
Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders

 ,
,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Subjects
2.2. Variables and Data Collection
2.3. Statistical Analysis
2.3.1. General Analyses
2.3.2. Dietary Patterns
2.3.3. Dietary Patterns with Clustering Analysis
3. Results
3.1. Subjects Characteristics
3.2. Food Group Consumption According to Food Frequency Questionnaires and Adequacy to the Spanish Society of Community Nutrition (SENC) Dietary Guidelines
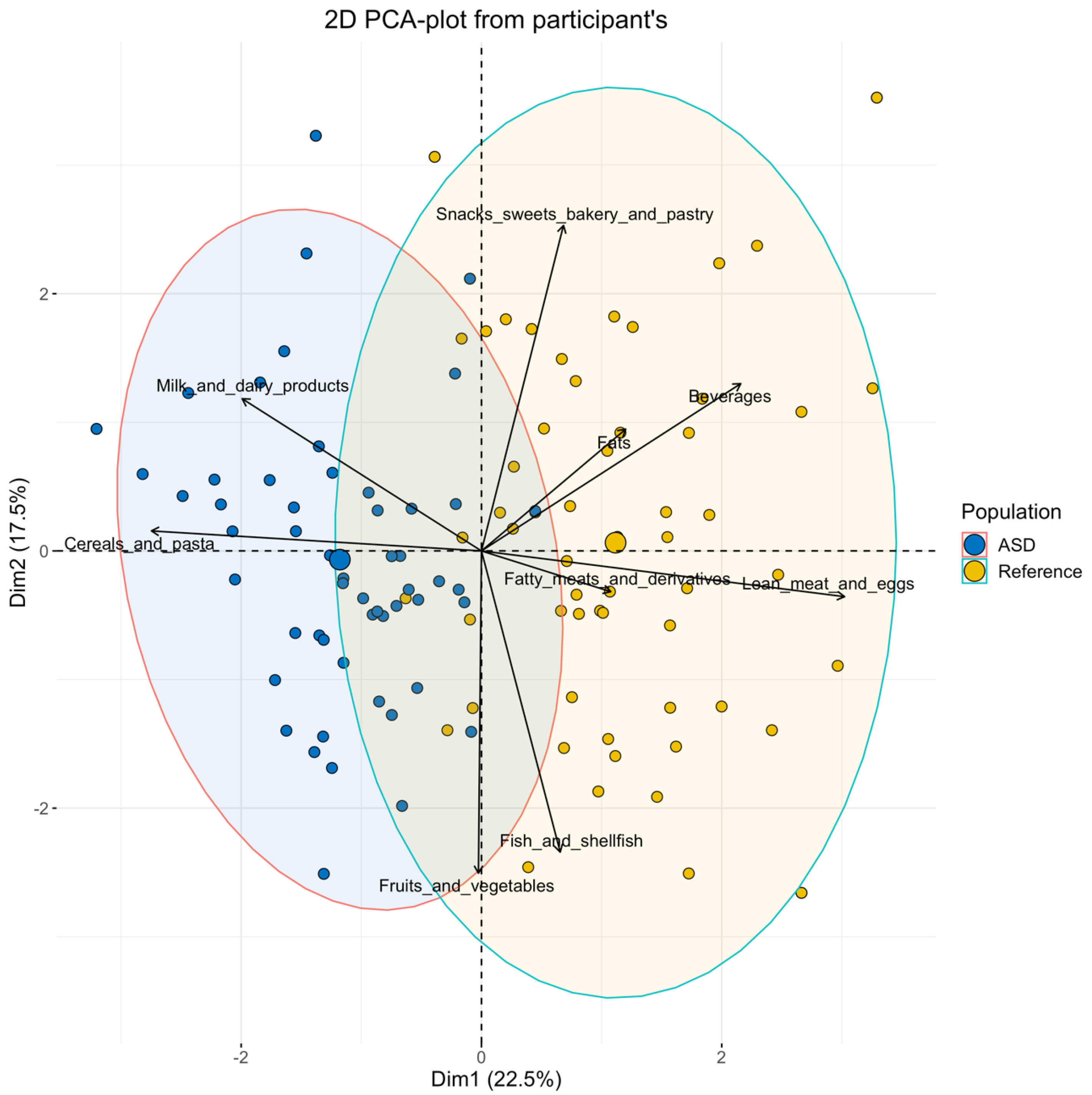
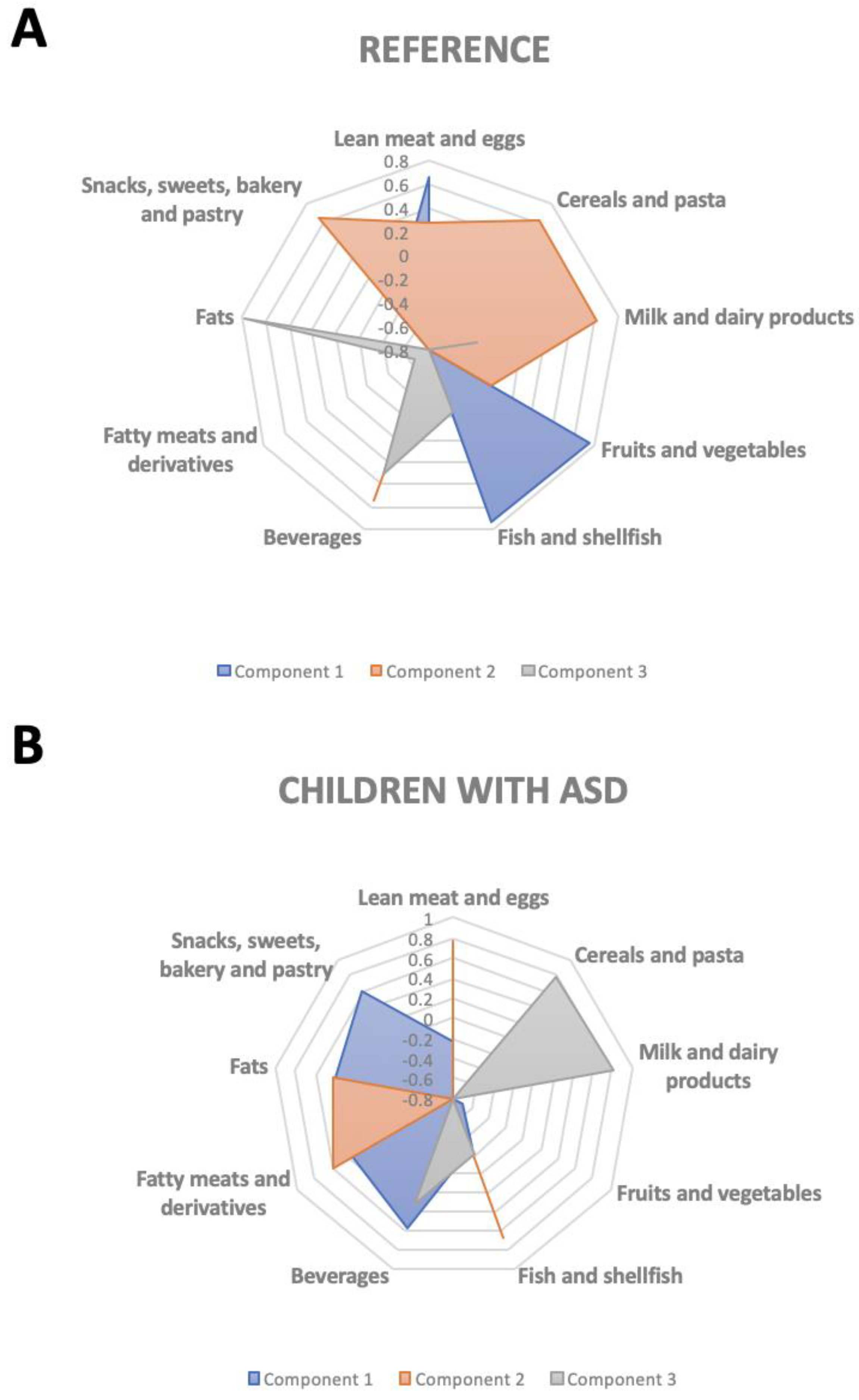
3.3. Dietary Patterns
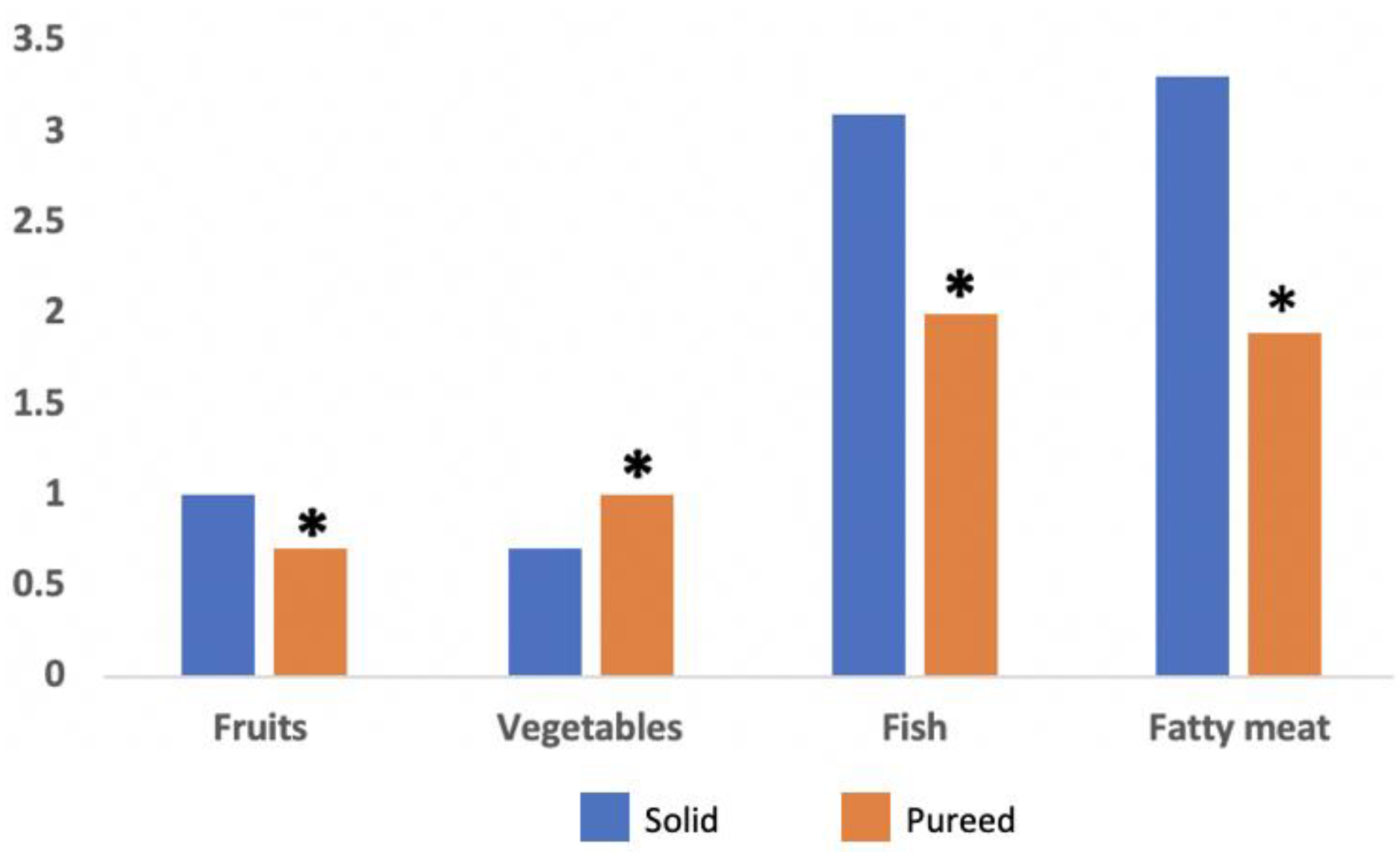
3.4. Eating Behavior
3.5. Adequacy of Nutrient Intakes to the European Food Safety Authority (EFSA) Recommendations
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychology Association. Paraphilic Disorders. Diagnostic and Statistical Manual of Mental Disorders; American Psychology Association: Washington, DC, USA, 2013; Volume 5, pp. 685–686. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Baio, J. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1. [Google Scholar] [CrossRef]
- Williams, P.G.; Dalrymple, N.; Neal, J. Eating habits of children with autism. Pediatr. Nurs. 2000, 26, 259. [Google Scholar]
- Ranjan, S.; Nasser, J.A. Nutritional status of individuals with autism spectrum disorders: Do we know enough? Adv. Nutr. 2015, 6, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Lázaro, C.P.; Pondé, M.P. Narratives of mothers of children with autism spectrum disorders: Focus on eating behavior. Trends Psychiatry Psychother. 2017, 39, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledford, J.R.; Gast, D.L. Feeding problems in children with autism spectrum disorders: A review. Focus Autism Other Dev. Disabil. 2006, 21, 153–166. [Google Scholar] [CrossRef] [Green Version]
- Råstam, M. Eating disturbances in autism spectrum disorders with focus on adolescent and adult years. Clin. Neuropsychiatry J. Treat. Eval. 2008, 5, 31–42. [Google Scholar]
- Brzoska, A.; Kazek, B.; Koziol, K.; Kapinos-Gorczyca, A.; Ferlewicz, M.; Babraj, A.; Makosz-Raczek, A.; Likus, W.; Paprocka, J.; Matusik, P.; et al. Eating Behaviors of Children with Autism-Pilot Study. Nutrients 2021, 13, 2687. [Google Scholar] [CrossRef] [PubMed]
- Schreck, K.A.; Williams, K.; Smith, A.F. A comparison of eating behaviors between children with and without autism. J. Autism Dev. Disord. 2004, 34, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, K.L.; Anderson, S.E.; Curtin, C.; Must, A.; Bandini, L.G. A comparison of food refusal related to characteristics of food in children with autism spectrum disorder and typically developing children. J. Acad. Nutr. Diet. 2014, 114, 1981–1987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyman, S.L.; Levy, S.E.; Myers, S.M. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wigham, S.; Rodgers, J.; South, M.; McConachie, H.; Freeston, M. The interplay between sensory processing abnormalities, intolerance of uncertainty, anxiety and restricted and repetitive behaviours in autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Geraghty, M.E.; Depasquale, G.M.; Lane, A.E. Nutritional intake and therapies in autism: A spectrum of what we know: Part 1. ICAN Infant Child Adolesc. Nutr. 2010, 2, 62–69. [Google Scholar] [CrossRef]
- Lukens, C.T.; Linscheid, T.R. Development and validation of an inventory to assess mealtime behavior problems in children with autism. J. Autism Dev. Disord. 2008, 38, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Sharp, W.G.; Berry, R.C.; McCracken, C.; Nuhu, N.N.; Marvel, E.; Saulnier, C.A.; Klin, A.; Jones, W.; Jaquess, D.L. Feeding problems and nutrient intake in children with autism spectrum disorders: A meta-analysis and comprehensive review of the literature. J. Autism Dev. Disord. 2013, 43, 2159–2173. [Google Scholar] [CrossRef] [PubMed]
- Baumer, N.; Spence, S.J. Evaluation and management of the child with autism spectrum disorder. Contin. Lifelong Learn. Neurol. 2018, 24, 248–275. [Google Scholar] [CrossRef]
- Bennetto, L.; Kuschner, E.S.; Hyman, S.L. Olfaction and taste processing in autism. Biol. Psychiatry 2007, 62, 1015–1021. [Google Scholar] [CrossRef] [Green Version]
- Bresnahan, M.; Hornig, M.; Schultz, A.F.; Gunnes, N.; Hirtz, D.; Lie, K.K.; Magnus, P.; Reichborn-Kjennerud, T.; Roth, C.; Schjølberg, S. Association of maternal report of infant and toddler gastrointestinal symptoms with autism: Evidence from a prospective birth cohort. JAMA Psychiatry 2015, 72, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Samsam, M.; Ahangari, R.; Naser, S.A. Pathophysiology of autism spectrum disorders: Revisiting gastrointestinal involvement and immune imbalance. World J. Gastroenterol. WJG 2014, 20, 9942. [Google Scholar] [CrossRef]
- Margari, L.; Marzulli, L.; Gabellone, A.; de Giambattista, C. Eating and Mealtime Behaviors in Patients with Autism Spectrum Disorder: Current Perspectives. Neuropsychiatr Dis. Treat. 2020, 16, 2083–2102. [Google Scholar] [CrossRef]
- Canals-Sans, J.; Esteban-Figuerola, P.; Morales-Hidalgo, P.; Arija, V. Do Children with Autism Spectrum Disorders Eat Differently and Less Adequately than Those with Subclinical ASD and Typical Development? EPINED Epidemiological Study. J. Autism Dev. Disord. 2021. [Google Scholar] [CrossRef]
- Stepanova, E.; Dowling, S.; Phelps, M.; Findling, R.L. Pharmacotherapy of emotional and behavioral symptoms associated with autism spectrum disorder in children and adolescents. Dialogues Clin. Neurosci. 2017, 19, 395. [Google Scholar]
- DeFilippis, M. The use of complementary alternative medicine in children and adolescents with autism Spectrum disorder. Psychopharmacol. Bull. 2018, 48, 40. [Google Scholar] [PubMed]
- Nath, D. Complementary and alternative medicine in the school-age child with autism. J. Pediatr. Health Care 2017, 31, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Posar, A.; Visconti, P. Complementary and alternative medicine in autism: The question of omega-3. Pediatr. Ann. 2016, 45, e103–e107. [Google Scholar] [CrossRef]
- Hopf, K.P.; Madren, E.; Santianni, K.A. Use and perceived effectiveness of complementary and alternative medicine to treat and manage the symptoms of autism in children: A survey of parents in a community population. J. Altern. Complement. Med. 2016, 22, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Hernandez, F.; Gomez-Fernandez, A.R.; la Torre-Aguilar, M.J.; Perez-Navero, J.L.; Flores-Rojas, K.; Martin-Borreguero, P.; Gil-Campos, M. Neurotoxicity by mercury is not associated with autism spectrum disorders in Spanish children. Ital. J. Pediatr. 2020, 46, 19. [Google Scholar] [CrossRef]
- Hernandez, M.; Castellet, J.; Narvaiza, J.; Rincón, J.; Ruiz, E.; Sánchez, E.; Sobradillo, B.; Zurimendi, A. Curvas y Tablas de Crecimiento; Instituto de Investigación Sobre Crecimiento y Desarrollo; Fundación Faustino Orbegozo: Bilbao, Spain, 2002. [Google Scholar]
- Kim, S.H.; Thurm, A.; Shumway, S.; Lord, C. Multisite study of new autism diagnostic interview-revised (ADI-R) algorithms for toddlers and young preschoolers. J. Autism Dev. Disord. 2013, 43, 1527–1538. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranceta-Bartrina, J.; Partearroyo, T.; López-Sobaler, A.M.; Ortega, R.M.; Varela-Moreiras, G.; Serra-Majem, L.; Pérez-Rodrigo, C. Updating the Food-Based Dietary Guidelines for the Spanish Population: The Spanish Society of Community Nutrition (SENC) Proposal. Nutrients 2019, 11, 2675. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. 2013, 11, 3408. [Google Scholar]
- Alamri, E.S. Efficacy of gluten-and casein-free diets on autism spectrum disorders in children. Saudi Med. J. 2020, 41, 1041–1046. [Google Scholar] [CrossRef]
- Horvath, A.; Łukasik, J.; Szajewska, H. ω-3 fatty acid supplementation does not affect autism spectrum disorder in children: A systematic review and meta-analysis. J. Nutr. 2017, 147, 367–376. [Google Scholar] [CrossRef]
- Mari-Bauset, S.; Zazpe, I.; Mari-Sanchis, A.; Llopis-Gonzalez, A.; Morales-Suarez-Varela, M. Evidence of the gluten-free and casein-free diet in autism spectrum disorders: A systematic review. J. Child Neurol. 2014, 29, 1718–1727. [Google Scholar] [CrossRef]
- Reissmann, A.; Hauser, J.; Makulska-Gertruda, E.; Tomsa, L.; Lange, K.W. Gluten-free and casein-free diets in the treatment of autism. Funct. Foods Health Dis. 2014, 4, 349–361. [Google Scholar] [CrossRef]
- Emond, A.; Emmett, P.; Steer, C.; Golding, J. Feeding symptoms, dietary patterns, and growth in young children with autism spectrum disorders. Pediatrics 2010, 126, e337–e342. [Google Scholar] [CrossRef] [PubMed]
- Martins, Y.; Young, R.L.; Robson, D.C. Feeding and eating behaviors in children with autism and typically developing children. J. Autism Dev. Disord. 2008, 38, 1878–1887. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.; Heiss, C.J.; Campbell, E.E. A comparison of nutrient intake and eating behaviors of boys with and without autism. Top. Clin. Nutr. 2008, 23, 23–31. [Google Scholar] [CrossRef]
- Clark, M.J.; Slavin, J.L. The effect of fiber on satiety and food intake: A systematic review. J. Am. Coll. Nutr. 2013, 32, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Sahan, A.K.; Ozturk, N.; Demir, N.; Karaduman, A.A.; Serel Arslan, S. A Comparative Analysis of Chewing Function and Feeding Behaviors in Children with Autism. Dysphagia 2021. [Google Scholar] [CrossRef]
- Madrigal, C.; Soto-Mendez, M.J.; Hernandez-Ruiz, A.; Valero, T.; Avila, J.M.; Ruiz, E.; Villoslada, F.L.; Leis, R.; Martinez de Victoria, E.; Moreno, J.M.; et al. Energy Intake, Macronutrient Profile and Food Sources of Spanish Children Aged One to <10 Years-Results from the EsNuPI Study. Nutrients 2020, 12, 893. [Google Scholar] [CrossRef] [Green Version]
- Partearroyo, T.; Samaniego-Vaesken, M.L.; Ruiz, E.; Aranceta-Bartrina, J.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Current Food Consumption amongst the Spanish ANIBES Study Population. Nutrients 2019, 11, 2663. [Google Scholar] [CrossRef] [Green Version]
- Plaza-Diaz, J.; Molina-Montes, E.; Soto-Mendez, M.J.; Madrigal, C.; Hernandez-Ruiz, A.; Valero, T.; Lara Villoslada, F.; Leis, R.; Martinez de Victoria, E.; Moreno, J.M.; et al. Clustering of Dietary Patterns and Lifestyles Among Spanish Children in the EsNuPI Study (dagger). Nutrients 2020, 12, 2536. [Google Scholar] [CrossRef]
- Samaniego-Vaesken, M.L.; Partearroyo, T.; Valero, T.; Rodriguez, P.; Soto-Mendez, M.J.; Hernandez-Ruiz, A.; Villoslada, F.L.; Leis, R.; Martinez de Victoria, E.; Moreno, J.M.; et al. Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years-Results from the EsNuPI Study. Nutrients 2020, 12, 3171. [Google Scholar] [CrossRef] [PubMed]
- Sharp, W.G.; Postorino, V.; McCracken, C.E.; Berry, R.C.; Criado, K.K.; Burrell, T.L.; Scahill, L. Dietary intake, nutrient status, and growth parameters in children with autism spectrum disorder and severe food selectivity: An electronic medical record review. J. Acad. Nutr. Diet. 2018, 118, 1943–1950. [Google Scholar] [CrossRef]
- Tachibana, Y.; Miyazaki, C.; Ota, E.; Mori, R.; Hwang, Y.; Kobayashi, E.; Terasaka, A.; Tang, J.; Kamio, Y. A systematic review and meta-analysis of comprehensive interventions for pre-school children with autism spectrum disorder (ASD). PLoS ONE 2017, 12, e0186502. [Google Scholar] [CrossRef] [PubMed]
- Busdiecker, S.; Castillo, C.; Salas, I. Cambios en los hábitos de alimentación durante la infancia: Una visión antropológica. Rev. Chil. Pediatr. 2000, 71, 5–11. [Google Scholar] [CrossRef]
- Babinska, K.; Celusakova, H.; Belica, I.; Szapuova, Z.; Waczulikova, I.; Nemcsicsova, D.; Tomova, A.; Ostatnikova, D. Gastrointestinal Symptoms and Feeding Problems and Their Associations with Dietary Interventions, Food Supplement Use, and Behavioral Characteristics in a Sample of Children and Adolescents with Autism Spectrum Disorders. Int. J. Environ. Res. Public Health 2020, 17, 6372. [Google Scholar] [CrossRef]
- Kohane, I.S.; McMurry, A.; Weber, G.; MacFadden, D.; Rappaport, L.; Kunkel, L.; Bickel, J.; Wattanasin, N.; Spence, S.; Murphy, S. The co-morbidity burden of children and young adults with autism spectrum disorders. PLoS ONE 2012, 7, e33224. [Google Scholar] [CrossRef]
- Esteban-Figuerola, P.; Canals, J.; Fernandez-Cao, J.C.; Arija Val, V. Differences in food consumption and nutritional intake between children with autism spectrum disorders and typically developing children: A meta-analysis. Autism 2019, 23, 1079–1095. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Huerta, O.D.; Gomez-Fernandez, A.; de la Torre-Aguilar, M.J.; Gil, A.; Perez-Navero, J.L.; Flores-Rojas, K.; Martin-Borreguero, P.; Gil-Campos, M. Metabolic profiling in children with autism spectrum disorder with and without mental regression: Preliminary results from a cross-sectional case-control study. Metabolomics 2019, 15, 99. [Google Scholar] [CrossRef]
- Jory, J. Abnormal fatty acids in Canadian children with autism. Nutrition 2016, 32, 474–477. [Google Scholar] [CrossRef]
- Vancassel, S.; Durand, G.; Barthelemy, C.; Lejeune, B.; Martineau, J.; Guilloteau, D.; Andres, C.; Chalon, S. Plasma fatty acid levels in autistic children. Prostaglandins Leukot. Essent. Fat. Acids (PLEFA) 2001, 65, 1–7. [Google Scholar] [CrossRef]
- Amminger, G.P.; Berger, G.E.; Schafer, M.R.; Klier, C.; Friedrich, M.H.; Feucht, M. Omega-3 fatty acids supplementation in children with autism: A double-blind randomized, placebo-controlled pilot study. Biol. Psychiatry 2007, 61, 551–553. [Google Scholar] [CrossRef]
- Bell, J.G.; Sargent, J.R.; Tocher, D.R.; Dick, J.R. Red blood cell fatty acid compositions in a patient with autistic spectrum disorder: A characteristic abnormality in neurodevelopmental disorders? Prostaglandins Leukot. Essent. Fat. Acids (PLEFA) 2000, 63, 21–25. [Google Scholar] [CrossRef]
- Bozzatello, P.; Brignolo, E.; De Grandi, E.; Bellino, S. Supplementation with Omega-3 Fatty Acids in Psychiatric Disorders: A Review of Literature Data. J. Clin. Med. 2016, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- Das, U. Long-chain polyunsaturated fatty acids in the growth and development of the brain and memory. Nutrition 2003, 19, 62. [Google Scholar] [CrossRef]
- Karhu, E.; Zukerman, R.; Eshraghi, R.S.; Mittal, J.; Deth, R.C.; Castejon, A.M.; Trivedi, M.; Mittal, R.; Eshraghi, A.A. Nutritional interventions for autism spectrum disorder. Nutr. Rev. 2020, 78, 515–531. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Nobile, M.; Ciappolino, V.; Delvecchio, G.; Tesei, A.; Turolo, S.; Crippa, A.; Mazzocchi, A.; Altamura, C.A.; Brambilla, P. The role of omega-3 fatty acids in developmental psychopathology: A systematic review on early psychosis, autism, and ADHD. Int. J. Mol. Sci. 2017, 18, 2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.-S.; Tseng, P.-T.; Chen, Y.-W.; Stubbs, B.; Yang, W.-C.; Chen, T.-Y.; Wu, C.-K.; Lin, P.-Y. Supplementation of omega 3 fatty acids may improve hyperactivity, lethargy, and stereotypy in children with autism spectrum disorders: A meta-analysis of randomized controlled trials. Neuropsychiatr. Dis. Treat. 2017, 13, 2531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazahery, H.; Stonehouse, W.; Delshad, M.; Kruger, M.C.; Conlon, C.A.; Beck, K.L.; Von Hurst, P.R. Relationship between long chain n-3 polyunsaturated fatty acids and autism spectrum disorder: Systematic review and meta-analysis of case-control and randomised controlled trials. Nutrients 2017, 9, 155. [Google Scholar] [CrossRef] [Green Version]
- FAO. Grasas y Ácidos Grasos en Nutrición Humana Consulta de Expertos; Organización de las Naciones Unidas para la Alimentación y la Agricultura [FAO] y la Fundación Iberoamericana de Nutrición [FINUT]: Ginebra, Switzerland, 2008; pp. 1–175. [Google Scholar]
- Ministry of Environment and Rural and Marine Affairs (MARM) (2008–2021). La Alimentación en España. Ministerio de Agricultura, Pesca y Alimentación, Madrid, España: Madrid. Available online: https://www.mapa.gob.es/es/estadistica/temas/estadisticas-pesqueras/default.aspx (accessed on 1 September 2021).
- Hyman, S.L.; Stewart, P.A.; Schmidt, B.; Lemcke, N.; Foley, J.T.; Peck, R.; Clemons, T.; Reynolds, A.; Johnson, C.; Handen, B. Nutrient intake from food in children with autism. Pediatrics 2012, 130, S145–S153. [Google Scholar] [CrossRef] [Green Version]
- Malhi, P.; Venkatesh, L.; Bharti, B.; Singhi, P. Feeding problems and nutrient intake in children with and without autism: A comparative study. Indian J. Pediatr. 2017, 84, 283–288. [Google Scholar] [CrossRef]
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatr. 2011, 11, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Amberg, N.; Laukoter, S.; Hippenmeyer, S. Epigenetic cues modulating the generation of cell-type diversity in the cerebral cortex. J. Neurochem. 2019, 149, 12–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, S.J.; Melnyk, S.; Jernigan, S.; Cleves, M.A.; Halsted, C.H.; Wong, D.H.; Cutler, P.; Bock, K.; Boris, M.; Bradstreet, J.J. Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2006, 141, 947–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahams, B.S.; Geschwind, D.H. Connecting genes to brain in the autism spectrum disorders. Arch. Neurol. 2010, 67, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modabbernia, A.; Velthorst, E.; Reichenberg, A. Environmental risk factors for autism: An evidence-based review of systematic reviews and meta-analyses. Mol. Autism 2017, 8, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Archer, E.; Marlow, M.L.; Lavie, C.J. Controversy and debate: Memory-Based Methods Paper 1: The fatal flaws of food frequency questionnaires and other memory-based dietary assessment methods. J. Clin. Epidemiol. 2018, 104, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Golley, R.; Bell, L.; Hendrie, G.A.; Rangan, A.M.; Spence, A.; McNaughton, S.; Carpenter, L.; Allman-Farinelli, M.; de Silva, A.; Gill, T. Validity of short food questionnaire items to measure intake in children and adolescents: A systematic review. J. Hum. Nutr. Diet. 2017, 30, 36–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackerras, D.; Rutishauser, I. 24-Hour national dietary survey data: How do we interpret them most effectively? Public Health Nutr. 2005, 8, 657–665. [Google Scholar] [CrossRef] [Green Version]
- Edefonti, V.; De Vito, R.; Dalmartello, M.; Patel, L.; Salvatori, A.; Ferraroni, M. Reproducibility and validity of a posteriori dietary patterns: A systematic review. Adv. Nutr. 2020, 11, 293–326. [Google Scholar] [CrossRef]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary patterns: Challenges and opportunities in dietary patterns research: An Experimental Biology workshop, April 1, 2006. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef]
- Gomez-Fernandez, A.; de la Torre-Aguilar, M.J.; Gil-Campos, M.; Flores-Rojas, K.; Cruz-Rico, M.D.; Martin-Borreguero, P.; Perez-Navero, J.L. Children With Autism Spectrum Disorder With Regression Exhibit a Different Profile in Plasma Cytokines and Adhesion Molecules Compared to Children Without Such Regression. Front. Pediatr. 2018, 6, 264. [Google Scholar] [CrossRef] [Green Version]
- Plaza-Diaz, J.; Gomez-Fernandez, A.; Chueca, N.; Torre-Aguilar, M.J.; Gil, A.; Perez-Navero, J.L.; Flores-Rojas, K.; Martin-Borreguero, P.; Solis-Urra, P.; Ruiz-Ojeda, F.J.; et al. Autism Spectrum Disorder (ASD) with and without Mental Regression is Associated with Changes in the Fecal Microbiota. Nutrients 2019, 11, 337. [Google Scholar] [CrossRef] [Green Version]
- Martin-Borreguero, P.; Gomez-Fernandez, A.R.; De La Torre-Aguilar, M.J.; Gil-Campos, M.; Flores-Rojas, K.; Perez-Navero, J.L. Children With Autism Spectrum Disorder and Neurodevelopmental Regression Present a Severe Pattern After a Follow-Up at 24 Months. Front. Psychiatry 2021, 12, 644324. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control (n = 57) | ASD (n = 54) | p-Value |
|---|---|---|---|
| Age (months) | 51.5 (33–60) | 42 (33–51) | 0.07 |
| Sex (male) | 43 (75%) | 45 (83.33%) | 0.28 |
| Weight (kg) | 17.3 ± 2.5 | 16.7 ± 3.5 | 0.3 |
| Height (cm) | 106.3 ± 8.3 | 103.4 ± 9.7 | 0.6 |
| BMI (kg/m2) | 16.1 ± 1.7 | 15.9 ± 1.9 | 0.4 |
| Food Groups | Control (n = 57) | ASD (n = 54) |
|---|---|---|
| Cereals and pasta (s/d) | 2.6 ± 1.0 | 4.6 ± 1.5 * |
| Fruits and vegetables (s/d) | 2.0 ± 1.2 | 2.2 ± 0.9 |
| Milk and dairy products (s/d) | 3.2 ± 1.3 | 4.3 ± 1.6 * |
| Fish and shellfish (s/wk) | 2.6 ± 1.1 | 2.5 ± 1.2 |
| Lean meat and eggs (s/wk) | 4.6 ± 1.4 | 2.0 ± 0.5 * |
| Fatty meats and derivatives (s/wk) | 3.6 ± 2.3 | 2.8 ± 1.5 |
| Fats (s/d) | 2.8 ± 1.8 | 2.3 ± 0.6 |
| Beverages (s/wk) | 6.2 ± 3.1 | 4.1 ± 1.0 * |
| Snacks, sweets, bakery and pastry (s/wk) | 5.5 ± 3.2 | 4.6 ± 2.8 |
| Food Groups (SENC Guidelines) | Control (n = 57) | ASD (n = 54) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Cereals and pasta (4–6 s/d) | <4 | 4–6 | >6 | <4 | 4–6 | >6 | <0.001 |
| 82.5 | 17.5 | 0 | 25.9 | 63 | 11.1 | ||
| Fruits and vegetables (≥5 s/d) | <3 | >3 | <3 | >3 | 0.098 | ||
| 87.7 | 12.3 | 96.3 | 3.7 | ||||
| Milk and dairy products (2–4 s/d) | <2 | 2–4 | >4 | <2 | 2–4 | >4 | 0.041 |
| 10.5 | 71.9 | 17.5 | 3.7 | 59.3 | 37 | ||
| Fish and shellfish (3–4 s/wk) | >3 | 3–4 | >4 | >3 | 3–4 | >4 | 0.22 |
| 49.1 | 45.6 | 5.3 | 63 | 29.6 | 7.4 | ||
| Lean meat and eggs (3–5 s/wk) | <3 | 3–5 | >5 | <3 | 3–5 | >5 | <0.001 |
| 7.0 | 61.4 | 31.6 | 94.4 | 5.6 | 0 | ||
| Fatty meats and derivatives (≤1 s/wk) | 0 | 1 | >2 | 0 | 1 | >2 | 0.637 |
| 1.8 | 10.5 | 87.7 | 1.9 | 16.7 | 81.5 | ||
| Fats (2–3 s/d) * | <2 | 2–3 | >3 | <2 | 2–3 | >3 | <0.001 |
| 15.8 | 61.4 | 22.8 | 3.7 | 94.4 | 1.9 | ||
| Beverages (≤1 s/wk) | 0 | 1 | >2 | 0 | 1 | >2 | 0.328 |
| 0 | 1.8 | 98.2 | 0 | 0 | 100 | ||
| Snacks, sweets, bakery and pastry (≤1 s/wk) | 0 | 1 | >2 | 0 | 1 | >2 | 0.511 |
| 7 | 3.5 | 89.5 | 3.7 | 7.4 | 88.9 | ||
| Variables | Control Group (n = 57) | Children ASD (n = 47) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Percentage below AI or RI | Percentage within RI | Percentage over AI or RI | Percentage below AI or RI | Percentage within RI | Percentage over AI or RI | ||
| Energy | 22.8 | 77.2 | 2.1 | 97.9 | 0.002 | ||
| Proteins | 0 | 100 | 0 | 100 | 1 | ||
| Carbohydrates | 14.3 | 76.8 | 8.9 | 21.3 | 76.6 | 2.1 | 0.254 |
| Sugars | 15.8 | 84.2 | 6.4 | 93.6 | 0.135 | ||
| Fiber | 50.9 | 49.1 | 34.0 | 66.6 | 0.085 | ||
| Fats | 50.9 | 28.1 | 21.1 | 23.4 | 38.3 | 38.3 | 0.014 |
| Polyunsaturated fats | 68.4 | 31.6 | 72.3 | 27.7 | 0.664 | ||
| Saturated fats | 47.4 | 52.6 | 23.4 | 76.6 | 0.012 | ||
| Potassium | 31.6 | 68.4 | 34.0 | 66.6 | 0.79 | ||
| Calcium | 49.1 | 50.1 | 21.3 | 78.7 | 0.003 | ||
| Phosphorus | 14.0 | 86 | 19.1 | 80.9 | 0.483 | ||
| Magnesium | 98.2 | 1.8 | 100 | 0 | 0.362 | ||
| Iron | 80.7 | 19.3 | 97.9 | 2.1 | 0.006 | ||
| Zinc | 70.2 | 29.8 | 80.9 | 19.1 | 0.211 | ||
| Copper | 96.5 | 3.5 | 100 | 0 | 0.195 | ||
| Selenium | 15.8 | 84.2 | 29.8 | 70.2 | 0.087 | ||
| Manganese | 100 | 0 | 100 | 0 | 1 | ||
| Iodine | 63.2 | 36.8 | 100 | 0 | <0.001 | ||
| Vitamin A | 61.4 | 38.6 | 57.4 | 42.6 | 0.682 | ||
| Vitamin D | 91.2 | 8.8 | 95.7 | 4.3 | 0.36 | ||
| Vitamin E | 94.7 | 5.3 | 85.1 | 14.9 | 0.097 | ||
| Vitamin K | 57.9 | 42.1 | 44.7 | 55.3 | 0.179 | ||
| Vitamin B1 | 56.1 | 43.9 | 91.5 | 8.5 | <0.001 | ||
| Vitamin B2 | 24.6 | 75.4 | 68.1 | 31.9 | <0.001 | ||
| Vitamin B3 | 96.5 | 3.5 | 100 | 0 | 0.195 | ||
| Vitamin B6 | 33.3 | 66.7 | 53.2 | 46.8 | 0.041 | ||
| Vitamin B9 | 91.2 | 8.8 | 91.5 | 8.5 | 0.962 | ||
| Vitamin B12 | 24.6 | 75.4 | 48.9 | 51.1 | 0.01 | ||
| Vitamin C | 42.1 | 57.9 | 21.3 | 78.7 | 0.024 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plaza-Diaz, J.; Flores-Rojas, K.; Torre-Aguilar, M.J.d.l.; Gomez-Fernández, A.R.; Martín-Borreguero, P.; Perez-Navero, J.L.; Gil, A.; Gil-Campos, M. Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders. Nutrients 2021, 13, 3551. https://doi.org/10.3390/nu13103551
Plaza-Diaz J, Flores-Rojas K, Torre-Aguilar MJdl, Gomez-Fernández AR, Martín-Borreguero P, Perez-Navero JL, Gil A, Gil-Campos M. Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders. Nutrients. 2021; 13(10):3551. https://doi.org/10.3390/nu13103551
Chicago/Turabian StylePlaza-Diaz, Julio, Katherine Flores-Rojas, María José de la Torre-Aguilar, Antonio Rafael Gomez-Fernández, Pilar Martín-Borreguero, Juan Luis Perez-Navero, Angel Gil, and Mercedes Gil-Campos. 2021. "Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders" Nutrients 13, no. 10: 3551. https://doi.org/10.3390/nu13103551
APA StylePlaza-Diaz, J., Flores-Rojas, K., Torre-Aguilar, M. J. d. l., Gomez-Fernández, A. R., Martín-Borreguero, P., Perez-Navero, J. L., Gil, A., & Gil-Campos, M. (2021). Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders. Nutrients, 13(10), 3551. https://doi.org/10.3390/nu13103551