
Lower Interstitial Glucose Concentrations but Higher Glucose Variability during Low-Energy Diet Compared to Regular Diet—An Observational Study in Females with Obesity

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
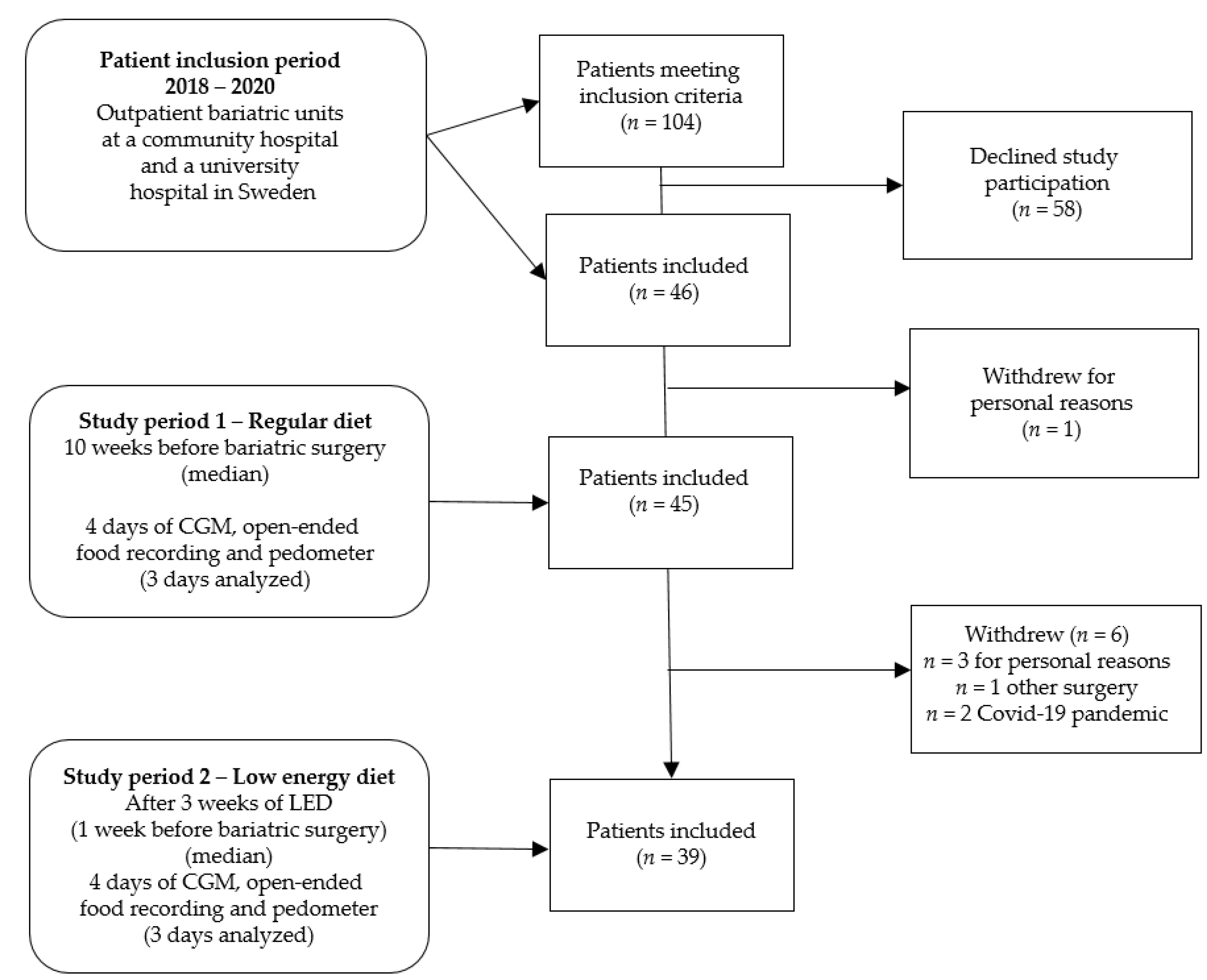
2.1. Study Design and Participants
2.2. Continuous Glucose Monitoring
2.3. Dietary Intake and Dietary Methods
2.4. Physical Activity
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
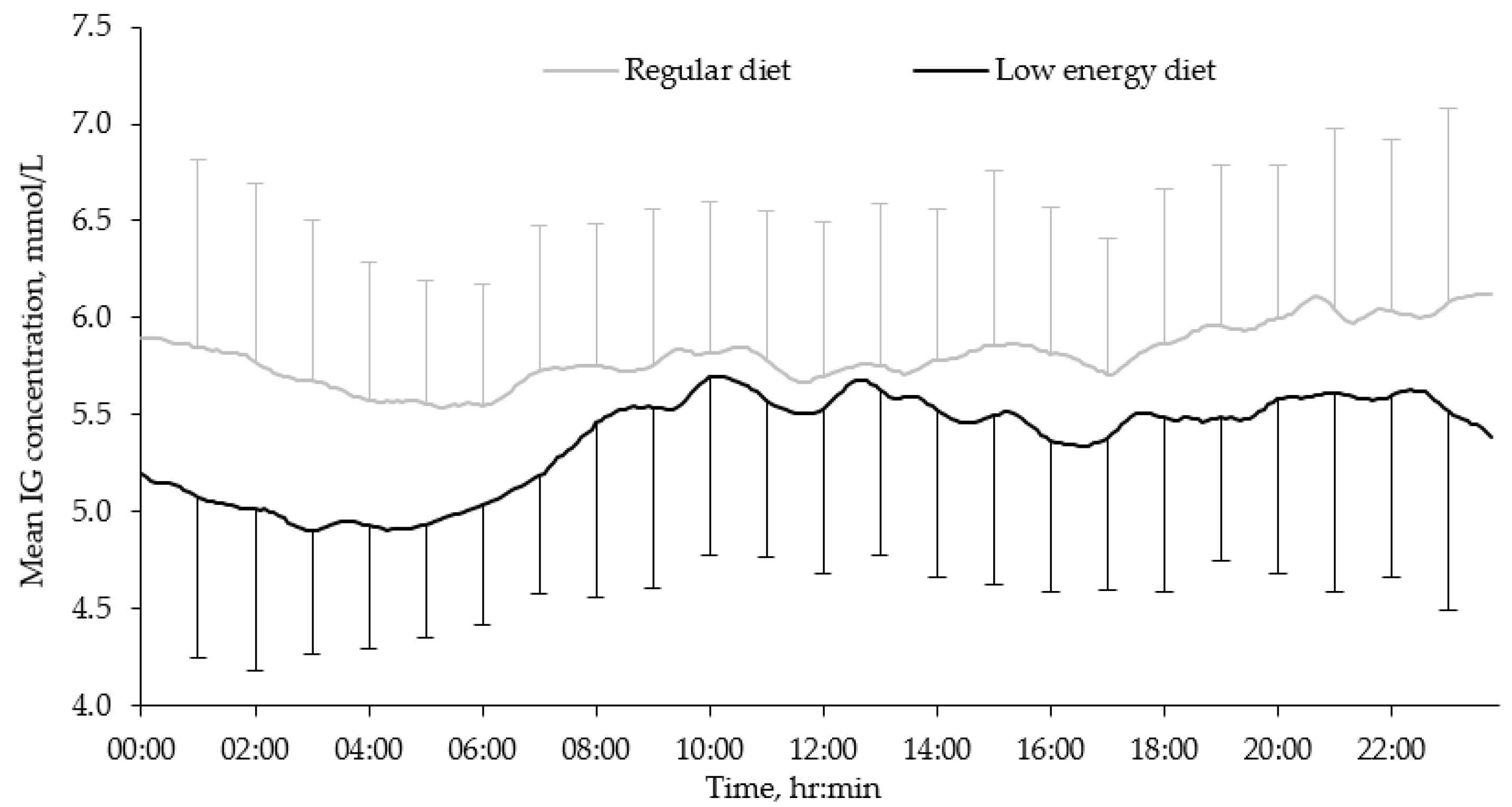
3.2. Diurnal IG Concentrations
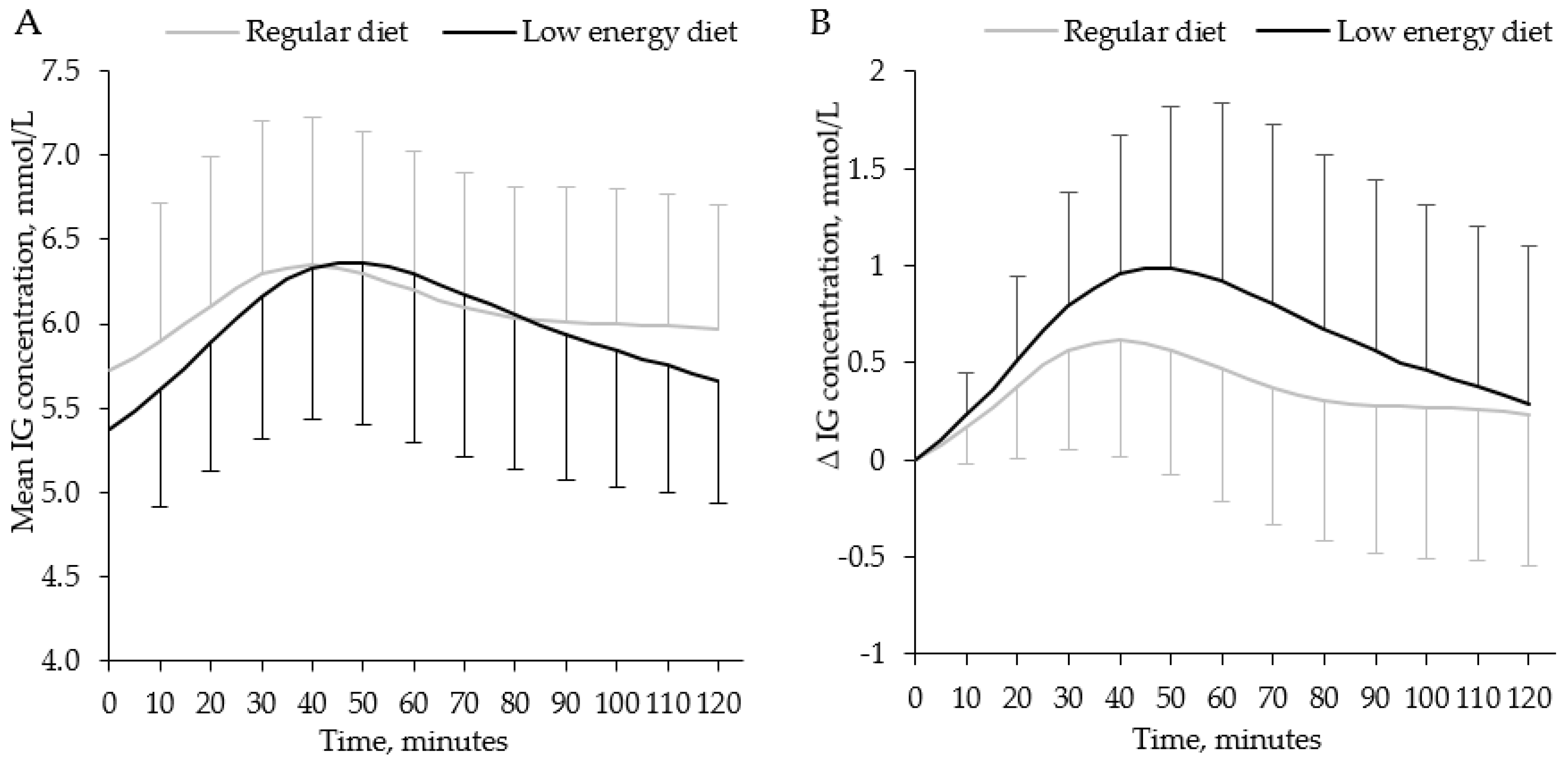
3.3. Breakfast IG Concentrations
3.4. Dietary Intake and Physical Activity
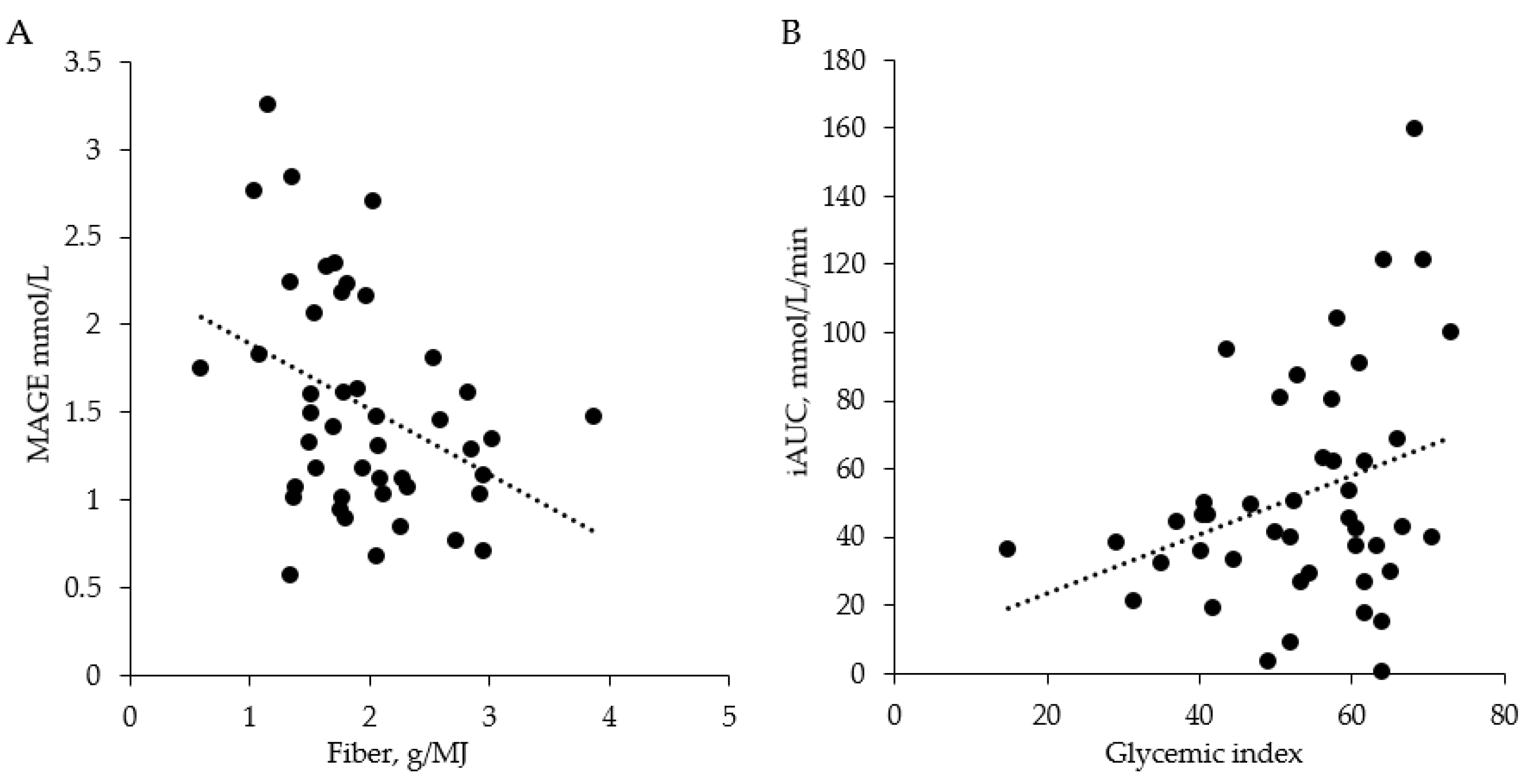
3.5. Independent Contributors to the Glycemic Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Null, N. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- Billeter, A.T.; Eichel, S.; Scheurlen, K.M.; Probst, P.; Kopf, S.; Müller-Stich, B.P. Meta-analysis of metabolic surgery versus medical treatment for macrovascular complications and mortality in patients with type 2 diabetes. Surg. Obes. Relat. Dis. 2019, 15, 1197–1210. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Peltonen, M.; Jacobson, P.; Ahlin, S.; Andersson-Assarsson, J.; Anveden, Å.; Bouchard, C.; Carlsson, B.; Karason, K.; Lönroth, H.; et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA 2014, 311, 2297–2304. [Google Scholar] [CrossRef] [Green Version]
- Cosentino, C.; Marchetti, C.; Monami, M.; Mannucci, E.; Cresci, B. Efficacy and effects of bariatric surgery in the treatment of obesity: Network meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2815–2824. [Google Scholar] [CrossRef] [PubMed]
- Golzarand, M.; Toolabi, K.; Farid, R. The bariatric surgery and weight losing: A meta-analysis in the long- and very long-term effects of laparoscopic adjustable gastric banding, laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy on weight loss in adults. Surg. Endosc. 2017, 31, 4331–4345. [Google Scholar] [CrossRef] [PubMed]
- Anderin, C.; Gustafsson, U.O.; Heijbel, N.; Thorell, A. Weight loss before bariatric surgery and postoperative complications. Ann. Surg. 2015, 261, 909–913. [Google Scholar] [CrossRef]
- Buscemi, S.; Cosentino, L.; Rosafio, G.; Morgana, M.; Mattina, A.; Sprini, D.; Verga, S.; Rini, G.B. Effects of hypocaloric diets with different glycemic indexes on endothelial function and glycemic variability in overweight and in obese adult patients at increased cardiovascular risk. Clin. Nutr. 2013, 32, 346–352. [Google Scholar] [CrossRef]
- Edholm, D.; Kullberg, J.; Karlsson, F.A.; Haenni, A.; Ahlström, H.; Sundbom, M. Changes in liver volume and body composition during 4 weeks of low calorie diet before laparoscopic gastric bypass. Surg. Obes. Relat. Dis. 2015, 11, 602–606. [Google Scholar] [CrossRef]
- Faria, S.L.; Faria, O.P.; Cardeal, M.D.A.; Ito, M.K. Effects of a very low calorie diet in the preoperative stage of bariatric surgery: A randomized trial. Surg. Obes. Relat. Dis. 2015, 11, 230–237. [Google Scholar] [CrossRef]
- Nielsen, L.V.; Nielsen, M.S.; Schmidt, J.B.; Pedersen, S.D.; Sjödin, A. Efficacy of a liquid low-energy formula diet in achieving preoperative target weight loss before bariatric surgery. J. Nutr. Sci. 2016, 5, e22. [Google Scholar] [CrossRef] [Green Version]
- Pournaras, D.J.; Nygren, J.; Toft, E.; Arner, P.; le Roux, C.W.; Thorell, A. Improved glucose metabolism after gastric bypass: Evolution of the paradigm. Surg. Obes. Relat. Dis. 2016, 12, 1457–1465. [Google Scholar] [CrossRef]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef]
- Schiavo, L.; Scalera, G.; Sergio, R.; De Sena, G.; Pilone, V.; Barbarisi, A. Clinical impact of Mediterranean-enriched-protein diet on liver size, visceral fat, fat mass, and fat-free mass in patients undergoing sleeve gastrectomy. Surg. Obes. Relat. Dis. 2015, 11, 1164–1170. [Google Scholar] [CrossRef]
- Augustin, L.; Kendall, C.; Jenkins, D.; Willett, W.; Astrup, A.; Barclay, A.; Björck, I.; Brand-Miller, J.; Brighenti, F.; Buyken, A.; et al. Glycemic index, glycemic load and glycemic response: An International Scientific Consensus Summit from the International Carbohydrate Quality Consortium (ICQC). Nutr. Metab. Cardiovasc. Dis. 2015, 25, 795–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary glycemic index and load and the risk of type 2 diabetes: Assessment of causal relations. Nutrients 2019, 11, 1436. [Google Scholar] [CrossRef] [Green Version]
- Alessa, H.B.; Bhupathiraju, S.N.; Malik, V.S.; Wedick, N.M.; Campos, H.; Rosner, B.; Willett, W.C.; Hu, F.B. Carbohydrate quality and quantity and risk of type 2 diabetes in US women. Am. J. Clin. Nutr. 2015, 102, 1543–1553. [Google Scholar] [CrossRef]
- Kim, D.-Y.; Kim, S.H.; Lim, H. Association between dietary carbohydrate quality and the prevalence of obesity and hypertension. J. Hum. Nutr. Diet. 2018, 31, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Fabricatore, A.N.; Ebbeling, C.B.; Wadden, T.A.; Ludwig, D.S. Continuous glucose monitoring to assess the ecologic validity of dietary glycemic index and glycemic load. Am. J. Clin. Nutr. 2011, 94, 1519–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annual Report Scandinavian Obesity Surgery Registry (SOReg). 2019. Available online: https://www.ucr.uu.se/soreg/ (accessed on 15 October 2021).
- Klonoff, D.C.; Ahn, D.; Drincic, A. Continuous glucose monitoring: A review of the technology and clinical use. Diabetes Res. Clin. Pr. 2017, 133, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Oliver, N.S.; Choudhary, P.; Levy, J.C.; Hindmarsh, P.; Matthews, D.R. Normal reference range for mean tissue glucose and glycemic variability derived from continuous glucose monitoring for subjects without diabetes in different ethnic groups. Diabetes Technol. Ther. 2011, 13, 921–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Sears, W.; Leblanc, S.; Drackley, J. Technical note: Comparison of 3 methods for analyzing areas under the curve for glucose and nonesterified fatty acids concentrations following epinephrine challenge in dairy cows. J. Dairy Sci. 2011, 94, 6111–6115. [Google Scholar] [CrossRef]
- Björck, I.; Elmståhl, H.L. The glycaemic index: Importance of dietary fibre and other food properties. Proc. Nutr. Soc. 2003, 62, 201–206. [Google Scholar] [CrossRef]
- Owens, D. Guideline for management of postmeal glucose in diabetes. Diabetes Res. Clin. Pr. 2014, 103, 256–268. [Google Scholar] [CrossRef]
- Seaquist, E.R.; Anderson, J.; Childs, B.; Cryer, P.; Dagogo-Jack, S.; Fish, L.; Heller, S.R.; Rodriguez, H.; Rosenzweig, J.; Vigersky, R. Hypoglycemia and diabetes: A report of a workgroup of the American Diabetes Association and The Endocrine Society. Diabetes Care 2013, 36, 1384–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, R.S. Principles of Nutritional Assessment, 2nd ed.; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Understanding meal patterns: Definitions, methodology and impact on nutrient intake and diet quality. Nutr. Res. Rev. 2015, 28, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, F.; Foster-Powell, K.; Brand-Miller, J. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Carbohydrates in Human Nutrition: Report of a Joint FAO/WHO Expert Consultation; FAO Food Nutrition Paper: Rome, Italy, 1998; pp. 1–140. [Google Scholar]
- Nordic Nutrition Recommendations. Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Amcoff, E.; Edberg, A.; Enghardt Barbieri, H.; Lindroos, A.K.; Nälsén, C.; Pearson, M.; Warensjö Lemming, E. Riksmaten—Vuxna 2010–11. Livsmedels–och Naringsintag Bland Vuxna i Sverige; Swedish Food Agency: Uppsala, Sweden, 2012. [Google Scholar]
- Modave, F.; Guo, Y.; Bian, J.; Gurka, M.J.; Parish, A.; Smith, M.D.; Lee, A.M.; Buford, T.W. Mobile device accuracy for step counting across age groups. JMIR mHealth uHealth 2017, 5, e88. [Google Scholar] [CrossRef]
- Barker, L.E.; Shaw, K.M. Best (but oft-forgotten) practices: Checking assumptions concerning regression residuals. Am. J. Clin. Nutr. 2015, 102, 533–539. [Google Scholar] [CrossRef] [Green Version]
- Campos, G.M.; Rabl, C.; Peeva, S.; Ciovica, R.; Rao, M.; Schwarz, J.-M.; Havel, P.; Schambelan, M.; Mulligan, K. Improvement in peripheral glucose uptake after gastric bypass surgery is observed only after substantial weight loss has occurred and correlates with the magnitude of weight lost. J. Gastrointest. Surg. 2009, 14, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Li, S.; Wang, Y.; Wang, M.; Yin, Q.; Mu, P.; Lin, S.; Qian, X.; Ye, X.; Chen, Y. Glycemic variability evaluated by continuous glucose monitoring system is associated with the 10-y cardiovascular risk of diabetic patients with well-controlled HbA1c. Clin. Chim. Acta 2016, 461, 146–150. [Google Scholar] [CrossRef]
- Xia, J.; Yin, C. Glucose variability and coronary artery disease. Hear. Lung Circ. 2019, 28, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Peters, H.P.F.; Ravestein, P.; Van Der Hijden, H.T.W.M.; Boers, H.M.; Mela, D. Effect of carbohydrate digestibility on appetite and its relationship to postprandial blood glucose and insulin levels. Eur. J. Clin. Nutr. 2010, 65, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrolix, R.; Mensink, R.P. Variability of the glycemic response to single food products in healthy subjects. Contemp. Clin. Trials 2010, 31, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.G.; Christian, P.E.; Coleman, R.E. Gastric emptying of varying meal weight and composition in man. Dig. Dis. Sci. 1981, 26, 16–22. [Google Scholar] [CrossRef]
- Okabe, T.; Terashima, H.; Sakamoto, A. Determinants of liquid gastric emptying: Comparisons between milk and isocalorically adjusted clear fluids. Br. J. Anaesth. 2015, 114, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anjana, R.M.; Gayathri, R.; Lakshmipriya, N.; Bai, M.R.; Shanmugam, S.; Unnikrishnan, R.; Krishnaswamy, K.; Henry, C.J.K.; Sudha, V.; Mohan, V. Effect of a novel high fiber rice diet on 24-hour glycemic responses in asian indians using continuous glucose monitoring: A randomized clinical trial. Diabetes Technol. Ther. 2019, 21, 177–182. [Google Scholar] [CrossRef]
- Behall, K.M.; Scholfield, D.J.; Hallfrisch, J.G.; Liljeberg-Elmståhl, H.G. Consumption of both resistant starch and -glucan improves postprandial plasma glucose and insulin in women. Diabetes Care 2006, 29, 976–981. [Google Scholar] [CrossRef]
- Festi, D.; Schiumerini, R.; Eusebi, L.H.; Marasco, G.; Taddia, M.; Colecchia, A. Gut microbiota and metabolic syndrome. World J. Gastroenterol. 2014, 20, 16079–16094. [Google Scholar] [CrossRef]
- Ashley, J.M.; Jarvis, W.T. Position of the American Dietetic Association: Health implications of dietary fiber. J. Am. Diet. Assoc. 2008, 108, 1716–1731. [Google Scholar] [CrossRef]
- Kochan, A.M.; Wolever, T.M.S.; Chetty, V.T.; Anand, S.S.; Gerstein, H.C.; Sharma, A.M. Glycemic index predicts individual glucose responses after self-selected breakfasts in free-living, abdominally obese adults. J. Nutr. 2011, 142, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Lagerpusch, M.; Enderle, J.; Later, W.; Eggeling, B.; Pape, D.; Müller, M.J.; Bosy-Westphal, A. Impact of glycaemic index and dietary fibre on insulin sensitivity during the refeeding phase of a weight cycle in young healthy men. Br. J. Nutr. 2012, 109, 1606–1616. [Google Scholar] [CrossRef] [Green Version]
- Hill, R.; Davies, P.S.W. The validity of self-reported energy intake as determined using the doubly labelled water technique. Br. J. Nutr. 2001, 85, 415–430. [Google Scholar] [CrossRef] [Green Version]
- Wehling, H.; Lusher, J. People with a body mass index ≥30 under-report their dietary intake: A systematic review. J. Health Psychol. 2017, 24, 2042–2059. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Age 2, y | 37 (17) |
| Body weight, kg | 122.5 ± 20.3 |
| BMI, kg/m2 | 43.6 ± 6.2 |
| Fasting P-glucose, mmol/L | 5.7 ± 0.5 |
| B-HbA1c, mmol/mol | 36.6 ± 4.0 |
| Fasting S-insulin, mE/L | 25.8 ± 1.5 |
| Regular Diet | LED | p | |
|---|---|---|---|
| 24 h mean glucose, mmol/L | 5.8 ± 0.5 | 5.4 ± 0.5 | <0.001 |
| 24 h MAGE, mmol/L | 1.5 ± 0.7 | 1.7 ± 0.7 | 0.031 |
| Glucose 2 ≥ 7.8 mmol/L | 38 (33%) | 31 (27%) | 0.229 |
| Glucose 2 ≤ 3.9 mmol/L | 10 (9%) | 25 (22%) | 0.011 |
| MAGE 2 ≥ 2.8 mmol/L | 5 (4%) | 8 (7%) | 0.581 |
| Regular Diet | LED | p | |
|---|---|---|---|
| Mean of 0–120 min glucose, mmol/L | 6.1 ± 0.7 | 6.0 ± 0.7 | 0.209 |
| Mean glucose at 0 min, mmol/L | 5.7 ± 0.8 | 5.4 ± 0.6 | <0.001 |
| Mean glucose at 120 min, mmol/L | 6.0 ± 0.7 | 5.7 ± 0.7 | <0.001 |
| 120 min positive iAUC 2, mmol/L/min | 43.5 (43.6) | 77.8 (62.4) | <0.001 |
| Glucose 3 ≥ 7.8 mmol/L | 13 (12%) | 16 (14%) | 0.648 |
| Glucose 3 ≤ 3.9 mmol/L | 0 | 0 | - |
| Regular Diet | LED | p | |
|---|---|---|---|
| Daily intake: | |||
| Energy, kcal | 2069 ± 688 | 827 ± 197 | <0.001 |
| Carbohydrate, g | 195.3 ± 7.0 | 98.5 ± 24.7 | <0.001 |
| Fiber, g | 16.1 ± 6.1 | 16.5 ± 4.9 | 0.583 |
| Fat, g | 97.9 ± 42.0 | 19.4 ± 9.2 | <0.001 |
| Protein, g | 79.7 ± 24.3 | 56.6 ± 11.1 | <0.001 |
| Alcohol, g | 7.6 ± 18.7 | 0.0 | <0.001 |
| Days on LED 2 | - | 21 (2) | - |
| Breakfast intake: | |||
| Breakfast time 2, h:min | 8:30 (2:45) | 9:00 (2:00) | 0.006 |
| Energy, kcal | 401 ± 198 | 218 ± 26 | <0.001 |
| Carbohydrates, g | 42.2 ± 21.7 | 26.4 ± 5.2 | <0.001 |
| Fiber, g | 3.8 ± 2.6 | 4.2 ± 1.2 | 0.088 |
| Fat, g | 17.6 ± 11.5 | 4.9 ± 1.3 | <0.001 |
| Proteins, g | 16.9 ± 8.9 | 14.8 ± 3.0 | 0.026 |
| GI 3 | 53 ± 15 | - | <0.001 |
| Simple Linear Regression of 24 h Glycemic Response | Multiple Linear Regression of 24 h Glycemic Response | ||||||
|---|---|---|---|---|---|---|---|
| Mean Glucose, mmol/L | MAGE, mmol/L | MAGE, mmol/L | |||||
| β | P | β | P | β | P | 95% CI | |
| Age, y | 0.01 | 0.103 | 0.00 | 0.938 | |||
| BMI, kg/m2 | −0.00 | 0.724 | 0.02 | 0.303 | |||
| Carbohydrate, g/MJ | 0.01 | 0.500 | 0.01 | 0.634 | |||
| Fiber, g/MJ | −0.21 | 0.064 | −0.37 | 0.011 | −0.31 | 0.032 | −0.59, −0.03 |
| Protein, g/MJ | −0.05 | 0.321 | −0.15 | 0.017 | −0.12 | 0.052 | −0.24, 0.00 |
| Fat, g/MJ | −0.02 | 0.722 | 0.04 | 0.546 | |||
| Step Counts | 0.00 | 0.159 | 0.00 | 0.766 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilsen, I.; Andersson, A.; Laurenius, A.; Osterberg, J.; Sundbom, M.; Haenni, A. Lower Interstitial Glucose Concentrations but Higher Glucose Variability during Low-Energy Diet Compared to Regular Diet—An Observational Study in Females with Obesity. Nutrients 2021, 13, 3687. https://doi.org/10.3390/nu13113687
Nilsen I, Andersson A, Laurenius A, Osterberg J, Sundbom M, Haenni A. Lower Interstitial Glucose Concentrations but Higher Glucose Variability during Low-Energy Diet Compared to Regular Diet—An Observational Study in Females with Obesity. Nutrients. 2021; 13(11):3687. https://doi.org/10.3390/nu13113687
Chicago/Turabian StyleNilsen, Inger, Agneta Andersson, Anna Laurenius, Johanna Osterberg, Magnus Sundbom, and Arvo Haenni. 2021. "Lower Interstitial Glucose Concentrations but Higher Glucose Variability during Low-Energy Diet Compared to Regular Diet—An Observational Study in Females with Obesity" Nutrients 13, no. 11: 3687. https://doi.org/10.3390/nu13113687
APA StyleNilsen, I., Andersson, A., Laurenius, A., Osterberg, J., Sundbom, M., & Haenni, A. (2021). Lower Interstitial Glucose Concentrations but Higher Glucose Variability during Low-Energy Diet Compared to Regular Diet—An Observational Study in Females with Obesity. Nutrients, 13(11), 3687. https://doi.org/10.3390/nu13113687