
Adherence to the Planetary Health Diet Index and Obesity Indicators in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
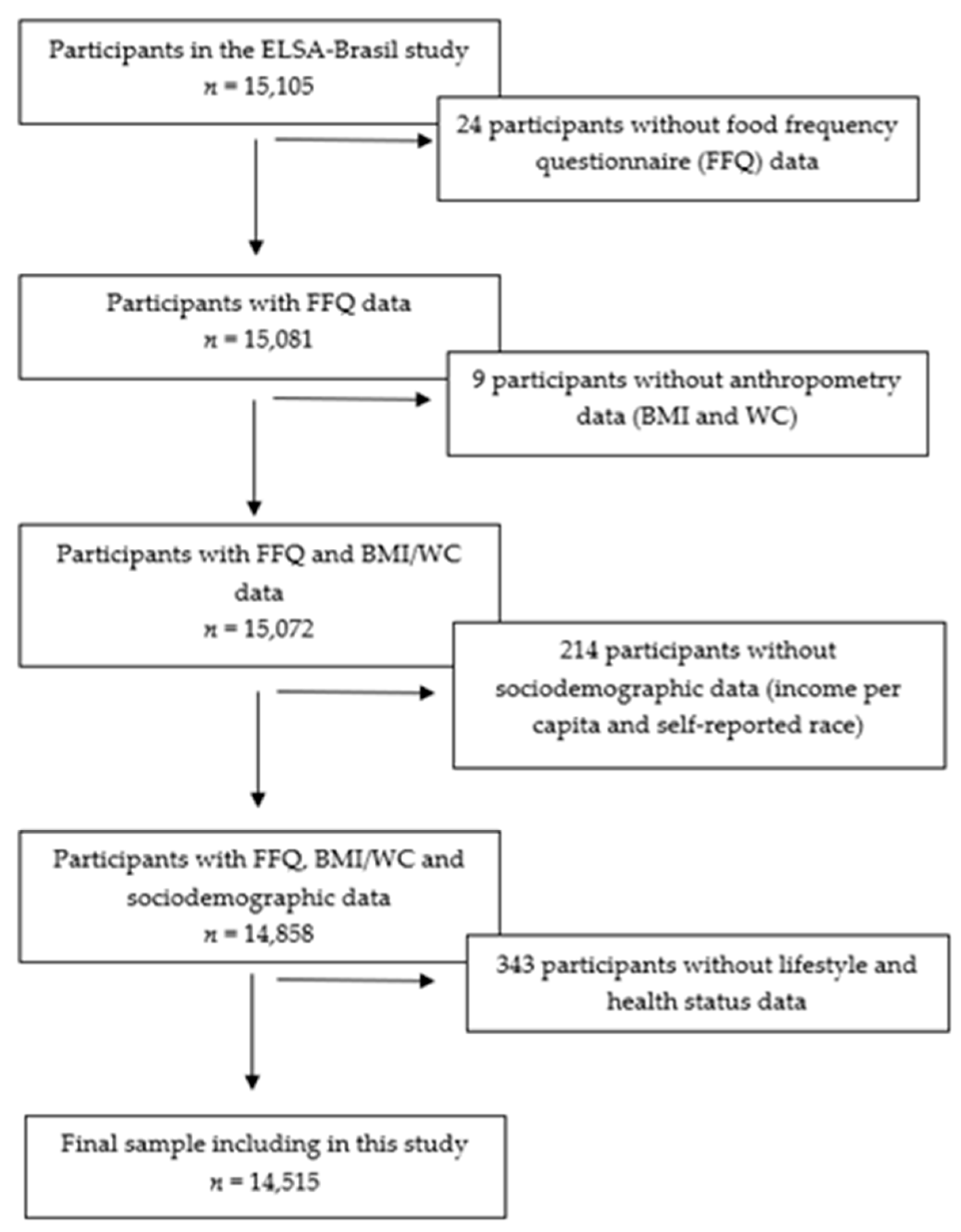
2.1. Study Design
2.2. Diet Assessment
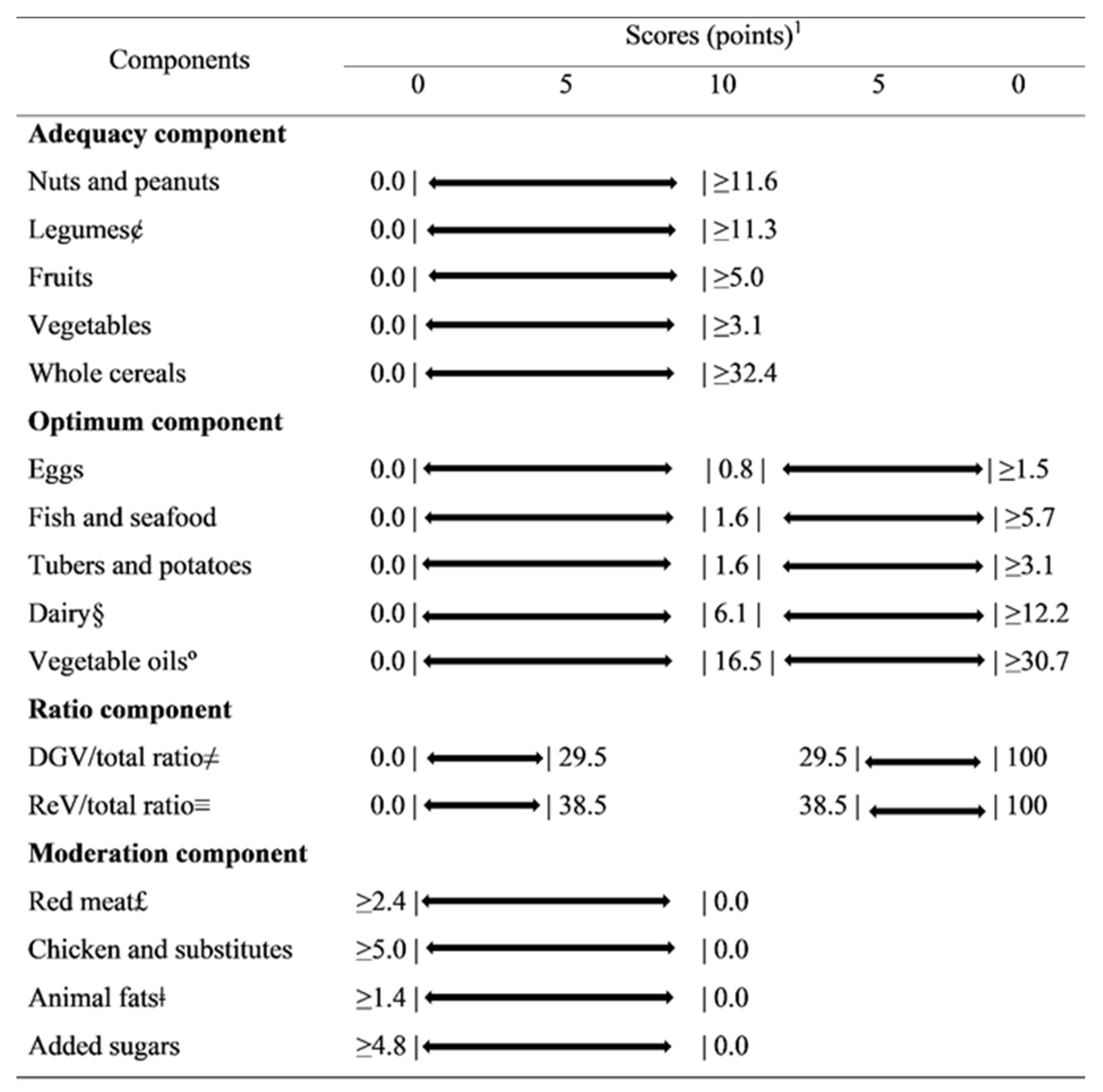
2.3. Planetary Health Diet Index
2.4. Outcome’s Assessment
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Springmann, M.; Afshin, A.; Rivera, J.A.; Wang, D.D.; Willett, W. The Benefits of the EAT-Lancet Commission’s Dietary Recommendations Are Significant and Robust. J. Nutr. 2020, 150, 2837–2838. [Google Scholar] [CrossRef] [PubMed]
- Tucci, M.; Martini, D.; Del Bo, C.; Marino, M.; Battezzati, A.; Bertoli, S.; Porrini, M.; Riso, P. An Italian-Mediterranean Dietary Pattern Developed Based on the EAT-Lancet Reference Diet (EAT-IT): A Nutritional Evaluation. Foods 2021, 10, 558. [Google Scholar] [CrossRef]
- Lassen, A.D.; Christensen, L.M.; Trolle, E. Development of a Danish Adapted Healthy Plant-Based Diet Based on the EAT-Lancet Reference Diet. Nutrients 2020, 12, 738. [Google Scholar] [CrossRef] [Green Version]
- Blackstone, N.T.; Conrad, Z. Comparing the Recommended Eating Patterns of the EAT-Lancet Commission and Dietary Guidelines for Americans: Implications for Sustainable Nutrition. Curr. Dev. Nutr. 2020, 4, nzaa015. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Kishore, A.; Roy, D.; Joshi, K. A comparison of the Indian diet with the EAT-Lancet reference diet. BMC Public Health 2020, 20, 812. [Google Scholar] [CrossRef]
- Drewnowski, A. Analysing the affordability of the EAT-Lancet diet. Lancet. Glob. Health 2020, 8, e6–e7. [Google Scholar] [CrossRef]
- Hirvonen, K.; Bai, Y.; Headey, D.; Masters, W.A. Affordability of the EAT-Lancet reference diet: A global analysis. Lancet. Glob. Health 2020, 8, e59–e66. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; de Pee, S.; Kim, B.; McKenzie, S.; Nachman, K.; Bloem, M.W. Adoption of the ‘planetary health diet’ has different impacts on countries’ greenhouse gas emissions. Nat. Food 2020, 1, 481–484. [Google Scholar] [CrossRef]
- Knuppel, A.; Papier, K.; Key, T.J.; Travis, R.C. EAT-Lancet score and major health outcomes: The EPIC-Oxford study. Lancet 2019, 394, 213–214. [Google Scholar] [CrossRef] [Green Version]
- Harcombe, Z. This is not the EAT-Lancet Diet. Lancet 2020, 395, 271–272. [Google Scholar] [CrossRef] [Green Version]
- Cacau, L.T.; De Carli, E.; de Carvalho, A.M.; Lotufo, P.A.; Moreno, L.A.; Bensenor, I.M.; Marchioni, D.M. Development and Validation of an Index Based on EAT-Lancet Recommendations: The Planetary Health Diet Index. Nutrients 2021, 13, 1698. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metab. Clin. Exp. 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Singh, G.M.; Danaei, G.; Farzadfar, F.; Stevens, G.A.; Woodward, M.; Wormser, D.; Kaptoge, S.; Whitlock, G.; Qiao, Q.; Lewington, S.; et al. The age-specific quantitative effects of metabolic risk factors on cardiovascular diseases and diabetes: A pooled analysis. PLoS ONE 2013, 8, e65174. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. New Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Bensenor, I.M.; Griep, R.H.; Pinto, K.A.; Faria, C.P.d.; Felisbino-Mendes, M.; Caetano, E.I.; Albuquerque, L.d.S.; Schmidt, M.I. Rotinas de organização de exames e entrevistas no centro de investigação ELSA-Brasil. Rev. De Saude Publica 2013, 47, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.I.; Duncan, B.B.; Mill, J.G.; Lotufo, P.A.; Chor, D.; Barreto, S.M.; Aquino, E.M.; Passos, V.M.A.; Matos, S.M.; Molina, M.d.C.B.; et al. Cohort Profile: Longitudinal Study of Adult Health (ELSA-Brasil). Int. J. Epidemiol. 2014, 44, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aquino, E.M.; Barreto, S.M.; Bensenor, I.M.; Carvalho, M.S.; Chor, D.; Duncan, B.B.; Lotufo, P.A.; Mill, J.G.; Molina Mdel, C.; Mota, E.L.; et al. Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Objectives and design. Am. J. Epidemiol. 2012, 175, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Mill, J.G.; Pinto, K.; Griep, R.H.; Goulart, A.; Foppa, M.; Lotufo, P.A.; Maestri, M.K.; Ribeiro, A.L.; Andreão, R.V.; Dantas, E.M.; et al. Aferições e exames clínicos realizados nos participantes do ELSA-Brasil. Rev. De Saude Publica 2013, 47, 54–62. [Google Scholar] [CrossRef]
- Molina, M.d.C.B.; Benseñor, I.M.; Cardoso, L.d.O.; Velasquez-Melendez, G.; Drehmer, M.; Pereira, T.S.S.; Faria, C.P.d.; Melere, C.; Manato, L.; Gomes, A.L.C.; et al. Reprodutibilidade e validade relativa do Questionário de Frequência Alimentar do ELSA-Brasil. Cad. De Saúde Pública 2013, 29, 379–389. [Google Scholar] [CrossRef]
- Molina, M.d.C.B.; Faria, C.P.d.; Cardoso, L.d.O.; Drehmer, M.; Velasquez-Meléndez, J.G.; Gomes, A.L.C.; Melere, C.; Diniz, M.d.F.H.S.; Sichieri, R.; Benseñor, I.J.M. Diet assessment in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Development of a food frequency questionnaire. Rev. De Nutr. 2013, 26, 167–176. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation on Obesity, Geneva, 3–5 June 1997; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Piccinelli, M.; Tessari, E.; Bortolomasi, M.; Piasere, O.; Semenzin, M.; Garzotto, N.; Tansella, M. Efficacy of the alcohol use disorders identification test as a screening tool for hazardous alcohol intake and related disorders in primary care: A validity study. BMJ 1997, 314, 420–424. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Shamah-Levy, T.; Gaona-Pineda, E.B.; Mundo-Rosas, V.; Méndez Gómez-Humarán, I.; Rodríguez-Ramírez, S. Asociación de un índice de dieta saludable y sostenible con sobrepeso y obesidad en adultos mexicanos. Salud Pública México 2020, 62, 745–753. [Google Scholar] [CrossRef]
- Burggraf, C.; Teuber, R.; Brosig, S.; Meier, T. Review of a priori dietary quality indices in relation to their construction criteria. Nutr. Rev. 2018, 76, 747–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seconda, L.; Egnell, M.; Julia, C.; Touvier, M.; Hercberg, S.; Pointereau, P.; Lairon, D.; Allès, B.; Kesse-Guyot, E. Association between sustainable dietary patterns and body weight, overweight, and obesity risk in the NutriNet-Santé prospective cohort. Am. J. Clin. Nutr. 2020, 112, 138–149. [Google Scholar] [CrossRef]
- Burlingame, B.; Dernini, S. Sustainable diets: The Mediterranean diet as an example. Public Health Nutr. 2011, 14, 2285–2287. [Google Scholar] [CrossRef] [Green Version]
- Dernini, S.; Berry, E.M.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.X.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Germani, A.; Vitiello, V.; Giusti, A.M.; Pinto, A.; Donini, L.M.; del Balzo, V. Environmental and economic sustainability of the Mediterranean Diet. Int. J. Food Sci. Nutr. 2014, 65, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Hamm, M.W.; Hu, F.B.; Abrams, S.A.; Griffin, T.S. Alignment of Healthy Dietary Patterns and Environmental Sustainability: A Systematic Review. Adv. Nutr. 2016, 7, 1005–1025. [Google Scholar] [CrossRef] [Green Version]
- Shatwan, I.M.; Alhinai, E.A.; Alawadhi, B.; Surendran, S.; Aljefree, N.M.; Almoraie, N.M. High Adherence to the Mediterranean Diet Is Associated with a Reduced Risk of Obesity among Adults in Gulf Countries. Nutrients 2021, 13, 995. [Google Scholar] [CrossRef] [PubMed]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients 2019, 11, 1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, S.; Shirani, F.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) diet on weight and body composition in adults: A systematic review and meta-analysis of randomized controlled clinical trials. Obes. Rev. 2016, 17, 442–454. [Google Scholar] [CrossRef]
- Fresán, U.; Sabaté, J. Vegetarian Diets: Planetary Health and Its Alignment with Human Health. Adv. Nutr. 2019, 10, S380–S388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.B.; Shivappa, N.; Hébert, J.R.; Page, A.J.; Gill, T.K.; Melaku, Y.A. Association between Dietary Inflammatory Index, Dietary Patterns, Plant-Based Dietary Index and the Risk of Obesity. Nutrients 2021, 13, 1536. [Google Scholar] [CrossRef]
- Carvalho, A.M.d.; César, C.L.G.; Fisberg, R.M.; Marchioni, D.M.L. Excessive meat consumption in Brazil: Diet quality and environmental impacts. Public Health Nutr. 2012, 16, 1893–1899. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, A.M.d.; Selem, S.S.a.d.C.; Miranda, A.M.; Marchioni, D.M. Excessive red and processed meat intake: Relations with health and environment in Brazil. Br. J. Nutr. 2016, 115, 2011–2016. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Planetary Health Diet Index | ||||||
|---|---|---|---|---|---|---|
| 1st | 2th | 3th | 4th | 5th | p-Value | |
| n (mean) | 2898 (44.7) | 2913 (53.8) | 2904 (59.9) | 2889 (66.2) | 2911 (76.8) | |
| Age group, n (%) | <0.001 | |||||
| Adults | 2328 (80.3) | 2345 (80.5) | 2307 (79.4) | 2280 (78.9) | 2134 (73.3) | |
| Elderly | 570 (19.7) | 568 (19.5) | 597 (20.6) | 609 (21.8) | 777 (26.7) | |
| Sex, n (%) | 0.223 | |||||
| Men | 1344 (46.4) | 1332 (45.7) | 1305 (44.9) | 1337 (46.3) | 1274 (43.8) | |
| Woman | 1554 (53.6) | 1581 (54.3) | 1599 (55.1) | 1552 (53.7 | 1637 (56.2) | |
| Self-reported race, n (%) | <0.001 | |||||
| White | 1421 (49.0) | 1452 (49.9) | 1540 (53.0) | 1545 (53.5) | 1587 (54.5) | |
| Brown | 902 (31.1) | 864 (29.7) | 806 (27.8) | 787 (27.7) | 739 (25.4) | |
| Black | 477 (16.5) | 500 (17.2) | 463 (15.9) | 454 (15.7) | 464 (15.9) | |
| Other | 98 (3.4) | 97 (3.3) | 95 (3.3) | 103 (3.6) | 121 (4.2) | |
| Per capita income, n (%) | <0.001 | |||||
| Low | 1126 (38.9) | 1123 (38.6) | 1125 (38.7) | 1067 (36.9) | 924 (31.7) | |
| Medium | 972 (33.5) | 1027 (35.3) | 956 (32.9) | 992 (34.3) | 1031 (35.4) | |
| High | 800 (27.6) | 763 (26.2) | 823 (28.3) | 830 (28.7) | 956 (32.8) | |
| Smoking, n (%) | <0.001 | |||||
| Never | 2442 (84.3) | 2533 (87.0) | 2521 (86.8) | 2555 (88.4) | 2577 (88.5) | |
| Current | 456 (15.7) | 380 (13.0) | 383 (13.2) | 334 (11.6) | 334 (11.5) | |
| Excessive alcohol consumption, n (%) | 0.002 | |||||
| No | 2493 (86.0) | 2505 (86.0) | 2534 (86.9) | 2485 (86.0) | 2587 (88.9) | |
| Yes | 405 (14.0) | 408 (14.0) | 380 (13.1) | 404 (14.0) | 324 (11.1) | |
| Physical activity, n (%) | <0.001 | |||||
| Low | 2353 (81.2) | 2302 (79.0) | 2258 (77.8) | 2200 (76.2) | 2059 (70.7) | |
| Moderate | 320 (11.0) | 359 (12.3) | 387 (13.3) | 424 (14.7) | 523 (18.0) | |
| Vigorous | 225 (7.8) | 252 (8.7) | 259 (8.9) | 265 (9.2) | 329 (11.3) | |
| Diabetes type 2, n (%) | <0.001 | |||||
| No | 2505 (86.4) | 2467 (84.7) | 2454 (84.5) | 2359 (81.7) | 2248 (77.2) | |
| Yes | 393 (13.6) | 446 (15.3) | 450 (15.5) | 530 (18.4) | 663 (22.8) | |
| Hypertension, n (%) | 0.009 | |||||
| No | 1891 (65.3) | 1906 (65.4) | 1914 (65.9) | 1839 (65.7) | 1794 (61.6) | |
| Yes | 1007 (34.8) | 1007 (34.6) | 990 (34.1) | 1050 (36.3) | 1117 (38.4) | |
| Dyslipidemia, n (%) | 0.694 | |||||
| No | 1235 (42.6) | 1253 (43.0) | 1198 (41.2) | 1217 (42.1) | 1219 (41.9) | |
| Yes | 1663 (57.4) | 1660 (57.0) | 1706 (58.8) | 1672 (57.9) | 1692 (58.1) | |
| BMI (kg/m2), mean (sd) | 27.1 (4.7) | 27.0 (4.8) | 26.9 (4.7) | 27.2 (4.8) | 26.8 (4.7) | <0.001 |
| WC (cm), mean (sd) | 91.7 (12.7) | 91.3 (12.7) | 90.7 (12.7) | 91.4 (12.9) | 90.6 (12.7) | <0.001 |
| Energy intake (kcal), mean (sd) | 1954.4 (755.6) | 1971.7 (718.4) | 1948.4 (702.1) | 1936.7 (670.4) | 1859.7 (607.7) | <0.001 |
| BMI status, n (%) | 0.002 | |||||
| Adequate | 1013 (35.0) | 1085 (37.3) | 1097 (37.8) | 1020 (35.3) | 1152 (39.6) | |
| Overweight | 1243 (42.9) | 1143 (39.2) | 1134 (39.1) | 1190 (41.2) | 1129 (38.8) | |
| Obesity | 642 (22.2) | 685 (23.5) | 673 (23.2) | 679 (23.5) | 630 (21.6) | |
| Abdominal obesity, n (%) | 0.050 | |||||
| Adequate | 1036 (35.8) | 1081 (37.1) | 1111 (38.3) | 1063 (36.8) | 1097 (37.7) | |
| Increased abdominal obesity | 803 (27.7) | 730 (25.1) | 749 (25.7) | 756 (26.2) | 805 (27.7) | |
| Substantially increased abdominal obesity | 1058 (36.5) | 1101 (37.8) | 1044 (36.0) | 1068 (37.0) | 1008 (34.6) | |
| Planetary Health Diet Index | |||||||
|---|---|---|---|---|---|---|---|
| Quintiles | Continuous (10-Point Increase in the Total Score) | ||||||
| 1st | 2th | 3th | 4th | 5th | p for Trend | ||
| β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | |||
| BMI (kg/m2) | |||||||
| Model age-adjusted £ | ref | −0.06 (−0.30:0.17) | −0.22 (−0.46:0.02) | 0.04 (−0.20:0.28) | −0.42 (−0.66:−0.18) | 0.007 | −0.12 (−0.19:−0.06) |
| Model fully adjusted § | ref | −0.11 (−0.34:0.12) | −0.25 (−0.48:−0.02) | −0.04 (−0.27:0.19) | −0.50 (−0.73:−0.27) | <0.001 | −0.15 (−0.21:−0.08) |
| WC (cm) | |||||||
| Model age-adjusted £ | ref | −0.40 (−1.04:0.24) | −1.13 (-1.77:−0.49) | −0.54 (−1.18:0.09) | −1.72 (−2.37:−1.09) | <0.001 | −0.52 (−0.70:−0.35) |
| Model fully adjusted § | ref | −0.44 (−1.02:0.14) | −1.10 (−1.68:−0.53) | −0.76 (−0.134:−0.18) | −1.70 (−2.28:−1.12) | <0.001 | −0.52 (−0.68:−0.36) |
| Overweight * | Obesity * | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Model age-adjusted £ | ||||
| PHDI quintiles | ||||
| 1st quintile | ref | ref | ||
| 2th quintile | 0.86 | 0.77:0.97 | 1.00 | 0.87:1.14 |
| 3th quintile | 0.85 | 0.76:0.95 | 0.95 | 0.83:1.09 |
| 4th quintile | 0.93 | 0.83:1.05 | 1.02 | 0.89:1.17 |
| 5th quintile | 0.76 | 0.68:0.86 | 0.82 | 0.72:0.94 |
| p for trend | <0.001 | <0.05 | ||
| Continuous (10 points increase in the total score) | 0.94 | 0.91:0.97 | 0.94 | 0.91:0.98 |
| Model fully adjusted § | ||||
| PHDI quintiles | ||||
| 1st quintile | ref | ref | ||
| 2th quintile | 0.85 | 0.76:0.96 | 0.97 | 0.84:1.13 |
| 3th quintile | 0.84 | 0.75:0.95 | 0.95 | 0.82:1.10 |
| 4th quintile | 0.92 | 0.82:1.04 | 0.97 | 0.84:1.13 |
| 5th quintile | 0.76 | 0.67:0.85 | 0.76 | 0.65:0.88 |
| p for trend | <0.001 | <0.001 | ||
| Continuous (10 points increase in the total score) | 0.93 | 0.90:0.97 | 0.92 | 0.88:0.96 |
| Increased Abdominal Obesity * | Substantially Increased Abdominal Obesity * | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Model age-adjusted £ | ||||
| PHDI quintiles | ||||
| 1st quintile | ref | ref | ||
| 2th quintile | 0.86 | 0.75:0.97 | 0.99 | 0.87:1.11 |
| 3th quintile | 0.85 | 0.75:0.97 | 0.88 | 0.78:0.99 |
| 4th quintile | 0.89 | 0.78:1.01 | 0.93 | 0.82:1.04 |
| 5th quintile | 0.87 | 0.76:0.99 | 0.80 | 0.71:0.90 |
| p for trend | 0.095 | <0.001 | ||
| Continuous (10 points increase in the total score) | 0.96 | 0.93:0.99 | 0.93 | 0.90:0.97 |
| Model fully adjusted § | ||||
| PHDI quintiles | ||||
| 1st quintile | ref | ref | ||
| 2th quintile | 0.86 | 0.75:0.98 | 0.97 | 0.85:1.11 |
| 3th quintile | 0.84 | 0.74:0.96 | 0.86 | 0.75:0.98 |
| 4th quintile | 0.88 | 0.77:1.00 | 0.89 | 0.77:1.01 |
| 5th quintile | 0.86 | 0.75:0.98 | 0.73 | 0.64:0.83 |
| p for trend | 0.066 | <0.001 | ||
| Continuous (10 points increase in the total score) | 0.95 | 0.92:0.99 | 0.91 | 0.87:0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacau, L.T.; Benseñor, I.M.; Goulart, A.C.; Cardoso, L.O.; Lotufo, P.A.; Moreno, L.A.; Marchioni, D.M. Adherence to the Planetary Health Diet Index and Obesity Indicators in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Nutrients 2021, 13, 3691. https://doi.org/10.3390/nu13113691
Cacau LT, Benseñor IM, Goulart AC, Cardoso LO, Lotufo PA, Moreno LA, Marchioni DM. Adherence to the Planetary Health Diet Index and Obesity Indicators in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Nutrients. 2021; 13(11):3691. https://doi.org/10.3390/nu13113691
Chicago/Turabian StyleCacau, Leandro Teixeira, Isabela Martins Benseñor, Alessandra Carvalho Goulart, Leticia Oliveira Cardoso, Paulo Andrade Lotufo, Luis A. Moreno, and Dirce Maria Marchioni. 2021. "Adherence to the Planetary Health Diet Index and Obesity Indicators in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)" Nutrients 13, no. 11: 3691. https://doi.org/10.3390/nu13113691
APA StyleCacau, L. T., Benseñor, I. M., Goulart, A. C., Cardoso, L. O., Lotufo, P. A., Moreno, L. A., & Marchioni, D. M. (2021). Adherence to the Planetary Health Diet Index and Obesity Indicators in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Nutrients, 13(11), 3691. https://doi.org/10.3390/nu13113691