
Maternal Vitamin D Status and Gestational Weight Gain as Correlates of Neonatal Bone Mass in Healthy Term Breastfed Young Infants from Montreal, Canada

 , ,
, ,
Abstract
:1. Introduction
2. Methods
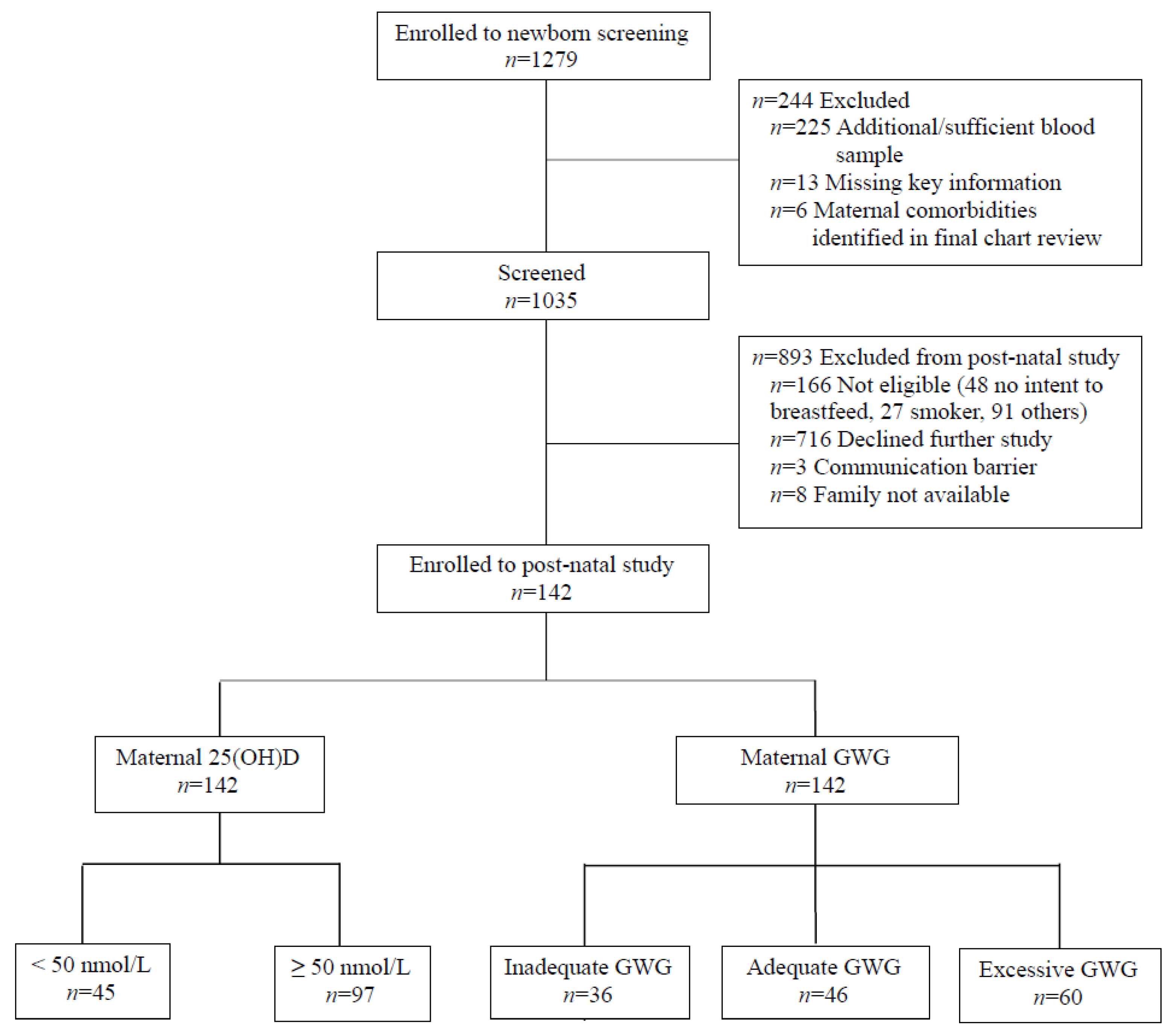
2.1. Sample and Study Design
2.2. Obstetric History, Anthropometric, and Demographic Data
2.3. Dietary Intake, Multivitamin Use, and Physical Activity
2.4. Serum 25(OH)D Concentration
2.5. Bone Outcomes
2.6. Ethical Approval
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baird, J.; Kurshid, M.A.; Kim, M.; Harvey, N.; Dennison, E.; Cooper, C. Does birthweight predict bone mass in adulthood? A systematic review and meta-analysis. Osteoporos. Int. 2011, 22, 1323–1334. [Google Scholar] [CrossRef]
- Orwoll, E.S.; Belknap, J.K.; Klein, R.F. Gender specificity in the genetic determinants of peak bone mass. J. Bone Miner. Res. 2001, 16, 1962–1971. [Google Scholar] [CrossRef]
- Dennison, E.; Cooper, C.; Cole, Z. Early development and osteoporosis and bone health. J. Dev. Orig. Health Dis. 2010, 1, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Steer, C.D.; Tobias, J.H. Insights into the programming of bone development from the Avon Longitudinal Study of Parents and Children (ALSPAC). Am. J. Clin. Nutr. 2011, 94, 1861S–1864S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godfrey, K.; Walker-Bone, K.; Robinson, S.; Taylor, P.; Shore, S.; Wheeler, T.; Cooper, C. Neonatal bone mass: Influence of parental birthweight, maternal smoking, body composition, and activity during pregnancy. J. Bone Miner. Res. 2001, 16, 1694–1703. [Google Scholar] [CrossRef]
- Keiver, K.; Weinberg, J. Effect of duration of maternal alcohol consumption on calcium metabolism and bone in the fetal rat. Alcohol Clin. Exp. Res. 2004, 28, 456–467. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288.e4. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.B.; Strøm, M.; Maslova, E.; Granström, C.; Vestergaard, P.; Mølgaard, C.; Olsen, S.F. Predicted vitamin D status during pregnancy in relation to offspring forearm fractures in childhood: A study from the Danish National Birth Cohort. Br. J. Nutr. 2015, 114, 1900–1908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, R.J.; Curtis, E.M.; Woolford, S.J.; Ashai, S.; Cooper, C.; Harvey, N.C. The importance of maternal pregnancy vitamin D for offspring bone health: Learnings from the MAVIDOS trial. Ther. Adv. Musculoskelet Dis. 2021, 13, 1759720X211006979. [Google Scholar] [CrossRef]
- Viljakainen, H.T.; Saarnio, E.; Hytinantti, T.; Miettinen, M.; Surcel, H.; Makitie, O.; Andersson, S.; Laitinen, K.; Lamberg-Allardt, C. Maternal vitamin D status determines bone variables in the newborn. J. Clin. Endocrinol. Metab. 2010, 95, 1749–1757. [Google Scholar] [CrossRef] [Green Version]
- Weiler, H.; Fitzpatrick-Wong, S.; Veitch, R.; Kovacs, H.; Schellenberg, J.; McCloy, U.; Yuen, C.K. Vitamin D deficiency and whole-body and femur bone mass relative to weight in healthy newborns. Can. Med. Assoc. J. 2005, 172, 757–761. [Google Scholar] [CrossRef] [Green Version]
- Mahon, P.; Harvey, N.; Crozier, S.; Inskip, H.; Robinson, S.; Arden, N.; Swaminathan, R.; Cooper, C.; Godfrey, K.; SWS Study Group. Low maternal vitamin D status and fetal bone development: Cohort study. J. Bone Miner. Res. 2010, 25, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawlor, D.A.; Wills, A.K.; Fraser, A.; Sayers, A.; Fraser, W.D.; Tobias, J.H. Association of maternal vitamin D status during pregnancy with bone-mineral content in offspring: A prospective cohort study. Lancet 2013, 381, 2176–2183. [Google Scholar] [CrossRef] [Green Version]
- Monjardino, T.; Henriques, A.; Moreira, C.; Rodrigues, T.; Adubeiro, N.; Nogueira, L.; Cooper, C.; Santos, A.C.; Lucas, R. Gestational weight gain and offspring bone mass: Different associations in healthy weight versus overweight women. J. Bone Miner. Res. 2019, 34, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, K.M.; Catalano, P.M.; Yaktine, A.L. New guidelines for weight gain during pregnancy: What obstetrician/gynecologists should know. Curr. Opin. Obstet. 2009, 21, 521. [Google Scholar] [CrossRef] [Green Version]
- Macdonald-Wallis, C.; Tobias, J.H.; Smith, G.D.; Lawlor, D.A. Relation of maternal prepregnancy body mass index with offspring bone mass in childhood: Is there evidence for an intrauterine effect? Am. J. Clin. Nutr. 2010, 92, 872–880. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, J.; Koes, B.W.; Paulis, W.D.; van Middelkoop, M. Differences in bone mineral density between normal-weight children and children with overweight and obesity: A systematic review and meta-analysis. Obes Rev. 2017, 18, 526–546. [Google Scholar] [CrossRef] [PubMed]
- Savvidis, C.; Tournis, S.; Dede, A.D. Obesity and bone metabolism. Hormones 2018, 17, 205–217. [Google Scholar] [CrossRef]
- Moon, R.J.; Harvey, N.C.; Cooper, C.; D’Angelo, S.; Crozier, S.R.; Inskip, H.M.; Shoenmakers, I.; Prentice, A.; Arden, N.K.; Bishop, N.J.; et al. Determinants of the maternal 25-hydroxyvitamin D response to vitamin D supplementation during pregnancy. J. Clin. Endocrinol. Metab. 2016, 101, 5012–5020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiely, M.; Hemmingway, A.; O’Callaghan, K.M. Vitamin D in pregnancy: Current perspectives and future directions. Ther. Adv. Musculoskelet Dis. 2017, 9, 145–154. [Google Scholar] [CrossRef]
- Aghajafari, F.; Field, C.J.; Kaplan, B.J.; Maggiore, J.A.; O’Beirne, M.; Hanley, D.A.; Eliasziw, M.; Dewey, D.; Ross, S.; Rabi, D.; et al. The high prevalence of vitamin D insufficiency in cord blood in Calgary, Alberta (APrON-D Study). J. Obstet. Gynaecol. Can. 2017, 39, 347–353.e1. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, C.G.; Giguère, Y.; Weiler, H.A.; Spencer, A.; Forest, J.-C.; Armson, B.A.; Dodds, L. Determinants of vitamin D status in pregnant women and neonates. Can. J. Public Health 2016, 107, e410–e416. [Google Scholar] [CrossRef] [Green Version]
- Ioannou, C.; Javaid, M.K.; Mahon, P.; Yaqub, M.; Harvey, N.C.; Godfrey, K.M.; Noble, J.A.; Cooper, C.; Papageorghiou, A.T. The Effect of Maternal Vitamin D Concentration on Fetal Bone. J. Clin. Endocrinol. Metab. 2012, 97, E2070–E2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viljakainen, H.; Korhonen, T.; Hytinantti, T.; Laitinen, E.K.A.; Andersson, S.; Mäkitie, O.; Lamberg-Allardt, C. Maternal vitamin D status affects bone growth in early childhood—A prospective cohort study. Osteoporos Int. 2011, 22, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Javaid, M.; Crozier, S.; Harvey, N.; Gale, C.; Dennison, E.; Boucher, B.J.; Arden, N.; Godfrey, K.; Cooper, C. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. Lancet 2006, 367, 36–43. [Google Scholar] [CrossRef]
- Zhu, K.; Whitehouse, A.J.O.; Hart, P.H.; Kusel, M.; Mountain, J.; Lye, S.; Pennell, C.; Walsh, J.P. Maternal vitamin D status during pregnancy and bone mass in offspring at 20 years of age: A prospective cohort study. J. Bone Miner. Res. 2014, 29, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.; Cooper, C. Vitamin D: Some perspective please. BMJ 2012, 19, e4695. [Google Scholar] [CrossRef] [PubMed]
- Akcakus, M.; Koklu, E.; Budak, N.; Kula, M.; Kurtoglu, S.; Koklu, S. The relationship between birthweight, 25-hydroxyvitamin D concentrations and bone mineral status in neonates. Ann. Trop. Paediatr. 2006, 26, 267–275. [Google Scholar] [CrossRef]
- Dror, D.K.; King, J.C.; Fung, E.B.; Loan, M.D.V.; Gertz, E.R.; Allen, L.H. Evidence of associations between feto-maternal vitamin D status, cord parathyroid hormone and bone-specific alkaline phosphatase, and newborn whole body bone mineral content. Nutrients 2012, 4, 68–77. [Google Scholar] [CrossRef]
- Prentice, A.; Jarjou, L.M.; Goldberg, G.R.; Bennett, J.; Cole, T.J.; Schoenmakers, I. Maternal plasma 25-hydroxyvitamin D concentration and birthweight, growth and bone mineral accretion of Gambian infants. Acta Paediatr. 2009, 98, 1360. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Harvey, N.C.; Bishop, N.J.; Kennedy, S.; Papageorghiou, A.T.; Schoenmakers, I.; Fraser, R.; Gandhi, S.V.; Carr, A.; D’Angelo, S.; et al. Maternal gestational vitamin D supplementation and offspring bone health (MAVIDOS): A multicentre, double-blind, randomised placebo-controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 393–402. [Google Scholar] [CrossRef] [Green Version]
- Canadian Institute for Health Information. Proposed Standards for Race-Based and Indigenous Identity Data. 2020. Available online: https://www.cihi.ca/en/proposed-standards-for-race-based-and-indigenous-identity-data (accessed on 22 January 2021).
- Statistics Canada. Market Income, Government Transfers, Total Income, Income Tax and After-Tax Income by Economic Family Type. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1110019001 (accessed on 8 March 2021).
- Greeley, S.; Storbakken, L.; Magel, R. Use of a modified food frequency questionnaire during pregnancy. J Am Coll Nutr. 1992, 11, 728–734. [Google Scholar] [CrossRef]
- Tobias, J.H.; Steer, C.D.; Emmett, P.; Tonkin, R.J.; Cooper, C.; Ness, A. Bone mass in childhood is related to maternal diet in pregnancy. Osteoporos. Int. 2005, 16, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- Masztalerz-Kozubek, D.; Zielinska-Pukos, M.A.; Hamulka, J. Maternal Diet, nutritional status, and birth-related factors influencing offspring’s bone mineral density: A narrative review of observational, cohort, and randomized controlled trials. Nutrients 2021, 13, 2302. [Google Scholar] [CrossRef]
- Binkley, N.; Sempos, C.T.; Program, V.D.S. Standardizing vitamin D assays: The way forward. J. Bone Miner. Res. 2014, 29, 1709–1714. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.C.; Manson, J.E.; Abrams, S.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.; Jones, G.; et al. The 2011 dietary reference intakes for calcium and vitamin D: What dietetics practitioners need to know. J. Am. Diet. Assoc. 2011, 111, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Baim, S.; Binkley, N.; Bilezikian, J.P.; Kendler, D.; Hans, D.B.; Lewiecki, E.M.; Silverman, S. Official positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Position Development Conference. J. Clin. Densitom. 2008, 11, 75–91. [Google Scholar] [CrossRef]
- Harvey, N.; Javaid, M.; Poole, J.R.; Taylor, P.; Robinson, S.; Inskip, H.; Godfrey, K.; Cooper, C.; Dennison, E. Paternal skeletal size predicts intrauterine bone mineral accrual. J. Clin. Endocrinol. Metab. 2008, 93, 1676–1681. [Google Scholar] [CrossRef] [Green Version]
- Kurl, S.; Heinonen, K.; Jurvelin, J.S.; Länsimies, E. Lumbar bone mineral content and density measured using a Lunar DPX densitometer in healthy full-term infants during the first year of life. Clin. Physiol. Funct. Imaging. 2002, 22, 222–225. [Google Scholar] [CrossRef]
- Gallo, S.; Vanstone, C.A.; Weiler, H.A. Normative data for bone mass in healthy term infants from birth to 1 year of age. J Osteoporos. 2012, 2012, 672403. [Google Scholar] [CrossRef] [PubMed]
- Hillman, L.S. Bone mineral content in term infants fed human milk, cow milk-based formula, or soy-based formula. J. Pediatr. 1988, 113, 208–212. [Google Scholar] [CrossRef]
- Harvey, N.C.; Javaid, M.K.; Arden, N.K.; Poole, J.R.; Crozier, S.R.; Robinson, S.M.; Inskip, H.M.; Godfrey, K.M.; Dennison, E.M.; Cooper, C.; et al. Maternal predictors of neonatal bone size and geometry: The Southampton Women’s Survey. J. Dev. Orig. Health Dis. 2010, 1, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Rudäng, R.; Mellström, D.; Clark, E.; Ohlsson, C.; Lorentzon, M. Advancing maternal age is associated with lower bone mineral density in young adult male offspring. Osteoporos. Int. 2012, 23, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Mays, S.; Ives, R.; Brickley, M. The effects of socioeconomic status on endochondral and appositional bone growth, and acquisition of cortical bone in children from 19th century Birmingham, England. Am. J. Phys. Anthropol. 2009, 140, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Von Holle, A.; North, K.E.; Gahagan, S.; Burrows, R.A.; Blanco, E.; Lozoff, B.; Howard, A.G.; Justice, A.; Graff, M.; Voruganti, V.S. Sociodemographic predictors of early postnatal growth: Evidence from a Chilean infancy cohort. BMJ Open 2020, 10, e033695. [Google Scholar] [CrossRef]
- Clark, E.M.; Ness, A.; Tobias, J.H. Social position affects bone mass in childhood through opposing actions on height and weight. J. Bone Miner. Res. 2005, 20, 2082–2089. [Google Scholar] [CrossRef] [PubMed]
- Weiler, H.A.; Vanstone, C.A.; Razagji, M.; Gharibeh, N.; Patel, S.; Wei, S.Q.; McNally, D. Disparities in vitamin D status of newborn infants from a diverse sociodemographic population in Montreal, Canada. J. Nutr. 2021, nxab344. [Google Scholar] [CrossRef] [PubMed]
- Kalkwarf, H.J.; Abrams, S.A.; DiMeglio, L.A.; Koo, W.W.; Specker, B.L.; Weiler, H. Bone densitometry in infants and young children: The 2013 ISCD Pediatric Official Positions. J. Clin. Densitom. 2014, 17, 243–257. [Google Scholar] [CrossRef]
- McDowell, M.; Cain, M.A.; Brumley, J. Excessive gestational weight gain. J. Midwifery Women’s Health 2019, 64, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Balasubramanian, S. Vitamin D deficiency in breastfed infants & the need for routine vitamin D supplementation. Indian J. Med. Res. 2011, 133, 250. [Google Scholar]
- Dror, D.; King, J.; Durand, D.; Fung, E.; Allen, L. Feto-maternal vitamin D status and infant whole-body bone mineral content in the first weeks of life. Eur. J. Clin. Nutr. 2012, 66, 1016–1019. [Google Scholar] [CrossRef] [Green Version]
- Larqué, E.; Morales, E.; Leis, R.; Blanco-Carnero, J.E. Maternal and foetal health implications of vitamin D status during pregnancy. Ann. Nutr. Metab. 2018, 72, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Bone development in the fetus and neonate: Role of the calciotropic hormones. Curr. Osteoporos. Rep. 2011, 9, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S.; Kronenberg, H.M. Maternal-fetal calcium and bone metabolism during pregnancy, puerperium, and lactation. Endocr. Rev. 1997, 18, 832–872. [Google Scholar]
- Government of Canada. The Canadian Maternity Experiences Survey. Available online: https://www.canada.ca/en/public-health/services/injury-prevention/health-surveillance-epidemiology-division/maternal-infant-health/canadian-maternity-experiences-survey.html (accessed on 8 March 2021).
- Wagner, C.L.; McNeil, R.B.; Johnson, D.D.; Hulsey, T.C.; Ebeling, M.; Robinson, C.; Hamilton, S.A.; Hollis, B.W. Health characteristics and outcomes of two randomized vitamin D supplementation trials during pregnancy: A combined analysis. J Steroid Biochem. Mol. Biol. 2013, 136, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Gilmore, L.A.; Redman, L.M. Weight gain in pregnancy and application of the 2009 IOM guidelines: Toward a uniform approach. Obesity 2015, 23, 507–511. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Clinical Research Involving Children; Field, M.J.; Behrman, R.E. (Eds.) Ethical Conduct of Clinical Research Involving Children; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Turner, M.A. Clinical trials of medicines in neonates: The influence of ethical and practical issues on design and conduct. Br. J. Clin. Pharmacol. 2015, 79, 370–378. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal 25(OH)D (nmol/L) | Gestational Weight Gain | ||||||
|---|---|---|---|---|---|---|---|
| <50 (n = 45) | ≥50 (n = 97) | p-value | Inadequate (n = 36) | Adequate (n = 46) | Excessive (n = 60) | p-Value | |
| Infant | |||||||
| Sex, n (%) | 0.80 | 0.71 | |||||
| Male | 27 (19.0) | 56 (39.4) | 21 (14.8) | 29 (20.4) | 33 (23.2) | ||
| Female | 18 (12.7) | 41 (28.9) | 15 (10.6) | 17 (12.0) | 27 (19.0) | ||
| WAZ at birth | 0.3 ± 0.8 | 0.1 ± 0.7 | 0.12 | −0.3 ± 0.7 a | 0.2 ± 0.8 b | 0.4 ± 0.7 b | 0.0002 |
| Age (month) at follow-up | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.31 | 0.7 ± 0.3 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.83 |
| WAZ at follow-up | 0.1 ± 0.8 | −0.2 ± 0.8 | 0.13 | −0.4 ± 0.8 a | −0.0 ± 0.8 ab | 0.1 ± 0.7 b | 0.02 |
| LAZ at follow-up | 0.2 ± 1.0 | −0.1 ± 0.9 | 0.05 | −0.4 ± 0.9 a | −0.0 ± 0.9 ab | 0.2 ± 0.9 b | 0.02 |
| Mother | |||||||
| Age at delivery (year) | 31.8 ± 5.3 | 32.4 ± 4.0 | 0.45 | 31.9 ± 5.0 | 33.0 ± 3.8 | 31.7 ± 4.5 | 0.32 |
| Gravida, n (%) | 0.11 | 0.34 | |||||
| 1 | 18 (12.7) | 26 (18.3) | 14 (9.9) | 11 (7.8) | 19 (13.4) | ||
| >1 | 27 (19.0) | 71 (50.0) | 22 (15.5) | 35 (24.6) | 41 (28.8) | ||
| Self-reported population group, n (%) | 0.0003 | 0.12 | |||||
| White | 15 (10.6) | 64 (45.1) | 15 (10.6) | 26 (18.3) | 38 (26.8) | ||
| All other† | 30 (21.1) | 33 (23.2) | 21 (14.8) | 20 (14.1) | 22 (15.4) | ||
| Education, n (%) | 0.0266 | 0.97 | |||||
| University | 31 (21.8) | 68 (47.9) | 24 (16.9) | 33 (23.2) | 42 (29.6) | ||
| College/Vocational | 6 (4.2) | 24 (16.9) | 9 (6.3) | 9 (6.3) | 12 (8.5) | ||
| Elementary/High school | 8 (5.6) | 5 (3.6) | 3 (2.1) | 4 (2.8) | 6 (4.3) | ||
| Family income, n (%) | 0.15 | 0.37 | |||||
| ≥ CAD 70,000 | 20 (14.1) | 60 (42.3) | 20 (14.1) | 26 (18.3) | 34 (23.9) | ||
| < CAD 70,000 | 17 (12.0) | 24 (16.9) | 9 (6.3) | 11 (7.8) | 21 (14.8) | ||
| Not reported | 8 (5.6) | 13 (9.1) | 7 (4.9) | 9 (6.3) | 5 (3.6) | ||
| Pre-pregnancy BMI | 0.05 | 0.03 | |||||
| < 25 kg/m2 | 25 (17.6) | 70 (49.3) | 29 (20.4) | 33 (23.2) | 33 (23.2) | ||
| ≥ 25 kg/m2 | 20 (14.1) | 27 (19.0) | 7 (5.0) | 13 (9.2) | 27 (19.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gharibeh, N.; Razaghi, M.; Vanstone, C.A.; Wei, S.; McNally, D.; Rauch, F.; Jones, G.; Kaufmann, M.; Weiler, H.A. Maternal Vitamin D Status and Gestational Weight Gain as Correlates of Neonatal Bone Mass in Healthy Term Breastfed Young Infants from Montreal, Canada. Nutrients 2021, 13, 4189. https://doi.org/10.3390/nu13124189
Gharibeh N, Razaghi M, Vanstone CA, Wei S, McNally D, Rauch F, Jones G, Kaufmann M, Weiler HA. Maternal Vitamin D Status and Gestational Weight Gain as Correlates of Neonatal Bone Mass in Healthy Term Breastfed Young Infants from Montreal, Canada. Nutrients. 2021; 13(12):4189. https://doi.org/10.3390/nu13124189
Chicago/Turabian StyleGharibeh, Nathalie, Maryam Razaghi, Catherine A. Vanstone, ShuQin Wei, Dayre McNally, Frank Rauch, Glenville Jones, Martin Kaufmann, and Hope A. Weiler. 2021. "Maternal Vitamin D Status and Gestational Weight Gain as Correlates of Neonatal Bone Mass in Healthy Term Breastfed Young Infants from Montreal, Canada" Nutrients 13, no. 12: 4189. https://doi.org/10.3390/nu13124189
APA StyleGharibeh, N., Razaghi, M., Vanstone, C. A., Wei, S., McNally, D., Rauch, F., Jones, G., Kaufmann, M., & Weiler, H. A. (2021). Maternal Vitamin D Status and Gestational Weight Gain as Correlates of Neonatal Bone Mass in Healthy Term Breastfed Young Infants from Montreal, Canada. Nutrients, 13(12), 4189. https://doi.org/10.3390/nu13124189