
Snack Food Consumption across the Pune Transect in India: A Comparison of Dietary Behaviors Based on Consumer Characteristics and Locations

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods and Materials
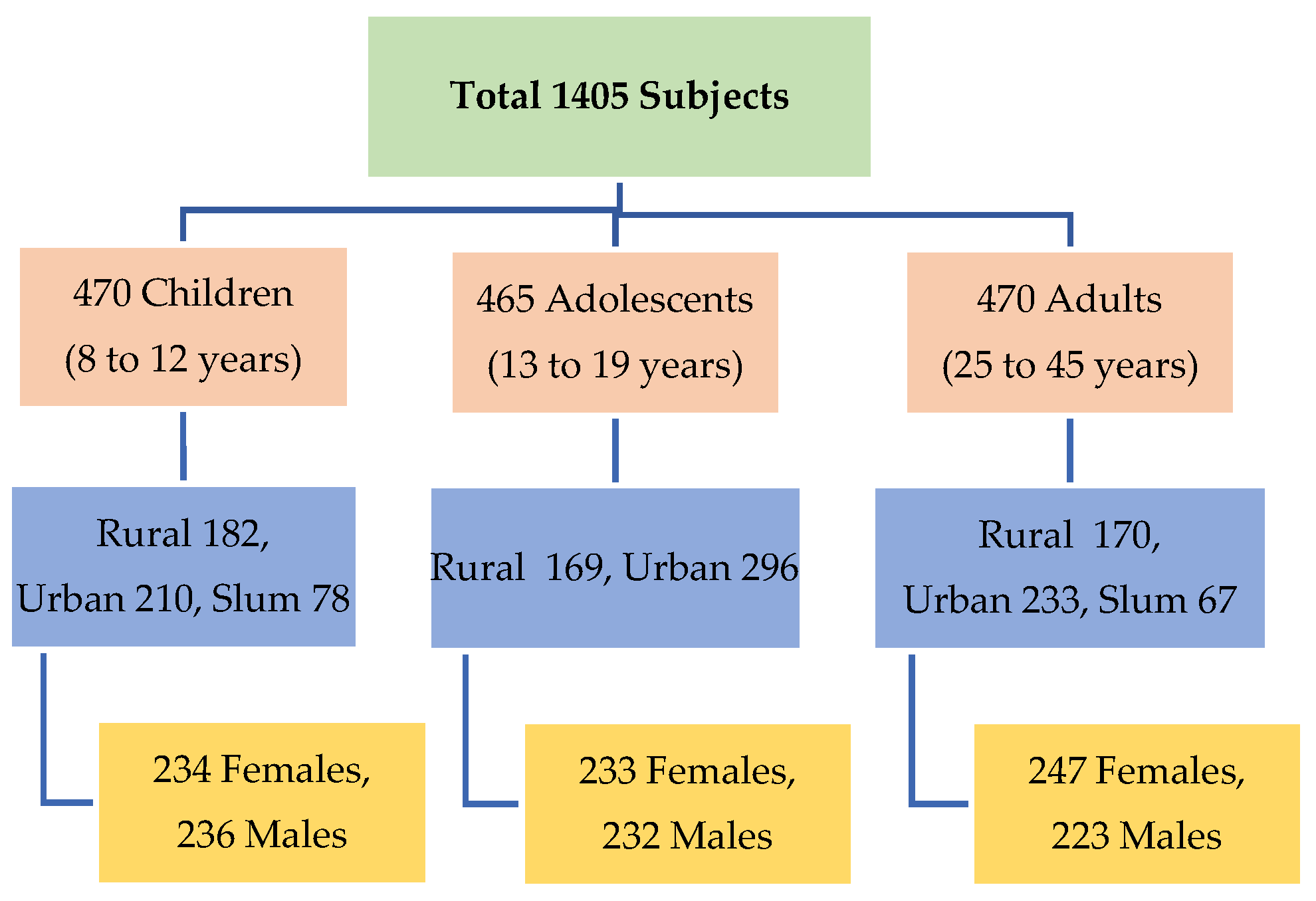
2.1. Study Population and Design
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Reasons for SFC
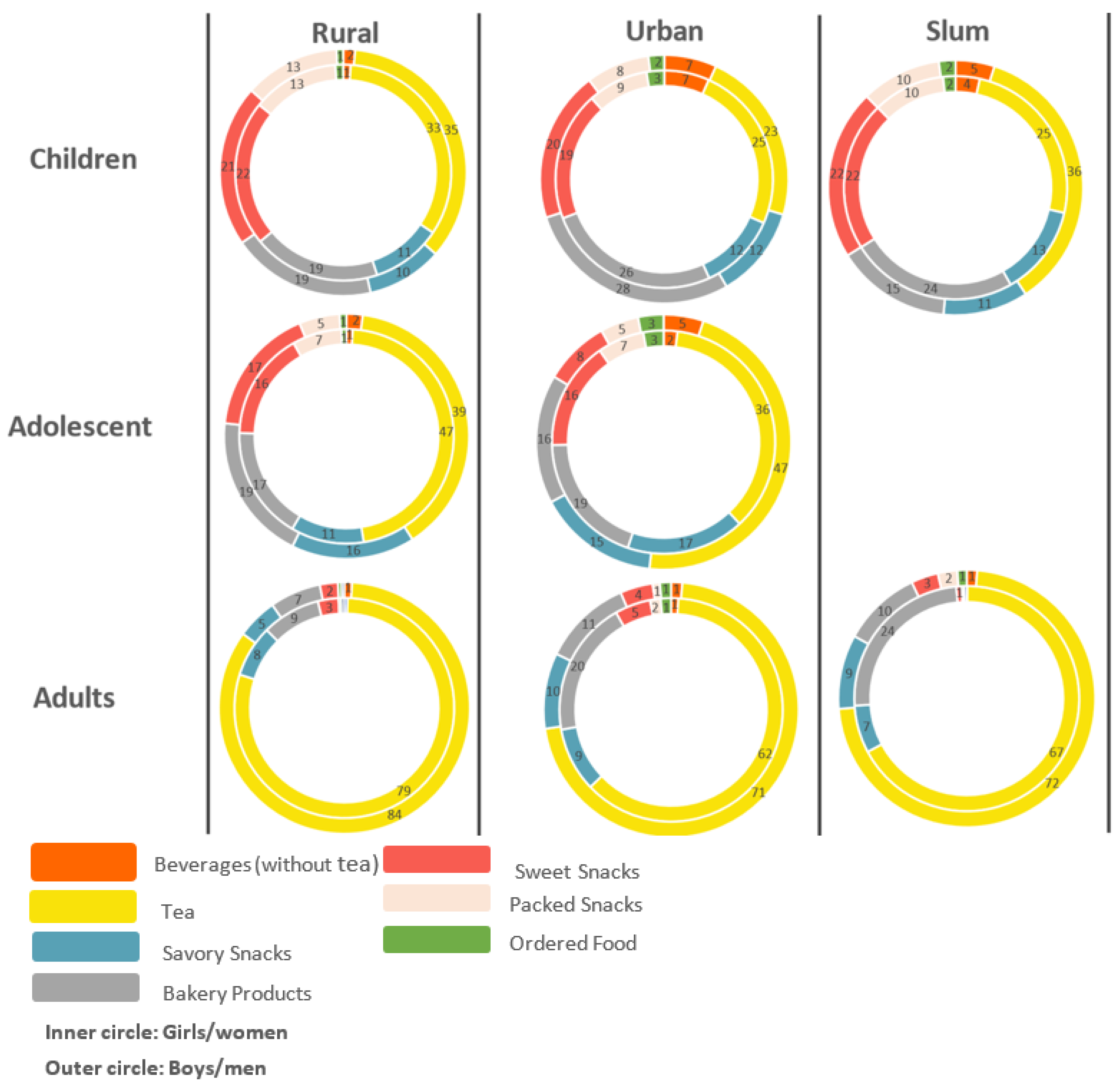
3.2. Place of SFC
3.3. Physical Activity and Screen Time
4. Discussion
Limitations of the Study
5. Conclusions
Further Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meenakshi, J.V. Trends and Patterns in the Triple Burden of Malnutrition in India. Agric. Econ. 2016, 47, 115–134. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.; Friel, S. Food Systems Transformations, Ultra-Processed Food Markets and the Nutrition Transition in Asia. Glob. Health 2016, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Vatanparast, H.; Islam, N.; Patil, R.P.; Shafiee, M.; Smith, J.; Whiting, S. Snack Consumption Patterns among Canadians. Nutrients 2019, 11, 1152. [Google Scholar] [CrossRef] [Green Version]
- Hess, J.M.; Jonnalagadda, S.S.; Slavin, J.L. What Is a Snack, Why Do We Snack, and How Can We Choose Better Snacks? A Review of the Definitions of Snacking, Motivations to Snack, Contributions to Dietary Intake, and Recommendations for Improvement. Adv. Nutr. 2016, 7, 466–475. [Google Scholar] [CrossRef] [Green Version]
- Wansink, B. From Mindless Eating to Mindlessly Eating Better. Physiol. Behav. 2010, 100, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.H.; Anderson, G.H. Snacking Definitions: Impact on Interpretation of the Literature and Dietary Recommendations. Crit. Rev. Food Sci. Nutr. 2010, 50, 848–871. [Google Scholar] [CrossRef]
- Larson, N.; Story, M. A Review of Snacking Patterns among Children and Adolescents: What Are the Implications of Snacking for Weight Status? Child. Obes. 2013, 9, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.W.; Jacques, P.F.; Dallal, G.E.; Sacheck, J.; Must, A. The Role of Eating Frequency on Total Energy Intake and Diet Quality in a Low-Income, Racially Diverse Sample of Schoolchildren. Public Health Nutr. 2015, 18, 474–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, K.; Livingstone, M.B.E. Associations between Meal and Snack Frequency and Overweight and Abdominal Obesity in US Children and Adolescents from National Health and Nutrition Examination Survey (NHANES) 2003–2012. Br. J. Nutr. 2016, 115, 1819–1829. [Google Scholar] [CrossRef] [Green Version]
- Dwyer, J.T.; Allison, D.B.; Coates, P.M. Dietary Supplements in Weight Reduction. J. Am. Diet. Assoc. 2005, 105, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Beets, M.W.; Tilley, F.; Kyryliuk, R.; Weaver, R.G.; Moore, J.B.; Turner-McGrievy, G. Children Select Unhealthy Choices When Given a Choice among Snack Offerings. J. Acad. Nutr. Diet. 2014, 114, 1440–1446. [Google Scholar] [CrossRef] [Green Version]
- Fayet-Moore, F.; Peters, V.; McConnell, A.; Petocz, P.; Eldridge, A.L. Weekday Snacking Prevalence, Frequency, and Energy Contribution Have Increased While Foods Consumed during Snacking Have Shifted among Australian Children and Adolescents: 1995, 2007 and 2011–12 National Nutrition Surveys. Nutr. J. 2017, 16, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, A.; Anderson, C.; McCullough, F. Associations between Children’s Diet Quality and Watching Television during Meal or Snack Consumption: A Systematic Review. Matern. Child. Nutr. 2017, 13. [Google Scholar] [CrossRef] [PubMed]
- Collings, P.J.; Kelly, B.; West, J.; Wright, J. Associations of TV Viewing Duration, Meals and Snacks Eaten When Watching TV, and a TV in the Bedroom with Child Adiposity. Obesity 2018, 26, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, A.; Bonell, C.; Sorhaindo, A. You Are What Your Friends Eat: Systematic Review of Social Network Analyses of Young People’s Eating Behaviours and Bodyweight. J. Epidemiol. Community Health 2011, 65, 548–555. [Google Scholar] [CrossRef]
- Julian, C.; Santaliestra-Pasías, A.M.; Miguel-Berges, M.L.; Moreno, L.A. Frequency and Quality of Mid-Afternoon Snack among Spanish Children. Nutr. Hosp. 2017, 34, 827–833. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, S. Trends in Food Locations and Sources among Adolescents and Young Adults. Prev. Med. 2002, 35, 107–113. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. 40-Year Trends in Meal and Snack Eating Behaviors of American Adults. J. Acad. Nutr. Diet. 2015, 115, 50–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taillie, L.S.; Afeiche, M.C.; Eldridge, A.L.; Popkin, B.M. Increased Snacking and Eating Occasions Are Associated with Higher Energy Intake among Mexican Children Aged 2–13 Years. J. Nutr. 2015, 145, 2570–2577. [Google Scholar] [CrossRef] [Green Version]
- van Ansem, W.J.C.; Schrijvers, C.T.M.; Rodenburg, G.; van de Mheen, D. Children’s Snack Consumption: Role of Parents, Peers and Child Snack-Purchasing Behaviour. Results from the INPACT Study. Eur. J. Public Health 2015, 25, 1006–1011. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.I.; Miller, J.M.; Watts, A.W.; Story, M.T.; Neumark-Sztainer, D.R. Adolescent Snacking Behaviors Are Associated with Dietary Intake and Weight Status. J. Nutr. 2016, 146, 1348–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekiyama, M.; Roosita, K.; Ohtsuka, R. Snack Foods Consumption Contributes to Poor Nutrition of Rural Children in West Java, Indonesia. Asia Pac. J. Clin. Nutr. 2012, 21, 558–567. [Google Scholar]
- Wang, D.; Van der Klazine, H.; Jacquier, E.; Afeiche, M.; Eldridge, A. Snacking Patterns in Children: A Comparison between Australia, China, Mexico, and the US. Nutrients 2018, 10, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa-Burrows, P.; Burrows, R.; Orellana, Y.; Ivanovic, D. The Relationship between Unhealthy Snacking at School and Academic Outcomes: A Population Study in Chilean Schoolchildren. Public Health Nutr. 2015, 18, 2022–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deierlein, A.L.; Galvez, M.P.; Yen, I.H.; Pinney, S.M.; Biro, F.M.; Kushi, L.H.; Teitelbaum, S.; Wolff, M.S. Local Food Environments Are Associated with Girls’ Energy, Sugar-Sweetened Beverage and Snack-Food Intakes. Public Health Nutr. 2014, 17, 2194–2200. [Google Scholar] [CrossRef]
- Green, H.; Siwajek, P.; Roulin, A. Use of Nutrient Profiling to Identify Healthy versus Unhealthy Snack Foods and Whether They Can Be Part of a Healthy Menu Plan. J. Nutr. Intermed. Metab. 2017, 9, 1–5. [Google Scholar] [CrossRef]
- Mithra, P.; Unnikrishnan, B.; Thapar, R.; Kumar, N.; Hegde, S.; Mangaldas, K.A.; Kulkarni, V.; Holla, R.; Darshan, B.B.; Tanuj, K.; et al. Snacking Behaviour and Its Determinants among College-Going Students in Coastal South India. J. Nutr. Metab. 2018, 2018, 6785741. [Google Scholar] [CrossRef] [Green Version]
- Rathi, N.; Riddell, L.; Worsley, A. Urban Indian Adolescents Practise Unhealthy Dietary Behaviours. Br. Food J. 2018, 120, 1657–1665. [Google Scholar] [CrossRef]
- Riediger, N.; Dhalla, A.; Cooper, M.; Bombak, A.; Sreeramaiah, H. A Qualitative Analysis of the Perceived Socio-Cultural Contexts and Health Concerns of Sugar-Sweetened Beverages among Adults Studying or Working at a Post-Secondary Institution in Dharwad, India. BMC Public Health 2021, 21, 1016. [Google Scholar] [CrossRef]
- Alifia, B.; Neha, S.; Tasneem, A.K.; Sherebanu, Z.P.; Laveeza, M.A.A.; Fatema, M.K.; Tasneem, A.B. Changes in Snacking Patterns during COVID-19 Lockdown in Adults from Mumbai City, India. Curr. Res. Nutr. Food Sci. 2021, 9, 3. [Google Scholar]
- Wang, Z.; Zhai, F.; Zhang, B.; Popkin, B.M. Trends in Chinese Snacking Behaviors and Patterns and the Social-Demographic Role between 1991 and 2009. Asia Pac. J. Clin. Nutr. 2012, 21, 253–262. [Google Scholar]
- Sharma, M.; Kishore, A.; Roy, D.; Joshi, K. A Comparison of the Indian Diet with the EAT-Lancet Reference Diet. BMC Public Health 2020, 20, 812. [Google Scholar] [CrossRef]
- Mo, H.F.W. GOI National Family Health Survey (NFHS-4); International Institute for Population Sciences: Mumbai, India, 2015. [Google Scholar]
- Bogers, R.P.; Brug, J.; van Assema, P.; Dagnelie, P.C. Explaining Fruit and Vegetable Consumption: The Theory of Planned Behaviour and Misconception of Personal Intake Levels. Appetite 2004, 42, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Sanghvi, S. Cardiac Rehabilitation. In Tidy’s Physiotherapy; Elsevier: Amsterdam, The Netherlands, 2013; pp. 147–168. ISBN 978-0-7020-4344-4. [Google Scholar]
- World Health Organsation Tools and Toolkit. 2021. Available online: https://www.who.int/tools (accessed on 29 October 2021).
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Pennington Biomedical Research Center BMI Calculator. Pennington Biomedical Research Center. Available online: https://www.pbrc.edu/research-trials/BMI-Calculator.aspx (accessed on 29 October 2021).
- Jahns, L.; Siega-Riz, A.M.; Popkin, B.M. The Increasing Prevalence of Snacking among US Children from 1977 to 1996. J. Pediatr. 2001, 138, 493–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debruijn, G.; Kremers, S.; Schaalma, H.; Vanmechelen, W.; Brug, J. Determinants of Adolescent Bicycle Use for Transportation and Snacking Behavior. Prev. Med. 2005, 40, 658–667. [Google Scholar] [CrossRef]
- Anding, J.D.; Kubena, K.S.; McIntosh, W.A.; Wolinsky, I. Dietary Intake and the Contribution of Snacks among Adolescents during the Summer Months. J. Consum. Stud. Home Econ. 1998, 22, 131–138. [Google Scholar] [CrossRef]
- Savige, G.; MacFarlane, A.; Ball, K.; Worsley, A.; Crawford, D. Snacking Behaviours of Adolescents and Their Association with Skipping Meals. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A.E.; Austin, S.B.; Gillman, M.W.; Rosner, B.; Rockett, H.R.; Colditz, G.A. Snack Food Intake Does Not Predict Weight Change among Children and Adolescents. Int. J. Obes. 2004, 28, 1210–1216. [Google Scholar] [CrossRef] [Green Version]
- Bellisle, F. Meals and Snacking, Diet Quality and Energy Balance. Physiol. Behav. 2014, 134, 38–43. [Google Scholar] [CrossRef]
- Chapelot, D. The Role of Snacking in Energy Balance: A Biobehavioral Approach. J. Nutr. 2011, 141, 158–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapelot, D.; Marmonier, C.; Aubert, R.; Gausseres, N.; Louis-Sylvestre, J. A Role for Glucose and Insulin Preprandial Profiles to Differentiate Meals and Snacks. Physiol. Behav. 2004, 80, 721–731. [Google Scholar] [CrossRef]
- Pearson, N.; MacFarlane, A.; Crawford, D.; Biddle, S.J.H. Family Circumstance and Adolescent Dietary Behaviours. Appetite 2009, 52, 668–674. [Google Scholar] [CrossRef]
- Krølner, R.; Rasmussen, M.; Brug, J.; Klepp, K.-I.; Wind, M.; Due, P. Determinants of Fruit and Vegetable Consumption among Children and Adolescents: A Review of the Literature. Part II: Qualitative Studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 112. [Google Scholar] [CrossRef] [Green Version]
- van der Horst, K.; Oenema, A.; Ferreira, I.; Wendel-Vos, W.; Giskes, K.; van Lenthe, F.; Brug, J. A Systematic Review of Environmental Correlates of Obesity-Related Dietary Behaviors in Youth. Health Educ. Res. 2006, 22, 203–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wouters, E.J.; Larsen, J.K.; Kremers, S.P.; Dagnelie, P.C.; Geenen, R. Peer Influence on Snacking Behavior in Adolescence. Appetite 2010, 55, 11–17. [Google Scholar] [CrossRef]
- Salvy, S.-J.; Kluczynski, M.A.; Nitecki, L.A.; O’Connor, B.C. Peer Influence on Youth’s Snack Purchases: A Laboratory Analog of Convenience Store Shopping. Eat. Behav. 2012, 13, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Salvy, S.-J.; Elmo, A.; Nitecki, L.A.; Kluczynski, M.A.; Roemmich, J.N. Influence of Parents and Friends on Children’s and Adolescents’ Food Intake and Food Selection. Am. J. Clin. Nutr. 2011, 93, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Bell, R.; Marshall, D.W. The Construct of Food Involvement in Behavioral Research: Scale Development and Validation. Appetite 2003, 40, 235–244. [Google Scholar] [CrossRef]
- Kerr, M.A.; Rennie, K.L.; McCaffrey, T.A.; Wallace, J.M.W.; Hannon-Fletcher, M.P.; Livingstone, M.B.E. Snacking Patterns among Adolescents: A Comparison of Type, Frequency and Portion Size between Britain in 1997 and Northern Ireland in 2005. Br. J. Nutr. 2008, 101, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Vereecken, C.; Huybrechts, I.; Maes, L.; De Henauw, S. Food Consumption among Preschoolers. Does the School Make a Difference? Appetite 2008, 51, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Adair, L.S.; Popkin, B.M. Are Child Eating Patterns Being Transformed Globally? Obes. Res. 2005, 13, 1281–1299. [Google Scholar] [CrossRef]
- Sebastian, R.S.; Enns, C.W.; Goldman, J.D. My Pyramid Intakes and Snacking Patterns of US Adults. NHANES 2011, 7, 2007–2008. [Google Scholar]
- Myhre, J.B.; Løken, E.B.; Wandel, M.; Andersen, L.F. The Contribution of Snacks to Dietary Intake and Their Association with Eating Location among Norwegian Adults–Results from a Cross-Sectional Dietary Survey. BMC Public Health 2015, 15, 369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliday, T.J.; Kwak, S. Weight Gain in Adolescents and Their Peers. Econ. Hum. Biol. 2009, 7, 181–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Monthly Freq of SFC | Monthly SFC (in g) | Hunger as a Reason for Snacking (%) | Chi Square for Hunger | |||||
|---|---|---|---|---|---|---|---|---|
| Factors | Mean | SD | Mean | SD | Mean | SD | Pearson Chi Square | Pr |
| Overall | 36.6 | 37.5 | 2206.8 | 3133.0 | 69.0 | 46.3 | ||
| Children | 51.7 | 43.0 | 2673.6 | 3341.6 | 71.9 | 45.0 | 2.86 | 0.090 |
| Adolescent | 36.1 | 36.1 | 2254.0 | 3402.5 | 66.2 | 47.3 | 2.42 | 0.120 |
| Adult | 22.0 | 25.2 | 1693.2 | 2505.7 | 68.7 | 46.4 | 0.02 | 0.880 |
| p for comparison (t value) | ||||||||
| Child and Adolescent | 4.5 *** | 1.8 * | ||||||
| Child and Adult | 9.5 *** | 4.3 *** | ||||||
| Adolescent and Adult | 5.3 *** | 2.4 ** | ||||||
| Rural location | 34.2 | 35.8 | 2736.0 | 3774.8 | 62.8 | 48.4 | 14.89 | 0.000 |
| Urban location | 37.7 | 38.2 | 1810.0 | 2451.9 | 73.7 | 44.0 | 16.64 | 0.000 |
| Slum lcation | 39.7 | 39.9 | 2327.3 | 3405.9 | 66.9 | 47.2 | 0.32 | 0.560 |
| p for comparison (t value) | ||||||||
| Rural and Urban | −6.2 *** | −6.2 *** | ||||||
| Rural and Slum | 9.9 *** | 9.8 *** | ||||||
| Urban and Slum | 15.6 *** | 15.5 *** | ||||||
| Male | 33.9 | 36.3 | 2081.4 | 2834.0 | ||||
| Female | 39.2 | 38.5 | 2328.1 | 3394.9 | ||||
| p for comparison (t value) | ||||||||
| Male and Female | 2.7 ** | 1.5 ns | ||||||
| Low SES | 26.6 | 27.2 | 1777.9 | 3170.5 | 79.8 | 40.2 | 35.68 | 0.000 |
| Mid SES | 29.6 | 32.1 | 2196.1 | 2829.4 | 60.9 | 48.9 | 10.60 | 0.001 |
| High SES | 31.4 | 36.6 | 1924.5 | 2976.4 | 60.4 | 49.0 | 8.27 | 0.004 |
| p for comparison (t value) | ||||||||
| Low and Mid | −1.3 ns | −1.3 ns | ||||||
| Low and High | 0.7 ns | 0.8 ns | ||||||
| Mid and High | 1.9 ns | 1.9 ns | ||||||
| OLS Model | Monthly Frequency of Snack Foods (log) | Monthly Consumption of Snack Foods in Gram (log) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome Variable: | Children | Adolescent | Adult | Children | Adolescent | Adult | ||||||
| Coef | SE | Coef | SE | Coef | SE | Coef | SE | Coef | SE | Coef | SE | |
| Hunger ^ | −0.025 | (0.105) | −0.164 | (0.103) | −0.030 | (0.136) | −0.051 | (0.136) | −0.055 | (0.141) | −0.135 | (0.160) |
| Access ^ | −0.098 | (0.201) | 0.765 * | (0.409) | 0.038 | (0.216) | 0.039 | (0.243) | 0.683 ** | (0.281) | 0.146 | (0.245) |
| Company of friends ^ | −0.000 | (0.231) | −0.914 ** | (0.414) | −0.334 * | (0.198) | −0.066 | (0.265) | −0.777 *** | (0.284) | −0.447 * | (0.232) |
| Gender (Male = 1; Otherwise = 0) | −0.060 | (0.088) | −0.295 *** | (0.093) | −0.205 ** | (0.101) | −0.081 | (0.100) | −0.223 * | (0.115) | −0.046 | (0.114) |
| Household size (nos) | 0.017 | (0.021) | −0.011 | (0.022) | 0.033 | (0.023) | 0.003 | (0.025) | −0.040 | (0.027) | −0.007 | (0.028) |
| Illiterate (Mother/ Father = 1; Otherwise = 0) | −0.266 | (0.216) | −0.256 | (0.219) | −0.244 ** | (0.117) | −0.287 | (0.195) | −0.412 | (0.269) | −0.140 | (0.133) |
| Assets (Base: Poor) | ||||||||||||
| Middle ^ | 0.141 | (0.107) | 0.009 | (0.108) | −0.010 | (0.121) | 0.030 | (0.118) | −0.172 | (0.127) | 0.028 | (0.141) |
| Rich ^ | 0.070 | (0.137) | 0.054 | (0.143) | 0.003 | (0.145) | −0.158 | (0.157) | −0.296 * | (0.155) | 0.200 | (0.166) |
| Location (Base: Rural) | ||||||||||||
| Urban ^ | 0.274 | (0.203) | 0.077 | (0.234) | 0.503 *** | (0.169) | −0.131 | (0.245) | 0.291 | (0.273) | 0.130 | (0.194) |
| Slum ^ | 0.425 ** | (0.198) | 0.432 ** | (0.191) | 0.050 | (0.233) | −0.059 | (0.214) | ||||
| Any migrated from family ^ | −0.140 | (0.134) | 0.319 *** | (0.112) | 0.127 | (0.157) | −0.081 | (0.167) | 0.136 | (0.146) | 0.053 | (0.223) |
| Private School Type ^ | −0.390 ** | (0.161) | −0.268 | (0.169) | ||||||||
| Screen time in minutes (log) | 0.092 * | (0.056) | 0.062 * | (0.037) | −0.002 | (0.042) | 0.115 ** | (0.058) | 0.133 ** | (0.052) | 0.061 | (0.053) |
| Food access based on location (Base: Low) | ||||||||||||
| Moderate ^ | 0.407 ** | (0.166) | −0.206 | (0.200) | 0.165 | (0.226) | −0.691 *** | (0.250) | ||||
| High ^ | −0.416 ** | (0.207) | −0.184 | (0.178) | −0.058 | (0.234) | −0.761 *** | (0.219) | ||||
| Light Activity in minutes (log) | −0.071 | (0.470) | 0.230 | (0.262) | 0.129 | (0.172) | −0.143 | (0.527) | −0.390 | (0.271) | −0.198 | (0.191) |
| Moderate Activity in minutes (log) | 0.006 | (0.048) | 0.069 | (0.054) | −0.012 | (0.048) | −0.031 | (0.057) | −0.021 | (0.068) | −0.014 | (0.062) |
| Heavy Activity in minutes (log) | −0.014 | (0.024) | −0.025 | (0.027) | −0.002 | (0.028) | −0.019 | (0.033) | ||||
| Skip Breakfast ^ | −0.063 | (0.106) | 0.116 | (0.091) | −0.140 | (0.100) | 0.016 | (0.141) | −0.015 | (0.115) | −0.145 | (0.119) |
| Order food ^ | −0.122 | (0.148) | 0.319 *** | (0.107) | 0.483 *** | (0.165) | 0.066 | (0.169) | 0.140 | (0.151) | 0.129 | (0.220) |
| Read label ^ | 0.013 | (0.100) | −0.037 | (0.099) | 0.060 | (0.115) | −0.304 *** | (0.110) | 0.074 | (0.120) | 0.175 | (0.134) |
| Access to snack food (on campus) ^ | −0.118 | (0.116) | −0.071 | (0.137) | −0.086 | (0.147) | −0.186 | (0.163) | ||||
| Access to snack food (nearby campus) ^ | 0.313 * | (0.184) | 0.459 | (0.287) | −0.012 | (0.239) | 0.405 | (0.284) | ||||
| Carry home tiffin ^ | −0.101 | (0.198) | −0.127 | (0.092) | 0.004 | (0.228) | 0.116 | (0.124) | ||||
| Checks before buying any snacks | ||||||||||||
| Price ^ | −0.110 | (0.140) | −0.237 | (0.151) | −0.226 | (0.149) | −0.269 | (0.168) | 0.017 | (0.216) | 0.042 | (0.191) |
| Brand ^ | 0.250 *** | (0.089) | −0.068 | (0.097) | 0.139 | (0.113) | 0.184 * | (0.100) | 0.094 | (0.135) | 0.049 | (0.133) |
| Taste ^ | −0.042 | (0.098) | 0.153 | (0.102) | 0.111 | (0.119) | −0.028 | (0.113) | 0.312 *** | (0.120) | 0.062 | (0.134) |
| Advertisement ^ | 0.189 * | (0.107) | −0.177 | (0.108) | −0.468 *** | (0.107) | 0.133 | (0.114) | 0.123 | (0.124) | −0.481 *** | (0.120) |
| Availability ^ | −0.015 | (0.093) | −0.069 | (0.091) | 0.055 | (0.099) | −0.082 | (0.123) | −0.013 | (0.112) | 0.012 | (0.115) |
| Nutrition ^ | −0.138 | (0.102) | −0.065 | (0.092) | −0.206 * | (0.114) | 0.060 | (0.122) | −0.098 | (0.117) | −0.230 * | (0.137) |
| Food safety ^ | 0.049 | (0.105) | −0.019 | (0.094) | −0.190 | (0.122) | 0.182 | (0.130) | −0.077 | (0.117) | −0.187 | (0.145) |
| Got Pocket Money ^ | 0.328 *** | (0.096) | 0.236 ** | (0.099) | 0.337 *** | (0.115) | 0.171 | (0.118) | ||||
| Domestic Help ^ | 0.346 | (0.223) | −0.012 | (0.132) | −0.158 | (0.205) | −0.120 | (0.293) | −0.102 | (0.265) | −0.093 | (0.254) |
| Any Disease (Diabetes/Hypertension) ^ | −0.148 | (0.247) | −0.137 | (0.285) | ||||||||
| Constant | 3.119 | (3.174) | 1.190 | (1.912) | 2.030 | (1.236) | 8.399 ** | (3.583) | 9.260 *** | (1.997) | 8.384 *** | (1.392) |
| Observations | 439 | 446 | 450 | 430 | 417 | 418 | ||||||
| R-squared | 0.200 | 0.182 | 0.226 | 0.164 | 0.229 | 0.084 | ||||||
| Age-Group (0–20 years) | In Numbers | In Percentage (%) | |||||
|---|---|---|---|---|---|---|---|
| BMI Category | Percentile | Children | Adolescent | Total | Children | Adolescent | Total |
| Underweight | <5th | 360 | 130 | 490 | 79.3 | 28.1 | 53.5 |
| Normal Weight | 5th to 85th | 80 | 234 | 314 | 17.6 | 50.7 | 34.3 |
| Overweight | 85th to 95th | 11 | 75 | 86 | 2.4 | 16.2 | 9.4 |
| Obese | >95th | 3 | 23 | 26 | 0.7 | 5.0 | 2.8 |
| Total | 454 | 462 | 916 | 100.0 | 100.0 | 100.0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy, D.; Boss, R.; Saroj, S.; Karandikar, B.; Pradhan, M.; Pandey, H. Snack Food Consumption across the Pune Transect in India: A Comparison of Dietary Behaviors Based on Consumer Characteristics and Locations. Nutrients 2021, 13, 4325. https://doi.org/10.3390/nu13124325
Roy D, Boss R, Saroj S, Karandikar B, Pradhan M, Pandey H. Snack Food Consumption across the Pune Transect in India: A Comparison of Dietary Behaviors Based on Consumer Characteristics and Locations. Nutrients. 2021; 13(12):4325. https://doi.org/10.3390/nu13124325
Chicago/Turabian StyleRoy, Devesh, Ruchira Boss, Sunil Saroj, Bhushana Karandikar, Mamata Pradhan, and Himanshi Pandey. 2021. "Snack Food Consumption across the Pune Transect in India: A Comparison of Dietary Behaviors Based on Consumer Characteristics and Locations" Nutrients 13, no. 12: 4325. https://doi.org/10.3390/nu13124325
APA StyleRoy, D., Boss, R., Saroj, S., Karandikar, B., Pradhan, M., & Pandey, H. (2021). Snack Food Consumption across the Pune Transect in India: A Comparison of Dietary Behaviors Based on Consumer Characteristics and Locations. Nutrients, 13(12), 4325. https://doi.org/10.3390/nu13124325