Dietary Micronutrients from Zygote to Senility: Updated Review of Minerals’ Role and Orchestration in Human Nutrition throughout Life Cycle with Sex Differences

 ,
,  ,
,
Abstract
:1. Introduction
Search Strategy
2. Selenium
2.1. Fertility and Perinatal Period
2.2. Childhood and Adolescents
2.3. Adulthood and the Elderly
3. Iodine
3.1. Fertility and Perinatal Period
3.2. Childhood and Adolescence
3.3. Adulthood and the Elderly
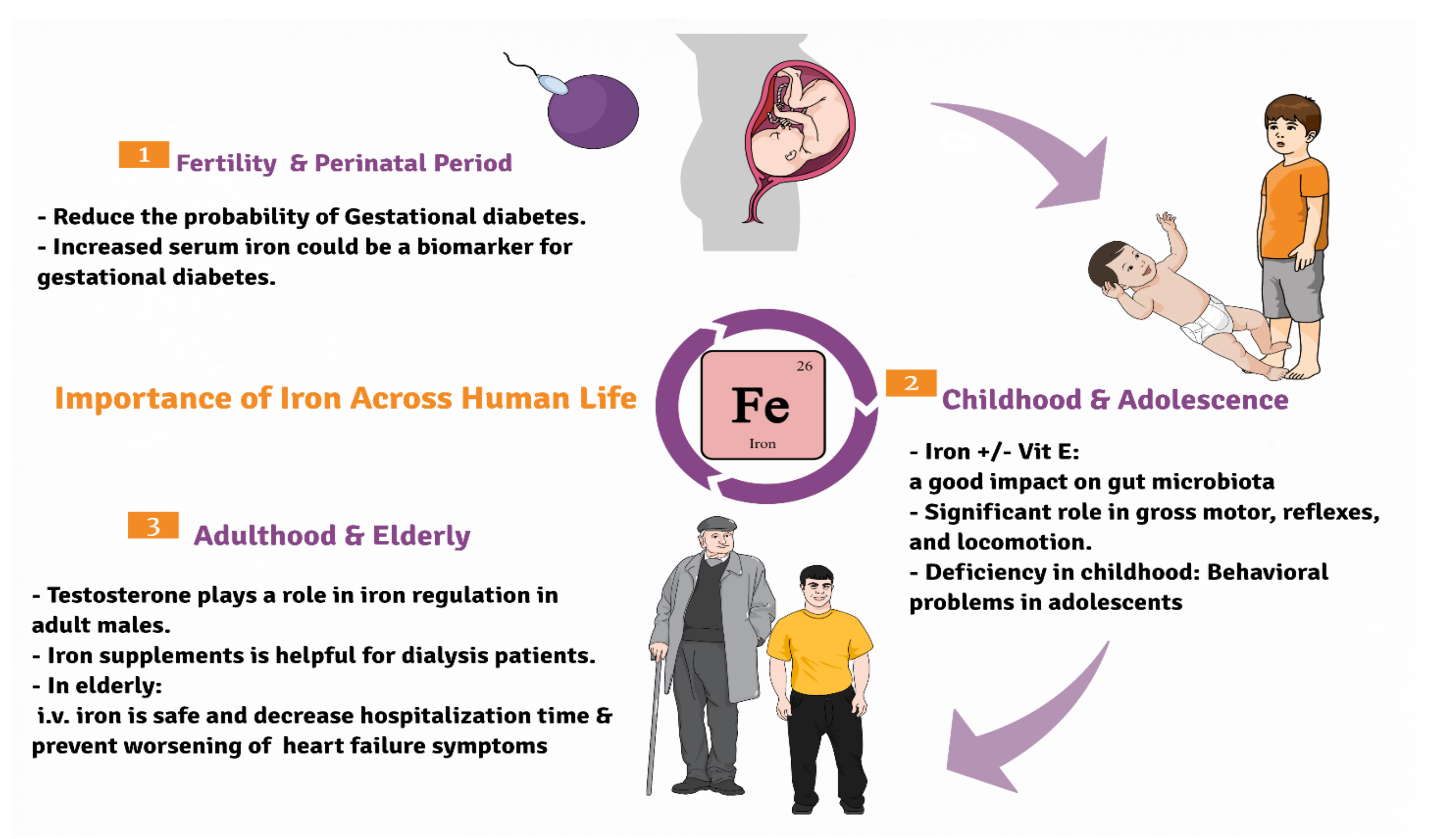
4. Iron
4.1. Fertility and Perinatal Period
4.2. Childhood and Adolescence
4.3. Adulthood and the Elderly
5. Cobalt
5.1. Fertility and Perinatal Period
5.2. Childhood and Adolescence
5.3. Adulthood and the Elderly
6. Fluoride
6.1. Fertility and Perinatal Period
6.2. Childhood and Adolescence
6.3. Adulthood and the Elderly
7. Zinc
7.1. Fertility and Pregnancy
7.2. Childhood and Adolescence
7.3. Adulthood and the Elderly
8. Manganese (Mn)
8.1. Fertility and Perinatal Period
8.2. Childhood and Adolescence
8.3. Adulthood and the Elderly
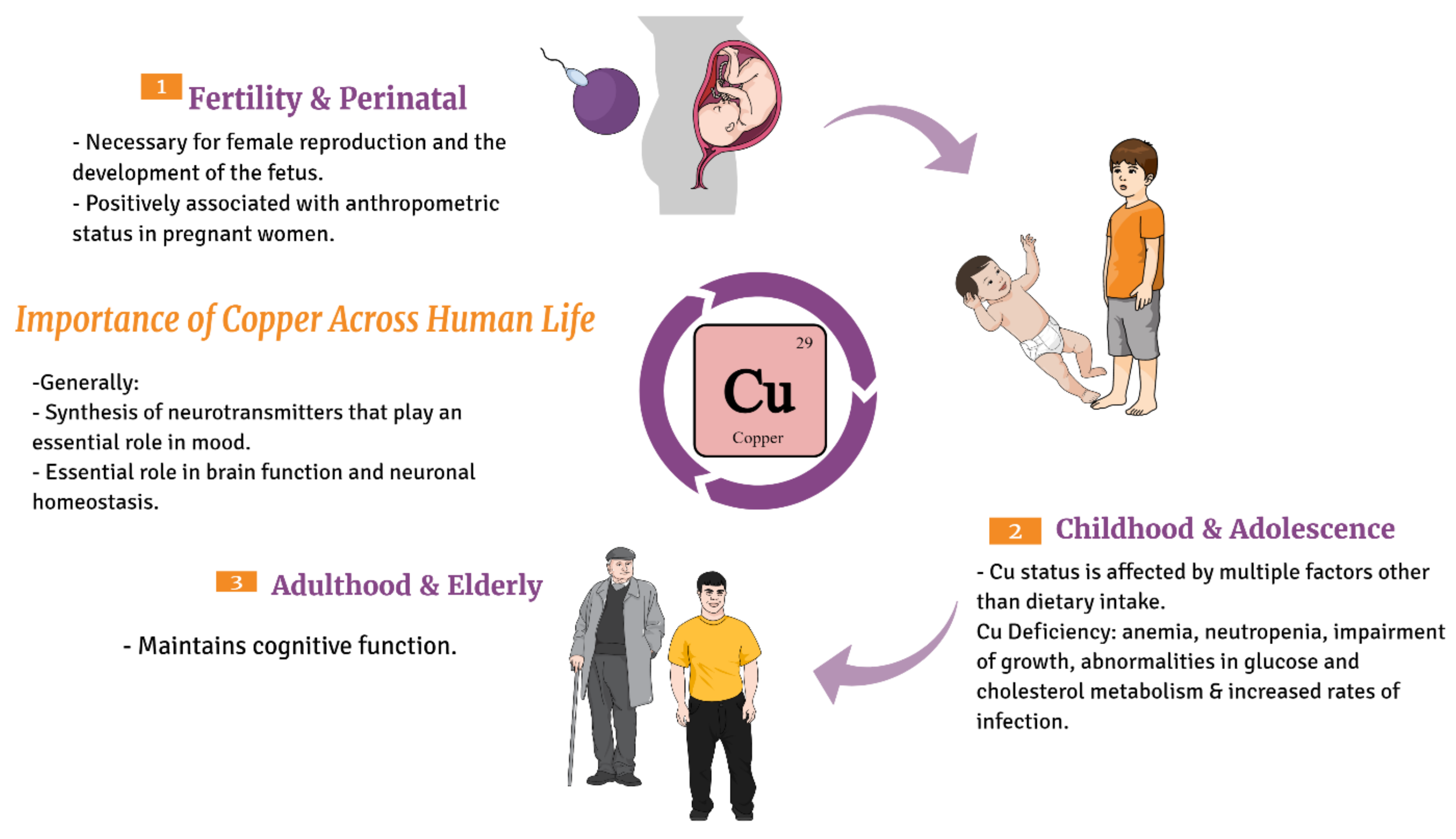
9. Copper (Cu)
9.1. Fertility and Perinatal Period
9.2. Childhood and Adolescence
9.3. Adulthood and the Elderly
10. Molybdenum
10.1. Fertility and Perinatal Period
10.2. Childhood and Adolescence
10.3. Adulthood and the Elderly
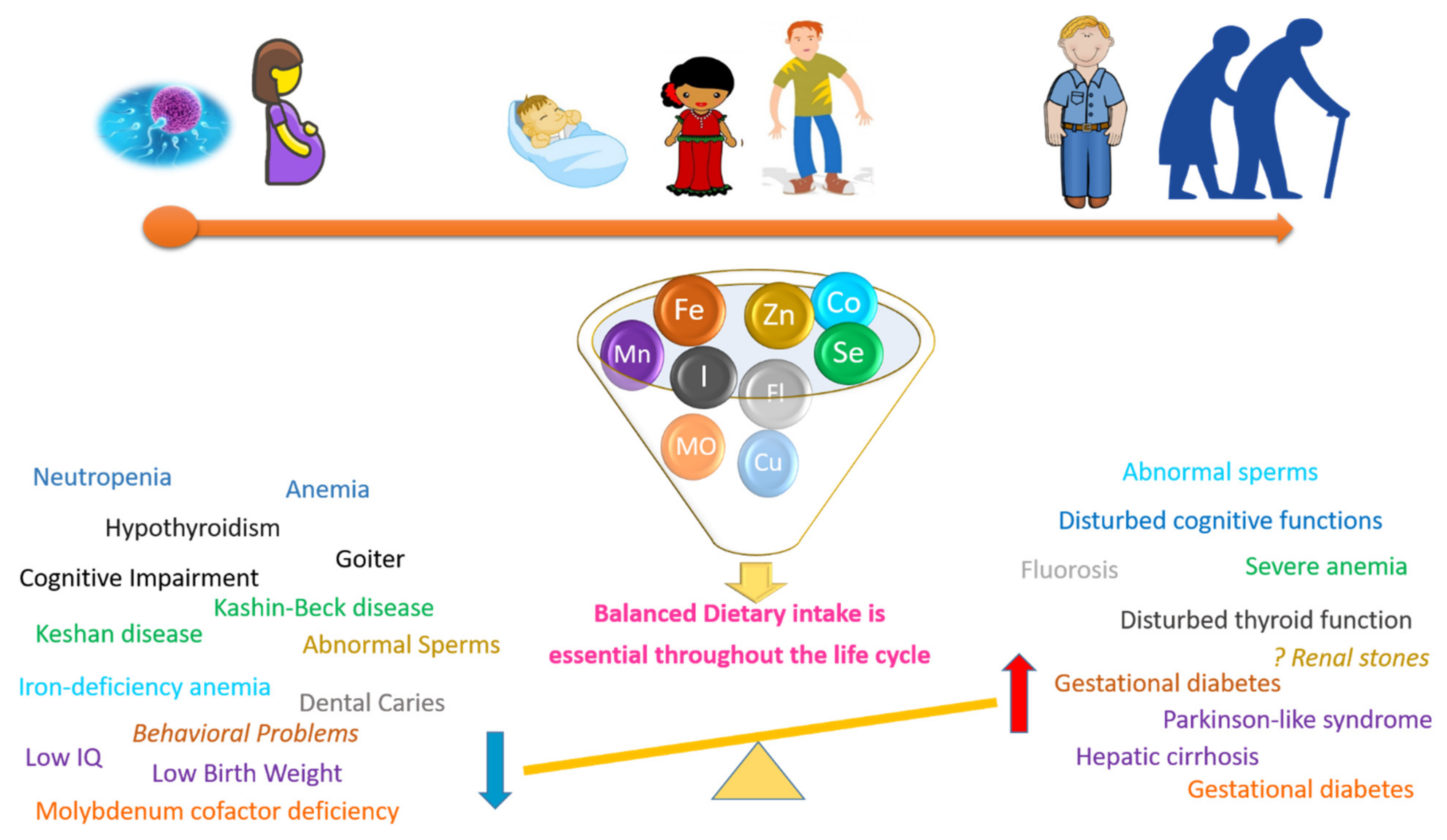
11. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ADHD | Attention Deficits and Hyperactive Disorder; |
| BMI | Body Mass Index; |
| BDNF | Brain-Derived Neurotropic Factor; |
| CAT | Catalase; |
| CNS | Central Nervous System; |
| Co | Cobalt; |
| EPA | Environmental Protection Agency; |
| FDA | Food and Drug Administration; |
| IDA | Iron deficiency anaemia; |
| IDD | Iodine deficiency disorder; |
| IQ | Intelligence Quotient; |
| LBW | Low birth weight; |
| MetS | Metabolic syndrome; |
| PIH | Pregnancy-induced hypertension syndrome; |
| PTB | Preterm birth; |
| PTB | Preterm birth; |
| UTI | Urinary Tract Infection; |
| RDA | Recommended Dietary Allowance; |
| WHO | World Health Organization; |
| Zfp | Zinc finger proteins |
References
- Zoroddu, M.A.; Aaseth, J.; Crisponi, G.; Medici, S.; Peana, M.; Nurchi, V.M. The Essential Metals for Humans: A Brief Overview. J. Inorg. Biochem. 2019, 195, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Berdanier, C.; Dwyer, D.; Heber, D. Hand Book of Nutrition and Food, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2016; ISBN 978-1-4665-0572-8. [Google Scholar]
- Awuchi, C.G.I.; Ikechukwu, V.S.A.; Echeta, C.K. Health Benefits of Micronutrients (Vitamins and Minerals) and Their Associated Deficiency Diseases: A Systematic Review. Int. J. Food Sci. 2020, 3, 1–32. [Google Scholar]
- Awuchi, C.; Victory, I.; Echeta, C. The Functional Properties of Foods and Flours. Int. J. Adv. Acad. Res. 2019, 5, 139–160. [Google Scholar]
- Blancquaert, D.; Steur, H.D.; Gellynck, X.; Straeten, D.V.D. Metabolic Engineering of Micronutrients in Crop Plants. Ann. N. Y. Acad. Sci. 2017, 1390, 59–73. [Google Scholar] [CrossRef] [Green Version]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P.; Christian, P. Micronutrient Deficiencies in Pregnancy Worldwide: Health Effects and Prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, V.H. Minerals and Pregnancy; Blackwell Science Publ.: Oxford, UK, 2011; pp. 149–167. ISBN 978-1-4443-3305-3. [Google Scholar]
- Khayat, S.; Fanaei, H.; Ghanbarzehi, A. Minerals in Pregnancy and Lactation: A Review Article. J. Clin. Diagn. Res. JCDR 2017, 11, QE01–QE05. [Google Scholar] [CrossRef]
- Liochev, S.I. Reactive Oxygen Species and the Free Radical Theory of Aging. Free Radic. Biol. Med. 2013, 60, 1–4. [Google Scholar] [CrossRef]
- Rodier, F.; Zhou, D.; Ferbeyre, G. Cellular Senescence, Geroscience, Cancer and Beyond. Aging 2018, 10, 2233–2242. [Google Scholar] [CrossRef]
- Mravunac, M.; Szymlek-Gay, E.A.; Daly, R.M.; Roberts, B.R.; Formica, M.; Gianoudis, J.; O’Connell, S.L.; Nowson, C.A.; Cardoso, B.R. Greater Circulating Copper Concentrations and Copper/Zinc Ratios Are Associated with Lower Psychological Distress, But Not Cognitive Performance, in a Sample of Australian Older Adults. Nutrients 2019, 11, 2503. [Google Scholar] [CrossRef] [Green Version]
- Pfrimer, K.; Ferriolli, E.; Takeuchi, P.L.; Salles, M.S.; Saran-Netto, A.; Zanetti, M.A.; Roma-Junior, L.C.; Braga, C.B.M.; Domenici, F.A.; Valim, Y.M.; et al. Effects of the Consumption of Milk Biofortified with Selenium, Vitamin E, and Different Fatty Acid Profile on Immune Response in the Elderly. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; van Veldhuisen, D.J.; Comin-Colet, J.; Ertl, G.; Komajda, M.; Mareev, V.; McDonagh, T.; Parkhomenko, A.; Tavazzi, L.; Levesque, V.; et al. Beneficial Effects of Long-Term Intravenous Iron Therapy with Ferric Carboxymaltose in Patients with Symptomatic Heart Failure and Iron Deficiency. Eur. Heart J. 2015, 36, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Haryanto, B.; Suksmasari, T.; Wintergerst, E.; Maggini, S. Multivitamin Supplementation Supports Immune Function and Ameliorates Conditions Triggered By Reduced Air Quality. Vitam. Miner. 2015, 4, 1–15. [Google Scholar] [CrossRef]
- Kieliszek, M.; Błażejak, S. Selenium: Significance, and Outlook for Supplementation. Nutrition 2013, 29, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Saeed, F.; Nadeem, M.; Ahmed, R.S.; Nadeem, M.T.; Arshad, M.S.; Ullah, A. Studying the Impact of Nutritional Immunology Underlying the Modulation of Immune Responses by Nutritional Compounds—A Review. Food Agric. Immunol. 2016, 27, 205–229. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Health Selenium Fact Sheet for Health Professionals. 2020. Available online: https://ods.od.nih.gov/Factsheets/Selenium-HealthProfessional/#en2 (accessed on 26 March 2021).
- Terry, E.N.; Diamond, A.M.; Erdman, J.; Macdonald, I.; Zeisel, S. Selenium. In Present Knowledge in Nutrition; Wiley-Blackwell: Washington, DC, USA, 2012; pp. 568–587. [Google Scholar]
- Galan-Chilet, I.; Tellez-Plaza, M.; Guallar, E.; de Marco, G.; Lopez-Izquierdo, R.; Gonzalez-Manzano, I.; Tormos, M.C.; Martin-Nuñez, G.M.; Rojo-Martinez, G.; Saez, G.T.; et al. Plasma Selenium Levels and Oxidative Stress Biomarkers: A Gene-Environment Interaction Population-Based Study. Free Radic. Biol. Med. 2014, 74, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H.; Benvenga, S. Selenium: An Element for Life. Endocrine 2015, 48, 756–775. [Google Scholar] [CrossRef]
- Alahmadi, B.A.; El-Alfy, S.H.; Hemaid, A.M.; Abdel-Nabi, I.M. The Protective Effects of Vitamin E against Selenium-Induced Oxidative Damage and Hepatotoxicity in Rats. J. Taibah Univ. Sci. 2020, 14, 709–720. [Google Scholar] [CrossRef]
- Kieliszek, M.; Błażejak, S. Current Knowledge on the Importance of Selenium in Food for Living Organisms: A Review. Molecules 2016, 21, 609. [Google Scholar] [CrossRef] [Green Version]
- Bampidis, V.; Azimonti, G.; de Lourdes Bastos, M.; Christensen, H.; Dusemund, B.; Kouba, M.; Kos Durjava, M.; López-Alonso, M.; López Puente, S.; Marcon, F.; et al. Assessment of the Application for Renewal of Authorisation of Selenomethionine Produced by Saccharomyces Cerevisiae NCYC R397 for All Animal Species. EFSA J. 2019, 17, e05539. [Google Scholar] [CrossRef]
- Kipp, A.P.; Strohm, D.; Brigelius-Flohé, R.; Schomburg, L.; Bechthold, A.; Leschik-Bonnet, E.; Heseker, H.; German Nutrition Society (DGE). Revised Reference Values for Selenium Intake. J. Trace Elem. Med. Biol. 2015, 32, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Higdon, J.; Drake, V.; Delage, B.; Tsuji, P. Selenium. Available online: https://lpi.oregonstate.edu/mic/minerals/selenium (accessed on 3 July 2021).
- Ross, A.C.; Caballero, B.H.; Cousins, R.J.; Tucker, K.L.; Ziegler, T.R. Modern Nutrition in Health and Disease: Eleventh Edition; Wolters Kluwer Health Adis (ESP): Alphen aan den Rijn, The Netherlands, 2012; ISBN 978-1-60547-461-8. [Google Scholar]
- Wang, L.; Yin, J.; Yang, B.; Qu, C.; Lei, J.; Han, J.; Guo, X. Serious Selenium Deficiency in the Serum of Patients with Kashin-Beck Disease and the Effect of Nano-Selenium on Their Chondrocytes. Biol. Trace Elem. Res. 2020, 194, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Hubalewska-Dydejczyk, A.; Duntas, L.; Gilis-Januszewska, A. Pregnancy, thyroid, and the potential use of selenium. Hormones 2020, 19, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Bizerea, T.O.; Dezsi, S.G.; Marginean, O.; Stroescu, R.; Rogobete, A.; Bizerea-Spiridon, O.; Ilie, C. The Link Between Selenium, Oxidative Stress and Pregnancy Induced Hypertensive Disorders. Clin. Lab. 2018, 64, 1593–1610. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium and Human Health. Lancet Lond. Engl. 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Lewandowska, M.; Sajdak, S.; Lubiński, J. Serum Selenium Level in Early Healthy Pregnancy as a Risk Marker of Pregnancy Induced Hypertension. Nutrients 2019, 11, 1028. [Google Scholar] [CrossRef] [Green Version]
- Tindell, R.; Tipple, T. Selenium: Implications for Outcomes in Extremely Preterm Infants. J. Perinatol. 2018, 38, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Nourbakhsh, M.; Ahmadpour, F.; Chahardoli, B.; Malekpour-Dehkordi, Z.; Nourbakhsh, M.; Hosseini-Fard, S.R.; Doustimotlagh, A.; Golestani, A.; Razzaghy-Azar, M. Selenium and Its Relationship with Selenoprotein P and Glutathione Peroxidase in Children and Adolescents with Hashimoto’s Thyroiditis and Hypothyroidism. J. Trace Elem. Med. Biol. 2016, 34, 10–14. [Google Scholar] [CrossRef]
- Cai, Z.; Zhang, J.; Li, H. Selenium, Aging and Aging-Related Diseases. Aging Clin. Exp. Res. 2019, 31, 1035–1047. [Google Scholar] [CrossRef]
- Jenzer, H. Iodine: Biochemistry, Deficiency and Application in Clinical Nutrition. Can. J. Clin. Nutr. 2016, 5, 1–8. [Google Scholar] [CrossRef]
- Pearce, E.N. Iodine Deficiency in Children. Paediatr. Thyroidol. 2014, 26, 130–138. [Google Scholar] [CrossRef]
- Zimmermann, M.B. Iodine Deficiency. Endocr. Rev. 2009, 30, 376–408. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, J.H. The Importance of Iodine in Public Health. Environ. Geochem. Health 2015, 37, 605–618. [Google Scholar] [CrossRef]
- Sun, X.; Shan, Z.; Teng, W. Effects of Increased Iodine Intake on Thyroid Disorders. Endocrinol. Metab. Seoul Korea 2014, 29, 240–247. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.; Trumbo, P.R. Iodine1. Adv. Nutr. 2013, 4, 262–264. [Google Scholar] [CrossRef]
- National Institute of Health Office of Dietary Supplements—Iodine. Available online: https://ods.od.nih.gov/factsheets/Iodine-HealthProfessional/ (accessed on 3 July 2021).
- Zimmermann, M.B. The Importance of Adequate Iodine during Pregnancy and Infancy. Hidden Hunger 2016, 115, 118–124. [Google Scholar] [CrossRef]
- Melse-Boonstra, A.; Jaiswal, N. Iodine Deficiency in Pregnancy, Infancy and Childhood and Its Consequences for Brain Development. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Moog, N.K.; Entringer, S.; Heim, C.; Wadhwa, P.D.; Kathmann, N.; Buss, C. Influence of Maternal Thyroid Hormones during Gestation on Fetal Brain Development. Neuroscience 2017, 342, 68–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.I. Hypothyroidism in Older Adults. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Grossman, A., Hershman, J.M., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Díez, J. Hyperthyroidism in Patients Older than 55 Years: An Analysis of the Etiology and Management. Gerontology 2003, 49, 316–323. [Google Scholar] [CrossRef]
- O’Kane, S.M.; Pourshahidi, L.K.; Mulhern, M.S.; Strain, J.; Mackle, E.M.; Koca, D.; Schomburg, L.; Hill, S.; O’Reilly, J.; Kmiotek, D.; et al. Cow Milk Consumption Increases Iodine Status in Women of Childbearing Age in a Randomized Controlled Trial. J. Nutr. 2018, 148, 401–408. [Google Scholar] [CrossRef]
- Elbon, S.M.; Johnson, M.A.; Fischer, J.G. Milk Consumption in Older Americans. Am. J. Public Health 1998, 88, 1221–1224. [Google Scholar] [CrossRef] [PubMed]
- Kaur, D.; Rasane, P.; Singh, J.; Kaur, S.; Kumar, V.; Mahato, D.K.; Dey, A.; Dhawan, K.; Kumar, S. Nutritional Interventions for Elderly and Considerations for the Development of Geriatric Foods. Curr. Aging Sci. 2019, 12, 15–27. [Google Scholar] [CrossRef]
- Dev, S.; Babitt, J.L. Overview of Iron Metabolism in Health and Disease. Hemodial. Int. Int. Symp. Home Hemodial. 2017, 21 (Suppl. 1), S6–S20. [Google Scholar] [CrossRef]
- Nutrient Reference Values—For Australia and New Zealand Iron; National Health and Medical Research Council: Canberra, Australia, 2014.
- National Institute of Health Office of Dietary Supplements—Iron. Available online: https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/ (accessed on 3 July 2021).
- Nguyen, P.H.; Young, M.; Gonzalez-Casanova, I.; Pham, H.Q.; Nguyen, H.; Truong, T.V.; Nguyen, S.V.; Harding, K.B.; Reinhart, G.A.; Martorell, R.; et al. Impact of Preconception Micronutrient Supplementation on Anemia and Iron Status during Pregnancy and Postpartum: A Randomized Controlled Trial in Rural Vietnam. PLoS ONE 2016, 11, e0167416. [Google Scholar] [CrossRef] [PubMed]
- Darling, A.M.; Mitchell, A.A.; Werler, M.M. Preconceptional Iron Intake and Gestational Diabetes Mellitus. Int. J. Environ. Res. Public. Health 2016, 13, 525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behboudi-Gandevani, S.; Safary, K.; Moghaddam-Banaem, L.; Lamyian, M.; Goshtasebi, A.; Goshtasbi, A.; Alian-Moghaddam, N. The Relationship between Maternal Serum Iron and Zinc Levels and Their Nutritional Intakes in Early Pregnancy with Gestational Diabetes. Biol. Trace Elem. Res. 2013, 154, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Helin, A.; Kinnunen, T.I.; Raitanen, J.; Ahonen, S.; Virtanen, S.M.; Luoto, R. Iron Intake, Haemoglobin and Risk of Gestational Diabetes: A Prospective Cohort Study. BMJ Open 2012, 2, e001730. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Zhang, N.; Zhang, D.; Ren, Q.; Ganz, T.; Liu, S.; Nemeth, E. Iron Homeostasis in Pregnancy and Spontaneous Abortion. Am. J. Hematol. 2019, 94, 184–188. [Google Scholar] [CrossRef] [Green Version]
- Jorgensen, J.M.; Yang, Z.; Lönnerdal, B.; Chantry, C.J.; Dewey, K.G. Effect of Iron Supplementation during Lactation on Maternal Iron Status and Oxidative Stress: A Randomized Controlled Trial. Matern. Child. Nutr. 2017, 13. [Google Scholar] [CrossRef] [Green Version]
- Marin, G.; Mestorino, N.; Errecalde, J.; Huber, B.; Uriarte, A.; Orchuela, J. Personalised Iron Supply for Prophylaxis and Treatment of Pregnant Women as a Way to Ensure Normal Iron Levels in Their Breast Milk. J. Med. Life 2012, 5, 29–32. [Google Scholar]
- Friel, J.; Qasem, W.; Cai, C. Iron and the Breastfed Infant. Antioxidants 2018, 7, 54. [Google Scholar] [CrossRef] [Green Version]
- Krebs, N.F.; Sherlock, L.G.; Westcott, J.; Culbertson, D.; Hambidge, K.M.; Feazel, L.M.; Robertson, C.E.; Frank, D.N. Effects of Different Complementary Feeding Regimens on Iron Status and Enteric Microbiota in Breastfed Infants. J. Pediatr. 2013, 163, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Tang, M.; Frank, D.; Sherlock, L.; Ir, D.; Robertson, C.; Krebs, N. Effect of Vitamin E With Therapeutic Iron Supplementation on Iron Repletion and Gut Microbiome in US Iron Deficient Infants and Toddlers. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Angulo-Barroso, R.M.; Li, M.; Santos, D.C.C.; Bian, Y.; Sturza, J.; Jiang, Y.; Kaciroti, N.; Richards, B.; Lozoff, B. Iron Supplementation in Pregnancy or Infancy and Motor Development: A Randomized Controlled Trial. Pediatrics 2016, 137, e20153547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doom, J.R.; Richards, B.; Caballero, G.; Delva, J.; Gahagan, S.; Lozoff, B. Infant Iron Deficiency and Iron Supplementation Predict Adolescent Internalizing, Externalizing, and Social Problems. J. Pediatr. 2018, 195, 199–205.e2. [Google Scholar] [CrossRef] [PubMed]
- Lange, K.W.; Hauser, J.; Lange, K.M.; Makulska-Gertruda, E.; Nakamura, Y.; Reissmann, A.; Sakaue, Y.; Takano, T.; Takeuchi, Y. The Role of Nutritional Supplements in the Treatment of ADHD: What the Evidence Says. Curr. Psychiatry Rep. 2017, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Chao, K.-C.; Chang, C.-C.; Chiou, H.-Y.; Chang, J.-S. Serum Ferritin Is Inversely Correlated with Testosterone in Boys and Young Male Adolescents: A Cross-Sectional Study in Taiwan. PLoS ONE 2015, 10, e0144238. [Google Scholar] [CrossRef]
- Dhindsa, S.; Ghanim, H.; Batra, M.; Kuhadiya, N.D.; Abuaysheh, S.; Green, K.; Makdissi, A.; Chaudhuri, A.; Dandona, P. Effect of Testosterone on Hepcidin, Ferroportin, Ferritin and Iron Binding Capacity in Patients with Hypogonadotropic Hypogonadism and Type 2 Diabetes. Clin. Endocrinol. 2016, 85, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Beggs, L.A.; Yarrow, J.F.; Conover, C.F.; Meuleman, J.R.; Beck, D.T.; Morrow, M.; Zou, B.; Shuster, J.J.; Borst, S.E. Testosterone Alters Iron Metabolism and Stimulates Red Blood Cell Production Independently of Dihydrotestosterone. Am. J. Physiol. Endocrinol. Metab. 2014, 307, E456–E461. [Google Scholar] [CrossRef]
- El Osta, R.; Grandpre, N.; Monnin, N.; Hubert, J.; Koscinski, I. Hypogonadotropic Hypogonadism in Men with Hereditary Hemochromatosis. Basic Clin. Androl. 2017, 27, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von, H.S.; Ebner, N.; Evertz, R.; Ponikowski, P.; Anker, S.D. Iron Deficiency in Heart Failure. JACC Heart Fail. 2019, 7, 36–46. [Google Scholar] [CrossRef]
- Portolés, J.; Martín, L.; Broseta, J.J.; Cases, A. Anemia in Chronic Kidney Disease: From Pathophysiology and Current Treatments, to Future Agents. Front. Med. 2021, 8, 328. [Google Scholar] [CrossRef]
- Lewis, J.B.; Sika, M.; Koury, M.J.; Chuang, P.; Schulman, G.; Smith, M.T.; Whittier, F.C.; Linfert, D.R.; Galphin, C.M.; Athreya, B.P.; et al. Ferric Citrate Controls Phosphorus and Delivers Iron in Patients on Dialysis. J. Am. Soc. Nephrol. JASN 2015, 26, 493–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hokin, B.; Adams, M.; Ashton, J.; Louie, H. Comparison of the Dietary Cobalt Intake in Three Different Australian Diets. Asia Pac. J. Clin. Nutr. 2004, 13, 289–291. [Google Scholar] [PubMed]
- Adolfo, F.R.; Do Nascimento, P.C.; Bohrer, D.; De Carvalho, L.M.; Viana, C.; Guarda, A.; Nunes Colim, A.; Mattiazzi, P. Simultaneous Determination of Cobalt and Nickel in Vitamin B12 Samples Using High-Resolution Continuum Source Atomic Absorption Spectrometry. Talanta 2016, 147, 241–245. [Google Scholar] [CrossRef]
- Tvermoes, B.E.; Finley, B.L.; Unice, K.M.; Otani, J.M.; Paustenbach, D.J.; Galbraith, D.A. Cobalt Whole Blood Concentrations in Healthy Adult Male Volunteers Following Two-Weeks of Ingesting a Cobalt Supplement. Food Chem. Toxicol. 2013, 53, 432–439. [Google Scholar] [CrossRef]
- National Institute of Health Office of Dietary Supplements—Vitamin B12. Available online: https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/ (accessed on 3 July 2021).
- Marzec-Wróblewska, U.; Kamiński, P.; Łakota, P.; Szymański, M.; Wasilow, K.; Ludwikowski, G.; Jerzak, L.; Stuczyński, T.; Woźniak, A.; Buciński, A. Human Sperm Characteristics with Regard to Cobalt, Chromium, and Lead in Semen and Activity of Catalase in Seminal Plasma. Biol. Trace Elem. Res. 2019, 188, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.-J.; Liang, C.-M.; Xia, X.; Huang, K.; Yan, S.-Q.; Tao, R.W.; Pan, W.-J.; Sheng, J.; Tao, Y.-R.; Xiang, H.-Y.; et al. Association between Maternal and Umbilical Cord Serum Cobalt Concentration during Pregnancy and the Risk of Preterm Birth: The Ma’anshan Birth Cohort (MABC) Study. Chemosphere 2019, 218, 487–492. [Google Scholar] [CrossRef]
- Angelova, M.G.; Petkova-Marinova, T.V.; Pogorielov, M.V.; Loboda, A.N.; Nedkova-Kolarova, V.N.; Bozhinova, A.N. Trace Element Status (Iron, Zinc, Copper, Chromium, Cobalt, and Nickel) in Iron-Deficiency Anaemia of Children under 3 Years. Anemia 2014, 2014, 718089. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Sood, S.; Arora, B.; Singh, M.; Beena. Effect of Duration of Fluoride Exposure on the Reproductive System in Male Rabbits. J. Hum. Reprod. Sci. 2010, 3, 148–152. [Google Scholar] [CrossRef]
- Aldrees, A.; Al-Manea, S. Fluoride Content of Bottled Drinking Waters Available in Riyadh, Saudi Arabia. Saudi Dent. J. 2010, 22, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoun, A.; Darwiche, F.; Al Hayek, S.; Doumit, J. The Fluoride Debate: The Pros and Cons of Fluoridation. Prev. Nutr. Food Sci. 2018, 23, 171–180. [Google Scholar] [CrossRef]
- National Institute of Health Office of Dietary Supplements—Fluoride. Available online: https://ods.od.nih.gov/factsheets/Fluoride-HealthProfessional/ (accessed on 3 July 2021).
- Chaithra, B.; Sarjan, H.N.; Shivabasavaiah. A Comparative Analysis of Fluoride-Contaminated Groundwater and Sodium Fluoride-Induced Reproductive Toxicity and Its Reversibility in Male Rats. Biol. Trace Elem. Res. 2020, 197, 507–521. [Google Scholar] [CrossRef] [PubMed]
- Darmani, H.; Al-Hiyasat, A.S.; Irbid, A.M.E. Effects of Sodium Fluoride in Drinking Water on Fertility in Female Mice. Fluoride 2001, 34, 242–249. [Google Scholar]
- Abduweli Uyghurturk, D.; Goin, D.E.; Martinez-Mier, E.A.; Woodruff, T.J.; DenBesten, P.K. Maternal and Fetal Exposures to Fluoride during Mid-Gestation among Pregnant Women in Northern California. Environ. Health 2020, 19, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, R.; Lanphear, B.; Hornung, R.; Flora, D.; Martinez-Mier, E.A.; Neufeld, R.; Ayotte, P.; Muckle, G.; Till, C. Association Between Maternal Fluoride Exposure During Pregnancy and IQ Scores in Offspring in Canada. JAMA Pediatr. 2019, 173, 940. [Google Scholar] [CrossRef]
- Goyal, L.D.; Bakshi, D.K.; Arora, J.K.; Manchanda, A.; Singh, P. Assessment of Fluoride Levels during Pregnancy and Its Association with Early Adverse Pregnancy Outcomes. J. Fam. Med. Prim. Care 2020, 9, 2693–2698. [Google Scholar] [CrossRef]
- Shivarajashankara, Y.; Shivashankara, A.; Rao, S.H.; Karnataka, P.G.B. Oxidative Stress in Children with Endemic Skeletal Fluorosis. Fluoride 2001, 34, 103–107. [Google Scholar]
- Liu, Y.; Téllez-Rojo, M.; Hu, H.; Sánchez, B.N.; Martinez-Mier, E.A.; Basu, N.; Mercado-García, A.; Solano-González, M.; Peterson, K.E. Fluoride Exposure and Pubertal Development in Children Living in Mexico City. Environ. Health 2019, 18, 26. [Google Scholar] [CrossRef] [Green Version]
- Malin, A.J.; Bose, S.; Busgang, S.A.; Gennings, C.; Thorpy, M.; Wright, R.O.; Wright, R.J.; Arora, M. Fluoride Exposure and Sleep Patterns among Older Adolescents in the United States: A Cross-Sectional Study of NHANES 2015–2016. Environ. Health 2019, 18, 106. [Google Scholar] [CrossRef] [Green Version]
- Toumba, K.J.; Twetman, S.; Splieth, C.; Parnell, C.; van Loveren, C.; Lygidakis, N.A. Guidelines on the Use of Fluoride for Caries Prevention in Children: An Updated EAPD Policy Document. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2019, 20, 507–516. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E. Editorial - Prevention of Dental Caries through the Use of FLuoride—The WHO Approach. Community Dent. Health 2016, 66–68. [Google Scholar] [CrossRef]
- O’Mullane, D.M. Fluoride and Oral Health. Community Dent. Health 2016, 69–99. [Google Scholar] [CrossRef]
- Griffin, S.O.; Regnier, E.; Griffin, P.M.; Huntley, V. Effectiveness of Fluoride in Preventing Caries in Adults. J. Dent. Res. 2007, 86, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Souza-Rodrigues, R.D.; da Silva Ferreira, S.; D’almeida-Couto, R.S.; Lachowski, K.M.; Sobral, M.Â.P.; Marques, M.M. Choice of Toothpaste for the Elderly: An in Vitro Study. Braz. Oral Res. 2015, 29, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, K.R. High Fluoride Dentifrices for Elderly and Vulnerable Adults: Does It Work and If So, Then Why? Caries Res. 2016, 50 (Suppl. 1), 15–21. [Google Scholar] [CrossRef] [Green Version]
- Chasapis, C.T.; Spiliopoulou, C.A.; Loutsidou, A.C.; Stefanidou, M.E. Zinc and Human Health: An Update. Arch. Toxicol. 2012, 86, 521–534. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health Office of Dietary Supplements—Zinc. Available online: https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/ (accessed on 3 July 2021).
- Kerns, K.; Zigo, M.; Sutovsky, P. Zinc: A Necessary Ion for Mammalian Sperm Fertilization Competency. Int. J. Mol. Sci. 2018, 19, 4097. [Google Scholar] [CrossRef] [Green Version]
- Fallah, A.; Mohammad-Hasani, A.; Colagar, A.H. Zinc Is an Essential Element for Male Fertility: A Review of Zn Roles in Men’s Health, Germination, Sperm Quality, and Fertilization. J. Reprod. Infertil. 2018, 19, 69–81. [Google Scholar]
- Sørensen, M.B.; Bergdahl, I.A.; Hjøllund, N.H.I.; Bonde, J.P.E.; Stoltenberg, M.; Ernst, E. Zinc, Magnesium and Calcium in Human Seminal Fluid: Relations to Other Semen Parameters and Fertility. Mol. Hum. Reprod. 1999. [Google Scholar] [CrossRef] [Green Version]
- Alemu, B.; Gashu, D. Association of Maternal Anthropometry, Hemoglobin and Serum Zinc Concentration during Pregnancy with Birth Weight. Early Hum. Dev. 2020, 142, 104949. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Black, R.E.; Brown, K.H.; Meeks Gardner, J.; Gore, S.; Hidayat, A.; Khatun, F.; Martorell, R.; Ninb, N.X.; Penny, M.E.; et al. Prevention of Diarrhea and Pneumonia by Zinc Supplementation in Children in Developing Countries: Pooled Analysis of Randomized Controlled Trials. J. Pediatr. 1999, 135, 689–697. [Google Scholar] [CrossRef]
- Kaur, K.; Gupta, R.; Saraf, S.A.; Saraf, S.K. Zinc: The Metal of Life. Compr. Rev. Food Sci. Food Saf. 2014, 13, 358–376. [Google Scholar] [CrossRef] [PubMed]
- Valavi, E.; Hakimzadeh, M.; Shamsizadeh, A.; Aminzadeh, M.; Alghasi, A. The Efficacy of Zinc Supplementation on Outcome of Children with Severe Pneumonia. A Randomized Double-Blind Placebo-Controlled Clinical Trial. Indian J. Pediatr. 2011, 78, 1079–1084. [Google Scholar] [CrossRef]
- Basnet, S.; Shrestha, P.S.; Sharma, A.; Mathisen, M.; Prasai, R.; Bhandari, N.; Adhikari, R.K.; Sommerfelt, H.; Valentiner-Branth, P.; Strand, T.A. A Randomized Controlled Trial of Zinc as Adjuvant Therapy for Severe Pneumonia in Young Children. Pediatrics 2012, 129, 701–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sempértegui, F.; Estrella, B.; Rodríguez, O.; Gómez, D.; Cabezas, M.; Salgado, G.; Sabin, L.L.; Hamer, D.H. Zinc as an Adjunct to the Treatment of Severe Pneumonia in Ecuadorian Children: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2014, 99, 497–505. [Google Scholar] [CrossRef]
- Shah, G.S.; Dutta, A.K.; Shah, D.; Mishra, O.P. Role of Zinc in Severe Pneumonia: A Randomized Double Bind Placebo Controlled Study. Ital. J. Pediatr. 2012, 38, 36. [Google Scholar] [CrossRef] [Green Version]
- Zabihi, F.; Mostafavi, M.; Esmaeili, M.; Cheshani, M.I. Investigating the Effect of Zinc Deficiency on the Risk of Urinary Tract Infection in Children. Int. J. Pediatr. 2020, 8, 11959–11966. [Google Scholar]
- Negri, A.L. The Role of Zinc in Urinary Stone Disease. Int. Urol. Nephrol. 2018, 50, 879–883. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, Y.; Wang, D.; Zhou, Q. Dietary Zinc Intake, Supplemental Zinc Intake and Serum Zinc Levels and the Prevalence of Kidney Stones in Adults. J. Trace Elem. Med. Biol. 2020, 57, 126410. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, F.; Corbi, G.; Mazzeo, G.; Boccia, M.; Aronne, L.; D’Agnano, V.; Komici, K.; Mazzarella, G.; Parrella, R.; Bianco, A. COVID-19 and the Elderly: Insights into Pathogenesis and Clinical Decision-Making. Aging Clin. Exp. Res. 2020, 1–10. [Google Scholar] [CrossRef]
- Amore, S.; Puppo, E.; Melara, J.; Terracciano, E.; Gentili, S.; Liotta, G. Impact of COVID-19 on Older Adults and Role of Long-Term Care Facilities during Early Stages of Epidemic in Italy. Sci. Rep. 2021, 11, 12530. [Google Scholar] [CrossRef] [PubMed]
- de Almeida Brasiel, P.G. The Key Role of Zinc in Elderly Immunity: A Possible Approach in the COVID-19 Crisis. Clin. Nutr. ESPEN 2020, 38, 65–66. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Wu, W.; Gu, X.; Dai, S.; Zhou, Q.; Deng, H.; Shen, F.; Chen, J. Association of Serum Copper, Zinc and Selenium Levels with Risk of Metabolic Syndrome: A Nested Case-Control Study of Middle-Aged and Older Chinese Adults. J. Trace Elem. Med. Biol. 2019, 52, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Yeung, D.C.Y.; Lam, K.S.L.; Wang, Y.; Tso, A.W.K.; Xu, A. Serum Zinc-A2-Glycoprotein Correlates with Adiposity, Triglycerides, and the Key Components of the Metabolic Syndrome in Chinese Subjects. J. Clin. Endocrinol. Metab. 2009, 94, 2531–2536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, A.; Zahediasl, S.; Hosseini-Esfahani, F.; Azizi, F. Gender Differences in the Relationship between Serum Zinc Concentration and Metabolic Syndrome. Ann. Hum. Biol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Bornhorst, J.; Aschner, M. Manganese Metabolism in Humans. Front. Biosci. Landmark Ed. 2018, 23, 1655–1679. [Google Scholar] [CrossRef] [Green Version]
- Kumar, K.K.; Lowe, J.; Aboud, A.A.; Neely, M.D.; Redha, R.; Bauer, J.A.; Odak, M.; Weaver, C.D.; Meiler, J.; Aschner, M.; et al. Cellular Manganese Content Is Developmentally Regulated in Human Dopaminergic Neurons. Sci. Rep. 2014, 4, 6801. [Google Scholar] [CrossRef]
- Lucchini, R.G.; Aschner, M.; Kim, Y.; Šarić, M. Manganese. In Handbook on the Toxicology of Metals; Elsevier Inc.: Amsterdam, The Netherlands, 2015. [Google Scholar] [CrossRef]
- National Institute of Health Office of Dietary Supplements—Manganese. Available online: https://ods.od.nih.gov/factsheets/Manganese-HealthProfessional/ (accessed on 3 July 2021).
- McRae, N.; Bello, G.; Svensson, K.; Solano-González, M.; Wright, R.J.; Niedzwiecki, M.M.; Calapiz, M.T.; Amarasiriwardena, C.; Schnaas, L.; Tamayo-Ortiz, M.; et al. Blood Manganese Levels during Pregnancy and Postpartum Depression: A Cohort Study among Women in Mexico. Neurotoxicology 2020, 76, 183–190. [Google Scholar] [CrossRef]
- Gromova, O.A.; Andreeva, E.N.; Torshin, I.Y.; Tapilskaya, N.I.; Uvarova, E.V. A systemic biological analysis of the role of manganese in obstetrics and gynaecology: Women’s reproductive health, menstrual cycle regulation and prevention of fetal malformations. Gynecol. Obstet. Perinatol. 2020, 19, 103–113. [Google Scholar] [CrossRef]
- Slicker, J.; Vermilyea, S. Pediatric Parenteral Nutrition: Putting the Microscope on Macronutrients and Micronutrients. Nutr. Clin. Pract. 2009, 24, 481–486. [Google Scholar] [CrossRef]
- Erikson, K.M.; Aschner, M. Manganese: Its Role in Disease and Health. In Essential Metals in Medicine: Therapeutic Use and Toxicity of Metal Ions in the Clinic; Carver, P.L., Ed.; Walter De Gruyter Gmbh: Berlin, Germany, 2019; Volume 19, pp. 253–266. ISBN 978-3-11-052787-2. [Google Scholar]
- Bailey, R.L.; Fulgoni, V.L.; Keast, D.R.; Dwyer, J.T. Dietary Supplement Use Is Associated with Higher Intakes of Minerals from Food Sources. Am. J. Clin. Nutr. 2011, 94, 1376–1381. [Google Scholar] [CrossRef] [Green Version]
- Stierman, B.; Woolf, A.; Korrick, S. Associations of Prenatal Manganese with Visual-Motor Skills in Adolescence. Clin. Toxicol. 2019, 57, 872–873. [Google Scholar]
- Gong, J.H.; Lo, K.; Liu, Q.; Li, J.; Lai, S.; Shadyab, A.H.; Arcan, C.; Snetselaar, L.; Liu, S. Dietary Manganese, Plasma Markers of Inflammation, and the Development of Type 2 Diabetes in Postmenopausal Women: Findings From the Women’s Health Initiative. Diabetes Care 2020, 43, 1344–1351. [Google Scholar] [CrossRef]
- Kresovich, J.K.; Bulka, C.M.; Joyce, B.T.; Vokonas, P.S.; Schwartz, J.; Baccarelli, A.A.; Hibler, E.A.; Hou, L. The Inflammatory Potential of Dietary Manganese in a Cohort of Elderly Men. Biol. Trace Elem. Res. 2018, 183, 49–57. [Google Scholar] [CrossRef]
- Eaton-Evans, J.; Mcllrath, E.M.; Jackson, W.E.; McCartney, H.; Strain, J.J. Copper Supplementation and the Maintenance of Bone Mineral Density in Middle-Aged Women. J. Trace Elem. Exp. Med. 1996, 9, 87–94. [Google Scholar] [CrossRef]
- Al-khateeb, E.; Al-zayadneh, E.; Al-dalahmah, O.; Alawadi, Z.; khatib, F.; Naffa, R.; Shafagoj, Y. Relation between Copper, Lipid Profile, and Cognition in Elderly Jordanians. J. Alzheimers Dis. JAD 2014, 41, 203–211. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health Office of Dietary Supplements—Copper. Available online: https://ods.od.nih.gov/factsheets/Copper-HealthProfessional/ (accessed on 3 July 2021).
- Kashanian, M.; Hadizadeh, H.; Faghankhani, M.; Nazemi, M.; Sheikhansari, N. Evaluating the Effects of Copper Supplement during Pregnancy on Premature Rupture of Membranes and Pregnancy Outcome. J. Matern.-Fetal Neonatal Med. 2018, 31, 39–46. [Google Scholar] [CrossRef]
- Sak, S.; Barut, M.; Çelik, H.; Incebiyik, A.; Ağaçayak, E.; Uyanikoglu, H.; Kirmit, A.; Sak, M. Copper and Ceruloplasmin Levels Are Closely Related to the Severity of Preeclampsia. J. Matern.-Fetal Neonatal Med. 2020, 33, 96–102. [Google Scholar] [CrossRef]
- Latorre, M.; Troncoso, R.; Uauy, R. Chapter 4 - Biological Aspects of Copper. In Clinical and Translational Perspectives on WILSON DISEASE; Kerkar, N., Roberts, E.A., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 25–31. ISBN 978-0-12-810532-0. [Google Scholar]
- Olivares, M.; Lönnerdal, B.; Abrams, S.A.; Pizarro, F.; Uauy, R. Age and Copper Intake Do Not Affect Copper Absorption, Measured with the Use of 65Cu as a Tracer, in Young Infants. Am. J. Clin. Nutr. 2002, 76, 641–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domellof, M. Nutritional Care of Premature Infants: Microminerals. In Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines; Koletzko, B., Poindexter, B., Uauy, R., Eds.; Karger: Basel, Switzerland, 2014; Volume 110, pp. 121–139. ISBN 978-3-318-02641-2. [Google Scholar]
- Nakamura, M.; Miura, A.; Nagahata, T.; Shibata, Y.; Okada, E.; Ojima, T. Low Zinc, Copper, and Manganese Intake Is Associated with Depression and Anxiety Symptoms in the Japanese Working Population: Findings from the Eating Habit and Well-Being Study. Nutrients 2019, 11, 847. [Google Scholar] [CrossRef] [Green Version]
- Ni, M.; You, Y.; Chen, J.; Zhang, L. Copper in Depressive Disorder: A Systematic Review and Meta-Analysis of Observational Studies. Psychiatry Res. 2018, 267, 506–515. [Google Scholar] [CrossRef]
- Styczeń, K.; Sowa-Kućma, M.; Siwek, M.; Dudek, D.; Reczyński, W.; Misztak, P.; Szewczyk, B.; Topór-Mądry, R.; Opoka, W.; Nowak, G. Study of the Serum Copper Levels in Patients with Major Depressive Disorder. Biol. Trace Elem. Res. 2016, 174, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Sfar, S.; Jawed, A.; Braham, H.; Amor, S.; Laporte, F.; Kerkeni, A. Zinc, Copper and Antioxidant Enzyme Activities in Healthy Elderly Tunisian Subjects. Exp. Gerontol. 2009, 44, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, A.; Terazawa-Watanabe, M.; Kazumi, T.; Fukuo, K. Associations of Decreased Serum Transthyretin with Elevated High-Sensitivity CRP, Serum Copper and Decreased Hemoglobin in Ambulatory Elderly Women. Asia Pac. J. Clin. Nutr. 2015, 24, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Tsongas, T.A.; Meglen, R.R.; Walravens, P.A.; Chappell, W.R. Molybdenum in the Diet: An Estimate of Average Daily Intake in the United States. Am. J. Clin. Nutr. 1980, 33, 1103–1107. [Google Scholar] [CrossRef] [Green Version]
- Novotny, J.A. Molybdenum Nutriture in Humans. J. Evid.-Based Complement. Altern. Med. 2011, 16, 164–168. [Google Scholar] [CrossRef]
- Garrett, R.M.; Johnson, J.L.; Graf, T.N.; Feigenbaum, A.; Rajagopalan, K.V. Human Sulfite Oxidase R160Q: Identification of the Mutation in a Sulfite Oxidase-Deficient Patient and Expression and Characterization of the Mutant Enzyme. Proc. Natl. Acad. Sci. USA 1998, 95, 6394–6398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, B.; Reichmann, D.; Niks, D.; Krompholz, N.; Havemeyer, A.; Clement, B.; Messerschmidt, T.; Rothkegel, M.; Biester, H.; Hille, R.; et al. Biochemical and Spectroscopic Characterization of the Human Mitochondrial Amidoxime Reducing Components HmARC-1 and HmARC-2 Suggests the Existence of a New Molybdenum Enzyme Family in Eukaryotes. J. Biol. Chem. 2010, 285, 37847–37859. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization; International Atomic Energy Agency; Food and Agriculture Organization of the United Nations. Trace Elements in Human Nutrition and Health; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Reiss, J.; Hahnewald, R. Molybdenum Cofactor Deficiency: Mutations in GPHN, MOCS1, and MOCS2. Hum. Mutat. 2011, 32, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Novotny, J.A.; Turnlund, J.R. Molybdenum Intake Influences Molybdenum Kinetics in Men. J. Nutr. 2007, 137, 37–42. [Google Scholar] [CrossRef]
- Vázquez-Salas, R.A.; López-Carrillo, L.; Menezes-Filho, J.A.; Rothenberg, S.J.; Cebrián, M.E.; Schnaas, L.; de Souza Viana, G.F.; Torres-Sánchez, L. Prenatal Molybdenum Exposure and Infant Neurodevelopment in Mexican Children. Nutr. Neurosci. 2014, 17, 72–80. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhang, C.; Weisskopf, M.; Williams, P.L.; Parsons, P.J.; Palmer, C.D.; Buck Louis, G.M.; James-Todd, T. A Prospective Study of Early Pregnancy Essential Metal(Loid)s and Glucose Levels Late in the Second Trimester. J. Clin. Endocrinol. Metab. 2019, 104, 4295–4303. [Google Scholar] [CrossRef]
- Lee, E.J.; Dandamudi, R.; Granadillo, J.L.; Grange, D.K.; Kakajiwala, A. Rare Cause of Xanthinuria: A Pediatric Case of Molybdenum Cofactor Deficiency B. CEN Case Rep. 2021, 10, 378–382. [Google Scholar] [CrossRef]
- Schuierer, G.; Kurlemann, G.; Bick, U.; Stephani, U. Molybdenum-Cofactor Deficiency: CT and MR Findings. Neuropediatrics 1995, 26, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Guallar, E.; Cowie, C.C. Metals in Urine and Diabetes in U.S. Adults. Diabetes 2016, 65, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, R.; Singh, S.P. Effects of Molybdenum on Fertility of Male Rats. Biometals 2002, 15, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Zhai, X.-W.; Zhang, Y.-L.; Qi, Q.; Bai, Y.; Chen, X.-L.; Jin, L.-J.; Ma, X.-G.; Shu, R.-Z.; Yang, Z.-J.; Liu, F.-J. Effects of Molybdenum on Sperm Quality and Testis Oxidative Stress. Syst. Biol. Reprod. Med. 2013, 59, 251–255. [Google Scholar] [CrossRef]
- Meeker, J.D.; Rossano, M.G.; Protas, B.; Padmanabhan, V.; Diamond, M.P.; Puscheck, E.; Daly, D.; Paneth, N.; Wirth, J.J. Environmental Exposure to Metals and Male Reproductive Hormones: Circulating Testosterone Is Inversely Associated with Blood Molybdenum. Fertil. Steril. 2010, 93, 130. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Selenium | Iodine | |||||
|---|---|---|---|---|---|---|
| Life Stage | Age | Males (µg/day) | Females (µg/day) | Age | Males (µg/day) | Females (µg/day) |
| Infants | 0–6 months | 15 | 15 | 0–6 months | 110 | 110 |
| 7–12 months | 20 | 20 | 7–12 months | 130 | 130 | |
| Children | 1–3 years | 20 | 20 | 1–8 years | 90 | 90 |
| 4–8 years | 30 | 30 | 9–13 years | 120 | 120 | |
| 9–13 years | 40 | 40 | 14–18 years | 150 | 150 | |
| Adolescents | 14–18 years | 55 | 55 | ≥19 years | 150 | 150 |
| Adults | 19–50 years | 55 | 55 | - | - | - |
| Pregnant | - | - | 60 | - | 220 | |
| Breastfeeding | - | - | 70 | - | - | 290 |
| Iron | Vit. B12 (Cobalt) | |||||
|---|---|---|---|---|---|---|
| Life Stage | Age in Years | Males (mg/day) | Females (mg/day) | Age in Years | Males (µg/day) | Females (µg/day) |
| Children | 1–3 | 9 | 9 | 1–3 | 0.9 | 0.9 |
| 4–8 | 10 | 10 | 4–8 | 1.2 | 1.2 | |
| 9–13 | 8 | 8 | 9–13 years | 1.8 | 1.8 | |
| Adolescents | 14–18 | 11 | 15 | 14–18 years | 2.4 | 2.4 |
| Adults | 19–50 | 8 | 18 | 19 years | 2.4 | 2.4 |
| 51–>70 | 8 | 8 | - | - | - | |
| Pregnant | 19–50 | - | 27 | 2.6 | ||
| Breastfeeding | 19–50 | - | 9 | 2.8 | ||
| Fluoride | Zinc | |||||
|---|---|---|---|---|---|---|
| Life Stage | Age in Years | Males (mg/day) | Females (mg/day) | Age in Years | Males (mg/day) | Females (mg/day) |
| Children | 1–3 | 0.7 | 0.7 | 1–3 | 3 | 3 |
| 4–8 | 1 | 1 | 4–8 | 5 | 5 | |
| 9–13 | 2 | 2 | 9–13 years | 8 | 8 | |
| Adolescents | 14–18 | 3 | 3 | 14–18 years | 11 | 9 |
| Adults | ≥19 | 4 | 3 | ≥19 years | 11 | 9 |
| Pregnant | ≥19 years | - | 3 | ≥19 years | - | 11 |
| Breastfeeding | ≥19 years | - | 3 | ≥19 years | - | 12 |
| Manganese | Copper | |||||
|---|---|---|---|---|---|---|
| Life Stage | Age in Years | Males (mg/day) | Females (mg/day) | Age in Years | Males (µg/day) | Females (µg/day) |
| Children | 1–3 | 1.2 | 1.2 | 1–3 | 340 | 340 |
| 4–8 | 1.5 | 1.5 | 4–8 | 440 | 440 | |
| 9–13 | 1.9 | 1.6 | 9–13 | 700 | 700 | |
| Adolescents | 14–18 | 2.2 | 1.6 | 14–18 | 890 | 890 |
| Adults | ≥19 | 2.3 | 1.8 | ≥19 | 900 | 900 |
| Pregnant | ≥19 years | - | 2 | ≥19 years | - | 1300 |
| Breastfeeding | ≥19 years | - | 2.6 | ≥19 years | - | 1300 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farag, M.A.; Hamouda, S.; Gomaa, S.; Agboluaje, A.A.; Hariri, M.L.M.; Yousof, S.M. Dietary Micronutrients from Zygote to Senility: Updated Review of Minerals’ Role and Orchestration in Human Nutrition throughout Life Cycle with Sex Differences. Nutrients 2021, 13, 3740. https://doi.org/10.3390/nu13113740
Farag MA, Hamouda S, Gomaa S, Agboluaje AA, Hariri MLM, Yousof SM. Dietary Micronutrients from Zygote to Senility: Updated Review of Minerals’ Role and Orchestration in Human Nutrition throughout Life Cycle with Sex Differences. Nutrients. 2021; 13(11):3740. https://doi.org/10.3390/nu13113740
Chicago/Turabian StyleFarag, Mohamed A., Samia Hamouda, Suzan Gomaa, Aishat A. Agboluaje, Mohamad Louai M. Hariri, and Shimaa Mohammad Yousof. 2021. "Dietary Micronutrients from Zygote to Senility: Updated Review of Minerals’ Role and Orchestration in Human Nutrition throughout Life Cycle with Sex Differences" Nutrients 13, no. 11: 3740. https://doi.org/10.3390/nu13113740
APA StyleFarag, M. A., Hamouda, S., Gomaa, S., Agboluaje, A. A., Hariri, M. L. M., & Yousof, S. M. (2021). Dietary Micronutrients from Zygote to Senility: Updated Review of Minerals’ Role and Orchestration in Human Nutrition throughout Life Cycle with Sex Differences. Nutrients, 13(11), 3740. https://doi.org/10.3390/nu13113740