
Iodine Intake from Food and Iodized Salt as Related to Dietary Salt Consumption in the Italian Adult General Population

 ,
,  , , , ,
, , , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
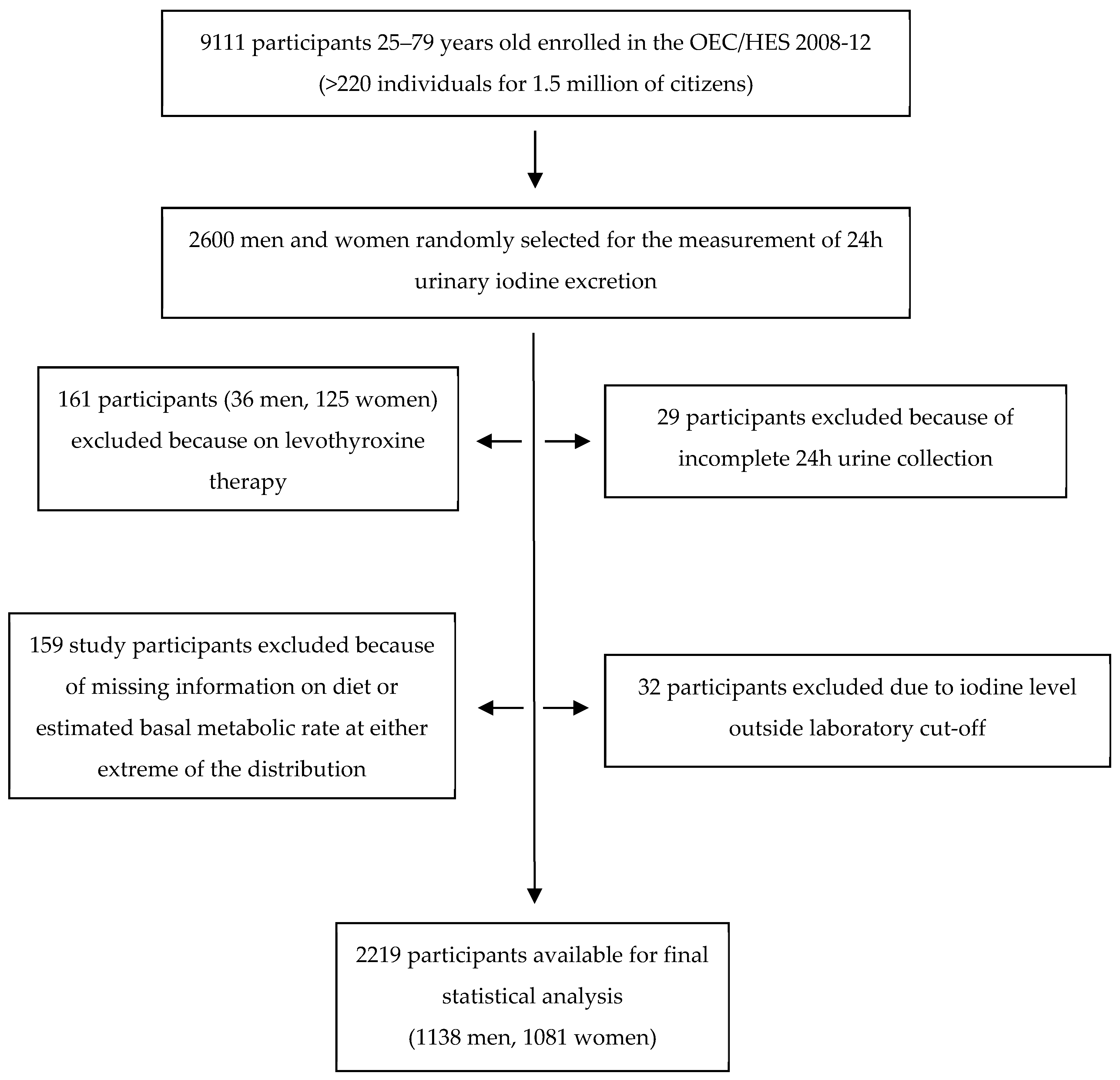
2.1. Study Population and Survey Protocol
2.2. Study Procedures
2.2.1. Protocol for the Estimation of Salt Consumption and Iodine Intake
2.2.2. Estimation of Dietary Iodine and Iodized Salt Consumption
2.3. Statistical Analysis
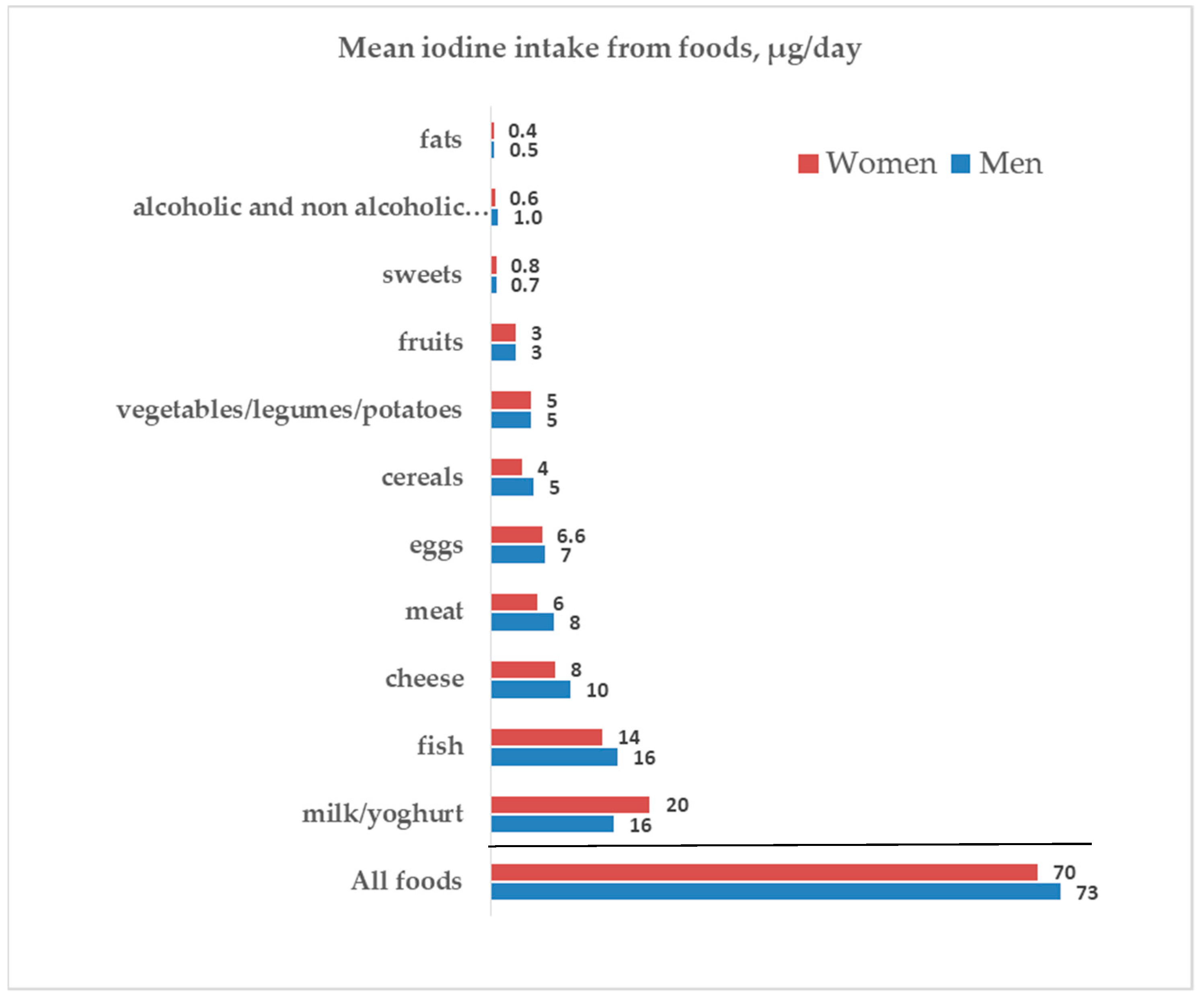
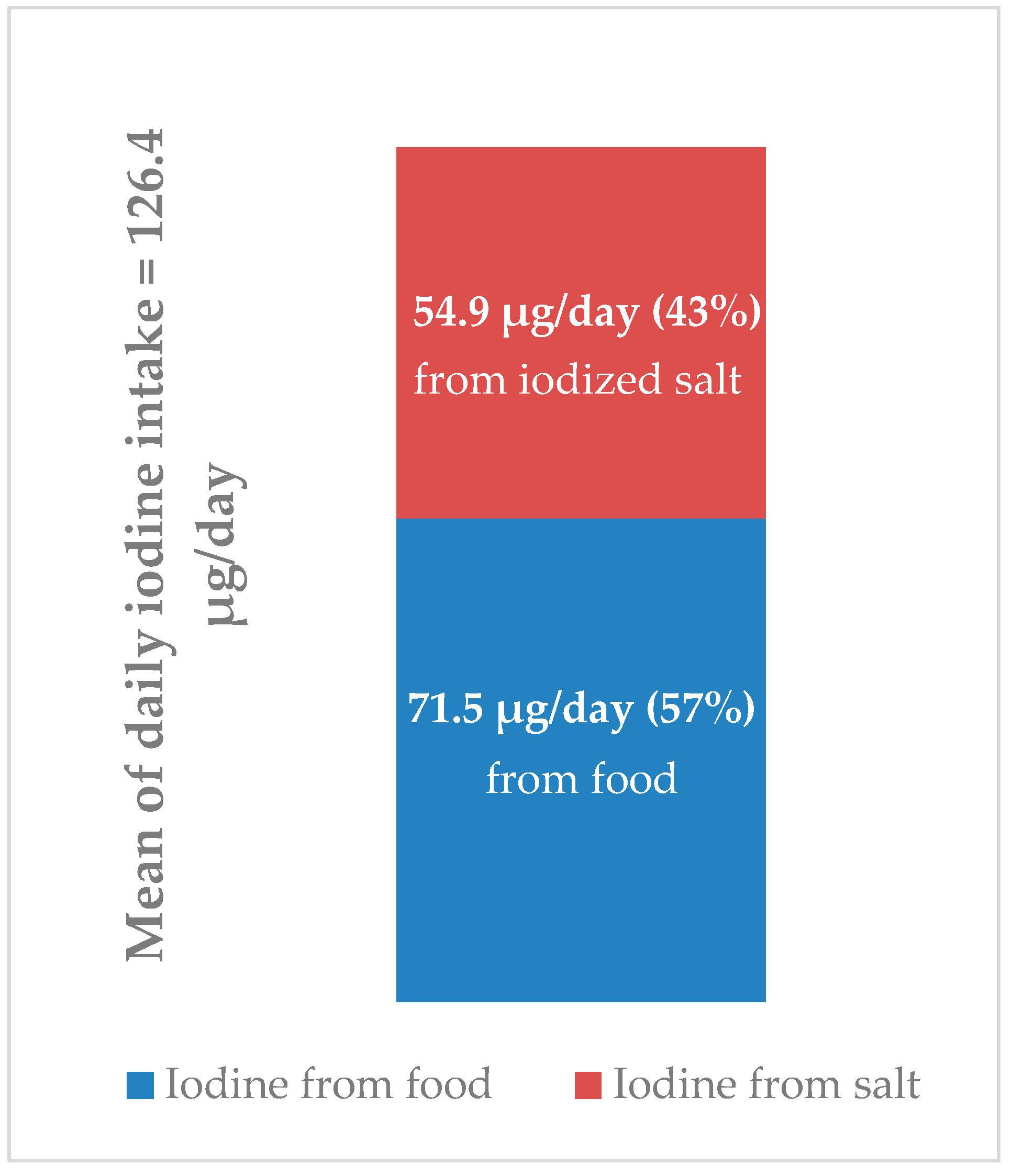
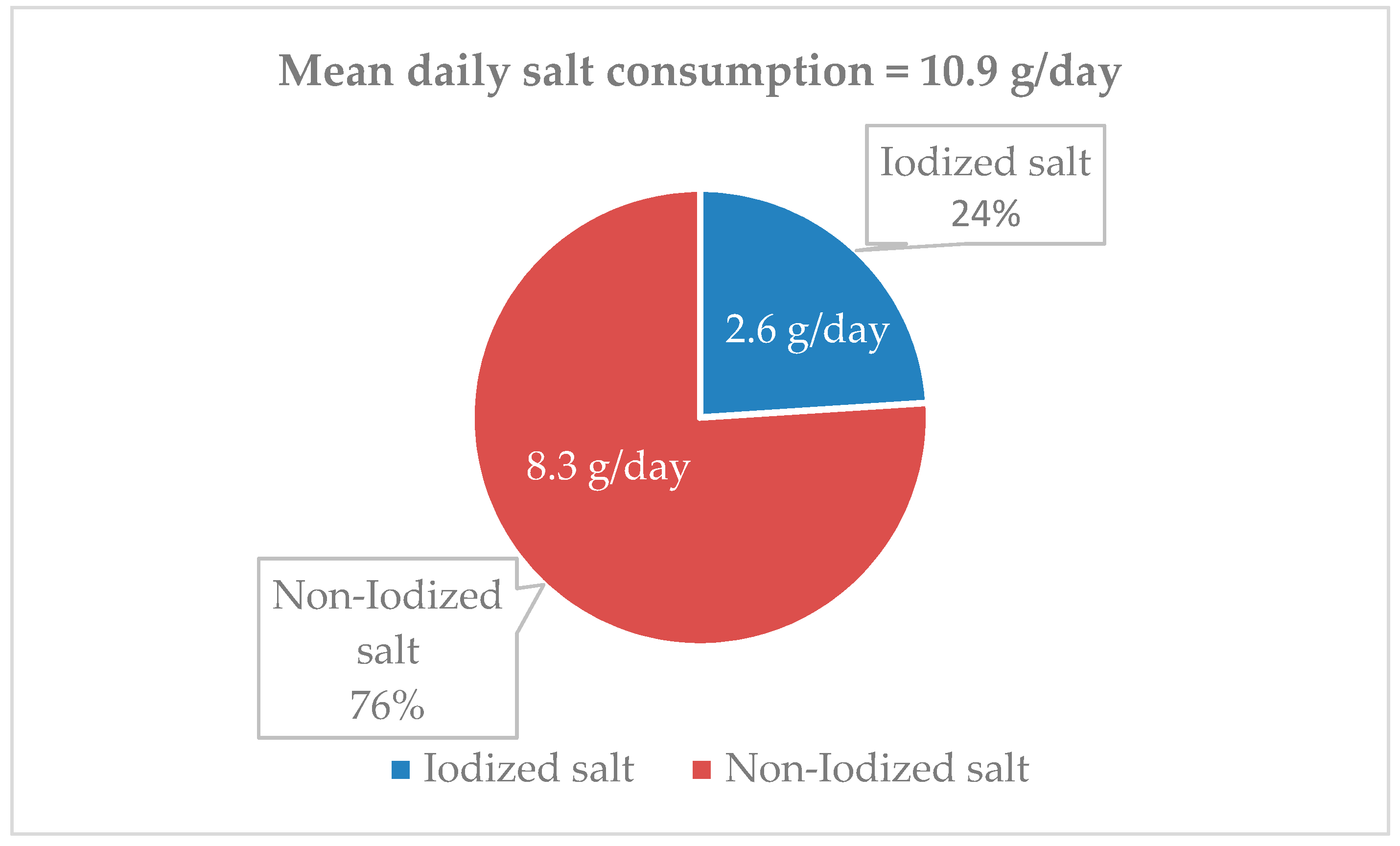
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions and Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Guideline: Fortification of Food-Grade Salt with Iodine for the Prevention and Control of Iodine Deficiency Disorders; World Health Organization: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/bitstream/handle/10665/136908/9789241507929_eng.pdf?ua=1 (accessed on 23 July 2021).
- WHO; UNICEF; ICCIDD. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination; World Health Organization: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/bitstream/handle/10665/43781/9789241595827_eng.pdf (accessed on 23 July 2021).
- Salt as a Vehicle for Fortifcation. In Report of a WHO Expert Consultant; World Health Organization: Luxembourg, 2007; Available online: https://apps.who.int/iris/bitstream/handle/10665/43908/9789241596787_eng.pdf?ua=1 (accessed on 23 July 2021).
- Law 21 March 55/2005. Available online: https://www.gazzettaufficiale.it/eli/gu/2005/04/20/91/sg/pdf (accessed on 23 July 2021).
- WHO. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting World Health Organization 2007. Available online: https://www.who.int/dietphysicalactivity/Salt_Report_VC_april07.pdf (accessed on 23 July 2021).
- D’Elia, L.; Galletti, F.; La Fata, E.; Sabino, P.; Strazzullo, P. Effect of dietary sodium restriction on arterial stiffness: Systematic review and meta-analysis of the randomized controlled trials. J. Hypertens. 2018, 36, 734–743. [Google Scholar] [CrossRef]
- WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 23 July 2021).
- Donfrancesco, C.; Ippolito, R.; Lo Noce, C.; Palmieri, L.; Iacone, R.; Russo, O.; Vanuzzo, D.; Galletti, F.; Galeone, D.; Giampaoli, S.; et al. Excess dietary sodium and inadequate potassium intake in Italy: Results of the MINISAL study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 850–856. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socioeconomic variation of sodium and potassium intake in Italy: Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar] [CrossRef] [Green Version]
- Iacone, R.; Iaccarino Idelson, P.; Formisano, P.; Russo, O.; Lo Noce, C.; Donfrancesco, C.; Macchia, P.E.; Palmieri, L.; Galeone, D.; di Lenarda, A.; et al. Iodine Intake Estimated by 24h Urine Collection in the Italian Adult Population: 2008–2012 Survey. Nutrients 2021, 13, 1529. [Google Scholar] [CrossRef]
- Giampaoli, S.; Palmieri, L.; Donfrancesco, C.; Lo Noce, C.; Pilotto, L.; Vanuzzo, D. Osservatorio Epidemiologico Cardiovascolare/Health Examination Survey Research Group. Cardiovascular health in Italy. Ten-year surveillance of cardiovascular diseases and risk factors: Osservatorio Epidemiologico Cardiovascolare/Health Examination Survey 1998–2012. Eur. J. Prev. Cardiol. 2015, 22 (Suppl. S2), 9–37. [Google Scholar]
- Donfrancesco, C.; Lo Noce, C.; Russo, O.; Minutoli, D.; Di Lonardo, A.; Profumo, E.; Buttari, B.; Iacone, R.; Vespasiano, F.; Vannucchi, S.; et al. Trend of salt intake measured by 24-h urine collection in the Italian adult population between the 2008 and 2018 CUORE Project surveys. NMCD 2020, 31, 802–813. [Google Scholar] [CrossRef] [PubMed]
- Pisani, P.; Faggiano, F.; Krogh, V.; Palli, D.; Vineis, P.; Berrino, F. Relative validity and reproducibility of a food frequency dietary questionnaire for use in the Italian EPIC centres. Int. J. Epidemiol. 1997, 26 (Suppl. S1), S152–S160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanozzi, A.; Rutigliano, I.; Macchia, P.E.; De Filippo, G.; Barbato, A.; Iacone, R.; Russo, O.; D’Angelo, G.; Frigeri, M.; Pensabene, L.; et al. Iodine deficiency among Italian children and adolescents assessed through 24-hour urinary iodine excretion. Am. J. Clin. Nutr. 2019, 109, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; The National Academies Press: Washington, DC, USA, 2001; p. 264. [Google Scholar] [CrossRef] [Green Version]
- EFSA NDA Panel (EFSA Panel on Panel on Dietetic Products Nutrition and Allergies). Scientific Opinion on Dietary Ref-erence Values for iodine. EFSA J. 2014, 12, 3660. Available online: https://efsa.onlinelibrary.wiley.com/doi/epdf/10.2903/j.efsa.2014.3660 (accessed on 23 July 2021). [CrossRef] [Green Version]
- Cogswell, M.E.; Maalouf, J.; Elliott, P.; Loria, C.M.; Patel, S.; Bowman, B.A. Use of Urine Biomarkers to Assess Sodium Intake: Challenges and Opportunities. Annu. Rev. Nutr. 2015, 35, 349–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvini, S.; Parpinel, M.; Gnagnarella, P.; Maissoneuve, P.; Turrini, A. Banca Dati di Composizione Degli Alimenti Per Studi Epidemiologici in Italia; European Institute of Oncology: Milan, Italy, 1998; Available online: http://www.bda-ieo.it/wordpress/en (accessed on 23 July 2021).
- Pastorelli, A.A.; Stacchini, P.; Olivieri, A. Daily iodine intake and the impact of salt reduction on iodine prophylaxis in the Italian population. Eur. J. Clin. Nutr. 2015, 69, 211–215. [Google Scholar] [CrossRef]
- Iacone, R.; Iaccarino Idelson, P.; Campanozzi, A.; Rutigliano, I.; Russo, O.; Formisano, P.; Galeone, D.; Macchia, P.E.; Strazzullo, P. MINISAL-GIRCSI Study Group. Relationship between salt consumption and iodine intake in a pediatric population. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef]
- Leclercq, C.; Arcella, D.; Piccinelli, R.; Sette, S.; Le Donne, C.; Turrini, A. INRAN-SCAI 2005-06 Study Group. The Italian National Food Consumption Survey INRAN-SCAI 2005-06: Main results in terms of food consumption. Public Health Nutr. 2009, 12, 2504–2532. [Google Scholar] [CrossRef] [Green Version]
- Olivieri, A.; Vitti, P. Istituto Superiore Di Sanità. Rapporti ISTISAN 14/6. Attività Di Monitoraggio Del Programma Nazionale per la Prevenzione Dei Disordini Da Carenza Iodica. Epidemiologia E Sanità Pubblica. 2014. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2375_allegato.pdf (accessed on 19 July 2021).
- Leclercq, C.; Ferro-Luzzi, A. Total and domestic consumption of salt and their determinants in three regions of Italy. Eur. J. Clin. Nutr. 1991, 45, 151–159. [Google Scholar] [PubMed]
- Iaccarino Idelson, P.; D’Elia, L.; Cairella, G.; Sabino, P.; Scalfi, L.; Fabbri, A.; Galletti, F.; Garbagnati, F.; Lionetti, L.; Paolella, G.; et al. On Behalf Of The Sinu-Gircsi Working Group. Salt and Health: Survey on Knowledge and Salt Intake Related Behaviour in Italy. Nutrients 2020, 12, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Istituto Superiore di Sanità. L’epidemiologia per La Sanità Pubblica: Sorveglianza PASSI. Available online: https://www.epicentro.iss.it/passi/dati/sale (accessed on 19 July 2021).
- Consiglio per La Ricerca in Agricoltura E L’analisi Dell’economia Agraria (CREA). Linee Guida per Una Sana Alimentazione. Revisione. 2018. Available online: https://www.crea.gov.it/documents/59764/0/LINEE-GUIDA+DEFINITIVO.pdf/28670db4-154c-0ecc-d187-1ee9db3b1c65?t=1576850671654 (accessed on 19 July 2021).
- Zimmermann, M.B.; Aeberli, I.; Torresani, T.; Bürgi, H. Increasing the iodine concentration in the Swiss iodized salt program markedly improved iodine status in pregnant women and children: A 5-y prospective national study. Am. J. Clin. Nutr. 2005, 82, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Haldimann, M.; Bochud, M.; Burnier, M.; Paccaud, F.; Dudler, V. Prevalence of iodine inadequacy in Switzerland assessed by the estimated average requirement cut-point method in relation to the impact of iodized salt. Public Health Nutr. 2015, 18, 1333–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remer, T.; Neubert, A. A never-ending story of an insufficient iodine status without mandatory iodization of foods? A German experience. J. Clin. Endocrinol. Metab. 1998, 83, 3755–3756. [Google Scholar] [CrossRef]
- Esche, J.; Thamm, M.; Remer, T. Contribution of iodized salt to total iodine and total salt intake in Germany. Eur. J. Nutr. 2020, 59, 3163–3169. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.; Ware, L.J.; Menyanu, E.; Biritwum, R.B.; Naidoo, N.; Pieterse, C.; Madurai, S.; Baumgartner, J.; Asare, G.A.; Thiele, E.; et al. Leveraging ongoing research to evaluate the health impacts of South Africa’s salt reduction strategy: A prospective nested cohort within the WHO-SAGE multicountry, longitudinal study. BMJ Open 2016, 6, e013316. [Google Scholar] [CrossRef] [Green Version]
- He, F.J.; Wu, Y.; Feng, X.X.; Ma, J.; Ma, Y.; Wang, H.; Zhang, J.; Yuan, J.; Lin, C.P.; Nowson, C.; et al. School based education programme to reduce salt intake in children and their families (School-Edu Salt): Cluster randomised controlled trial. BMJ 2015, 350, h770. [Google Scholar] [CrossRef] [Green Version]
- König, F.; Andersson, M.; Hotz, K.; Aeberli, I.; Zimmermann, M.B. Ten repeat collections for urinary iodine from spot samples or 24-hour samples are needed to reliably estimate individual iodine status in women. J. Nutr. 2011, 141, 2049–2054. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Population n = 2219 | Men n = 1138 | Women n = 1081 | p * | |
|---|---|---|---|---|
| Age, years | 56 (46–66) | 56 (45–66) | 57 (46–67) | 0.304 |
| BMI, kg/m2 | 26.7 (24.0–30.2) | 27.1 (24.9–30.2) | 26.1 (23.0–30.2) | <0.001 |
| Salt consumption, g/day | 10.2 (7.8–13.3) | 11.7 (8.9–14.9) | 9.1 (6.8–11.5) | <0.001 |
| Iodine intake, µg/day | 95 (51–165) | 110 (60–189) | 84 (43–138) | <0.001 |
| Whole Population | I Quintile | II Quintile | III Quintile | IV Quintile | V Quintile |
|---|---|---|---|---|---|
| n = 444 | n = 444 | n = 444 | n = 443 | n = 444 | |
| Salt intake | 5.8 (4.9–6.5) | 8.3 (7.8–8.8) | 10.2 (9.7–10.8) | 12.6 (11.9–13.3) | 16.7 (15.3–19.3) |
| Iodine intake | 61 * (29–105) | 82 * (48–130) | 96 * (51–154) | 111 * (67–177) | 148 (78–231) |
| Men | I quintile | II quintile | III quintile | IV quintile | V quintile |
| n = 228 | n = 228 | n = 227 | n = 227 | n = 228 | |
| Salt intake | 6.8 (5.7–7.4) | 9.4 (8.9–9.9) | 11.7 (11.2–12.4) | 14.0 (13.5–14.9) | 18.1 (16.6–21.1) |
| Iodine intake | 68 * (37–113) | 93 * (55–152) | 119 * (71–179) | 134 * (75–201) | 174 (85–240) |
| Women | I quintile | II quintile | III quintile | IV quintile | V quintile |
| n = 216 | n = 216 | n = 217 | n = 216 | n = 216 | |
| Salt intake | 5.3 (4.2–5.8) | 7.3 (6.8–7.8) | 9.1 (8.6–9.5) | 10.9 (10.3–11.5) | 14.2 (12.9–16.4) |
| Iodine intake | 52 * (25–95) | 78 * (44–120) | 91 * (52–147) | 89 * (45–148) | 120 * (66–186) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iacone, R.; Iaccarino Idelson, P.; Russo, O.; Donfrancesco, C.; Krogh, V.; Sieri, S.; Macchia, P.E.; Formisano, P.; Lo Noce, C.; Palmieri, L.; et al. Iodine Intake from Food and Iodized Salt as Related to Dietary Salt Consumption in the Italian Adult General Population. Nutrients 2021, 13, 3486. https://doi.org/10.3390/nu13103486
Iacone R, Iaccarino Idelson P, Russo O, Donfrancesco C, Krogh V, Sieri S, Macchia PE, Formisano P, Lo Noce C, Palmieri L, et al. Iodine Intake from Food and Iodized Salt as Related to Dietary Salt Consumption in the Italian Adult General Population. Nutrients. 2021; 13(10):3486. https://doi.org/10.3390/nu13103486
Chicago/Turabian StyleIacone, Roberto, Paola Iaccarino Idelson, Ornella Russo, Chiara Donfrancesco, Vittorio Krogh, Sabina Sieri, Paolo Emidio Macchia, Pietro Formisano, Cinzia Lo Noce, Luigi Palmieri, and et al. 2021. "Iodine Intake from Food and Iodized Salt as Related to Dietary Salt Consumption in the Italian Adult General Population" Nutrients 13, no. 10: 3486. https://doi.org/10.3390/nu13103486
APA StyleIacone, R., Iaccarino Idelson, P., Russo, O., Donfrancesco, C., Krogh, V., Sieri, S., Macchia, P. E., Formisano, P., Lo Noce, C., Palmieri, L., Galeone, D., Rendina, D., Galletti, F., Di Lenarda, A., Giampaoli, S., Strazzullo, P., & on behalf of the MINISAL-GIRCSI Study Group. (2021). Iodine Intake from Food and Iodized Salt as Related to Dietary Salt Consumption in the Italian Adult General Population. Nutrients, 13(10), 3486. https://doi.org/10.3390/nu13103486