
The Effects of Sodium Phosphate Supplementation on the Cardiorespiratory System and Gross Efficiency during Exercise under Hypoxia in Male Cyclists: A Randomized, Placebo-Controlled, Cross-Over Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
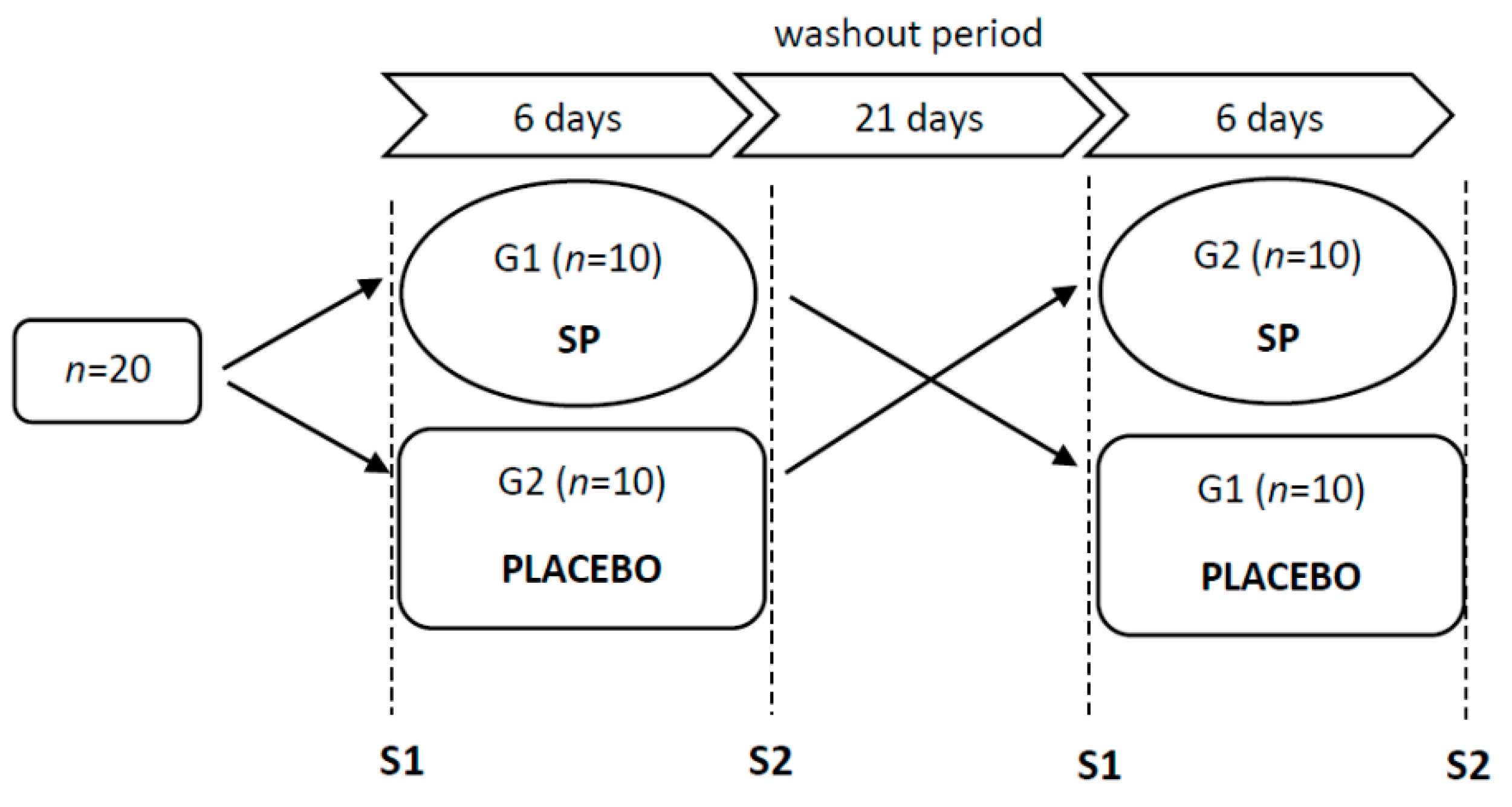
2.2. Study Design
2.3. Incremental Exercise Test
2.4. Supplementation with Sodium Phosphate
2.5. Determination of Gross Efficiency
2.6. Statistical Analysis
3. Results
3.1. Exercise Intensity
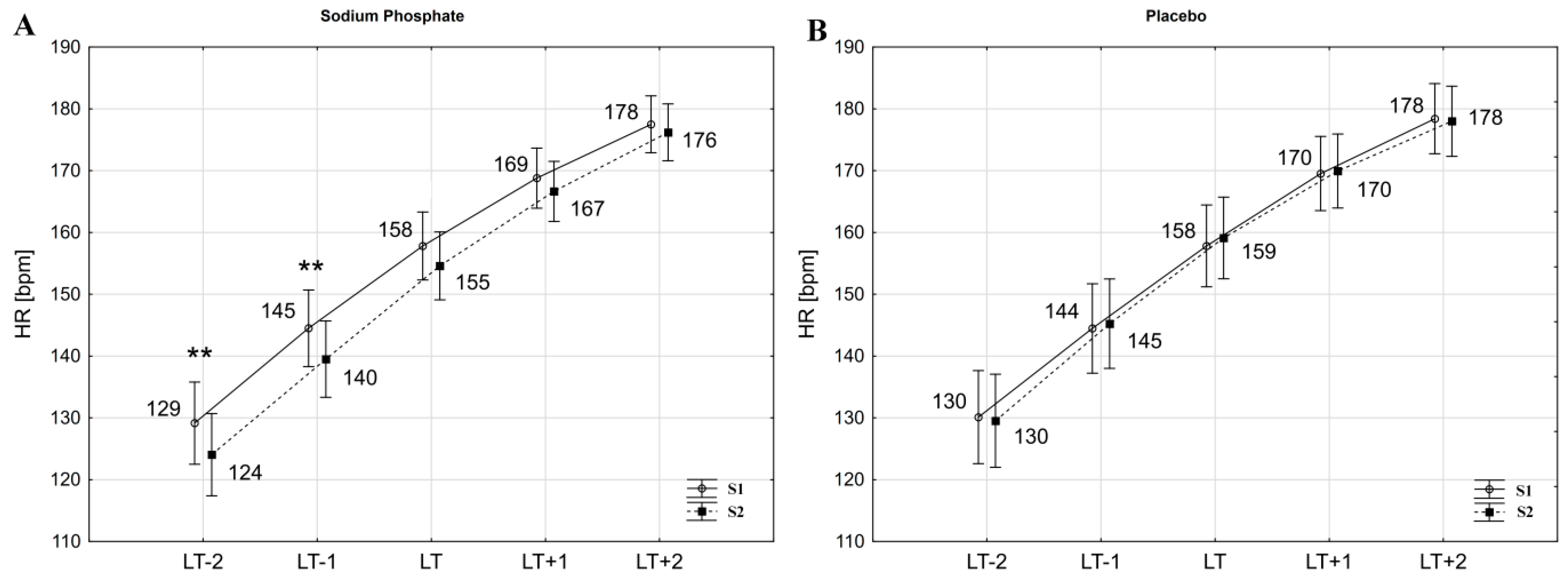
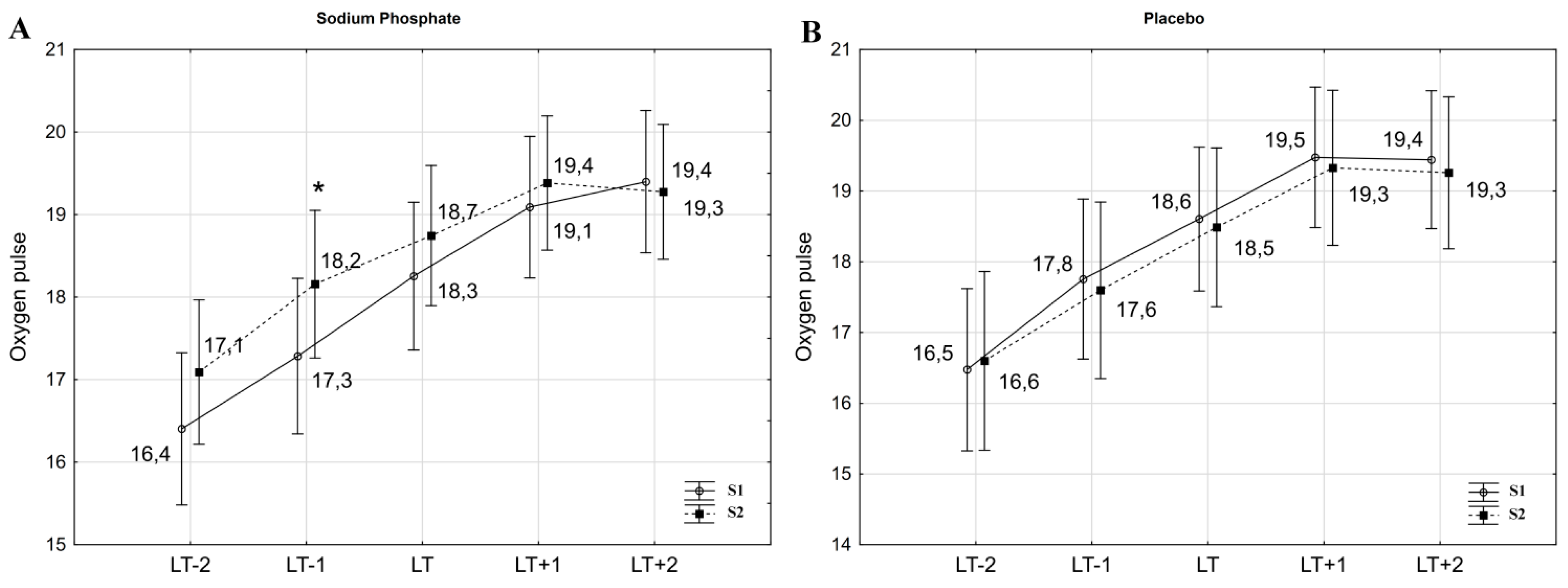
3.2. Cardiorespiratory Variables
3.3. Gross Efficiency
3.4. Serum Phosphate and Calcium Concentrations
3.5. Hematocrit and Plasma Volume
4. Discussion
5. Practical Applications
6. Study Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buck, C.L.; Wallman, K.E.; Dawson, B.; Guelfi, K.J. Sodium phosphate as an ergogenic aid. Sports Med. 2013, 43, 425–435. [Google Scholar] [CrossRef]
- The AIS Sports Supplement Framework. Available online: https://www.ais.gov.au/nutrition/supplements (accessed on 29 May 2021).
- Cade, R.; Conte, M.; Zauner, C.; Mars, D.; Peterson, J.; Lunne, D.; Hommen, N.; Packer, D. Effects of phosphate loading on 2,3-diphosphoglycerate and maximal oxygen uptake. Med. Sci. Sports Exerc. 1984, 16, 263–268. [Google Scholar] [CrossRef]
- Kreider, R.; Miller, G.W.; Williams, M.H.; Somma, C.T.; A Nasser, T. Effects of phosphate loading on oxygen uptake, ventilatory anaerobic threshold, and run performance. Med. Sci. Sports Exerc. 1990, 22, 250–256. [Google Scholar]
- Stewart, I.; McNaughton, L.; Davies, P.; Tristram, S. Phosphate loading and the effects on VO2max in trained cyclists. Res. Q. Exerc. Sport 1990, 61, 80–84. [Google Scholar] [CrossRef]
- Czuba, M.; Zajac, A.; Poprzęcki, S.; Cholewa, J. The influence of sodium phosphate supplementation on VO2max, Serum 2,3-diphosphoglycerate level and heart rate in off-road cyclists. J. Hum. Kinet. 2008, 19, 149–164. [Google Scholar] [CrossRef]
- Czuba, M.; Zajac, A.; Poprzęcki, S.; Cholewa, J.; Woska, S. Effects of sodium phosphate loading on aerobic power and capacity in off road cyclists. J. Sports Sci. Med. 2009, 8, 591–599. [Google Scholar]
- Brewer, C.P.; Dawson, B.; Wallman, K.E.; Guelfi, K.J. Effect of repeated sodium phosphate loading on cycling time-trial performance and VO2peak. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 187–194. [Google Scholar] [CrossRef]
- Kreider, R.; Miller, G.W.; Schenck, D.; Cortes, C.W.; Miriel, V.; Somma, C.T.; Rowland, P.; Turner, C.; Hill, D. Effects of phosphate loading on metabolic and myocardial responses to maximal and endurance exercise. Int. J. Sport Nutr. 1992, 2, 20–47. [Google Scholar] [CrossRef]
- Folland, J.P.; Stern, R.; Brickley, G. Sodium phosphate loading improves laboratory cycling time-trial performance in trained cyclists. J. Sci. Med. Sport 2008, 11, 464–468. [Google Scholar] [CrossRef]
- Brewer, C.P.; Dawson, B.; Wallman, K.E.; Guelfi, K.J. Effect of sodium phosphate supplementation on repeated high-intensity cycling efforts. J. Sports Sci. 2014, 33, 1109–1116. [Google Scholar] [CrossRef]
- Buck, C.L.; Henry, T.; Guelfi, K.; Dawson, B.; Mc Naughton, L.R.; Wallman, K. Effects of sodium phosphate and beetroot juice supplementation on repeated-sprint ability in females. Eur. J. Appl. Physiol. 2015, 115, 2205–2213. [Google Scholar] [CrossRef]
- Buck, C.; Guelfi, K.; Dawson, B.; McNaughton, L.; Wallman, K. Effects of sodium phosphate and caffeine loading on repeated-sprint ability. J. Sports Sci. 2015, 33, 1971–1979. [Google Scholar] [CrossRef]
- Kopec, B.J.; Dawson, B.T.; Buck, C.; Wallman, K.E. Effects of sodium phosphate and caffeine ingestion on repeated-sprint ability in male athletes. J. Sci. Med. Sport 2016, 19, 272–276. [Google Scholar] [CrossRef]
- King, J.; Lowery, D.R. Physiology, Cardiac Output; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Farber, O.M.; Sullivan, T.Y.; Fineberg, N.; Carlone, S.; Manfredi, F. Effect of decreased O2 affinity of hemoglobin on work performance during exercise in healthy humans. J. Lab. Clin. Med. 1984, 104, 166–175. [Google Scholar]
- Lunne, D.; Zauner, C.; Cade, R.; Wright, T.; Conte, M. Effect of phosphate loading on RBC 2–3 DPG, cardiac-output, and oxygen utilization at rest and during vigorous exercise. Clin. Res. 1990, 28, 810. [Google Scholar]
- Siebenmann, C.; Lundby, C. Regulation of cardiac output in hypoxia. Scand. J. Med. Sci. Sports 2015, 25, 53–59. [Google Scholar] [CrossRef] [Green Version]
- West, J.B.; Schoene, R.B.; Luks, A.M.; Milledge, J.S. High Altitude Medicine and Physiology, 5th ed.; CRC Press Taylor & Francis: Boca Raton, FL, USA, 2013; pp. 101–120. [Google Scholar]
- Mazzeo, R.S. Physiological responses to exercise at altitude: An update. Sports Med. 2008, 38, 1–8. [Google Scholar] [CrossRef]
- Mourot, L. Limitation of maximal heart rate in hypoxia: Mechanisms and clinical importance. Front. Physiol. 2018, 9, 972. [Google Scholar] [CrossRef] [Green Version]
- Mallet, R.T.; Burtscher, J.; Richalet, J.-P.; Millet, G.P.; Burtscher, M. Impact of high altitude on cardiovascular health: Current perspectives. Vasc. Health Risk Manag. 2021, 17, 317–335. [Google Scholar] [CrossRef]
- Clark, S.A.; Bourdon, P.C.; Schmidt, W.; Singh, B.; Cable, G.; Onus, K.J.; Woolford, S.M.; Stanef, T.; Gore, C.J.; Aughey, R. The effect of acute simulated moderate altitude on power, performance and pacing strategies in well-trained cyclists. Eur. J. Appl. Physiol. 2007, 102, 45–55. [Google Scholar] [CrossRef]
- Płoszczyca, K.; Czuba, M.; Chalimoniuk, M.; Gajda, R.; Baranowski, M. Red blood cell 2,3-diphosphoglycerate decreases in response to a 30 km time trial under hypoxia in cyclists. Front. Physiol. 2021, 12, 670977. [Google Scholar] [CrossRef]
- Weavil, J.C.; Duke, J.W.; Stickford, J.L.; Stager, J.M.; Chapman, R.F.; Mickleborough, T.D. Endurance exercise performance in acute hypoxia is influenced by expiratory flow limitation. Eur. J. Appl. Physiol. 2015, 115, 1653–1663. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Haykowsky, M.J.; Quinney, H.A.; Blackmore, D.; Teo, K.K.; Humen, D.P. Myocardial response to incremental exercise in endurance-trained athletes: Influence of Heart rate, contractility and the frank-starling effect. Exp. Physiol. 2002, 87, 613–622. [Google Scholar] [CrossRef]
- Vella, C.A.; Robergs, R.A. A review of the stroke volume response to upright exercise in healthy subjects. Br. J. Sports Med. 2005, 39, 190–195. [Google Scholar] [CrossRef]
- Joyner, M.J.; Coyle, E.F. Endurance exercise performance: The physiology of champions. J. Physiol. 2008, 586, 35–44. [Google Scholar] [CrossRef]
- Płoszczyca, K.; Foltyn, J.; Goliniewski, J.; Krȩżelok, J.; Poprzȩcki, S.; Ozimek, M.; Czuba, M. Seasonal changes in gross efficiency and aerobic capacity in well-trained road cyclists. Isokinet. Exerc. Sci. 2019, 27, 193–202. [Google Scholar] [CrossRef]
- Faria, E.W.; Parker, D.L.; Faria, I.E. The science of cycling: Factors affecting performance-Part 2. Sports Med. 2005, 35, 313–337. [Google Scholar] [CrossRef]
- Layec, G.; Haseler, L.J.; Hoff, J.; Richardson, R.S. Evidence that a higher ATP cost of muscular contraction contributes to the lower mechanical efficiency associated with COPD: Preliminary findings. Am. J. Physiol. Integr. Comp. Physiol. 2011, 300, R1142–R1147. [Google Scholar] [CrossRef] [Green Version]
- Jabbour, G.; Iancu, H.-D. Mechanical efficiency improvement in relation to metabolic changes in sedentary obese adults. BMJ Open Sport Exerc. Med. 2015, 1, e000044. [Google Scholar] [CrossRef] [Green Version]
- Schuler, B.; Thomsen, J.J.; Gassmann, M.; Lundby, C. Timing the arrival at 2340 m altitude for aerobic performance. Scand. J. Med. Sci. Sports 2007, 17, 588–594. [Google Scholar] [CrossRef]
- Van Erck, D.; Wenker, E.J.; Levels, K.; Foster, C.; De Koning, J.J.; Noordhof, D.A. Cycling at altitude: Lower absolute power output as the main cause of lower gross efficiency. Int. J. Sports Physiol. Perform. 2019, 14, 1117–1123. [Google Scholar] [CrossRef]
- Noordhof, D.A.; Schoots, T.; Hoekert, D.H.; De Koning, J.J. Is gross efficiency lower at acute simulated altitude than at sea level? Int. J. Sports Physiol. Perform. 2013, 8, 319–322. [Google Scholar] [CrossRef]
- Lardy, H.A.; Wellman, H. Oxidative phosphorylations: Rôle of inorganic phosphate and acceptor systems in control of metabolic rates. J. Biol. Chem. 1952, 195, 215–224. [Google Scholar] [CrossRef]
- Pesta, D.H.; Tsirigotis, D.N.; Befroy, D.E.; Caballero, D.; Jurczak, M.J.; Rahimi, Y.; Cline, G.W.; Dufour, S.; Birkenfeld, A.L.; Rothman, D.L.; et al. Hypophosphatemia promotes lower rates of muscle ATP synthesis. FASEB J. 2016, 30, 3378–3387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcos, M.; Olcina, G.; Timón, R.; Sánchez, F.; Maynar, M. Efecto ergogénico de la ingesta de fosfato sódico en sujetos físicamente activos/Ergogenic effect of sodium phosphate intake in physically active subjects. Rev. Int. Med. Cienc. Act. Física Deporte 2016, 16, 33–44. [Google Scholar] [CrossRef] [Green Version]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 4.0) [Computer Software]. Available online: http://www.randomizer.org/ (accessed on 14 September 2020).
- Nadler, S.B.; Hidalgo, J.H.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar]
- Cheng, B.; Kuipers, H.; Snyder, A.C.; Keizer, H.A.; Jeukendrup, A.; Hesselink, M. A New Approach for the determination of ventilatory and lactate thresholds. Int. J. Sports Med. 1992, 13, 518–522. [Google Scholar] [CrossRef]
- Czuba, M.; Zajac, A.; Cholewa, J.; Poprzęcki, S.; Waśkiewicz, Z.; Mikołajec, K. Lactate threshold (D-Max Method) and maximal lactate steady state in cyclists. J. Hum. Kinet. 2009, 21, 49. [Google Scholar] [CrossRef] [Green Version]
- Płoszczyca, K.; Jazic, D.; Piotrowicz, Z.; Chalimoniuk, M.; Langfort, J.; Czuba, M. Comparison of maximal lactate steady state with anaerobic threshold determined by various methods based on graded exercise test with 3-minute stages in elite cyclists. BMC Sports Sci. Med. Rehabil. 2020, 12, 70. [Google Scholar] [CrossRef]
- West, J.S.; Ayton, T.; Wallman, K.E.; Guelfi, K. The effect of 6 days of sodium phosphate supplementation on appetite, energy intake, and aerobic capacity in trained men and women. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 422–429. [Google Scholar] [CrossRef] [Green Version]
- Brewer, C.P.; Dawson, B.; Wallman, K.E.; Guelfi, K. Effect of Sodium phosphate supplementation on cycling time trial performance and VO2 1 and 8 days post loading. J. Sports Sci. Med. 2014, 13, 529–534. [Google Scholar] [PubMed]
- Buck, C.L.; Dawson, B.; Guelfi, K.; McNaughton, L.; Wallman, K.E. Sodium phosphate supplementation and time trial performance in female cyclists. J. Sports Sci. Med. 2014, 13, 469–475. [Google Scholar] [PubMed]
- Tremblay, M.S.; Galloway, S.D.; Sexsmith, J.R. Ergogenic effects of phosphate loading: Physiological fact or methodological fiction? Can. J. Appl. Physiol. 1994, 19, 1–11. [Google Scholar] [CrossRef]
- Galloway, S.D.R.; Tremblay, M.S.; Sexsmith, J.R.; Roberts, C.J. The effects of acute phosphate supplementation in subjects of different aerobic fitness levels. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 72, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Lusk, G. Animal calorimetry twenty-fourth paper. Analysis of the oxidation of 423 mixtures of carbohydrate and fat. J. Biol. Chem. 1924, 59, 41–42. [Google Scholar] [CrossRef]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urhausen, A.; Weiler, B.; Coen, B.; Kindermann, W. Plasma catecholamines during endurance exercise of different intensities as related to the individual anaerobic threshold. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 69, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Chmura, J.; Nazar, K.; Kaciuba-Uścilko, H. Choice Reaction time during graded exercise in relation to blood lactate and plasma catecholamine thresholds. Int. J. Sports Med. 1994, 15, 172–176. [Google Scholar] [CrossRef]
- Gordan, R.; Gwathmey, J.K.; Xie, L.-H. Autonomic and endocrine control of cardiovascular function. World J. Cardiol. 2015, 7, 204–214. [Google Scholar] [CrossRef]
- Macdonald, E.A.; Rose, R.A.; Quinn, T.A. Neurohumoral control of sinoatrial node activity and heart rate: Insight from experimental models and findings from humans. Front. Physiol. 2020, 11, 170. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, L.R.; Wheeler, W.S.; Bethune, J.E. Effect of hypophosphatemia on myocardial performance in man. N. Engl. J. Med. 1977, 297, 901–903. [Google Scholar] [CrossRef] [PubMed]
- Stoff, J.S. Phosphate homeostasis and hypophosphatemia. Am. J. Med. 1982, 72, 489–495. [Google Scholar] [CrossRef]
- Rubin, M.F.; Narins, R.G. Hypophosphatemia: Pathophysiological and practical aspects of its therapy. Semin. Nephrol. 1990, 10, 536–545. [Google Scholar]
- Brautbar, N.; Altura, B.M. Hypophosphatemia and hypomagnesemia result in cardiovascular dysfunction: Theoretical basis for alcohol-induced cellular injury. Alcohol. Clin. Exp. Res. 1987, 11, 118–126. [Google Scholar] [CrossRef]
- Davis, S.V.; Olichwier, K.K.; Chakko, S.C. Reversible depression of myocardial performance in hypophosphatemia. Am. J. Med Sci. 1988, 295, 183–187. [Google Scholar] [CrossRef]
- Bredle, D.L.; Stager, J.M.; Brechue, W.F.; Farber, M.O. Phosphate supplementation, cardiovascular function, and exercise performance in humans. J. Appl. Physiol. 1988, 65, 1821–1826. [Google Scholar] [CrossRef]
- Mannix, E.T.; Stager, J.M.; Harris, A.; O Farber, M. Oxygen delivery and cardiac output during exercise following oral phosphate-glucose. Med. Sci. Sports Exerc. 1990, 22, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Schierbauer, J.; Hoffmeister, T.; Treff, G.; Wachsmuth, N.B.; Schmidt, W.F.J. Effect of exercise-induced reductions in blood volume on cardiac output and oxygen transport capacity. Front. Physiol. 2021, 12, 679232. [Google Scholar] [CrossRef]
- Sawka, M.N.; Coyle, E.F. Influence of body water and blood volume on thermoregulation and exercise performance in the heat. Exerc. Sport Sci. Rev. 1999, 27, 167–218. [Google Scholar] [PubMed]
- Hamouti, N.; Fernández-Elías, V.E.; Ortega, J.F.; Mora-Rodriguez, R. Ingestion of sodium plus water improves cardiovascular function and performance during dehydrating cycling in the heat. Scand. J. Med. Sci. Sports 2012, 24, 507–518. [Google Scholar] [CrossRef]
- Clarkson, P.M.; Haymes, E.M. Exercise and mineral status of athletes: Calcium, magnesium, phosphorus, and iron. Med. Sci. Sports Exerc. 1995, 27, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Bers, D.M. Calcium fluxes involved in control of cardiac myocyte contraction. Circ. Res. 2000, 87, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Baird, G.S. Ionized calcium. Clin. Chim. Acta 2011, 412, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.; Williams, G.R. Hypocalcaemia. Medicine 2009, 37, 465–468. [Google Scholar] [CrossRef]
- Brown, J.A.; Glaister, M. The Effects of sodium phosphate supplementation on physiological responses to submaximal exercise and 20 km cycling time-trial performance. J. Diet. Suppl. 2019, 16, 564–575. [Google Scholar] [CrossRef] [Green Version]
- Cerretelli, P.; Gelfi, C. Energy metabolism in hypoxia: Reinterpreting some features of muscle physiology on molecular grounds. Eur. J. Appl. Physiol. 2010, 111, 421–432. [Google Scholar] [CrossRef]
- Laursen, P.B.; Rhodes, E.C. Factors affecting performance in an ultraendurance triathlon. Sports Med. 2001, 31, 195–209. [Google Scholar] [CrossRef]
- Laursen, P.B.; Rhodes, E.C.; Langill, R.H.; McKenzie, D.C.; Taunton, J.E. Relationship of exercise test variables to cycling performance in an Ironman triathlon. Eur. J. Appl. Physiol. 2002, 87, 433–440. [Google Scholar] [CrossRef]
- Davies, C.T.; Thompson, M.W. Physiological responses to prolonged exercise in ultramarathon athletes. J. Appl. Physiol. 1986, 61, 611–617. [Google Scholar] [CrossRef]
- Barrero, A.; Chaverri, D.; Erola, P.; Iglesias, X.; Rodríguez, F.A. Intensity profile during an ultra-endurance triathlon in relation to testing and performance. Int. J. Sports Med. 2014, 35, 1170–1178. [Google Scholar] [CrossRef]
- Fornasiero, A.; Savoldelli, A.; Fruet, D.; Boccia, G.; Pellegrini, B.; Schena, F. Physiological intensity profile, exercise load and performance predictors of a 65-km mountain ultra-marathon. J. Sports Sci. 2017, 36, 1287–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumayr, G.; Pfister, R.; Mitterbauer, G.; Gaenzer, H.; Sturm, W.; Hoertnagl, H. Heart rate response to ultraendurance cycling. Br. J. Sports Med. 2003, 37, 89–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattsson, C.M.; Ståhlberg, M.; Larsen, F.J.; Braunschweig, F.; Ekblom, B. Late Cardiovascular drift observable during ultraendurance exercise. Med. Sci. Sports Exerc. 2011, 43, 1162–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, R.A.; Smith, B.E.; Madigan, V.M. Stroke volume monitoring: Novel continuous wave doppler parameters, algorithms and advanced noninvasive haemodynamic concepts. Curr. Anesthesiol. Rep. 2017, 7, 387–398. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Workload | Variable | Sodium Phosphate | Placebo | ||
|---|---|---|---|---|---|
| S1 | S2 | S1 | S2 | ||
| LT−2 | % of actual VO2max | 61.5 ± 1.3 | 59.9 ± 1.2 | 62.0 ± 1.3 | 62.7 ± 1.3 |
| LT−1 | % of actual VO2max | 72.7 ± 1.1 | 72.0 ± 1.2 | 74.1 ± 1.2 | 74.7 ± 1.3 |
| LT | % of actual VO2max | 83.9 ± 0.9 | 82.3 ± 1.0 | 84.5 ± 0.9 | 85.6 ± 1.1 |
| LT+1 | % of actual VO2max | 93.7 ± 0.7 | 92.0 ± 0.9 | 94.4 ± 0.8 | 94.9 ± 1.0 |
| LT+2 | % of actual VO2max | 99.3 ± 0.5 | 96.6 * ± 0.8 | 97.3 ± 0.6 | 98.6 ± 1.0 |
| Workload | Variables | Sodium Phosphate | Placebo | ||
|---|---|---|---|---|---|
| S1 | S2 | S1 | S2 | ||
| LT−2 | SV (mL) | 123.6 ± 2.9 | 128.2 ± 3.6 | 120.8 ± 3.0 | 121.2 ± 3.7 |
| Q (L∙min−1) | 15.95 ± 0.27 | 15.85 ± 0.32 | 16.15 ± 0.28 | 15.88 ± 0.38 | |
| VO2 (L∙min−1) | 2.12 ± 0.06 | 2.10 ± 0.06 | 2.17 ± 0.06 | 2.18 ± 0.06 | |
| LT−1 | SV (mL) | 117.9 ± 2.7 | 122.7 ** ± 3.1 | 117.4 ± 2.8 | 116.9 ± 3.2 |
| Q (L∙min−1) | 17.10 ± 0.27 | 17.08 ± 0.32 | 17.36 ± 0.28 | 17.17 ± 0.32 | |
| VO2 (L∙min−1) | 2.51 ± 0.06 | 2.53 ± 0.07 | 2.59 ± 0.06 | 2.59 ± 0.07 | |
| LT | SV (mL) | 113.8 ± 2.6 | 116.6 * ± 2.5 | 113.6 ± 2.6 | 113.3 ± 2.6 |
| Q (L∙min−1) | 18.05 ± 0.27 | 17.97 ± 0.28 | 18.22 ± 0.28 | 18.19 ± 0.29 | |
| VO2 (L∙min−1) | 2.90 ± 0.06 | 2.89 ± 0.06 | 2.95 ± 0.06 | 2.97 ± 0.06 | |
| LT+1 | SV (mL) | 110.8 ± 2.4 | 112.3 ± 2.3 | 110.2 ± 2.5 | 110.6 ± 2.4 |
| Q (L∙min−1) | 18.75 ± 0.29 | 18.69 ± 0.28 | 18.94 ± 0.30 | 18.93 ± 0.29 | |
| VO2 (L∙min−1) | 3.23 ± 0.06 | 3.22 ± 0.06 | 3.32 ± 0.07 | 3.30 ± 0.06 | |
| LT+2 | SV (mL) | 107.6 ± 3.0 | 109.2 ± 3.2 | 109.4 ± 3.5 | 109.4 ± 3.7 |
| Q (L∙min−1) | 19.17 ± 0.40 | 19.10 ± 0.44 | 19.50 ± 0.47 | 19.48 ± 0.51 | |
| VO2 (L∙min−1) | 3.44 ± 0.06 | 3.38 ± 0.06 | 3.46 ± 0.07 | 3.43 ± 0.07 | |
| Workload | Variables | Sodium Phosphate | Placebo | ||
|---|---|---|---|---|---|
| S1 | S2 | S1 | S2 | ||
| LT−2 | GE (%) | 18.73 ± 0.47 | 18.96 ± 0.45 | 19.06 ± 0.50 | 19.00 ± 0.48 |
| RER | 0.94 ± 0.01 | 0.93 ± 0.01 | 0.94 ± 0.01 | 0.93 ± 0.01 | |
| LT−1 | GE (%) | 20.20 ± 0.43 | 20.05 ± 0.41 | 20.54 ± 0.45 | 20.39 ± 0.43 |
| RER | 0.97 ± 0.01 | 0.97 ± 0.01 | 0.98 ± 0.01 | 0.97 ± 0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Płoszczyca, K.; Gajda, R.; Czuba, M. The Effects of Sodium Phosphate Supplementation on the Cardiorespiratory System and Gross Efficiency during Exercise under Hypoxia in Male Cyclists: A Randomized, Placebo-Controlled, Cross-Over Study. Nutrients 2021, 13, 3556. https://doi.org/10.3390/nu13103556
Płoszczyca K, Gajda R, Czuba M. The Effects of Sodium Phosphate Supplementation on the Cardiorespiratory System and Gross Efficiency during Exercise under Hypoxia in Male Cyclists: A Randomized, Placebo-Controlled, Cross-Over Study. Nutrients. 2021; 13(10):3556. https://doi.org/10.3390/nu13103556
Chicago/Turabian StylePłoszczyca, Kamila, Robert Gajda, and Miłosz Czuba. 2021. "The Effects of Sodium Phosphate Supplementation on the Cardiorespiratory System and Gross Efficiency during Exercise under Hypoxia in Male Cyclists: A Randomized, Placebo-Controlled, Cross-Over Study" Nutrients 13, no. 10: 3556. https://doi.org/10.3390/nu13103556
APA StylePłoszczyca, K., Gajda, R., & Czuba, M. (2021). The Effects of Sodium Phosphate Supplementation on the Cardiorespiratory System and Gross Efficiency during Exercise under Hypoxia in Male Cyclists: A Randomized, Placebo-Controlled, Cross-Over Study. Nutrients, 13(10), 3556. https://doi.org/10.3390/nu13103556