
Effects of Peanut Protein Supplementation on Resistance Training Adaptations in Younger Adults


 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Ethical Approval and Participant Inclusion Criteria
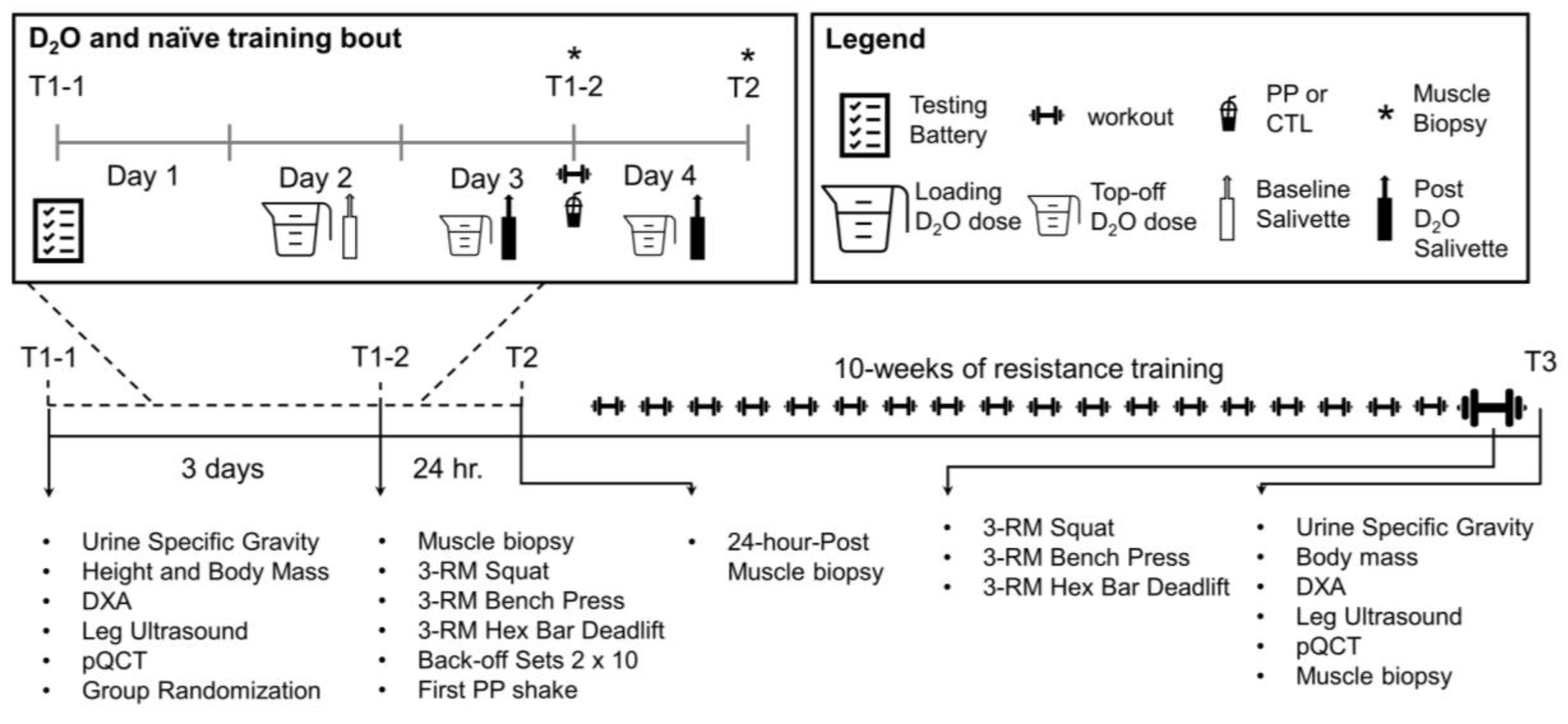
2.2. Study Design
2.3. Specific Testing Procedures
2.3.1. Urine Specific Gravity
2.3.2. Body Composition
2.3.3. Peripheral Quantitative Computed Tomography
2.3.4. Ultrasound
2.3.5. Isokinetic Dynamometry
2.3.6. Strength Testing
2.4. Skeletal Muscle Biopsies
2.5. Resistance Training Protocol and PP Supplementation
- (i)
- A general warm-up of 25 jumping jacks and 10 body weight squats,
- (ii)
- A specific warm-up of 1 set of 10 reps at 50% of working weight, 1 set of 5 repetitions at 75% of working weight, and 1 set of 3 repetitions of 90% of working weight,
- (iii)
- Either 4 sets of 10 repetitions, or 5 sets of 6 reps per exercise
2.6. Wet Laboratory Analyses
2.7. Food Log Analysis
3. Statistical Analysis
4. Results
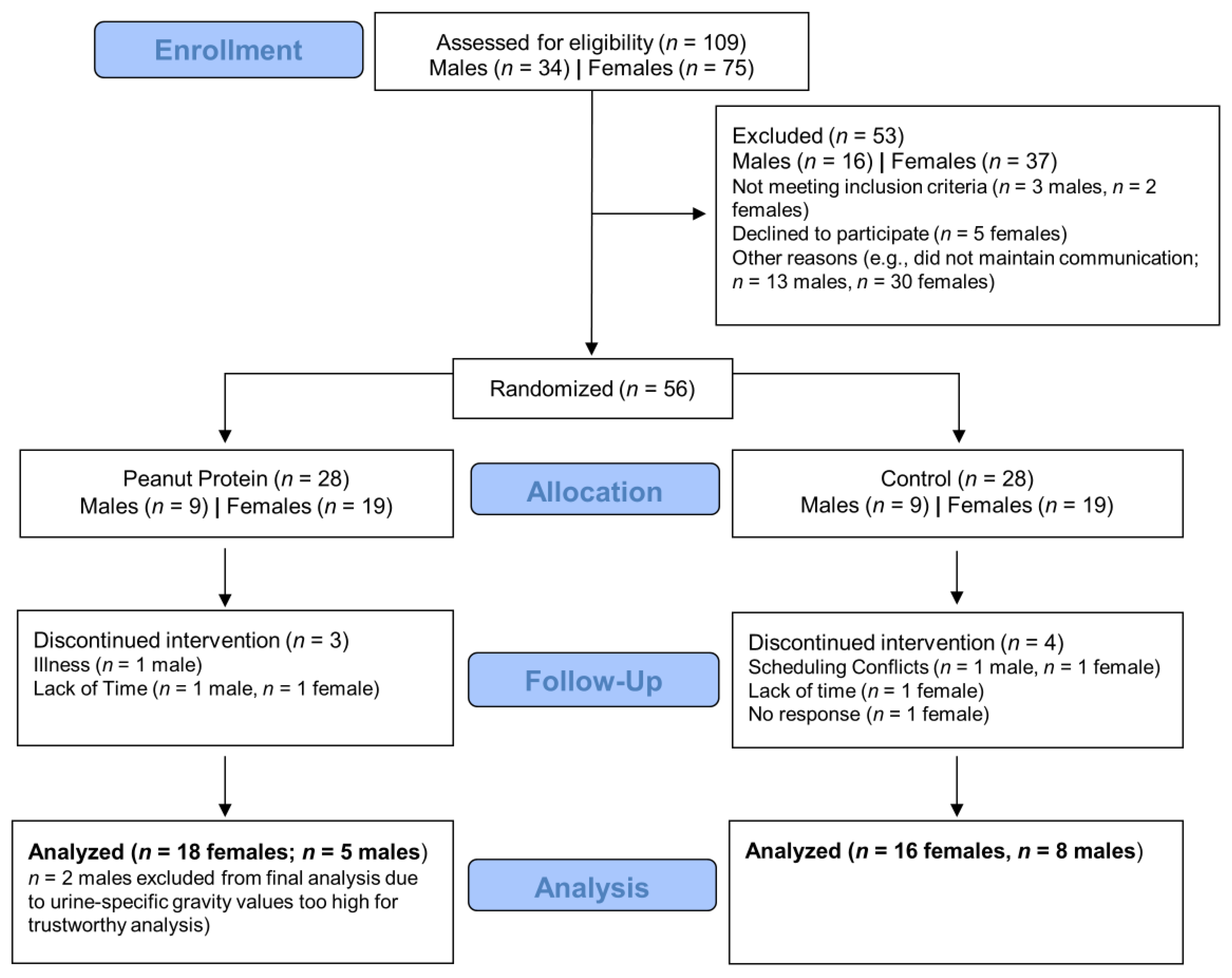
4.1. Consort Diagram
4.2. Baseline Participant Characteristics
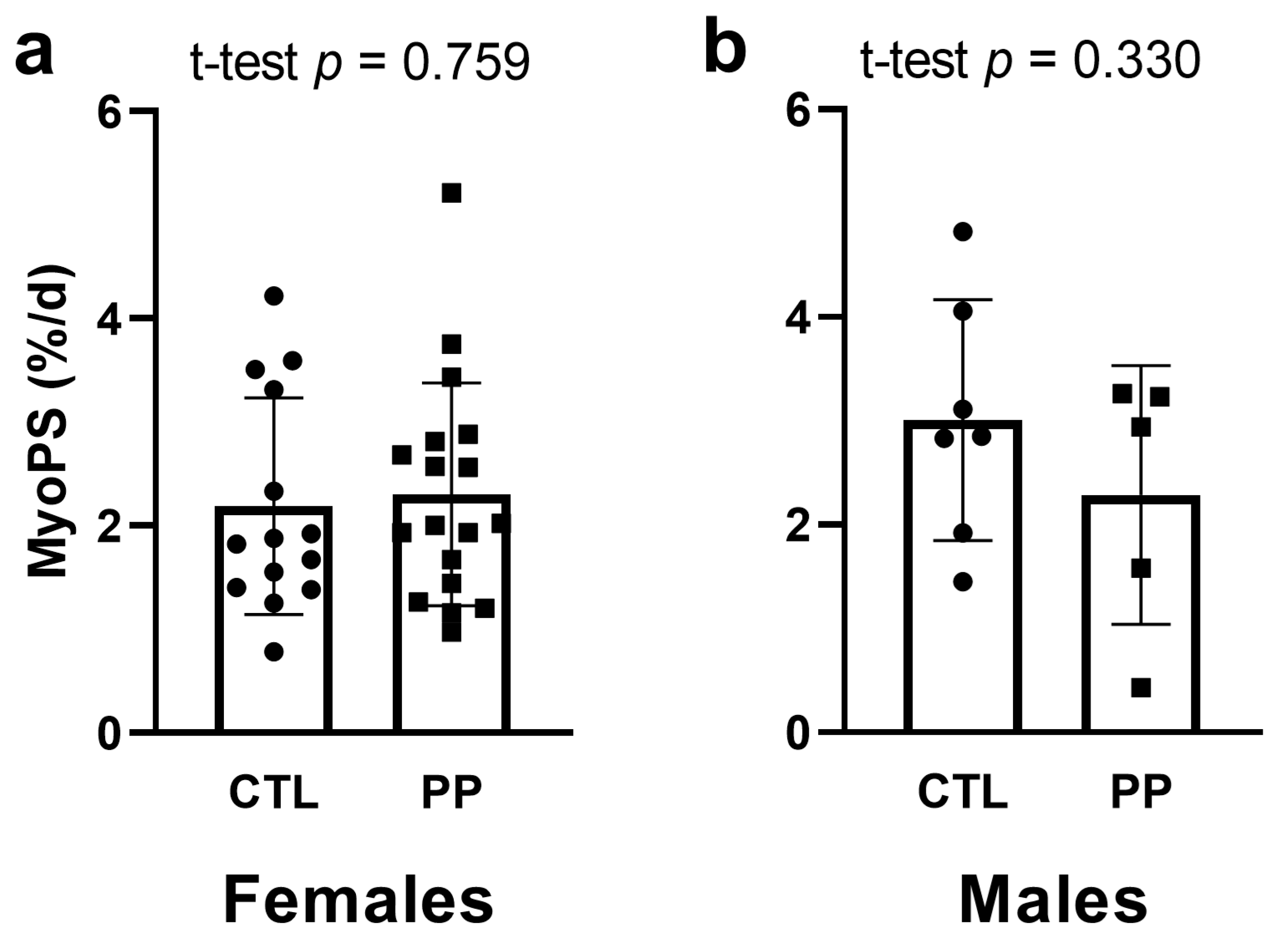
4.3. MyoPS Response to First Bout of Training
4.4. Nutritional Intakes Prior to and at the End of the 10-Week Intervention
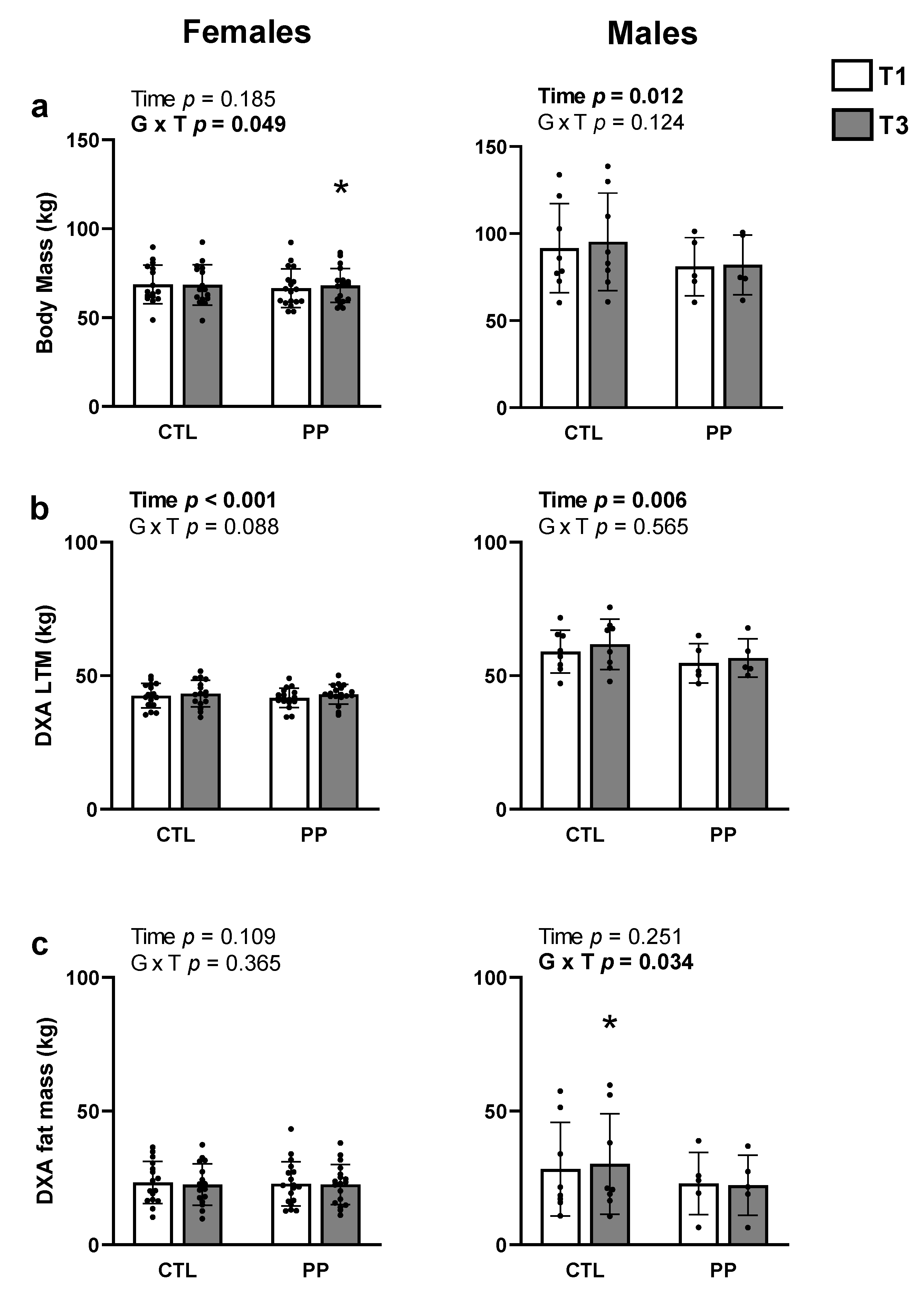
4.5. Body Composition Changes with Training in PP versus CTL
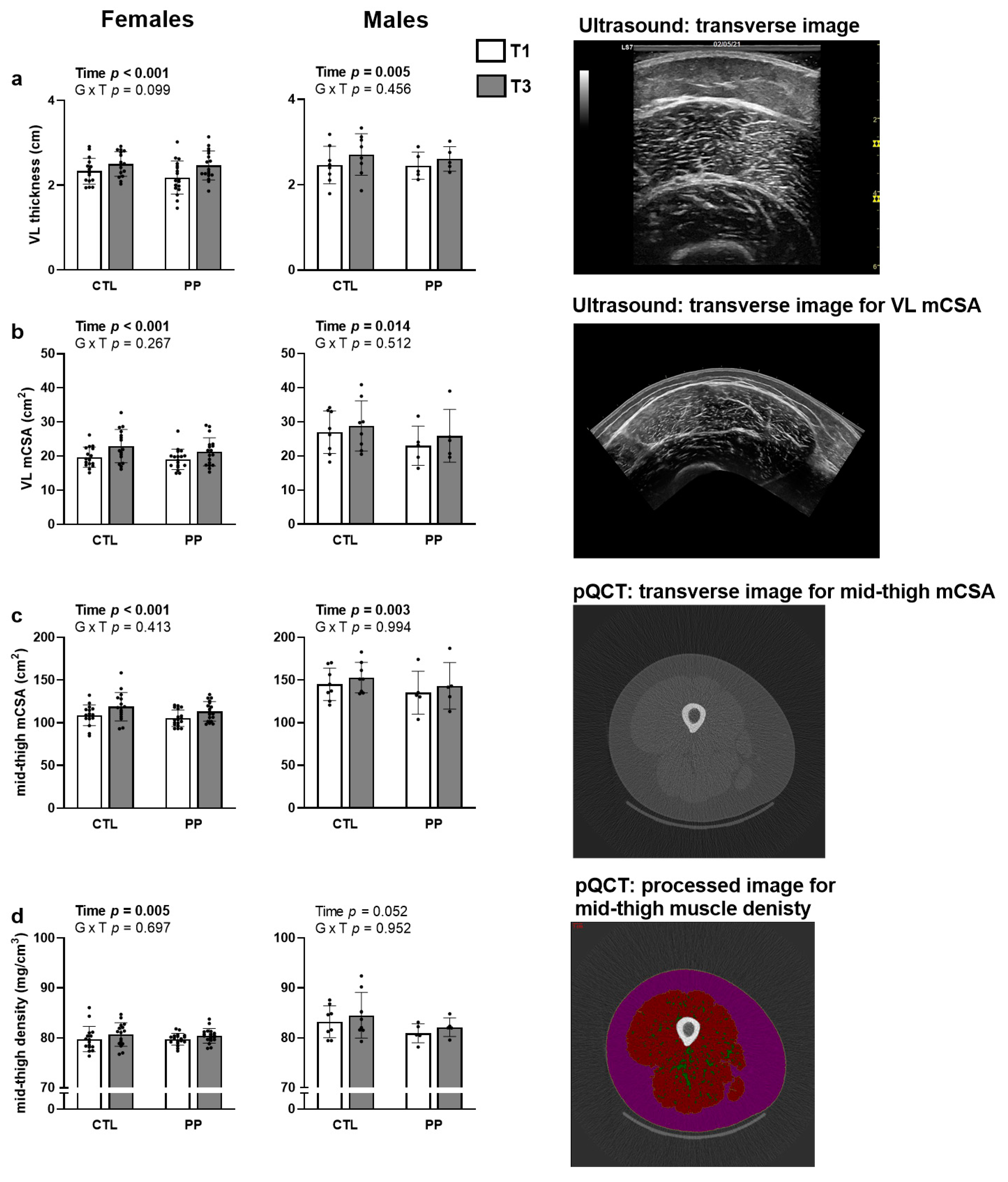
4.6. Mid-Thigh Characteristics with Training in PP versus CTL
4.7. Total Training Volume and Strength Adaptations with Training in PP versus CTL
4.8. Muscle Fiber Adaptations with Training in PP versus CTL in Female Participants
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Phillips, S.M.; Chevalier, S.; Leidy, H.J. Protein “requirements” beyond the RDA: Implications for optimizing health. Appl. Physiol. Nutr. Metab. 2016, 41, 565–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, R.R.; Cifelli, A.M.; Kostas, G.; Kim, I.Y. Optimizing Protein Intake in Adults: Interpretation and Application of the Recommended Dietary Allowance Compared with the Acceptable Macronutrient Distribution Range. Adv. Nutr. 2017, 8, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.E.; Alexander, D.D.; Perez, V. Effects of whey protein and resistance exercise on body composition: A meta-analysis of randomized controlled trials. J. Am. Coll. Nutr. 2014, 33, 163–175. [Google Scholar] [CrossRef]
- Moore, J.; McClain, A.; Hong, M.Y. Dietary Supplement Use in the United States: Prevalence, Trends, Pros, and Cons. Nutr. Today 2020, 55, 174–181. [Google Scholar] [CrossRef]
- Mobley, C.B.; Haun, C.T.; Roberson, P.A.; Mumford, P.W.; Romero, M.A.; Kephart, W.C.; Anderson, R.G.; Vann, C.G.; Osburn, S.C.; Pledge, C.D.; et al. Effects of Whey, Soy or Leucine Supplementation with 12 Weeks of Resistance Training on Strength, Body Composition, and Skeletal Muscle and Adipose Tissue Histological Attributes in College-Aged Males. Nutrients 2017, 9, 972. [Google Scholar] [CrossRef]
- Phillips, S.M.; Tang, J.E.; Moore, D.R. The role of milk- and soy-based protein in support of muscle protein synthesis and muscle protein accretion in young and elderly persons. J. Am. Coll. Nutr. 2009, 28, 343–354. [Google Scholar] [CrossRef]
- Norton, L.E.; Layman, D.K.; Bunpo, P.; Anthony, T.G.; Brana, D.V.; Garlick, P.J. The leucine content of a complete meal directs peak activation but not duration of skeletal muscle protein synthesis and mammalian target of rapamycin signaling in rats. J. Nutr. 2009, 139, 1103–1109. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.E.; Moore, D.R.; Kujbida, G.W.; Tarnopolsky, M.A.; Phillips, S.M. Ingestion of whey hydrolysate, casein, or soy protein isolate: Effects on mixed muscle protein synthesis at rest and following resistance exercise in young men. J. Appl. Physiol. 2009, 107, 987–992. [Google Scholar] [CrossRef]
- Nelson, M.E.; Hamm, M.W.; Hu, F.B.; Abrams, S.A.; Griffin, T.S. Alignment of Healthy Dietary Patterns and Environmental Sustainability: A Systematic Review. Adv. Nutr. 2016, 7, 1005–1025. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef]
- De Boer, J.; Aiking, H. Prospects for pro-environmental protein consumption in Europe: Cultural, culinary, economic and psychological factors. Appetite 2018, 121, 29–40. [Google Scholar] [CrossRef]
- Lim, M.T.; Pan, B.J.; Toh, D.W.K.; Sutanto, C.N.; Kim, J.E. Animal Protein versus Plant Protein in Supporting Lean Mass and Muscle Strength: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 661. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Jagim, A.; Hagele, A.; Jager, R. Plant Proteins and Exercise: What Role Can Plant Proteins Have in Promoting Adaptations to Exercise? Nutrients 2021, 13, 1962. [Google Scholar] [CrossRef]
- Pinckaers, P.J.M.; Trommelen, J.; Snijders, T.; van Loon, L.J.C. The Anabolic Response to Plant-Based Protein Ingestion. Sports Med. 2021. [Google Scholar] [CrossRef]
- Arya, S.S.; Salve, A.R.; Chauhan, S. Peanuts as functional food: A review. J. Food Sci. Technol. 2016, 53, 31–41. [Google Scholar] [CrossRef] [Green Version]
- Hughes, G.J.; Ryan, D.J.; Mukherjea, R.; Schasteen, C.S. Protein digestibility-corrected amino acid scores (PDCAAS) for soy protein isolates and concentrate: Criteria for evaluation. J. Agric. Food Chem. 2011, 59, 12707–12712. [Google Scholar] [CrossRef]
- Lamb, D.A.; Moore, J.H.; Smith, M.A.; Vann, C.G.; Osburn, S.C.; Ruple, B.A.; Fox, C.D.; Smith, K.S.; Altonji, O.M.; Power, Z.M.; et al. The effects of resistance training with or without peanut protein supplementation on skeletal muscle and strength adaptations in older individuals. J. Int. Soc. Sports Nutr. 2020, 17, 66. [Google Scholar] [CrossRef]
- Schaafsma, G. The protein digestibility-corrected amino acid score (PDCAAS)-A concept for describing protein quality in foods and food ingredients: A critical review. J. Aoac. Int. 2005, 88, 988–994. [Google Scholar] [CrossRef] [Green Version]
- Rantalainen, T.; Nikander, R.; Heinonen, A.; Daly, R.M.; Sievanen, H. An open source approach for regional cortical bone mineral density analysis. J. Musculoskelet. Neuronal. Interact. 2011, 11, 243–248. [Google Scholar]
- Evans, W.J.; Phinney, S.D.; Young, V.R. Suction applied to a muscle biopsy maximizes sample size. Med. Sci. Sports Exerc. 1982, 14, 101–102. [Google Scholar]
- Vann, C.G.; Haun, C.T.; Osburn, S.C.; Romero, M.A.; Roberson, P.A.; Mumford, P.W.; Mobley, C.B.; Holmes, H.M.; Fox, C.D.; Young, K.C.; et al. Molecular Differences in Skeletal Muscle After 1 Week of Active vs. Passive Recovery From High-Volume Resistance Training. J. Strength Cond. Res. 2021, 35, 2102–2113. [Google Scholar] [CrossRef]
- Roberts, M.D.; Young, K.C.; Fox, C.D.; Vann, C.G.; Roberson, P.A.; Osburn, S.C.; Moore, J.H.; Mumford, P.W.; Romero, M.A.; Beck, D.T.; et al. An optimized procedure for isolation of rodent and human skeletal muscle sarcoplasmic and myofibrillar proteins. J. Biol. Methods 2020, 7, e127. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.E.; Brook, M.S.; Snijders, T.; Kumbhare, D.; Parise, G.; Smith, K.; Atherton, P.J.; Phillips, S.M. Integrated Myofibrillar Protein Synthesis in Recovery From Unaccustomed and Accustomed Resistance Exercise With and Without Multi-ingredient Supplementation in Overweight Older Men. Front. Nutr. 2019, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- McAdam, J.S.; McGinnis, K.D.; Beck, D.T.; Haun, C.T.; Romero, M.A.; Mumford, P.W.; Roberson, P.A.; Young, K.C.; Lohse, K.R.; Lockwood, C.M.; et al. Effect of Whey Protein Supplementation on Physical Performance and Body Composition in Army Initial Entry Training Soldiers. Nutrients 2018, 10, 1248. [Google Scholar] [CrossRef] [Green Version]
- Davies, R.W.; Bass, J.J.; Carson, B.P.; Norton, C.; Kozior, M.; Amigo-Benavent, M.; Wilkinson, D.J.; Brook, M.S.; Atherton, P.J.; Smith, K.; et al. Differential Stimulation of Post-Exercise Myofibrillar Protein Synthesis in Humans Following Isonitrogenous, Isocaloric Pre-Exercise Feeding. Nutrients 2019, 11, 1657. [Google Scholar] [CrossRef] [Green Version]
- Witard, O.C.; Jackman, S.R.; Breen, L.; Smith, K.; Selby, A.; Tipton, K.D. Myofibrillar muscle protein synthesis rates subsequent to a meal in response to increasing doses of whey protein at rest and after resistance exercise. Am. J. Clin. Nutr. 2014, 99, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Moore, D.R.; Robinson, M.J.; Fry, J.L.; Tang, J.E.; Glover, E.I.; Wilkinson, S.B.; Prior, T.; Tarnopolsky, M.A.; Phillips, S.M. Ingested protein dose response of muscle and albumin protein synthesis after resistance exercise in young men. Am. J. Clin. Nutr. 2009, 89, 161–168. [Google Scholar] [CrossRef]
- Volek, J.S.; Volk, B.M.; Gomez, A.L.; Kunces, L.J.; Kupchak, B.R.; Freidenreich, D.J.; Aristizabal, J.C.; Saenz, C.; Dunn-Lewis, C.; Ballard, K.D.; et al. Whey protein supplementation during resistance training augments lean body mass. J. Am. Coll. Nutr. 2013, 32, 122–135. [Google Scholar] [CrossRef]
- Hulmi, J.J.; Lockwood, C.M.; Stout, J.R. Effect of protein/essential amino acids and resistance training on skeletal muscle hypertrophy: A case for whey protein. Nutr. Metab. 2010, 7, 51. [Google Scholar] [CrossRef] [Green Version]
- Hector, A.J.; Phillips, S.M. Protein Recommendations for Weight Loss in Elite Athletes: A Focus on Body Composition and Performance. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 170–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Amount Per Daily Serving (3 Scoops or 75 g Powder) |
|---|---|
| Total protein 1 | 30.1 g |
| Essential 2 | |
| Histidine | 0.72 g |
| Isoleucine | 1.14 g |
| Leucine | 2.17 g |
| Lysine | 0.87 g |
| Methionine | 0.41 g |
| Phenylalanine | 1.66 g |
| Threonine | 0.86 g |
| Tryptophan | ND |
| Valine | 1.37 g |
| Total essential | 9.2 g |
| Non-essential | |
| Alanine | 1.37 g |
| Arginine | 3.71 g |
| Asparagine | 3.77 g |
| Cysteine | 0.45 g |
| Glutamic acid | 6.26 g |
| Glycine | 1.90 g |
| Proline | 1.37 g |
| Serine | 1.49 g |
| Tyrosine | 1.35 g |
| Total non-essential | 21.7 g |
| Variable | PP | CTL | p-Value |
|---|---|---|---|
| Females | |||
| Age (years) | 22 ± 2 | 21 ± 1 | 0.611 |
| Height (cm) | 171 ± 5 | 169 ± 5 | 0.176 |
| Body mass (kg) | 66.6 ± 10.8 | 68.7 ± 10.9 | 0.565 |
| DXA FM (kg) | 22.8 ± 8.3 | 23.2 ± 7.9 | 0.863 |
| DXA LTM (kg) | 41.7 ± 3.6 | 42.6 ± 4.6 | 0.529 |
| VL thickness (cm) | 2.18 ± 0.39 | 2.33 ± 0.30 | 0.229 |
| Males | |||
| Age (years) | 21 ± 2 | 21 ± 1 | 0.304 |
| Height (cm) | 177 ± 7 | 180 ± 8 | 0.506 |
| Body mass (kg) | 76.0 ± 14.2 | 91.6 ± 25.5 | 0.431 |
| DXA FM (kg) | 18.9 ± 8.7 | 28.3 ± 17.5 | 0.555 |
| DXA LTM (kg) | 53.5 ± 7.9 | 61.8 ± 9.5 | 0.347 |
| VL thickness (cm) | 2.39 ± 0.34 | 2.71 ± 0.49 | 0.948 |
| Variable | Group | T1 | T3 (Includes PP) |
|---|---|---|---|
| Females | |||
| Energy intake (kcal/d) | PP CTL | 1495 ± 430 1419 ± 458 | 1607 ± 513 1359 ± 327 |
| Fat intake (g/d) | PP CTL | 68 ± 19 59 ± 18 | 66 ± 25 60 ± 16 |
| Carbohydrate intake (g/d) | PP CTL | 152 ± 61 163 ± 83 | 167 ± 65 151 ± 45 |
| Protein intake (g/d) | PP CTL | 69 ± 29 a 60 ± 25 | 91 ± 23 b,c 51 ± 15 |
| Protein intake (g/kg body mass/d) | PP CTL | 1.02 ± 0.40 0.87 ± 0.32 | 1.36 ± 0.37 b,c 0.87 ± 0.27 |
| Males | |||
| Energy intake (kcal/d) | PP CTL | 2262 ± 766 1727 ± 656 | 2433 ± 685 1298 ± 324 |
| Fat intake (g/d) | PP CTL | 110 ± 29 83 ± 44 | 100 ± 32 53 ± 16 |
| Carbohydrate intake (g/d) | PP CTL | 197 ± 108 156 ± 80 | 245 ± 70 130 ± 37 |
| Protein intake (g/d) | PP CTL | 118 ± 38 90 ± 41 | 128 ± 17 74 ± 22 |
| Protein intake (g/kg body mass/d) | PP CTL | 1.62 ± 0.83 1.06 ± 0.53 | 1.68 ± 0.36 0.87 ± 0.43 |
| Week | Day | Sets × Repetitions | %1RM |
|---|---|---|---|
| 1 | 1 | 3-RM Testing (+2 × 10) | 50% |
| 2 | 5 × 6 | 56% | |
| 2 | 3 | 4 × 10 | 55% |
| 4 | 5 × 6 | 65% | |
| 3 | 5 | 4 × 10 | 60% |
| 6 | 5 × 6 | 74% | |
| 4 | 7 | 4 × 10 | 65% |
| 8 | 5 × 6 | 84% | |
| 5 | 9 | 4 × 10 | 50% |
| 10 | 5 × 6 | 50% | |
| 6 | 11 | 4 × 10 | 65% |
| 12 | 5 × 6 | 84% | |
| 7 | 13 | 4 × 10 | 70% |
| 14 | 5 × 6 | 90% | |
| 8 | 15 | 4 × 10 | 75% |
| 16 | 5 × 6 | 96% | |
| 9 | 17 | 4 × 10 | 80% |
| 18 | 5 × 6 | 98% | |
| 10 | 19 | 5 × 6 | 102% |
| 20 | 3-RM Testing | --- |
| Variable | Group | T1 | T3 |
|---|---|---|---|
| Females | |||
| Leg press 1RM (kg) | PP CTL | 79 ± 39 88 ± 39 | 160 ± 41 177 ± 55 |
| Bench press 1RM (kg) | PP CTL | 31 ± 6 32 ± 7 | 38 ± 6 41 ± 8 |
| Deadlift 1RM (kg) | PP CTL | 59 ± 14 62 ± 15 | 82 ± 19 88 ± 18 |
| Leg extensor peak torque (N × m) | PP CTL | 129 ± 32 141 ± 30 | 135 ± 38 155 ± 33 |
| Total training volume (kg) | PP CTL | 131,728 ± 27,867 137,228 ± 29,098 | |
| Males | |||
| Leg press 1RM (kg) | PP CTL | 152 ± 41 214 ± 53 | 260 ± 105 366 ± 87 |
| Bench press 1RM (kg) | PP CTL | 69 ± 19 74 ± 20 | 80 ± 19 83 ± 19 |
| Deadlift 1RM (kg) | PP CTL | 102 ± 31 111 ± 16 | 125 ± 38 151 ± 23 |
| Leg extensor peak torque (N × m) | PP CTL | 174 ± 30 184 ± 36 | 171 ± 37 225 ± 42 * |
| Total training volume (kg) | PP CTL | 280,345 ± 116,800 312,335 ± 152,903 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sexton, C.L.; Smith, M.A.; Smith, K.S.; Osburn, S.C.; Godwin, J.S.; Ruple, B.A.; Hendricks, A.M.; Mobley, C.B.; Goodlett, M.D.; Frugé, A.D.; et al. Effects of Peanut Protein Supplementation on Resistance Training Adaptations in Younger Adults. Nutrients 2021, 13, 3981. https://doi.org/10.3390/nu13113981
Sexton CL, Smith MA, Smith KS, Osburn SC, Godwin JS, Ruple BA, Hendricks AM, Mobley CB, Goodlett MD, Frugé AD, et al. Effects of Peanut Protein Supplementation on Resistance Training Adaptations in Younger Adults. Nutrients. 2021; 13(11):3981. https://doi.org/10.3390/nu13113981
Chicago/Turabian StyleSexton, Casey L., Morgan A. Smith, Kristen S. Smith, Shelby C. Osburn, Joshua S. Godwin, Bradley A. Ruple, Alex M. Hendricks, Christopher B. Mobley, Michael D. Goodlett, Andrew D. Frugé, and et al. 2021. "Effects of Peanut Protein Supplementation on Resistance Training Adaptations in Younger Adults" Nutrients 13, no. 11: 3981. https://doi.org/10.3390/nu13113981
APA StyleSexton, C. L., Smith, M. A., Smith, K. S., Osburn, S. C., Godwin, J. S., Ruple, B. A., Hendricks, A. M., Mobley, C. B., Goodlett, M. D., Frugé, A. D., Young, K. C., & Roberts, M. D. (2021). Effects of Peanut Protein Supplementation on Resistance Training Adaptations in Younger Adults. Nutrients, 13(11), 3981. https://doi.org/10.3390/nu13113981