Effects of Cistanche tubulosa Wight Extract on Locomotive Syndrome: A Placebo-Controlled, Randomized, Double-Blind Study


Abstract
:1. Introduction
2. Materials and Methods
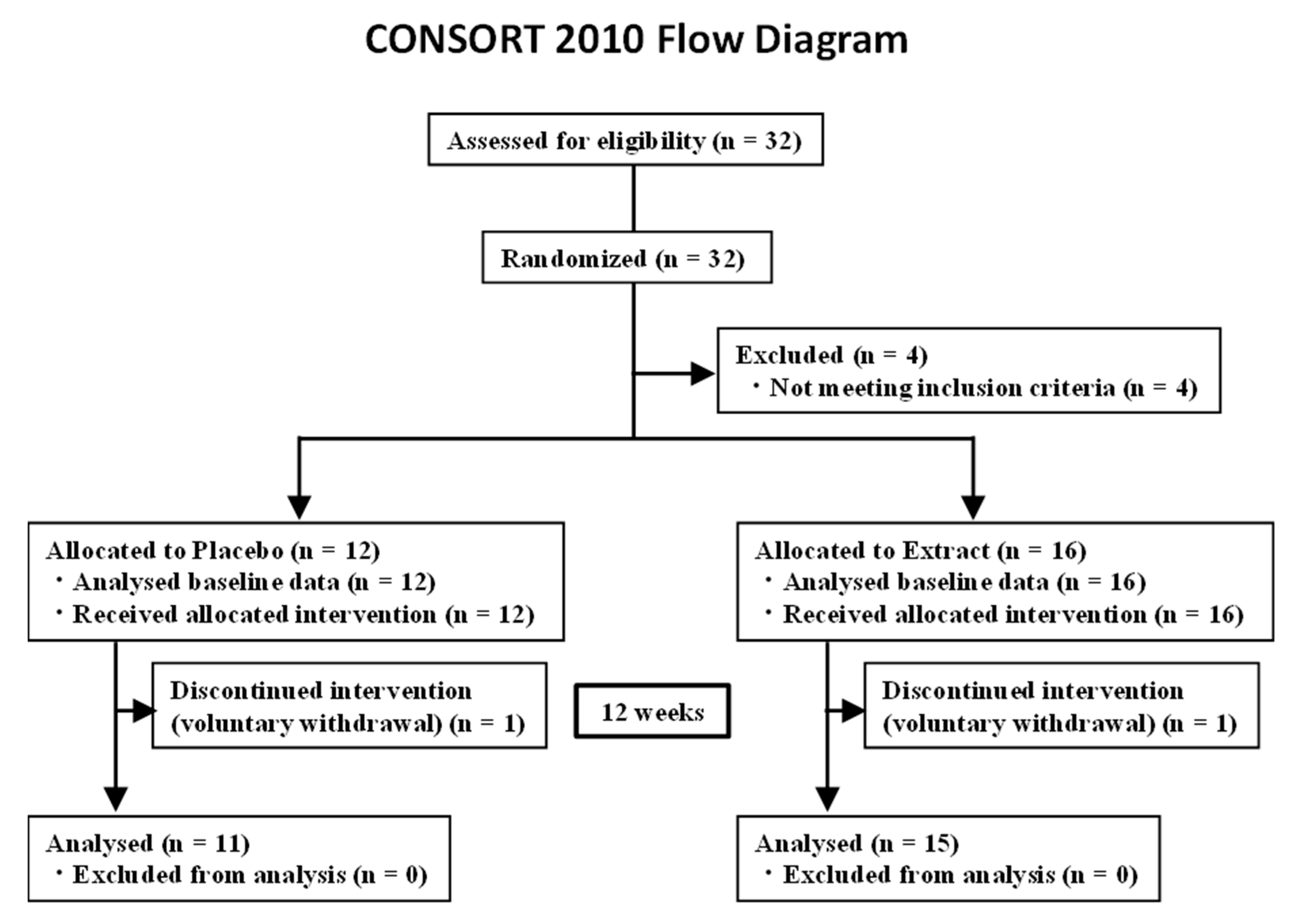
2.1. Trial Design
2.2. Participants
2.3. Intervention
2.4. Outcomes and Assessments
- You cannot put on a pair of socks while standing on one leg.
- You stumble or slip in your house.
- You need to use a handrail when going upstairs.
- You cannot get across the road at a crossing before the traffic light changes.
- You have difficulty walking continuously for 15 min.
- You find it difficult to walk home carrying a shopping bag weighing approximately 2 kg.
- You find it difficult to do housework requiring physical strength.
2.4.1. Measurement of Muscle Mass
2.4.2. Hand Grip Strength
2.4.3. Five-Meter Walking Speed
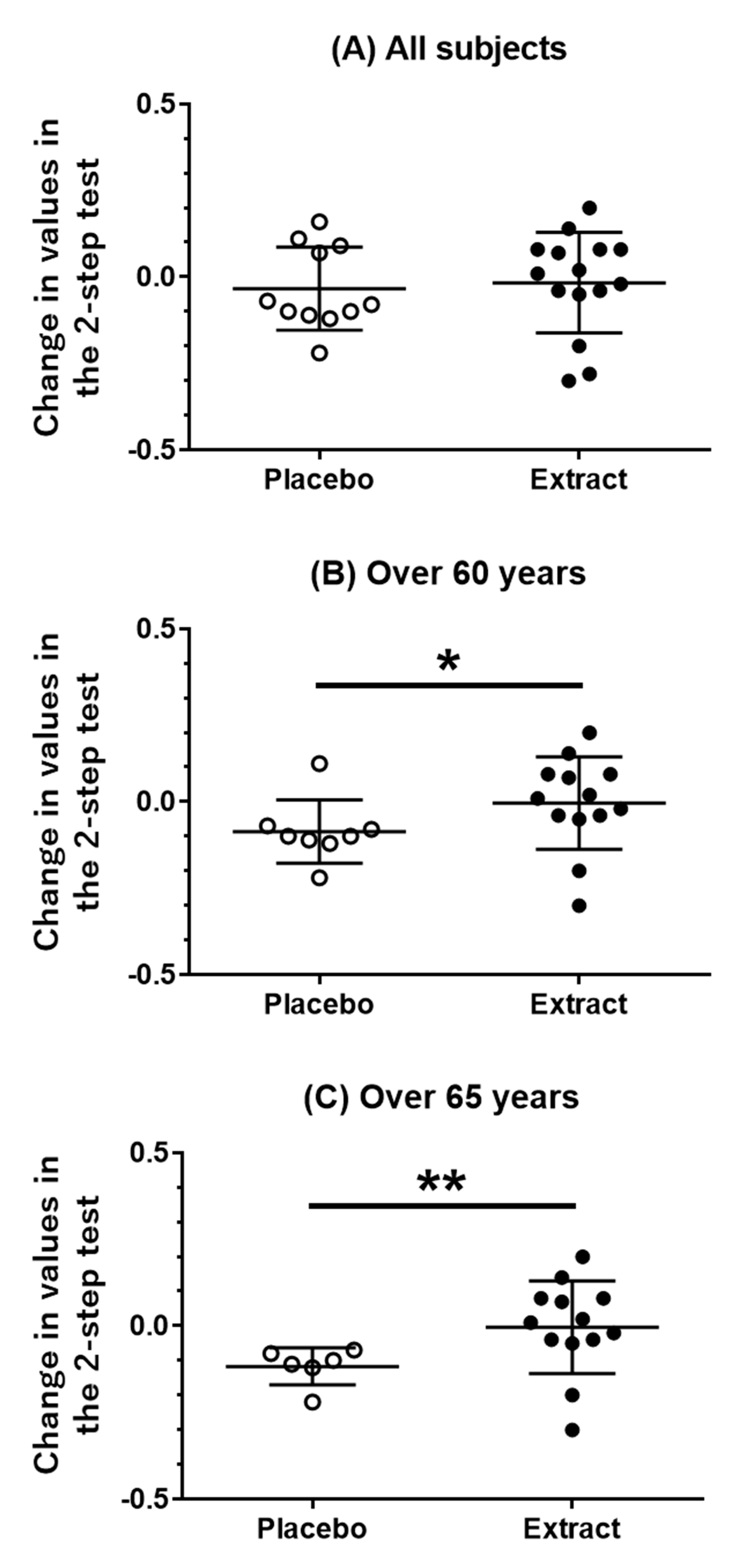
2.4.4. Two-Step Test
2.4.5. The Stand-Up Test
2.4.6. GLFS-25
2.5. Safety Assessment
2.6. Randomization
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Groups
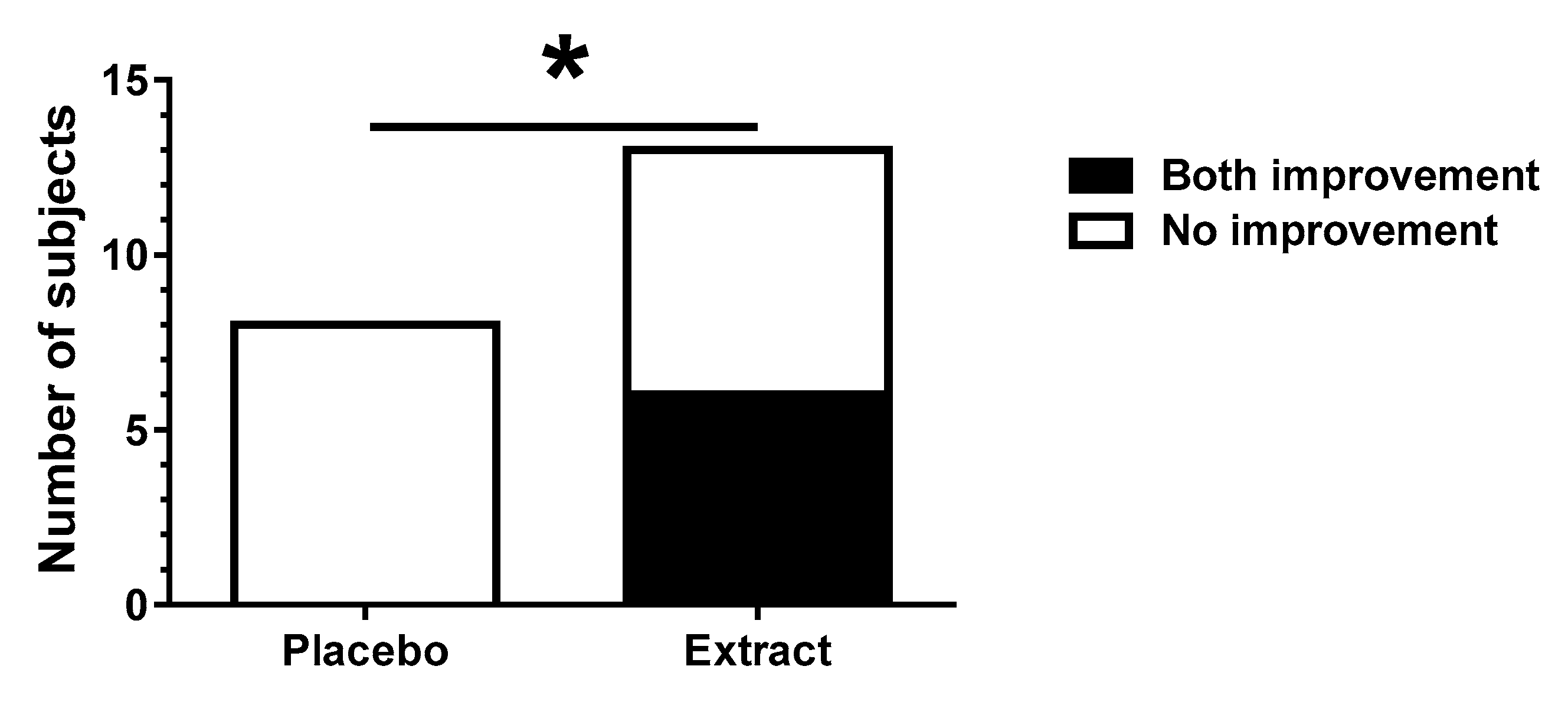
3.2. Muscle Mass and Physical Activities
3.3. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nakamura, K. A “super-aged” society and the “locomotive syndrome”. J. Orthop. Sci. 2008, 13, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, K.; Sakuma, M.; Ogisho, N.; Nakamura, K.; Chosa, E.; Endo, N. The effects of self-directed home exercise with serial telephone contacts on physical functions and quality of life in elderly people at high risk of locomotor dysfunction. Acta. Med. Okayama 2015, 69, 245–253. [Google Scholar] [CrossRef]
- Sato, H.; Kondo, S.; Saito, M.; Saura, R. Effects of strengthening the hip flexor muscles on walking ability and the locomotive syndrome rank test: An intervention study. J. Orthop. Sci. 2020, 25, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.; Sakuma, M.; Endo, N. The impact of exercise and vitamin D supplementation on physical function in community-dwelling elderly individuals: A randomized trial. J. Orthop. Sci. 2018, 23, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Suzukamo, C.; Ishimaru, K.; Ochiai, R.; Osaki, N.; Kato, T. Milk-fat globule membrane plus glucosamine improves joint function and physical performance: A randomized, double-blind, placebo-controlled, parallel-group study. J. Nutr. Sci. Vitaminol. 2019, 65, 242–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimbara, Y.; Shimada, Y.; Kuboyama, T.; Tohda, C. Cistanche tubulosa (Schenk) Wight extract enhances hindlimb performance and attenuates myosin heavy chain IId/IIx expression in cast-immobilized mice. Evid. Based Complement. Alternat. Med. 2019, 2019, 9283171. [Google Scholar] [CrossRef]
- Cai, R.L.; Yang, M.H.; Shi, Y.; Chen, J.; Li, Y.C.; Qi, Y. Antifatigue activity of phenylethanoid-rich extract from Cistanche deserticola. Phytother. Res. 2010, 24, 313–315. [Google Scholar] [CrossRef]
- Liao, F.; Zheng, R.L.; Gao, J.J.; Jia, Z.J. Retardation of skeletal muscle fatigue by the two phenylpropanoid glycosides: Verbascoside and martynoside from Pedicularis plicata maxim. Phytother. Res. 1999, 13, 621–623. [Google Scholar] [CrossRef]
- Kodani, A.; Kikuchi, T.; Tohda, C. Acteoside improves muscle atrophy and motor function by inducing new myokine secretion in chronic spinal cord injury. J. Neurotrauma 2019, 36, 1935–1948. [Google Scholar] [CrossRef] [Green Version]
- ORYZA OIL & FAT CHEMICAL CO., LTD. CISTANCHE TUBULOSA EXTRACT. Electric Catalog ver. 2.0 JT. Available online: http://www.oryza.co.jp/pdf/japanese/cistanche%20tuburosa%20extract_j%202.0.pdf (accessed on 1 October 2020).
- Nakamura, K. Guidebook on Locomotive Syndrome; Bunkodo: Tokyo, Japan, 2010. [Google Scholar]
- Muranaga, S.; Hirano, K. Development of a convenient way to predict ability to walk, using a two-step test. J. Showa Med. Assoc. 2003, 63, 301–303. [Google Scholar]
- Ogata, T.; Muranaga, S.; Ishibashi, H.; Ohe, T.; Izumida, R.; Yoshimura, N.; Tsutomu Iwaya, T.; Nakamura, K. Development of a screening program to assess motor function in the adult population: A cross-sectional observational study. J. Orthop. Sci. 2015, 20, 888–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seichi, A.; Hoshino, Y.; Doi, T.; Akai, M.; Tobimatsu, Y.; Iwaya, T. Development of a screening tool for risk of locomotive syndrome in the elderly: The 25-question Geriatric Locomotive Function Scale. J. Orthop. Sci. 2012, 17, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Strasser, E.M.; Hofmann, M.; Franzke, B.; Schober-Halper, B.; Oesen, S.; Jandrasits, W.; Graf, A.; Praschak, M.; Horvath-Mechtler, B.; Krammer, C.; et al. Strength training increases skeletal muscle quality but not muscle mass in old institutionalized adults: A randomized, multi-arm parallel and controlled intervention study. Eur. J. Phys. Rehabil. Med. 2018, 54, 921–933. [Google Scholar] [CrossRef]
- Najima, M.; Shirakawa, T.; Ishii, I.; Okamoto, K. A study for evaluating the effect of the supplement containing glucosamine on joint performance and daily physical performance: A randomized, double-blind, placebo-controlled, study mainly evaluated by subjects-oriented questionnaire. Jpn. Pharmacol. Ther. 2017, 45, 939–955. [Google Scholar]
- Aleman-Mateo, H.; Carreon, V.R.; Macias, L.; Astiazaran-Garcia, H.; Gallegos-Aguilar, A.C.; Enriquez, J.R.R. Nutrient-rich dairy proteins improve appendicular skeletal muscle mass and physical performance, and attenuate the loss of muscle strength in older men and women subjects: A single-blind randomized clinical trial. Clin. Interv. Aging. 2014, 9, 1517–1525. [Google Scholar] [CrossRef] [Green Version]
- Chanet, A.; Verlaan, S.; Salles, J.; Giraudet, C.; Patrac, V.; Pidou, V.; Pouyet, C.; Hafnaoui, N.; Blot, A.; Cano, N.; et al. Supplementing breakfast with a vitamin D and leucine-enriched whey protein medical nutrition drink enhances postprandial muscle protein synthesis and muscle mass in healthy older men. J. Nutr. 2017, 147, 2262–2271. [Google Scholar] [CrossRef] [Green Version]
- Ispoglou, T.; White, H.; Preston, T.; McElhone, S.; McKenna, J.; Hind, K. Double-blind, placebo-controlled pilot trial of L-leucine-enriched amino-acid mixtures on body composition and physical performance in men and women aged 65–75 years. Eur. J. Clin. Nutr. 2016, 70, 182–188. [Google Scholar] [CrossRef]
- Markofski, M.M.; Jennings, K.; Timmerman, K.L.; Dickinson, J.M.; Fry, C.S.; Borack, M.S.; Reidy, P.T.; Deer, R.R.; Randolph, A.; Rasmussen, B.B.; et al. Effect of aerobic exercise training and essential amino acid supplementation for 24 weeks on physical function, body composition and muscle metabolism in healthy, independent older adults: A randomized clinical trial. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1598–1604. [Google Scholar] [CrossRef]
- Scognamiglio, R.; Piccolotto, R.; Negut, C.; Tiengo, A.; Avogaro, A. Oral amino acids in elderly subjects: Effect on myocardial function and walking capacity. Gerontology. 2005, 51, 302–308. [Google Scholar] [CrossRef]
- Giuseppe, D.A.; Maurizio, R.; Annalisa, C.; Laura, T.; Marta, D.; Flavia, B.; Francesca, C.; Giovanni, C.; Roberto, B.; Michele, O.C.; et al. Branched-chain amino acid supplementation promotes survival and supports cardiac and skeletal muscle mitochondrial biogenesis in middle-aged mice. Cell Metab. 2010, 12, 362–372. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Both Legs | ||||
| 40 cm | 30 cm | 20 cm | 10 cm | |
| Success score | 1 | 2 | 3 | 4 |
| Right Legs | ||||
| 40 cm | 30 cm | 20 cm | 10 cm | |
| Success score | 5 | 10 | 15 | 20 |
| Left Legs | ||||
| 40 cm | 30 cm | 20 cm | 10 cm | |
| Success score | 5 | 10 | 15 | 20 |
| Item | Placebo (n = 11) | Extract (n = 15) | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| Male, n | 2 (18.2%) | 5 (33.3%) | ||||||
| Age (years) | 61.3 | ± | 8.8 | 69.2 | ± | 7.7 | 0.01 | * |
| Height (cm) | 156.5 | ± | 8.3 | 155.6 | ± | 9.1 | 0.83 | |
| Body weight (kg) | 61.3 | ± | 13.4 | 56.9 | ± | 8.1 | 0.44 | |
| BMI (kg/m2) | 24.9 | ± | 4.1 | 23.5 | ± | 2.8 | 0.39 | |
| Locomo 7 score | 2.1 | ± | 1.2 | 2.0 | ± | 1.8 | 0.50 | |
| All Subjects (n = 26) | Pre | Post | Intragroup Comparison (Pre vs. Post) | Changed Value (Post-Pre) | Comparison between Group (Extract vs. Placebo) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Muscle Mass | Mean | SD | Mean | SD | 95% CI | p Value | r | Mean | SD | 95% CI | p Value | r | |||
| Lower | Upper | Lower | Upper | ||||||||||||
| Whole body (kg) | Extract (n = 15) | 38.63 | 6.73 | 38.58 | 6.65 | −0.35 | 0.25 | 0.75 | 0.06 | −0.05 | 0.51 | −0.20 | 0.70 | 0.24 | 0.24 |
| Placebo (n = 11) | 39.52 | 8.73 | 39.66 | 9.03 | −0.35 | 0.60 | 0.40 | 0.17 | 0.15 | 0.67 | |||||
| Body trunk(kg) | Extract | 21.29 | 3.45 | 21.41 | 3.37 | −0.25 | 0.45 | 0.83 | 0.04 | 0.13 | 0.72 | −0.50 | 0.50 | 0.88 | 0.03 |
| Placebo | 21.93 | 4.69 | 21.99 | 4.75 | −0.30 | 0.40 | 0.84 | 0.04 | 0.06 | 0.57 | |||||
| Arm right (kg) | Extract | 2.00 | 0.45 | 2.00 | 0.42 | −0.05 | 0.05 | 1.00 | 0.00 | 0.00 | 0.10 | −0.10 | 0.10 | 0.80 | 0.05 |
| Placebo | 1.97 | 0.50 | 1.98 | 0.52 | −0.05 | 0.05 | 0.71 | 0.07 | 0.01 | 0.08 | |||||
| Arm left (kg) | Extract | 1.94 | 0.44 | 1.92 | 0.42 | −0.10 | 0.05 | 0.59 | 0.11 | −0.02 | 0.12 | 0.00 | 0.10 | 0.22 | 0.26 |
| Placebo | 1.89 | 0.54 | 1.94 | 0.55 | 0.00 | 0.10 | 0.13 | 0.30 | 0.05 | 0.09 | |||||
| Leg right (kg) | Extract | 6.76 | 1.43 | 6.66 | 1.40 | −0.30 | 0.10 | 0.43 | 0.16 | −0.10 | 0.32 | −0.10 | 0.20 | 0.81 | 0.08 |
| Placebo | 6.86 | 1.60 | 6.85 | 1.67 | −0.10 | 0.10 | 0.90 | 0.02 | −0.01 | 0.15 | |||||
| Leg left (kg) | Extract | 6.65 | 1.46 | 6.59 | 1.45 | −0.20 | 0.10 | 0.70 | 0.08 | −0.06 | 0.31 | −0.10 | 0.30 | 0.44 | 0.16 |
| Placebo | 6.86 | 1.63 | 6.90 | 1.74 | −0.10 | 0.20 | 0.57 | 0.11 | 0.04 | 0.22 | |||||
| Body weight (kg) | Extract | 56.91 | 8.09 | 57.06 | 8.39 | −0.85 | 0.95 | 0.84 | 0.04 | 0.15 | 1.78 | −1.20 | 0.60 | 0.33 | 0.19 |
| Placebo | 61.35 | 13.40 | 61.00 | 13.61 | −0.80 | 0.15 | 0.13 | 0.30 | −0.35 | 0.69 | |||||
| All Subjects (n = 26) | Pre | Post | Intragroup Comparison (Pre vs. Post) | Changed Value (Post-Pre) | Comparison between Group (Extract vs. Placebo) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical Activity | Mean | SD | Mean | SD | 95% CI | p Value | r | Mean | SD | 95% CI | p Value | r | |||
| Lower | Upper | Lower | Upper | ||||||||||||
| Hand grip right (kg) | Extract (n = 15) | 26.70 | 9.63 | 27.47 | 9.28 | −1.00 | 2.75 | 0.33 | 0.19 | 0.77 | 4.24 | −1.50 | 3.00 | 0.47 | 0.14 |
| Placebo (n = 11) | 29.95 | 7.29 | 31.68 | 7.19 | 0.50 | 3.00 | 0.04 | 0.40 | 1.73 | 3.45 | |||||
| Hand grip left (kg) | Extract | 25.62 | 8.71 | 26.67 | 8.89 | −0.75 | 2.50 | 0.27 | 0.22 | 1.05 | 2.92 | −2.50 | 2.00 | 0.88 | 0.03 |
| Placebo | 28.09 | 8.63 | 29.45 | 7.72 | −1.00 | 5.00 | 0.44 | 0.15 | 1.36 | 4.15 | |||||
| 5-m walking (s) | Extract | 3.09 | 1.63 | 2.88 | 1.49 | −0.34 | 0.03 | 0.13 | 0.30 | −0.21 | 0.51 | −0.19 | 0.35 | 0.47 | 0.14 |
| Placebo | 2.33 | 0.33 | 2.26 | 0.36 | −0.29 | 0.15 | 0.37 | 0.17 | −0.07 | 0.30 | |||||
| 2-step test (point) | Extract | 1.36 | 0.23 | 1.34 | 0.19 | −0.11 | 0.07 | 1.00 | 0.00 | −0.02 | 0.14 | −0.15 | 0.10 | 0.54 | 0.13 |
| Placebo | 1.43 | 0.19 | 1.40 | 0.17 | −0.11 | 0.04 | 0.42 | 0.16 | −0.03 | 0.12 | |||||
| Stand-up test (point) | Extract | 12.73 | 9.95 | 14.20 | 7.81 | 0.00 | 5.00 | 0.36 | 0.18 | 1.47 | 7.77 | −5.00 | 4.00 | 0.76 | 0.06 |
| Placebo | 14.45 | 11.86 | 15.91 | 12.23 | −3.00 | 5.50 | 0.78 | 0.06 | 1.45 | 7.57 | |||||
| GLFS-25 (point) | Extract | 13.53 | 15.36 | 13.33 | 10.42 | −4.00 | 0.00 | 0.68 | 0.08 | −0.20 | 11.99 | −9.00 | 2.00 | 0.22 | 0.25 |
| Placebo | 11.73 | 13.54 | 9.91 | 13.04 | −4.00 | 0.00 | 0.20 | 0.25 | −1.82 | 3.82 | |||||
| Over 60 Years (n = 21) | Pre | Post | Intragroup Comparison (Pre vs. Post) | Changed Value (Post-Pre) | Comparison between Group (Extract vs. Placebo) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical Activity | Mean | SD | Mean | SD | 95% CI | p Value | r | Mean | SD | 95% CI | p Value | r | ||||
| Lower | Upper | Lower | Upper | |||||||||||||
| Hand grip right (kg) | Extract (n = 13) | 10.40 | 2.88 | 9.99 | 2.77 | −1.75 | 2.75 | 0.61 | 0.10 | 0.50 | 4.47 | −2.00 | 3.50 | 0.46 | 0.16 | |
| Placebo (n = 8) | 28.63 | 7.28 | 30.38 | 7.29 | −1.50 | 5.75 | 0.12 | 0.30 | 1.75 | 4.06 | ||||||
| Hand grip left (kg) | Extract | 9.34 | 2.59 | 9.48 | 2.63 | −1.00 | 3.25 | 0.23 | 0.23 | 1.21 | 3.10 | −3.50 | 2.50 | 0.92 | 0.02 | |
| Placebo | 26.50 | 8.93 | 27.88 | 7.20 | −2.25 | 5.25 | 0.87 | 0.03 | 1.38 | 4.89 | ||||||
| 5-m walking (s) | Extract | 1.73 | 0.48 | 1.57 | 0.44 | −0.36 | 0.06 | 0.24 | 0.23 | −0.20 | 0.55 | −0.29 | 0.39 | 0.50 | 0.14 | |
| Placebo | 2.24 | 0.19 | 2.18 | 0.24 | −0.29 | 0.20 | 0.48 | 0.14 | −0.07 | 0.30 | ||||||
| 2-step test (point) | Extract | 0.23 | 0.07 | 0.20 | 0.06 | −0.09 | 0.08 | 0.86 | 0.03 | −0.01 | 0.13 | −0.18 | −0.02 | 0.05 | * | 0.40 |
| Placebo | 1.49 | 0.11 | 1.40 | 0.12 | −0.16 | 0.00 | 0.09 | 0.33 | −0.09 | 0.09 | ||||||
| Stand-up test (point) | Extract | 12.38 | 10.50 | 13.31 | 6.93 | −2.50 | 5.00 | 0.55 | 0.12 | 0.92 | 7.99 | −5.00 | 7.00 | 0.86 | 0.04 | |
| Placebo | 14.00 | 11.83 | 17.00 | 12.10 | −2.50 | 9.50 | 0.46 | 0.15 | 3.00 | 7.75 | ||||||
| GLFS-25 (point) | Extract | 16.55 | 4.59 | 10.89 | 3.02 | −9.50 | 7.50 | 0.64 | 0.09 | −0.08 | 12.78 | −9.00 | 3.00 | 0.34 | 0.20 | |
| Placebo | 8.00 | 3.85 | 7.00 | 5.95 | −4.00 | 2.00 | 0.50 | 0.13 | −1.00 | 3.78 | ||||||
| Over 65 Years (n = 19) | Pre | Post | Intragroup Comparison (Pre vs. Post) | Changed Value (Post-Pre) | Comparison between Group (Extract vs. Placebo) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical Activity | Mean | SD | Mean | SD | 95% CI | p Value | r | Mean | SD | 95% CI | p Value | r | |||||
| Lower | Upper | Lower | Upper | ||||||||||||||
| Hand grip right (kg) | Extract (n = 13) | 10.40 | 2.88 | 9.99 | 2.77 | −1.75 | 2.75 | 0.61 | 0.10 | 0.50 | 4.47 | −3.00 | 6.00 | 0.58 | 0.12 | ||
| Placebo (n = 6) | 29.92 | 7.95 | 31.83 | 7.79 | −1.75 | 6.75 | 0.25 | 0.23 | 1.92 | 4.79 | |||||||
| Hand grip left (kg) | Extract | 9.34 | 2.59 | 9.48 | 2.63 | −1.00 | 3.25 | 0.23 | 0.23 | 1.21 | 3.10 | −4.00 | 7.00 | 1.00 | 0.01 | ||
| Placebo | 27.08 | 10.34 | 28.83 | 8.03 | −3.00 | 8.75 | 0.92 | 0.02 | 1.75 | 5.72 | |||||||
| 5-m walking (s) | Extract | 1.73 | 0.48 | 1.57 | 0.44 | −0.36 | 0.06 | 0.24 | 0.23 | −0.20 | 0.55 | −0.33 | 0.35 | 0.52 | 0.13 | ||
| Placebo | 2.28 | 0.20 | 2.20 | 0.27 | −0.33 | 0.22 | 0.35 | 0.19 | −0.09 | 0.32 | |||||||
| 2-step test (point) | Extract | 0.23 | 0.07 | 0.20 | 0.06 | −0.09 | 0.08 | 0.86 | 0.03 | −0.01 | 0.13 | −0.21 | −0.04 | 0.01 | ** | 0.48 | |
| Placebo | 1.53 | 0.10 | 1.41 | 0.13 | −0.17 | −0.08 | 0.03 | * | 0.43 | −0.12 | 0.05 | ||||||
| Stand-up test (point) | Extract | 12.38 | 10.50 | 13.31 | 6.93 | −2.50 | 5.00 | 0.55 | 0.12 | 0.92 | 7.99 | −5.00 | 9.00 | 1.00 | 0.00 | ||
| Placebo | 14.83 | 12.80 | 17.67 | 13.88 | −5.00 | 11.50 | 0.89 | 0.03 | 2.83 | 8.89 | |||||||
| GLFS-25 (point) | Extract | 16.55 | 4.59 | 10.89 | 3.02 | −9.50 | 7.50 | 0.64 | 0.09 | −0.08 | 12.78 | −11.00 | 5.00 | 0.42 | 0.17 | ||
| Placebo | 8.83 | 4.17 | 8.00 | 6.66 | −4.50 | 3.50 | 0.72 | 0.07 | −0.83 | 4.36 | |||||||
| Changed Values | Between Groups | |||||||
|---|---|---|---|---|---|---|---|---|
| Placebo | Extract | p Value | 95% CI | |||||
| Mean | SD | Mean | SD | |||||
| HDL-cholesterol | −3.27 | 5.76 | −1.73 | 7.47 | 0.57 | −4.04 | to | 7.12 |
| Total protein | −0.01 | 0.24 | −0.01 | 0.23 | 0.96 | −0.20 | to | 0.19 |
| Billirubin direct | 0.01 | 0.03 | 0.01 | 0.03 | 0.83 | −0.03 | to | 0.02 |
| Billirubin indirect | 0.01 | 0.07 | 0.05 | 0.12 | 0.38 | −0.05 | to | 0.12 |
| Glucose | −2.18 | 17.71 | 0.33 | 13.79 | 0.69 | −10.22 | to | 15.25 |
| Total cholesterol | −1.00 | 12.30 | 4.33 | 15.46 | 0.35 | −6.33 | to | 16.99 |
| Triglyceride | 13.91 | 72.02 | 53.27 | 166.34 | 0.47 | −71.48 | to | 150.20 |
| Urea nitrogen | 0.95 | 2.37 | 0.07 | 3.10 | 0.43 | −3.19 | to | 1.42 |
| Creatinine | 0.02 | 0.03 | 0.01 | 0.11 | 0.72 | −0.09 | to | 0.06 |
| Uric acid | −0.03 | 0.40 | 0.01 | 0.63 | 0.88 | −0.41 | to | 0.48 |
| Na | 1.18 | 1.25 | 0.00 | 1.00 | 0.01 * | −2.09 | to | −0.27 |
| K | 0.03 | 0.36 | −0.01 | 0.29 | 0.79 | −0.30 | to | 0.23 |
| Cl | 0.36 | 2.25 | −0.33 | 1.11 | 0.31 | −2.08 | to | 0.68 |
| Amylase | −11.64 | 37.07 | −0.67 | 5.18 | 0.27 | −8.90 | to | 30.84 |
| Creatine kinase | −3.82 | 16.68 | −0.13 | 24.15 | 0.67 | −13.81 | to | 21.18 |
| Leucine aminopeptidase | 5.27 | 8.82 | −0.47 | 4.03 | 0.04 * | −11.04 | to | −0.44 |
| γ-GTP | 4.00 | 9.07 | −0.53 | 5.48 | 0.13 | −10.43 | to | 1.36 |
| Cholinesterase | −1.00 | 26.80 | 2.47 | 28.54 | 0.76 | −19.33 | to | 26.27 |
| AST(GOT) | 1.55 | 4.27 | −1.27 | 4.03 | 0.10 | −6.20 | to | 0.57 |
| ALT(GPT) | 1.91 | 5.05 | −0.07 | 6.92 | 0.43 | −7.06 | to | 3.11 |
| Lactate dehydorogenase | −0.36 | 20.25 | −6.33 | 34.14 | 0.61 | −29.87 | to | 17.93 |
| Alkaline phosphatase | −11.00 | 30.41 | 12.87 | 68.34 | 0.29 | −21.82 | to | 69.55 |
| Hemoglobin | −0.08 | 0.56 | 0.00 | 0.49 | 0.70 | −0.34 | to | 0.51 |
| Erythrocytes | −1.45 | 24.86 | −0.07 | 18.48 | 0.87 | −16.12 | to | 18.90 |
| Leukocytes | −300.00 | 734.85 | −280.00 | 838.54 | 0.95 | −632.90 | to | 672.90 |
| Hematocrit | −0.64 | 2.35 | −0.47 | 1.59 | 0.83 | −1.43 | to | 1.76 |
| Erythrocyte mean corpuscular volume | −1.12 | 0.94 | −1.17 | 1.55 | 0.92 | −1.15 | to | 1.04 |
| Erythrocyte mean corpuscular hemoglobin | −0.12 | 0.47 | −0.03 | 0.64 | 0.71 | −0.39 | to | 0.56 |
| Erythrocyte mean corpuscular hemoglobin concentration | 0.27 | 0.55 | 0.36 | 0.46 | 0.66 | −0.32 | to | 0.50 |
| Platelet | −0.82 | 2.70 | −0.82 | 2.57 | 1.00 | −2.15 | to | 2.15 |
| LDL-cholesterol | −0.18 | 11.36 | 1.20 | 14.09 | 0.79 | −9.29 | to | 12.05 |
| Albumin | 0.05 | 0.15 | 0.02 | 0.25 | 0.77 | −0.20 | to | 0.15 |
| Albumin | 0.75 | 1.45 | 0.47 | 1.79 | 0.67 | −1.64 | to | 1.07 |
| A1-G | −0.04 | 0.21 | −0.20 | 0.37 | 0.20 | −0.42 | to | 0.09 |
| A2-G | −0.19 | 0.43 | −0.15 | 0.62 | 0.86 | −0.41 | to | 0.49 |
| B1-G | −0.18 | 0.31 | −0.17 | 0.45 | 0.96 | −0.32 | to | 0.33 |
| B2-G | −0.07 | 0.22 | −0.07 | 0.60 | 1.00 | −0.39 | to | 0.39 |
| G-G | −0.27 | 0.85 | 0.13 | 0.56 | 0.15 | −0.16 | to | 0.97 |
| A/G | 0.05 | 0.09 | 0.05 | 0.09 | 0.97 | −0.07 | to | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inada, Y.; Tohda, C.; Yang, X. Effects of Cistanche tubulosa Wight Extract on Locomotive Syndrome: A Placebo-Controlled, Randomized, Double-Blind Study. Nutrients 2021, 13, 264. https://doi.org/10.3390/nu13010264
Inada Y, Tohda C, Yang X. Effects of Cistanche tubulosa Wight Extract on Locomotive Syndrome: A Placebo-Controlled, Randomized, Double-Blind Study. Nutrients. 2021; 13(1):264. https://doi.org/10.3390/nu13010264
Chicago/Turabian StyleInada, Yuna, Chihiro Tohda, and Ximeng Yang. 2021. "Effects of Cistanche tubulosa Wight Extract on Locomotive Syndrome: A Placebo-Controlled, Randomized, Double-Blind Study" Nutrients 13, no. 1: 264. https://doi.org/10.3390/nu13010264
APA StyleInada, Y., Tohda, C., & Yang, X. (2021). Effects of Cistanche tubulosa Wight Extract on Locomotive Syndrome: A Placebo-Controlled, Randomized, Double-Blind Study. Nutrients, 13(1), 264. https://doi.org/10.3390/nu13010264