
Hospital Food Service Strategies to Improve Food Intakes among Inpatients: A Systematic Review


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Management
2.4. Quality Assessment
2.5. Data Analysis and Synthesis
3. Results
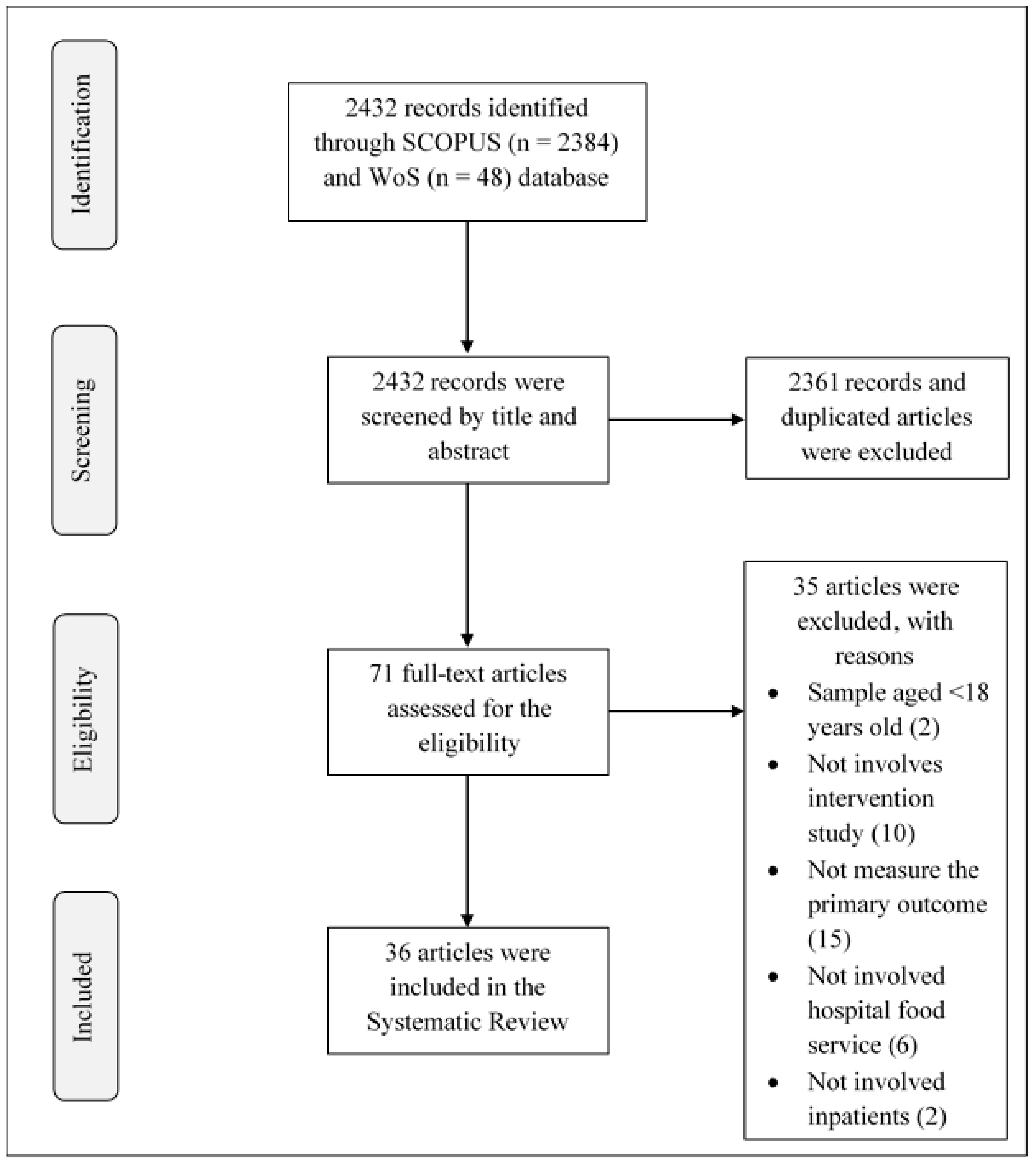
3.1. Study Selection and Characteristics
3.2. Foodservice Intervention Strategies on Food Intake
3.2.1. Foodservice System Intervention
3.2.2. Menu Modification and Meal Composition Intervention
3.2.3. Multidisciplinary Approaches Intervention
3.2.4. Protected Mealtime, Mealtime Assistance, and Environment Intervention
3.2.5. Meal Presentation Intervention
3.3. Outcome Measures
3.3.1. Food Intake
3.3.2. Patient Satisfaction
3.3.3. Nutritional Status
3.4. Quality Rating Studies
4. Discussion
5. Limitations of Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saunders, J.; Smith, T.; Stroud, M. Malnutrition and undernutrition. Medicine 2018, 47, 152–158. [Google Scholar] [CrossRef]
- Agarwal, E.; Ferguson, M.; Banks, M.; Batterham, M.; Bauer, J.; Capra, S.; Isenring, E. Malnutrition and poor food intake are associated with prolonged hospital stay, frequent readmissions, and greater in-hospital mortality: Results from the Nutrition Care Day Survey 2010. Clin. Nutr. 2013, 32, 735–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Ancum, J.M.; Scheerman, K.; Jonkman, N.H.; Kruizinga, R.C.; Meskers, C.G.; Maier, A.B. Change in muscle strength and muscle mass in older hospitalized patients: A systematic review and meta-analysis. Exp. Gerontol. 2017, 92, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Allard, J.P.; Keller, H.; Teterina, A.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R.; Gramlich, L.; Payette, H.; Bernier, P.; Davidson, B.; et al. Factors associated with nutritional decline in hospitalised medical and surgical patients admitted for 7 d or more: A prospective cohort study. Br. J. Nutr. 2015, 114, 1612–1622. [Google Scholar] [CrossRef] [Green Version]
- Kontogianni, M.D.; Anna, K.; Bersimis, F.; Sulz, I.; Schindler, K.; Hiesmayr, M.; Chourdakis, M. Exploring factors influencing dietary intake during hospitalization: Results from analyzing nutritionDay’s database (2006–2013). Clin. Nutr. ESPEN 2020, 38, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Norshariza, J.; Siti Farrah Zaidah, M.; Basmawati, B.; Leow, C.; Lina, I.; Norafidza, A.; Khalizah, J.; John Kong, J.P.; Lim, S.M. Evaluation of Factors Affecting Food Wastage among Hospitalized Patients on Therapeutic Diet at Ministry of Health (MOH) Hospitals. Asian J. Diet. 2019, 1, 111–120. [Google Scholar]
- Keller, H.; Allard, J.; Vesnaver, E.; Laporte, M.; Gramlich, L.; Bernier, P.; Davidson, B.; Duerksen, D.; Jeejeebhoy, K.; Payette, H. Barriers to food intake in acute care hospitals: A report of the Canadian Malnutrition Task Force. J. Hum. Nutr. Diet. 2015, 28, 546–557. [Google Scholar] [CrossRef]
- Sun, H.; Zhang, L.; Zhang, P.; Yu, J.; Kang, W.; Guo, S.; Chen, W.; Li, X.; Wang, S.; Chen, L.; et al. A comprehensive nutritional survey of hospitalized patients: Results from nutritionDay 2016 in China. PLoS ONE 2018, 13, 1–16. [Google Scholar] [CrossRef]
- Palmer, M.; Huxtable, S. Aspects of protected mealtimes are associated with improved mealtime energy and protein intakes in hospitalized adult patients on medical and surgical wards over 2 years. Eur. J. Clin. Nutr. 2015, 69, 961–965. [Google Scholar] [CrossRef]
- Guenter, P.; Jensen, G.; Patel, V.; Miller, S.; Mogensen, K.M.; Malone, A.; Corkins, M.; Hamilton, C.; Dimaria-Ghalili, R.A. Addressing Disease-Related Malnutrition in Hospitalized Patients: A Call for a National Goal. Jt. Comm. J. Qual. Patient Saf. 2015, 41, 469–473. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics. Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process. Available online: https://www.andeal.org/evidence-analysis-manual (accessed on 10 September 2020).
- Handu, D.; Moloney, L.; Wolfram, T.; Ziegler, P.; Acosta, A.; Steiber, A. Academy of Nutrition and Dietetics Methodology for Conducting Systematic Reviews for the Evidence Analysis Library. J. Acad. Nutr. Diet. 2016, 116, 311–318. [Google Scholar] [CrossRef]
- Beelen, J.; Vasse, E.; Janssen, N.; Roos, N.M.D.; De Groot, L.C.P.G.M. Protein-enriched familiar foods and drinks improve protein intake of hospitalized older patients: A randomized controlled trial. Clin. Nutr. 2018, 37, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Munk, T.; Bruun, N.; Nielsen, M.A.; Thomsen, T. From Evidence to Clinical Practice: Positive effect of implementing a protein-enriched hospital menu in conjunction with individualized dietary counseling. Nutr. Clin. Pract. 2017, 32, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Navarro, D.A.; Shapiro, Y.; Birk, R.; Boaz, M. Orange napkins increase food intake and satisfaction with hospital food service: A randomized intervention. Nutr. X 2019, 3–4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.; Haines, T.P.; Truby, H. The efficacy of Protected Mealtimes in hospitalised patients: A stepped wedge cluster randomised controlled trial. BMC Med. 2017, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rüfenacht, U.; Ruhlin, M.; Wegmann, M.; Imoberdorf, R.; Ballmer, P.E. Nutritional counseling improves quality of life and nutrient intake in hospitalized undernourished patients. Nutrition 2010, 26, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Ingadottir, A.R.; Hilmisdottir, H.B.; Ramel, A.; Gunnarsdottir, I. Energy-and Protein Intake of Surgical Patients after The Implementation of Energy Dense Hospital Menus. Clin. Nutr. ESPEN 2015, 10, e107–e111. [Google Scholar] [CrossRef] [PubMed]
- Holst, M.; Beermann, T.; Mortensen, M.N.; Skadhauge, L.B.; Lindorff-larsen, K.; Rasmussen, H. Multi-modal intervention improved oral intake in hospitalized patients. A one-year follow-up study. Clin. Nutr. 2015, 34, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Beermann, T.; Mortensen, M.N.; Skadhauge, L.B.; Høgsted, R.H.; Rasmussen, H.H.; Holst, M. Protein and energy intake improved by breakfast intervention in hospital. Clin. Nutr. ESPEN 2016, 13, e23–e27. [Google Scholar] [CrossRef] [PubMed]
- Van der Zanden, L.D.T.; van Essen, H.; van Kleef, E.; De Wijk, R.A.; van Trijp, H.C.M. Using a verbal prompt to increase protein consumption in a hospital setting: A field study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, K.L.; Webb, L.; Vivanti, A.; Varghese, P.; Ferguson, M. Comparison of three interventions in the treatment of malnutrition in hospitalised older adults: A clinical trial. Nutr. Diet. 2013, 70, 325–331. [Google Scholar] [CrossRef]
- Barrington, V.; Maunder, K.; Kelaart, A. Engaging the patient: Improving dietary intake and meal experience through bedside terminal meal ordering for oncology patients. J. Hum. Nutr. Diet. 2018, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Doorduijn, A.S.; van Gameren, Y.; Vasse, E.; de Roos, N.M. At Your Request® room service dining improves patient satisfaction, maintains nutritional status, and offers opportunities to improve intake. Clin. Nutr. 2016, 35, 1174–1180. [Google Scholar] [CrossRef]
- Hickson, M.; Connolly, A.; Whelan, K. Impact of Protected Mealtimes on Ward Mealtime Environment, Patient Experience and Nutrient Intake in Hospitalised Patients. Hum. Nutr. Diet. 2011, 24, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Holst, M.; Beerman, T.; Mortensen, M.N.; Skadhauge, L.B.; Køhler, M.; Lindorff-larsen, K.; Rasmussen, H.H. Optimizing Protein and Energy Intake in Hospitals by Improving Individualized Meal Serving, Hosting and the Eating Environment. Nutrition 2017, 34, 14–20. [Google Scholar] [CrossRef]
- Chan, C.; Koo, H.; Auyeung, T.-W.; Liu, T.-Y.; Sin, K.-L.; Man, S.-P.; Woo, C.-C.; Lai, Y.-L.; Chiu, L.-P. Use of condiments to increase oral food intake of older patients. Asian J. Gerontol. Geriatr. 2017, 12, 47–52. [Google Scholar]
- McCray, S.; Maunder, K.; Barsha, L.; Mackenzie-Shalders, K. Room service in a public hospital improves nutritional intake and increases patient satisfaction while decreasing food waste and cost. J Acad Nutr Diet. 2018, 112, 284–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, S.; Williams, L.T.; Sladdin, I.; Neil, H.; Hopper, Z.; Jenkins, J.; Spencer, A.; Marshall, A.P. Improving nutrition care, delivery, and intakes among hospitalised patients: A mixed methods, integrated knowledge translation study. Nutrients 2019, 11, 1417. [Google Scholar] [CrossRef] [Green Version]
- Calleja-fernández, A.; Velasco-gimeno, C.; Vidal-casariego, A.; Pintor-de-la-Maza, B.; Frías-Soriano, L.; Villar-Taibo, R.; García-Peris, P.; Cano-Rodríguez, I.; García-Fernández, C.; Ballesteros-Pomar, M.D. Impact of kitchen organization on oral intake of malnourished inpatients: A two-center study. Endocrinol. Diabetes Nutr. 2017, 64, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Sathiaraj, E.; Priya, K.; Chakraborthy, S.; Rajagopal, R. Patient-Centered Foodservice Model Improves Body Weight, Nutritional Intake and Patient Satisfaction in Patients Undergoing Cancer Treatment. Nutr. Cancer 2019, 71, 418–423. [Google Scholar] [CrossRef]
- Young, A.M.; de Jersey, S.J.; Ellick, J.; Lewis, C.; Banks, M. Comparison of Patient Food Intake, Satisfaction and Meal Quality Between Two Meal Service Styles in a Geriatric Inpatient Unit Meal Quality Between Two Meal Service Styles in a Geriatric Inpatient Unit. J. Nutr. Gerontol. Geriatr. 2018, 37, 158–168. [Google Scholar] [CrossRef] [Green Version]
- Collins, J.; Porter, J.; Truby, H.; Huggins, C.E. A foodservice approach to enhance energy intake of elderly subacute patients: A pilot study to assess impact on patient outcomes and cost. Age Aging 2017, 46, 486–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijxhoorn, D.N.; IJmker-Hemink, V.; Wanten, G.J.A.; van den Berg, M.G.A. Strategies to increase protein intake at mealtimes through a novel high-frequency food service in hospitalized patients. Eur. J. Clin. Nutr. 2019, 73, 910–916. [Google Scholar] [CrossRef]
- Goeminne, P.C.; De Wit, E.H.; Burtin, C.; Valcke, Y. Higher food intake and appreciation with a new food delivery system in a Belgian hospital. Meals on Wheels, a bedside meal approach q A prospective cohort trial. Appetite 2012, 59, 108–116. [Google Scholar] [CrossRef]
- Young, A.M.; Banks, M.D.; Mudge, A.M. Improving nutrition care and intake for older hospital patients through system-level dietary and mealtime interventions. Clin. Nutr. ESPEN 2018, 24, 140–147. [Google Scholar] [CrossRef]
- Munk, T.; Seidelin, W.; Rosenbom, E.; Nielsen, A.L.; Klausen, T.W.; Nielsen, M.A.; Thomsen, T. A 24-h a la carte food service as support for patients at nutritional risk: A pilot study. Hum. Nutr. Diet. 2012, 26, 268–275. [Google Scholar] [CrossRef]
- Markovski, K.; Nenov, A.; Ottaway, A.; Skinner, E. Does eating environment have an impact on the protein and energy intake in the hospitalised elderly? Nutr. Diet. 2017, 74, 224–228. [Google Scholar] [CrossRef]
- Farrer, O.; Olsen, C.; Mousley, K.; Teo, E. Does presentation of smooth pureed meals improve patients consumption in an acute care setting: A pilot study. Nutr. Diet. 2015, 73, 405–409. [Google Scholar] [CrossRef]
- Lindman, A.; Brygger, H.; Frost, N. Food caregivers influence on nutritional intake among admitted haematological cancer patients–A prospective study. Eur. J. Oncol. Nurs. 2013, 17, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Maunder, K.; Lazarus, C.; Walton, K.; Williams, P.; Ferguson, M.; Beck, E. Energy and protein intake increases with an electronic bedside spoken meal ordering system compared to a paper menu in hospital patients. Clin. Nutr. ESPEN 2015, 10, e134–e139. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, M.N.; Larsen, A.K.; Skadhauge, L.B.; Høgsted, R.H.; Beermann, T.; Cook, M.E.; Holst, M. Protein and energy intake improved by in-between meals: An intervention study in hospitalized patients. Clin. Nutr. ESPEN 2019, 30, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Navarro, D.A.; Boaz, M.; Krause, I.; Elis, A.; Chernov, K.; Giabra, M.; Levy, M.; Giboreau, A.; Kosak, S.; Mouhieddine, M.; et al. Improved meal presentation increases food intake and decreases readmission rate in hospitalized patients. Clin. Nutr. 2016, 35, 1153–1158. [Google Scholar] [CrossRef]
- Manning, F.; Harris, K.; Duncan, R.; Walton, K.; Bracks, J.; Larby, L.; Vari, L.; Jukkola, K.; Bell, J.; Chan, M.; et al. Additional feeding assistance improves the energy and protein intakes of hospitalised elderly patients. A health services evaluation. Appetite 2012, 59, 471–477. [Google Scholar] [CrossRef]
- Keller, H.H.; Chambers, L.W.; Fergusson, D.A.; Niezgoda, H.; Parent, M.; Caissie, D.; Lemire, N. A mix of bulk and ready-to-use modified-texture food: Impact on older adults requiring dysphagic food. Can. J. Aging. 2012, 31, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Laur, C.; Butterworth, D.; Nasser, R.; Bell, J.; Marcell, C.; Murphy, J.; Valaitis, R.; Bernier, P.; Ray, S.; Keller, H. Impact of Facilitated Behavior Change Strategies on Food Intake Monitoring and Body Weight Measurements in Acute Care: Case Examples From the More-2-Eat Study. Nutr. Clin. Pract. 2019, 34, 459–474. [Google Scholar] [CrossRef] [PubMed]
- Ofei, K.T.; Holst, M.; Rasmussen, H.H.; Mikkelsen, B.E. Effect of meal portion size choice on plate waste generation among patients with different nutritional status. An investigation using Dietary Intake Monitoring System (DIMS). Appetite 2015, 91, 157–164. [Google Scholar] [CrossRef]
- Capra, S.; Wright, O.; Sardie, M.; Bauer, J.; Askew, D. The Acute Hospital Foodservice Patient Satisfaction Questionnaire: The Development of a Valid and Reliable Tool to Measure Patient Satisfaction with Acute Care Hospital Foodservices. Foodserv. Res. Int. 2005, 16, 1–14. [Google Scholar] [CrossRef]
- Schindler, K.; Themessl-huber, M.; Hiesmayr, M.; Kosak, S.; Lainscak, M.; Laviano, A.; Pichard, C. To eat or not to eat? Indicators for reduced food intake in 91,245 patients hospitalized on nutritionDays 2006–2014 in 56 countries worldwide: A descriptive analysis. Am. J. Clin. Nutr. 2016, 104, 1393–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maia, I.; Xará, S.; Vaz, D.; Shiang, T.; Amaral, T.F. Undernutrition risk at hospital admission and length of stay among pulmonology inpatients. Pulmonology 2018, 24, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Nigatu, Y.D.; Gebreyesus, S.H.; Allard, J.P.; Endris, B.S. The effect of malnutrition at admission on length of hospital stay among adult patients in developing country: A prospective cohort study. Clin. Nutr. ESPEN 2021, 41, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Hartwell, H.; Johns, N.; Edwards, J.S.A. E-menus—Managing choice options in hospital foodservice. International Int. J. Hosp. Manag. 2016, 53, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Prgomet, M.; Li, J.; Li, L.; Georgiou, A.; Westbrook, J.I. The impact of electronic meal ordering systems on hospital and patient outcomes: A systematic review. Int. J. Med. Inform. 2019, 129, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Hartwell, H.; Edwards, J.S.A. A Preliminary Assessment of Two Hospital Food Service Systems Using Parameters of Food Safety and Consumer Opinion. J. R. Soc. Promot. Health 2001, 4, 236–242. [Google Scholar] [CrossRef]
- Hartwell, H.J.; Edwards, J.S.A.; Beavis, J. Plate versus Bulk Trolley Food Service in a Hospital: Comparison of Patients’ Satisfaction. Nutrition 2007, 23, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Jamaluddin, R.; Manan, N.A.A.; Basri, A.M.; Karim, M.S.A. Patients’ Satisfaction with the Bulk Trolley System in a Government Hospital in Malaysia. Leadersh. Health Serv. 2010, 27, 229–315. [Google Scholar] [CrossRef]
- Johns, N.; Edwards, J.S.A.; Hartwell, H.J. Hungry in hospital, well-fed in prison? A comparative analysis of food service systems. Appetite 2013, 68, 45–50. [Google Scholar] [CrossRef] [PubMed]
- British Dietetics Association. Available online: https://www.bda.uk.com/specialist-groups-and-branches/food-services-specialist-group/nutrition-and-hydration-digest.html (accessed on 18 March 2021).
- Pullen, K.; Collins, R.; Stone, T.; Carter, H.; Sadler, H.; Collinson, A. Are energy and protein requirements met in hospital? J. Hum. Nutr. Diet. 2017, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jayadevappa, R.; Chhatre, S. Patient Centered Care—A Conceptual Model and Review of the State of the Art Identification of Studies. Open Health Serv. Policy J. 2011, 4, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Nichani, S.; Fitterman, N.; Lukela, M.; Crocker, J. Team Approach and Multidisciplinary Care. Hospital Medicine Revised Core Competencies. J. Hosp. Med. 2017, 12, S81. [Google Scholar] [CrossRef] [Green Version]
- Leary, K.J.O.; Sehgal, N.L.; Terrell, G.; Williams, M.V. Interdisciplinary Teamwork in Hospitals: A Review and Practical Recommendations for Improvement. J. Hosp. Med. 2012, 7, 48–54. [Google Scholar] [CrossRef]
- Tappenden, K.A.; Quatrara, B.; Parkhurst, M.L.; Malone, A.M.; Fanjiang, G.; Ziegler, T.R. Critical Role of Nutrition in Improving Quality of Care: An Interdisciplinary Call to Action to Address Adult Hospital Malnutrition. J. Acad. Nutr. Diet. 2013, 113, 1219–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walton, K.; Williams, P.; Tapsell, L.; Hoyle, M.; Shen, Z.W.; Gladman, L.; Nurka, M. Observations of mealtimes in hospital aged care rehabilitation wards. Appetite 2013, 67, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, S.M.; Martin, H.J.; Roberts, H.C.; Sayer, A.A. A systematic review of the use of volunteers to improve mealtime care of adult patients or residents in institutional settings. J. Clin. Nurs. 2011, 20, 1810–1823. [Google Scholar] [CrossRef] [PubMed]
- Munk, T.; Beck, A.M.; Holst, M.; Rosenbom, E.; Rasmussen, H.H.; Nielsen, M.A.; Thomsen, T. Positive effect of protein-supplemented hospital food on protein intake in patients at nutritional risk: A randomised controlled trial. J. Hum. Nutr. Diet. 2014, 27, 122–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaid, Z.A.; Lim, V.; Chiann, C.; Jamhuri, N. Plate Wastage among Hospitalized Cancer Patients. Malays. J. Med. Health Sci. 2019, 15, 84–89. [Google Scholar]
- Abdelhafez, A.M.; Al Qurashi, L.; Al Ziyadi, R.; Kuwair, A.; Shobki, M.; Mograbi, H. Analysis of Factors Affecting the Satisfaction Levels of Patients Toward Food Services at General Hospitals in Makkah, Saudi Arabia. Am. J. Med. Med. Sci. 2012, 2, 123–130. [Google Scholar] [CrossRef]
- Messina, G.; Fenucci, R.; Vencia, F.; Niccolini, F.; Quercioli, C.; Nante, N. Patients’ Evaluation of Hospital Foodservice Quality in Italy: What Do Patients Really Value? Public Health Nutr. 2013, 16, 730–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahin, B.; Demir, C.; Celik, Y.; Teke, A.K. Factors Affecting Satisfaction Level with The Food Services in a Military Hospital. J. Med. Syst. 2006, 30, 381–387. [Google Scholar] [CrossRef]
- Wright, O.R.L.; Connelly, L.B.; Capra, S. Consumer Evaluation of Hospital Foodservice Quality: An Empirical Investigation. Int. J. Health Care Qual. Assur. 2006, 19, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.; Wei, C.; Koechl, J.M.; Keller, H. The effect of blue dishware versus white dishware on food intake and eating challenges among residents living with dementia: A crossover trial. BMC Res. Notes 2020, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: Strengths and weaknesses. FASEB J. 2014, 22, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated Ma). The Cochrane Collaboration. 2015. Available online: www.cochrane_handbook.org (accessed on 25 March 2021).
- West, S.L.; Gartlehner, G.; Mansfield, A.J.; Poole, C.; Tant, E.; Lenfestey, N.; Lux, J.L.; Amoozegar, J.; Morton, S.C.; Carey, T.C.; et al. Comparative Effectiveness Review Methods: Clinical Heterogeneity; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2010. Available online: https://www.ncbi.nlm.nih.gov/books/NBK53310/ (accessed on 23 March 2021).


{kind=link}
| Author (s), (Year), Country | Study Design; Sample Size; Age Group; Study Duration | Types of Intervention Strategies | Outcome Parameters | Results | Summary of Findings |
|---|---|---|---|---|---|
| Beelen et al. (2018) [15], Netherlands | RCT; 147 patients (RCT: 67; control: 80); patients ≥65 years old; 7 months | Meal composition modification | Protein intake | Protein intake: RCT = 105.7 ± 34.2 g vs. Control = 88.2 ± 24.4 g (p < 0.01). More patients in RCT than control group reached a protein intake of 1.2 G/KG/D (79% vs. 47.5%). | High protein intake in the intervention group. |
| Munk et al. (2017) [16], Denmark | RCT; 91 patients (HIG = 41, and IG = 50); >18 years old; 8 months | Multidisciplinary approaches | Energy and protein intake Estimation of energy and protein requirement | >75% of energy requirement: IG = 92% vs. HIG = 76% (p = 0.04). >75% of protein requirement: IG = 90% vs. HIG = 66% (p = <0.01) | High mean energy and protein intake and the high number of patients reached >75% of energy and protein requirement in IG. |
| Navarro et al. (2019) [17], Israel | Intervention study randomized patients; 131 patients (white napkin: 65, orange napkin: 66); >18 years old; NA | Meal presentation | Food intake Patient satisfaction | IG consumed 17.6% more hospital-provided food than CG. IG significantly greater satisfaction with the hospital’s food service than CG. | Increase food intake and patient satisfaction in the intervention group. |
| Porter et al. (2017) [18], Australia | A prospective, stepped wedge cluster randomized controlled trial; 149 patients; ≥65 years old; 4 weeks | Protected mealtime | Energy and protein intake Nutritional status | Energy intake: IG (6479 ± 2486 kJ/day) vs. CG (6532 ± 2328 kJ/day), p = 0.88. Protein intake: IC (68.6 ± 26.0 g/day) vs. CG (67.0 ± 25.2 g/day), p = 0.86. Energy deficit: (coefficient [robust 95% CI], p value) of −1405 (−2354 to −457), p = 0.004 | No significant difference in energy and protein intake for both groups. Significant finding in energy deficit. |
| Rüfenacht et al. (2010) [19], Switzerland | RCT; 36 patients (NT group = 18 vs. ONS group = 18); >18 years old; 10–15 days | Multidisciplinary approaches | Food intake QOL | Energy and protein intakes increased in both groups (p = 0.001). Energy intake that meets ER: NT (107%) vs. ONS (90%) Protein intake meets PR: NT (94%) vs. ONS (88%). QOL increased in NT (p = 0.016). | Increased QOL, energy and protein intake in both groups. |
| Ingadottir et al. (2015) [20], Iceland | Intervention study; 161 patients (2011 = 69, and 2013 = 92); ≥18 years old; 5 months | Menu modification | Energy and protein intake | Energy intake: IG (1293 ± 386 kcal/d) vs. CG (1096 ± 340 kcal/d), p = 0.001. Protein intake: IG (54.0 ± 17.8 g/d) vs. CG (49.1 ± 16.1 g/d), p = 0.085 | Increased energy intake in the intervention group. |
| Holst et al. (2015) [21], Denmark | An observational multi-model intervention study; 545 patients (baseline = 287 patients, post intervention = 258 patients); >18 years old; 12 months from the baseline | Multidisciplinary approaches | Energy and protein intake Staff KAP regarding clinical nutrition GNP initiatives | Energy intake improved from 52% to 68% (p < 0.007). Protein intake from 33% to 52% (p < 0.001) (>75% of requirements). Intake of less than 50% of requirements decreased with 50%. Screening improved from 56% to 77% (p < 0.001). Nutrition plans from 21% to 56% (p < 0.0001). Monitoring food intake from 29% to 58% (p < 0.0001). | Improvement in energy and protein intake. Improvement of screening and monitoring the food intake process. |
| Beermann et al. (2016) [22], Denmark | Intervention study; 60 patients (baseline:32; follow-up:30); >18-year-old; 6 weeks | Menu modification | Energy intake Protein intake | Energy intake at breakfast: CG (14%) vs. IG (22%), p < 0.001. Protein intake breakfast: CG (14 g) vs. IG (20 g), p < 0.002. Total protein intake: CG (64%) vs. IG (77%), p = 0.05. Total energy intake: CG (76%) vs. IG (99%), p < 0.01. | Energy and protein intake were improved. |
| van der Zanden et al. (2015) [23], Netherlands | Intervention study; 208 patients (control = 63 vs. intervention = 145); ≥18 years old; 14 days of 4 consecutive weeks | Foodservice system | Protein intake Caloric content Ordering of the target product | Meal ordering: CG (6.5%) vs. IG (45.2%). Protein content: larger in IG > CG (p < 0.025) | High significant protein intake and content in the intervention group. |
| Campbell et al. (2013) [24], Australia | Intervention study; 98 patients (group 1 traditional: 33; group 2 MedPass: 32; group 3 mid-meal trolley: 33); ≥60 years old; 24 months | Menu and meal composition modification | Food intake Energy intake Protein intake Clinical measurements QOL Cost assessment Patient satisfaction | Weight changes (mean ± SD): traditional = 0.4 ± 3.8%, MedPass = 1.5 ± 5.8%, mid-meal = 1.0 ± 3.1% (p = 0.53) Energy intake and protein intake (% of requirement): traditional (107 ± 26, 128 ± 35%), MedPass (109 ± 28, 126 ± 38%), mid-meal = (85 ± 25, 88 ± 26%) (p = 0.003 and p < 0.001, respectively) QoL ratings (scale 0–100): MedPass (mean change, 12.4 ± 20.9), mid-meal (21.1 ± 19.7), traditional (1.5 ± 18.1) (p = 0.05). Patient satisfaction: sensory qualities (taste, look, temperature, size) and perceived benefit (improved health and recovery) was rated highest for mid-meal trolley (all p < 0.05). | Significantly increased food intake and patient satisfaction improved QoL and cost-effectiveness in the intervention groups. Energy and protein intake was achieved in both groups. |
| Barrington et al. (2018) [25], Australia | An observational point prevalence study; Oncology patients (BMOS: 105; PMs: 96); >18 years old; 18 months | Foodservice system | Dietary intake Plate waste Meal ordering Patient meal experience survey | Meal ordering: Energy = BMOS (8683 kJ day−1) vs. PM (6773 kJ day−1), p = 0.004); Protein = BMOS (97 g day−1) vs. PM (82 g day−1), p = 0.023. Food intake: Energy = BMOS (6457 kJ day−1) vs. PM (4805 kJ day−1), p < 0.001; Protein = BMOS (73 g day−1) vs. PM (58 g day−1), p < 0.001. Plate waste: BMOS (34.3 ± 4.9) vs. PM (35.3 ± 4.5), p = 0.75 Patient meal experience survey = significant increase in BMOS receiving ordered food (p < 0.001), able to choose their preferred food (p = 0.006) and able to assess nutritional information of the menu (p = 0.002) compared to the PM. | A significant increase in food intakes and meal experience improved upon access to nutritional information in the intervention group. |
| Doorduijn et al. (2016) [26], Netherlands | An observational prospective study; 337 patients (traditional meal system = 168, At Your Request® = 169); ≥18 years old; 12 months | Foodservice system | Patient satisfaction Nutritional status Food choice and food intake | Patient satisfaction: increased after intervention from 7.5 to 8.1 (scale 1–10) and 124.5 to 135.9 point on a nutrition-related quality of life questionnaire (p < 0.05). Body weight: Traditional meal service (83.7 to 83.5 (0.2 ± 2.7) kg, p = 0.824), At Your Request® (77.6 kg to 77.4 (0.2 ± 2.6) kg, p = 0.851) Handgrip strength: Traditional meal service (Day 1: 30.2 kg, End: 30.5 kg) vs. At Your Request® (Day 1: 30.2 kg, End: 30.6 kg) MUST score: Improved in 18 patients in both groups. Protein intake (based on food records from patients on energy and protein enriched diet): Traditional meal service (n = 34, 0.91 g/kg) vs. At Your Request® (n = 38, 0.84 g/kg). | Significantly higher intake of energy and protein, and patient satisfaction in the intervention group. MUST score improved in both groups. |
| Hickson et al. (2011) [27], United Kingdom | Direct observational study; 99 patients (baseline = 39, PM = 60); NA; baseline: June/July 2008, PM: Oct/Nov 2009 | Protected mealtime | Mealtime experience Nutrient intake | Mealtime experience: Monitor using food/fluid charts (before PM (32%) vs. after PM (43%), p = 0.14); wash hands offer (before PM (30%) vs. after PM (40%), p = 0.03); served meals at uncluttered tables (before PM (54%) vs. after PM (64%), p = 0.04; experiencing mealtime interruptions (before PM (32%) vs. after PM (25%), p = 0.14). Energy intake: 1088 kJ vs. 837 kJ, p = 0.25 Protein intake: 14.0 g vs. 7.5 g, p = 0.25 | Improvement in mealtime experience. There was a decrease in protein intake observed after the implementation of PM. |
| Holst et al. (2017) [28], Denmark | Interventional study: 67 patients (baseline = 30, follow up = 37); >18 years old; 3 months | Multidisciplinary approaches | Demographic information Energy and protein intake Patient-perceived quality Staff-perceived quality | Food intake: Energy intake: the overall group (67.6% vs. 40%; p = 0.036) vs. the Heart–Lung Surgery group (85.7 vs. 38.5; p = 0.036); Protein intake: the overall group (37.8% vs. 33.3%, p = 0.7037). Patient and staff-perceived quality: IG reported satisfaction regarding individualized food serving, nurse communication, and improved meal environments. | The food and energy intake, patient satisfaction on individualize meal serving and nurse communication, and meal environment were improved in the intervention group. |
| Chan et al. (2017) [29], Hong Kong | Pre-post design; 100 older patients (male: 49; female: 51); >65 years old; 3 months | Menu modification | Food intake | Food intake: IG (68%) vs. CG (57%). Increased intake of food, energy, protein, and sodium in IG by 8% (p < 0.05), 10% (p < 0.01), 9% (p < 0.01), and 53% (p < 0.01), in all patients, and by 13% (p < 0.01), 19% (p < 0.01), 17% (p < 0.01), and 67% (p < 0.01). | Increased intake of food, energy, protein, and sodium intake in lunch with condiments. |
| McCray et al. (2018) [30], Australia | Pre-post study design; 187 patients (TM = 84 and RS = 103 patients respectively); >18 years old; 1 month for each cohort | Foodservice system | Nutritional intake Plate waste Patient satisfaction Patient meal cost | Energy intake: TM (5513 kJ day−1) vs. RS (6379 kJ day−1), p = 0.020 Protein intake: TM (53 g day−1) vs. RS (74 g day−1), p < 0.001 Plate waste: TM (30%) vs. RS (17%), p < 0.001 Patient satisfaction: TM (75%) vs. RS (98%), p < 0.04 Food cost: decreased by 28% per annum with RS. | Significant increases in energy and protein intake, improved patient satisfaction, reduced plate waste and food cost in the intervention group. |
| Palmer and Huxtable (2015) [10], Australia | Pre-post study; 798 patients (Pre-PMP = 348 vs. Post-PMP = 450); >18 years old; 24 months | Protected mealtime and mealtime assistant | Food intake Aspects of protected mealtimes | Food intake: mean intake energy (1419 ± 614 kJ) and protein (15 ± 7 g); intakes associated with gender, age, season, stopping or refusing a meal, time until discharge and eating at dinner (B = − 829–222 kJ, B = − 8.8 to 2.2 g protein, p = 0.000–0.032); Intake in intervention group (p = 0.094–0.157); association of aspects of protected mealtimes with intake such as the need for mealtime assistance, introduction of mealtime volunteers, time to eat and appropriate positioning during mealtimes (B = 177–296 kJ, B = 0.07–3.9 g protein, p = 0.000–0.014, R2 = 0.148–0.154). Protein intake in those requiring mealtime assistance was associated with mealtime volunteers and appropriate positioning (B = 4.1–4.4 g protein, p = 0.013–0.026, R2 = 0.197). | The intake was associated with aspects of protected mealtimes, mealtime volunteers and appropriate positioning. |
| Roberts et al. (2019) [31], Australia | Observational, pre-post study; 207 patients (pre = 116 vs. post = 91); ≥18 years old; 2 months | Multidisciplinary approaches | Demographic data Food intakes Mealtime environment | Energy intake: Pre (4818 ± 2179 kJ) vs. Post (5384 ± 1865), p = 0.119 Protein intake: Pre (48 ± 24 g) vs. post (57 ± 22 g), p = 0.042 Mealtime interruption: Pre (111/423 meals) vs. Post (150/400 meals), p < 0.001. No. patients to receive their meal tray: Pre (76%) vs. Post (84%), p < 0.05 | The number of patients with sufficient food consumption was doubled, and mean energy and protein intakes were significantly higher. |
| Calleja-fernández et al. (2017) [32], Spain | A cross-sectional, two-centre study; 201 patients (TK), 41 patients (CK); >18 years old; 18 months | Foodservice system | Energy intake Protein intake | Food intake: TK (median: 76.83%, IQR 45.76%) vs. CK (median: 83.43%, IQR 40.49%), p < 0.001 Energy intake: CK (1741.6 (SD 584.0) kcal) vs. TK (1481.7 kcal (SD 584.0) kcal) vs. TK (1481.7 kcal (SD 576.0) kcal); p = 0.014, after the statistical adjustment (1608.1 (SD 134.9) vs. 1466.8 kcal (SD 80.5) kcal; p = 0.243) Protein intake: CK (90.5 (SD 4.4) g) vs. TK (70.4 (SD 2.0) g); p < 0.001). after statistical adjustment (CK = 80.0 (SD 6.4) g vs. TK = 67.6 (SD 3.8) g; p = 0.032) | Higher energy and protein intake in the intervention group before the statistical adjustment. |
| Sathiaraj et al. (2019) [33], India | Cross-sectional analytical study; 160 patients (traditional foodservice = 60 vs. patient-centered foodservice = 100); >18 years old; 4 months | Menu modification | Nutritional intake Patient satisfaction | Energy intake: Patient-centered model: mean (SD) 1633.33 (158.11) kcal; Traditional foodservice model: mean (SD) 1501.67(171.22) kcal; p <0.001 Protein intake: Patient-centered model: mean (SD) 59.89 (10.897) kcal; Traditional foodservice model: mean (SD) 48.42 (10.794) g; p <0.001 In-hospital weight change: Patient-centered foodservice: mean (SD) 0.18 (0.99) kg; Traditional foodservice: mean (SD) −0.58 (1.25); p <0.001 Patient satisfaction: Quality of food (28.6 vs. 35.2%), timeliness of delivery (36.2 vs. 37.1%), flavour of food (21.9 vs. 37.1%), special/restricted diet explained (41 vs. 41.9%), and overall satisfaction (36.2 vs. 42.9%); p = 0.000 | The mean of energy and protein intake, weight, and overall patient satisfaction in the intervention group was significantly increased. |
| Young et al. (2018) [34], Australia | Cross-sectional study; 30 patients (pre-plated n = 16; bistro style n =14); ≥65 years old; 4 weeks | Foodservice system | Dietary intake Patient satisfaction Meal quality | Energy intake: Bistro (2524 ± 927 kJ) vs. Pre-plate (2692 ± 857 kJ), p = 0.612 Protein intake: Bistro (29 ± 12 g) vs. Pre-plate (27 ± 11 g), p = 0.699 Patient satisfaction: appearance (preplated: 50%, Bistro: 46%), quality (preplated: 57%, bistro: 54%), staff demeanor (preplated: 100%, bistro: 92%) Meal quality: sensory properties (preplated: 4.2 ± 0.4, Bistro: 4.4 ± 0.7) and temperature accuracy (preplated: 3.1 ± 0.9, Bistro: 3.6 ± 1.3). | There is no difference in energy and protein intakes, patient satisfaction, or meal quality in both groups. |
| Ofei et al. (2015) [35], Denmark | Prospective observational cohort study; 71 patients (256 meals; lunch n = 142; supper n = 114); ≥18 years old; five weekdays | Menu and meal composition modification | Food intake Plate waste | Positive relationship between meal portion size and plate waste (p = 0.002) and increased food waste in patients at nutritional risk during supper (p = 0.001). | Increased the proportion of energy and protein consumption in both groups. There was a relationship between meal portion size and plate waste and increased food waste in patients at risk during supper. |
| Dijxhoorn et al. (2019) [36], Netherlands | A prospective cohort study; 637 subjects (TMS: 326, FfC: 311); ≥18 years old; TMS: 12 months, FfC: 12 months | Meal presentation | Protein intake per mealtime | Protein intake (g) at all mealtimes (p < 0.05) except for dinner (median (IQR) at breakfast: 17 (6.5–25.7) vs. 10 (3.8–17); 10:00 a.m.: 3.3 (0.3−5.3) vs. 1 (0−2.2); lunch: 17.6 (8.4−25.8) vs. 13 (7−19.4); 2:30 p.m.: 5.4 (0.8–7.5) vs. 0 (0–1.8); 7:00 p.m.: 1 (0–3.5) vs. 0 (0–1.7); 9:00 p.m.: 0 (0–0.1) vs. 0 (0–0)). Protein intake highest for both food services during dinner (20.9 g (8.4–24.1) vs. 20.5 g (10.5–27.8)) | Protein intake higher in the intervention group except for dinner. |
| Goeminne et al. (2012) [37], Belgium | Prospective cohort trial; 189 patients (control = 83, MOW = 106); ≥18 years old; 2 months | Foodservice system | Food intake Food waste Food access and appreciation | Food intake: 236 g more in patients in the MOW group compared to controls (95% confidence interval: 163–308 g) Food waste: significantly less waste in the MOW group (p < 0.0001) Food access and appreciation: patients appreciated Meals on Wheels more than the old system in terms of choice (p = 0.048; OR 6.8; 95% CI (0.8–58)), hunger (p = 0.0012), food quality (p < 0.0001) and organization. | Food intake significantly increased for each meal, with reduced food waste, and greater ONS use in the MOW group. Patient noted increases in terms of choice, hunger, food quality and organization in MOW group. |
| Young et al. (2018) [38], Australia | Prospective cohort study; 320 patients (cohort 1 n = 129; cohort 2 n = 139; cohort 3 n = 52); ≥65 years old; 5 months for each cohort | Protected mealtime and mealtime assistant | Energy and protein intake Nutrition care process | Energy intake: cohort 1: 5073 kJ/d; cohort 2: 5403 kJ/d; cohort 3: 5989 kJ/d, p = 0.04 Protein intake: cohort 1: 48 g/d, cohort 2: 50 g/d, cohort 3: 57 g/d, p = 0.02 | Energy and protein intakes were significantly improved between cohorts. |
| Munk et al. (2012) [39], Denmark | Historically controlled intervention pilot study; 40 patients; ≥ 18 years old; 10 weeks | Menu modification | Food intake | Energy intake: time gradient in energy intake (p = 0.0005, r = 0.53) Protein intake: 17.5% of the patients in the IG reached minimum p requirements (p = 0.17) | No significant difference in energy and protein intake in both groups. A significant time gradient was recorded in the energy intake. |
| Markovski et al. (2017) [40], Australia | A prospective observational pilot study; 34 patients; >65 years old; 3 months | Protected mealtime | Food intake MST | Food intake: patients consumed 20% more energy and protein when dining in a communal environment (p = 0.006 and 0.01, respectively) Patients with a BMI >22 (p = 0.01 and 0.01, respectively) and those with significant cognitive impairment (p = 0.001 and 0.007, respectively) ate 30% more protein and energy in the dining room, and those identified as at risk of malnutrition (MST ≥ 2) ate 42% more energy and 27% more protein in the dining room. | Higher energy and protein intakes and mealtime preferences among patients in the dining room. |
| Collins et al. (2017) [35], Australia | Parallel controlled pilot study; 122 geriatric patients; >65 years old; 4 months | Menu modification | Weight changes HGS Energy intake Protein intake Patient satisfaction | Weight changes: IG vs. CG (−0.55 (3.43) vs. 0.26 (3.33) %, p = 0.338) HGS change: IG vs. CG (mean (SD): 1.7 (5.1) versus 1.4 (5.8) kg, p = 0.798) Energy intake: IG vs. CG (mean (SD) 132 (38) vs. 105 (34) kJ/kg/day, p = 0.003). Protein intake: IG vs. C (mean (SD) 1.4 (0.6) vs. 1.1 (0.4) g protein/kg/day, p = 0.035) Patient satisfaction: food quality (p = 0.743), meal service (p = 0.559) or staffing and service (p = 0.816) scores, physical environment significantly higher among IG (p = 0.013). | Significant higher mean intake of energy and protein in the intervention group. |
| Farrer at al. (2015) [41], Australia | Pilot study; 66 patients (control group = 38, treatment group = 27); ≥18 years old; 2 weeks | Menu modification | Food intake Plate waste Patient satisfaction | Food intake: increased oral intake in the IG (p = 0.03) Plate waste: CG (median: 286 g) vs. IG (median: 160 g), p = 0.09 Patient satisfaction: no significant in both groups (p = 0.31) | Significantly increased food intake in the proportion of intervention group, but there was no significant change in all groups. |
| Lindman et al. (2013) [42], Denmark | Quasi-experimental; 87 patients (before = 42, after = 45); >18 years old; 1 year | Mealtime assistant | Food intake Nutritional requirement | Energy requirement: before-group (76.2% (CI 95% 64.6–87.9) vs. after-group (93.3% (CI 95% 82.3–104.3), p = 0.03. Energy intake: before-group 21 (51%) vs. after-group (30 (67%)), p = 0.145 Protein intake: before-group (16 (39%)) vs. after-group (16 (36%)), p = 0.74. | Higher energy intake in the intervention group. The patients were informed about their nutritional needs after the intervention. |
| Maunder et al. (2015) [43], Australia | The quasi-experimental pre-test post-test cohort study; 119 patients (PM = 54 patients, BMOS = 65 patients); ≥18 years old; 1 months for each phase | Foodservice system | Dietary intake Patient satisfaction NA role | Energy intake: PM vs. BMOS (6273 kJ vs. 8273 kJ), p < 0.05 Protein intake: PM vs. BMOS (66 g vs. 83 g), p < 0.05 Patient satisfaction: PM (84%) vs. BMOS (82%), p > 0.05. NA role: mean NA time with patients increased significantly from 0.33 to 0.35 min/patient/day (p < 0.05) | Most of the patients preferred the BMOS and mean daily energy and protein intakes were significantly increased in the intervention group. |
| Mortensen et al. (2019) [44], Denmark | A quasi-experimental design with a non-equivalent control group; 92 patients (46 before and 46 after the intervention; >18 years old; 11 months | Menu and meal composition modification | Energy and protein intake | Energy intake: increased from 74% to 109% (p < 0.00) of requirements. Protein intake: increased from 49% to 88% (p < 0.00) of requirements. | Increased total energy and protein intake from the requirements, including between meals. |
| Navarro et al. (2016) [45], Israel | The prospective open labeled, non-randomized controlled study; 206 patients (control = 101, experimental = 105); >18 years old; 3 weeks | Meal presentation | Food intake Food waste Readmission rate | Food intake: 9% significantly higher in the experimental group vs. control group (0.77 ± 0.25 vs. 0.58 ± 0.31) Food waste: starch Participants from the experimental group left on their plate less starch (experimental (0.19 ± 0.30) vs. control (0.52 ± 0.41), p < 0.05; main course (experimental (0.18 ± 0.31) vs. control (0.46 ±0.41), p < 0.05; vegetable (experimental (0.37 ± 0.36) vs. control (0.29 ± 0.35), p > 0.05. Readmission rate: control (31.2%) vs. experimental (13.5%), p < 0.02 | There was significantly higher food intake, less food waste, improved food taste and decreased readmission rate in the intervention group. |
| Manning et al. (2012) [46], Australia | Mixed methods design; 23 patients; >65 years old; 3 months | Mealtime assistant | Food intake Grip strength MNA | Food intake: Energy and protein intakes increased significantly (396 kJ and 4.3 g, respectively) when volunteers were present. MNA: 52% at risk (MNA score between 17 and 23.5) and 35% malnourished (MNA score <17). | Energy and protein intake increased significantly during lunchtimes when volunteers were present. |
| Keller et al. (2012) [47], Canada | Prospective interrupted time-series study; 67 patients; ≥60 years old; 9 months | Menu and meal composition modification | Nutritional status Food intake Co-morbidity Oral supplements | Nutritional status: 74% patients achieved their goal weight at the end of the intervention period. Food intake: nonsignificant decrease in total grams of main-plate food consumed during the six-month intervention period when compared with the control period (p = 0.11). | Most of the patients in the intervention group achieved their weight goals. No significant difference in main-plate food intake. Higher fat intake in the intervention group. |
| Laur et al. (2019) [48], Canada | Case study approach; 4000 patients (Site A: 1127, Site B: 860, Site D: 988, Site E: 968); ≥18 years old; 18 months | Multidisciplinary approaches | Food intake Body weight | Food intake monitoring: Site A (Increased from 0% to 97%). Site E (increased from 0% to 61%). Site B (improved from 3% to 95%). Body weight monitoring: Site A (improved from 14% to 63%), Site D (improved from 11% to 49%). | Food intake and body weight improved through interdisciplinary team approaches and documentation. |
| Reference | Validity Items a | Quality Rating | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
| Beelen et al. (2018) [15] | + | + | + | + | + | + | + | + | - | - | Positive |
| Munk et al. (2017) [16] | + | + | - | - | U | + | + | + | + | NA | Neutral |
| Navarro et al. (2019) [17] | + | + | + | NA | + | + | + | + | + | NA | Positive |
| Porter et al. (2017) [18] | + | + | + | U | + | + | + | + | + | + | Positive |
| Rüfenacht et al. (2010) [19] | + | + | + | + | - | + | + | + | + | - | Positive |
| Ingadottir et al. (2015) [20] | + | + | + | - | - | + | + | + | + | + | Positive |
| Holst et al. (2015) [21] | + | + | + | + | - | + | + | + | + | U | Positive |
| Beermann et al. (2016) [22] | + | + | + | + | - | + | + | + | + | - | Positive |
| van der Zanden et al. (2015) [23] | + | + | + | NA | + | + | U | + | + | + | Neutral |
| Campbell et al. (2013) [24] | + | + | + | U | U | + | + | + | + | + | Positive |
| Barrington et al. (2018) [25] | + | + | + | - | - | + | + | + | + | + | Positive |
| Doorduijn et al. (2016) [26] | + | + | + | + | - | + | + | + | U | + | Positive |
| Hickson et al. (2011) [27] | + | + | + | + | + | + | + | + | + | + | Positive |
| Holst et al. (2017) [28] | + | + | + | + | + | + | + | + | + | U | Positive |
| Chan et al. (2017) [29] | + | + | + | - | - | + | U | + | + | - | Neutral |
| McCray et al. (2018) [30] | + | U | - | + | - | + | + | + | + | + | Neutral |
| Palmer and Huxtable (2015) [10] | + | + | + | + | U | + | + | + | + | + | Positive |
| Roberts et al. (2019) [31] | + | + | - | + | NA | + | + | + | + | + | Neutral |
| Calleja-fernández et al. (2017) [32] | + | U | - | + | - | + | + | + | + | + | Neutral |
| Sathiaraj et al. (2019) [33] | + | + | - | + | - | + | + | + | + | + | Neutral |
| Young et al. (2018) [34] | + | + | U | + | - | + | + | + | + | + | Neutral |
| Ofei et al. (2015) [35] | + | + | + | + | - | + | + | + | + | - | Positive |
| Dijxhoorn et al. (2019) [36] | + | + | - | + | - | + | + | + | + | + | Positive |
| Goeminne et al. (2012) [37] | + | + | + | - | - | + | + | + | + | - | Positive |
| Young et al. (2018) [38] | + | + | + | + | + | + | + | + | + | + | Positive |
| Munk et al. (2012) [39] | + | + | + | + | - | + | + | + | + | + | Positive |
| Markovski et al. (2017) [40] | + | + | + | + | - | + | + | + | + | + | Positive |
| Collins et al. (2017) [35] | + | + | + | + | - | + | + | + | + | + | Positive |
| Farrer et al. (2015) [41] | + | + | + | U | - | + | + | + | + | + | Positive |
| Lindman et al. (2013) [42] | + | + | + | + | - | + | + | + | + | + | Positive |
| Maunder et al. (2015) [43] | + | + | + | + | NA | + | + | + | + | + | Positive |
| Mortensen et al. (2019) [44] | + | + | + | + | NA | + | + | + | + | + | Positive |
| Navarro et al. (2016) [45] | + | + | + | NA | NA | + | + | + | + | + | Positive |
| Manning et al. (2012) [46] | + | + | + | + | NA | + | + | + | + | - | Positive |
| Keller et al. (2012) [47] | + | + | + | NA | + | + | + | + | + | NA | Positive |
| Laur et al. (2019) [48] | + | NA | - | - | - | + | + | U | + | + | Neutral |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osman, N.S.; Md Nor, N.; Md Sharif, M.S.; Hamid, S.B.A.; Rahamat, S. Hospital Food Service Strategies to Improve Food Intakes among Inpatients: A Systematic Review. Nutrients 2021, 13, 3649. https://doi.org/10.3390/nu13103649
Osman NS, Md Nor N, Md Sharif MS, Hamid SBA, Rahamat S. Hospital Food Service Strategies to Improve Food Intakes among Inpatients: A Systematic Review. Nutrients. 2021; 13(10):3649. https://doi.org/10.3390/nu13103649
Chicago/Turabian StyleOsman, Noor Suzana, Norazmir Md Nor, Mohd Shazali Md Sharif, Syahrul Bariah Abdul Hamid, and Syafiqah Rahamat. 2021. "Hospital Food Service Strategies to Improve Food Intakes among Inpatients: A Systematic Review" Nutrients 13, no. 10: 3649. https://doi.org/10.3390/nu13103649
APA StyleOsman, N. S., Md Nor, N., Md Sharif, M. S., Hamid, S. B. A., & Rahamat, S. (2021). Hospital Food Service Strategies to Improve Food Intakes among Inpatients: A Systematic Review. Nutrients, 13(10), 3649. https://doi.org/10.3390/nu13103649