koo, J.; Heller, M.; Lee, E.; Bhutani, T. Oral vitamin D, still a viable treatment option for psoriasis. J. Dermatolog. Treat. 2013, 24, 261–267. [Google Scholar] [CrossRef]
- Lourencetti, M.; Abreu, M.M. Use of active metabolites of vitamin D orally for the treatment of psoriasis. Rev. Assoc. Med. Bras. 2018, 64, 643–648. [Google Scholar] [CrossRef]
- Soleymani, T.; Hung, T.; Soung, J. The role of vitamin D in psoriasis: A review. Int. J. Dermatol. 2015, 54, 383–392. [Google Scholar] [CrossRef]
- Millsop, J.W.; Bhatia, B.K.; Debbaneh, M.; Koo, J.; Liao, W. Diet and psoriasis, part III: Role of nutritional supplements. J. Am. Acad. Dermatol. 2014, 71, 561–569. [Google Scholar] [CrossRef] [Green Version]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and extraskeletal actions of vitamin D: Current evidence and outstanding questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takamoto, S.; Onishi, T.; Morimoto, S.; Imanaka, S.; Yukawa, S.; Kozuka, T.; Kitano, Y.; Seino, Y.; Kumahara, Y. Effect of 1 alpha-hydroxycholecalciferol on psoriasis vulgaris: A pilot study. Calcif. Tissue Int. 1986, 39, 360–364. [Google Scholar] [CrossRef]
- Smith, E.L.; Pincus, S.H.; Donovan, L.; Holick, M.F. A novel approach for the evaluation and treatment of psoriasis. Oral or topical use of 1,25-dihydroxyvitamin D3 can be a safe and effective therapy for psoriasis. J. Am. Acad. Dermatol. 1988, 19, 516–528. [Google Scholar] [CrossRef]
- Hambly, R.; Kirby, B. The relevance of serum vitamin D in psoriasis: A review. Arch. Dermatol. Res. 2017, 309, 499–517. [Google Scholar] [CrossRef] [PubMed]
- Holland, D.B.; Wood, E.J.; Roberts, S.G.; West, M.R.; Cunliffe, W.J. Epidermal keratin levels during oral 1-alpha-hydroxyvitamin D3 treatment for psoriasis. Skin Pharmacol. 1989, 2, 68–76. [Google Scholar] [CrossRef]
- Huckins, D.; Felson, D.T.; Holick, M. Treatment of psoriatic arthritis with oral 1,25-dihydroxyvitamin D3: A pilot study. Arthritis Rheum. 1990, 33, 1723–172715. [Google Scholar] [CrossRef]
- Siddiqui, M.A.; Al-Khawajah, M.M. Vitamin D3 and psoriasis: A randomized double-blind placebo-controlled study. J. Dermatol. Treat. 1990, 1, 243–245. [Google Scholar] [CrossRef]
- Zuccotti, E.; Oliveri, M.; Girometta, C.; Ratto, D.; Di Iorio, C.; Occhinegro, A.; Rossi, P. Nutritional strategies for psoriasis: Current scientific evidence in clinical trials. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8537–8551. [Google Scholar] [CrossRef]
- Lugo-Somolinos, A.; Sanchez, J.L.; Haddock, L. Efficacy of 1, alpha 25-dihydroxyvitamin D (Calcitriol) in the treatment of psoriasis vulgaris: An open study. Bol. Asoc. Med. P R 1990, 82, 450–453. [Google Scholar]
- el-Azhary, R.A.; Peters, M.S.; Pittelkow, M.R.; Kao, P.C.; Muller, S.A. Efficacy of vitamin D3 derivatives in the treatment of psoriasis vulgaris: A preliminary report. Mayo Clin. Proc. 1993, 68, 835–841. [Google Scholar] [CrossRef]
- Perez, A.; Raab, R.; Chen, T.C.; Turner, A.; Holick, M.F. Safety and efficacy of oral calcitriol (1,25-dihydroxyvitamin D3) for the treatment of psoriasis. Br. J. Dermatol. 1996, 134, 1070–1078. [Google Scholar] [CrossRef]
- Barrea, L.; Savanelli, M.C.; Di Somma, C.; Napolitano, M.; Megna, M.; Colao, A.; Savastano, S. Vitamin D and its role in psoriasis: An overview of the dermatologist and nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Gaál, J.; Lakos, G.; Szodoray, P.; Kiss, J.; Horváth, I.; Horkay, E.; Nagy, G.; Szegedi, A. Immunological and clinical effects of alphacalcidol in patients with psoriatic arthropathy: Results of an open, follow-up pilot study. Acta Derm. Venereol. 2009, 89, 140–144. [Google Scholar]
- Finamor, D.C.; Sinigaglia-Coimbra, R.; Neves, L.C.; Gutierrez, M.; Silva, J.J.; Torres, L.D.; Surano, F.; Neto, D.J.; Novo, N.F.; Juliano, Y.; et al. A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis. Dermatoendocrinology 2013, 5, 222–234. [Google Scholar] [CrossRef] [Green Version]
- Umar, M.; Sastry, K.S.; Al Ali, F.; Al-Khulaifi, M.; Wang, E.; Chouchane, A. I: Vitamin D and the pathophysiology of inflammatory skin diseases. Skin Pharmacol. Physiol. 2018, 31, 74–86. [Google Scholar] [CrossRef]
- Hata, T.; Audish, D.; Kotol, P.; Coda, A.; Kabigting, F.; Miller, J.; Alexandrescu, D.; Boguniewicz, M.; Taylor, P.; Aertker, L.; et al. A randomized controlled double-blind investigation of the effects of vitamin D dietary supplementation in subjects with atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Jarrett, P.; Camargo, C.A., Jr.; Coomarasamy, C.; Scragg, R. A randomized, double-blind, placebo-controlled trial of the effect of monthly vitamin D supplementation in mild psoriasis. J. Dermatolog. Treat. 2018, 29, 324–328. [Google Scholar] [CrossRef]
- Ingram, M.A.; Jones, M.B.; Stonehouse, W.; Jarrett, P.; Scragg, R.; Mugridge, O.; von Hurst, P.R. Oral vitamin D3 supplementation for chronic plaque psoriasis: A randomized, double-blind, placebo-controlled trial. J. Dermatolog. Treat. 2018, 29, 648–657. [Google Scholar] [CrossRef]
- Disphanurat, W.; Viarasilpa, W.; Chakkavittumrong, P.; Pongcharoen, P. The clinical effect of oral vitamin D2 supplementation on psoriasis: A double-blind, randomized, placebo-controlled study. Dermatol. Res. Pract. 2019, 2019, 5237642. [Google Scholar] [CrossRef]
- Marino, R.; Misra, M. Extra-sekeletal effects of vitamin D. Nutrients 2019, 11, 1460. [Google Scholar] [CrossRef] [Green Version]
- Fredriksson, T.; Pettersson, U. Severe psoriasis—Oral therapy with a new retinoid. Dermatologica 1978, 157, 238–244. [Google Scholar] [CrossRef]
- Heaney, R.P. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutr. Rev. 2014, 72, 48–54. [Google Scholar] [CrossRef]
- Le, P.; Tu, J.; Gebauer, K.; Brown, S. Serum 25-hydroxyvitamin D increases with UVB and UVA/UVB phototherapy (broadband UVB, narrowband UVB (NBUVB) and heliotherapy) in patients with psoriasis and atopic dermatitis. Australas J. Dermatol. 2016, 57, 115–121. [Google Scholar] [CrossRef]
- Tremezaygues, L.; Reichrath, J. Vitamin D analogs in the treatment of psoriasis: Where are we standing and where will we be going? Dermatoendocrinology 2011, 3, 180–186. [Google Scholar] [CrossRef]
- Orgaz-Molina, J.; Buenda-Eisman, A.; Arrabal-Polo, M.A.; Ruiz, J.C.; Arias-Santiago, S. Deficiency of serum concentration of 25-hydroxyvitamin D in psoriatic patients: A case-control study. J. Am. Acad. Dermatol. 2012, 67, 931–938. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Update in vitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Werner de Castro, G.R.; Neves, F.S.; Pereira, I.A.; Fialho, S.C.; Ribeiro, G.; Zimmermann, A.F. Resolution of adalimumab-induced psoriasis after vitamin D deficiency treatment. Rheumatol. Int. 2011, 32, 1313–1316. [Google Scholar] [CrossRef]
- Thompson, K.G.; Kim, N. Dietary supplements in dermatology: A review of the evidence for zinc, biotin, vitamin D, nicotinamide, and Polypodium. J. Am. Acad. Dermatol. 2020. [Google Scholar] [CrossRef]
- Merola, J.F.; Han, J.; Li, T.; Qureshi, A.A. No association between vitamin D intake and incident psoriasis among US women. Arch. Dermatol. Res. 2014, 306, 305–307. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.J.; Lehrer, D.S.; Amend, J.J. Daily oral dosing of vitamin D3 using 5000 TO 50,000 international units a day in long-term hospitalized patients: Insights from a seven year experience. J. Steroid Biochem. Mol. Biol. 2019, 189, 228–239. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.; Amend, J.J. Results of daily oral dosing with up to 60,000 international units (iu) of vitamin D3 for 2 to 6 years in 3 adult males. J. Steroid Biochem. Mol. Biol. 2017, 173, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Garland, C.F.; French, C.B.; Baggerly, L.L.; Heaney, R.P. Vitamin D supplement doses and serum 25-hydroxyvitamin D in the range associated with cancer prevention. Anticancer Res. 2011, 31, 617–622. [Google Scholar]
- Dawson-Hughes, B.; Staten, M.A.; Knowler, W.C.; Nelson, J.; Vickery, E.M.; LeBlanc, E.S.; Neff, L.M.; Park, J.; Pittas, A.G.; D2d Research Group. Intratrial exposure to vitamin D and new-onset diabetes among adults with prediabetes: A secondary analysis from the vitamin D and type 2 diabetes (D2d) study. Diabetes Care 2020, 43, 2916–2922. [Google Scholar] [CrossRef]
- Danik, J.S.; Manson, J.E. Vitamin d and cardiovascular disease. Curr. Treat. Options Cardiovasc. Med. 2012, 14, 414–424. [Google Scholar] [CrossRef] [Green Version]
- Chai, B.; Gao, F.; Wu, R.; Dong, T.; Gu, C.; Lin, Q.; Zhang, Y. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: An updated meta-analysis. BMC Neurol. 2019, 19, 284. [Google Scholar] [CrossRef]
- Aghajafari, F.; Letourneau, N.; Mahinpey, N.; Cosic, N.; Giesbrecht, G. Vitamin D deficiency and antenatal and postpartum depression: A systematic review. Nutrients 2018, 10, 478. [Google Scholar] [CrossRef] [Green Version]
- Cuomo, A.; Giordano, N.; Goracci, A.; Fagiolini, A. Depression and vitamin D deficiency: Causality, assessment, and clinical practice implications. Neuropsyvchiatry 2017, 7, 606–614. [Google Scholar] [CrossRef] [Green Version]
- Gruber-Bzura, B.M. Vitamin D and influenza-prevention or therapy? Int. J. Mol. Sci. 2018, 19, 2419. [Google Scholar] [CrossRef] [Green Version]
- American Geriatrics Society Workgroup on Vitamin D Supplementation for Older Adult. Recommendations abstracted from the American geriatrics consensus statement on Vitamin D for prevention of falls and their consequences. J. Am. Geriatr. Soc. 2014, 62, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Goulão, B.; Stewart, F.; Ford, J.A.; MacLennan, G.; Avenell, J.A. Cancer and vitamin D supplementation: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2018, 107, 652–663. [Google Scholar] [CrossRef]
- Bittenbring, J.T.; Neumann, F.; Altmann, B.; Achenbach, M.; Reichrath, J.; Ziepert, M.; Geisel, J.; Regitz, E.; Held, G.; Pfreundschuh, M. Vitamin D deficiency impairs rituximab-mediated cellular cytotoxicity and outcome of patients with diffuse large B-cell lymphoma treated with but not without rituximab. J. Clin. Oncol. 2014, 32, 3242–3248. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Tang, Z.; Wang, Y.; Ding, X.; Rinaldi, G.; Rahmani, J.; Xing, F. Relationship between vitamin D level and mortality in adults with psoriasis: A retrospective cohort study of NHANES data. Clin. Ther. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Authors and Year | Type of Study | Number of Patients | Study Location | Reviews Including the Original Study from the First Column |
|---|---|---|---|---|
| Morimoto et al., 1986 [17] | Open-design study | 21 | Japan | Kamangar et al., 2013 [18] Lourenceti et al., 2018 [19] Soleymani et al., 2015 [20] Millsop et al., 2014 [21] Bouillon et al., 2018 [22] |
| Takamoto et al., 1986 [23] | Descriptive study | 7 | Japan | Kamangar et al., 2013 [18] Lourenceti et al., 2018 [19] |
| Smith et al., 1988 [24] | Descriptive study | 14 | USA | Kamangar et al., 2013 [18] Lourenceti et al., 2018 [19] Millsop et al., 2014 [21] Bouillon et al., 2018 [22] Hambly et al., 2017 [25] |
| Holland et al., 1989 [26] | Descriptive study | 15 | UK | Hambly et al., 2017 [25] |
| Huckins et al., 1990 [27] | Open-label trial | 6 | USA | Kamangar et al., 1990 [18] Lourenceti et al., 2018 [19] |
| Siddiqui et al., 1990 [28] | Prospective randomized double-blind control study | 41 | Saudi Arabia | Millsop et al., 2014 [21] Zuccotti et al., 2018 [29] |
| Lugo-Somolinos et al., 1990 [30] | Descriptive study | 10 | Puerto Rico | Hambly et al., 2017 [25] |
| El-Alzhari et al., 1993 [31] | Descriptive study | 8 | USA | Lourenceti et al., 2018 [19] Millsop et al., 2014 [21] |
| Perez et al., 1996 [32] | Open trial | 85 | USA | Kamangar et al., 2013 [18] Lourenceti et al., 2018 [19] Soleymani et al., 2015 [20] Millsop et al., 2014 [21] Barrea et al., 2017 [33] Bouillon et al., 2018 [22] Hambly et al., 2017 [25] |
| Gaal et al., 2009 [34] | Case-control | 10 | USA | Kamangar et al., 2013 [18] Zuccotti et al., 2018 [29] |
| Finamor et al., 2013 [35] | Open-label clinical trial | 9 | Hungary | Lourenceti et al., 2018 [19] Millsop et al., 2014 [21] Umar et al., 2018 [36] Hambly et al., 2017 [25] |
| Hata et al., 2014 [37] | Randomized placebo-controlled | 16 | Brazil | Hambly et al., 2017 [25] |
| Jarret et al., 2018 [38] | Randomized double blind, placebo-controlled study | 65 | USA | Zuccotti et al., 2018 [29] |
| Ingram et al., 2018 [39] | Randomized double blind, placebo-controlled study | 101 | New Zealand | |
| Disphanurat et al., 2019 [40] | Randomized double blind, placebo-controlled study | 45 | Thailand | Marino et al., 2019 [41] |
| Individual Studies, Year | Dose | Duration of Administration | Efficacy | Type/Severity of Psoriasis | Effectiveness | Treatment Side Effects |
|---|---|---|---|---|---|---|
| Morimoto et al., 1986 [17] | 1.0 μg/day 1α-(OH)D3 (40 IU/day) | 6 months | 2.7 +/− 0.6 months | Psoriasis vulgaris | More than moderate improvement (+2) in 76% of patients | No |
| 0.5 μg/day 1,25-(OH)2-D3 (20 IU/day) | 6 months | 3 months | Psoriasis vulgaris | Moderate improvement (+2) in 25% of patients | No | |
| Takamoto et al., 1986 [23] | 1.0 μg/day 1α-(OH)D3 (40 IU/day) | 12 months | more than 8 months | Psoriasis vulgaris |
| No |
| Smith et al., 1988 [24] | 0.25 μg (10 IU) once or twice/day increased by 0.25 to 0.5 μg/day every 2 weeks to a maximum of 2.0 μg (80 IU)/day 1,25-(OH)2-D3 | 2 months | less than 2 months | moderate to severe psoriasis |
| No |
| Holland et al., 1989 [26] | 1.0 μg/day 1α-(OH)D3 (40 IU) | 6 months | 6–8 weeks | Plaque psoriasis | 46.67% of patients had complete resolution of lesions (+4), 2 within 6 weeks and the rest after 4–6 months of therapy. | No |
| Huckins et al., 1990 [27] | 1.0 μg/day 0.5 μg/day increased by 0.25 μg/day every 2 weeks to a maximum of 2.0 μg (80 IU)/day 1,25-(OH)2-D3 | 6 months | 2–3 months | Psoriatic arthritis |
| hypercalciuria in 20% of patients |
| Siddiqui et al., 1990 [28] | 1 μg/day alpha-calcidol | 12 weeks | Not specified | Psoriasis vulgaris | 45% of patients showed slight improvement (+1). | |
| Lugo-Somolinos et al., 1990 [30] | 0.5 μg/day 1α,25-(OH)2 -D3 (20 IU) | after 3 months | Moderate to severe psoriasis | 40% of patients showed moderate improvement. | No | |
| El-Alzhari et al., 1993 [31] | 0.5 μg/day increased by 0.5 μg biweekly to a maximal dosage of 2.0 μg daily. 1,25-(OH)2-D3 | 6 months | 2 months | Psoriasis vulgaris moderate to severe |
| No |
| Perez et al., 1996 [32] | 0.5 μg/day increments of 0.5 μg every 2 weeks 1,25-(OH)2-D3 | 6 months–3 years | 6 months | Psoriasisvulgaris | Global severity score for the patients’ lesions had a mean value of 7.7 ± 1.2; the mean global severity score significantly decreased to 3.2 ± 1.9. The mean baseline PASI score was 18.4 ± 1.0; at 6 and 36 months of treatment the mean PASI score was reduced to 9.7 ± 0.8 and 7.0 ± 1.3, respectively. | No |
| Gaal et al., 2009 [34] | 0.25 μg twice daily 1α-(OH)D3 | 6 months | Not specified | Psoriatic arthritis | PASI scores were 12.8 +/− 14.3 vs. 11.9 +/− 14.4. on average. | No |
| Finamor et al., 2013 [35] | 35,000 IU per day vit. D3 | 6 months | Not specified | Psoriasis vulgaris moderate to severe | The clinical condition of all patients significantly improved (+3 to +4). | - |
| Hata et al., 2014 [37] | 4000 IU/day vit. D3 | 6 months | Not specified | Mild psoriasis | No change in PASI score (0) | No |
| Jarret et al., 2018 [38] | 100,000 IU/month (3300 IU/day) vit. D3 | 4 years | Not specified | Mild psoriasis | The trial results do not support the use of monthly vitamin D3 supplementation (100,000 IU per month) as a treatment for mild psoriasis in patients over 50 years old. | |
| Ingram et al., 2018 [39] | 200,000 IU at baseline, then 100,000 IU/month vit. D3 | 11 months | 6 months | Chronic psoriasis | No benefit | Not specified |
| Individual Studies/ Year | Dose | Period of Administration | Efficacy Observed | Type/Severity of Psoriasis | Effectiveness | Treatment Side Effects |
|---|---|---|---|---|---|---|
| Disphanurat et al., 2019 [40] | 20,000 IU/every 2 weeks vit. D2 | 6 months | 3–6 months | Chronic plaque-type psoriasis—mild psoriasis | PASI score decreased at 3 and 6 months, moderate improvement | No |
| Authors | Evaluation |
|---|---|
| Morimoto et al. [17] | Clinical photographs taken at every examination Clinical score: complete remission (+4), marked improvement (+3), moderate improvement (+2), slight improvement (+1), no change (o), deterioration (−1). |
| Smith et al. [24] | Clinical examination Clinical score: no change (0), minimal improvement up to 25% improved (+1), 26% to 50% improved (+2), 51% to 75% improved (+3), >75% improved to clear (+4). |
| Takamoto et al. [23] | Clinical examination: complete remission (4) (complete flattering of plaques including borders, percentage of area improved: 95% or more); marked improvement (3) (nearly complete flattering of all plaques still palpable, area improved: 50–90%); definite improvement (2) (partial flattering of plaque, less scaling and less erythema, area improved: 20–50%), minimal improvement (1) (slightly less scaling and less erythema, area improved: 5–20%); no change (0); aggravation (−1) by the percentage of skin involvement was improved. |
| Huckins et al. [27] | Clinical photographs taken at every examination Clinical score of erythema: deterioration (−1), no change (0), mild improvement (1), moderate improvement (2), marked improvement (3) |
| Gaal et al. [34] |
|
| Perez et al. [32] | Clinical photographs taken at every examination PASI score, global severity score Global Improvement Scale: deterioration (−1), no change (0), mild improvement (1), moderate improvement (2), excellent improvement (3) |
| El-Azhary et al. [31] | Clinical evaluation of the percentage of body surface involved Grading the erythema, scale, and thickness of the lesions as worsening (−1), no improvement (0), mild improvement (+1), moderate improvement (+2), marked improvement (+3). |
| Finamor et al. [35] |
|
| Siddiqui et al. [28] | PASI score Worsening PASI score (−1), no improvement (0), slight improvement (+1), moderate improvement (+2), marked improvement (+3). |
| Holland et al. [26] |
|
| Hata et al. [37] | PASI score Punch biopsies of psoriatic skin lesion and uninvolved skin |
| Jarret et al. [38] |
|
| Ingram et al. [39] |
|
| Disphanurat et al. [40] |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanescu, A.M.A.; Simionescu, A.A.; Diaconu, C.C. Oral Vitamin D Therapy in Patients with Psoriasis. Nutrients 2021, 13, 163. https://doi.org/10.3390/nu13010163
Stanescu AMA, Simionescu AA, Diaconu CC. Oral Vitamin D Therapy in Patients with Psoriasis. Nutrients. 2021; 13(1):163. https://doi.org/10.3390/nu13010163
Chicago/Turabian StyleStanescu, Ana Maria Alexandra, Anca Angela Simionescu, and Camelia Cristina Diaconu. 2021. "Oral Vitamin D Therapy in Patients with Psoriasis" Nutrients 13, no. 1: 163. https://doi.org/10.3390/nu13010163
APA StyleStanescu, A. M. A., Simionescu, A. A., & Diaconu, C. C. (2021). Oral Vitamin D Therapy in Patients with Psoriasis. Nutrients, 13(1), 163. https://doi.org/10.3390/nu13010163