
Effect of Acute and Chronic Oral l-Carnitine Supplementation on Exercise Performance Based on the Exercise Intensity: A Systematic Review

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategies
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Outcome Measures
2.5. Quality Assessment of the Experiments
3. Results
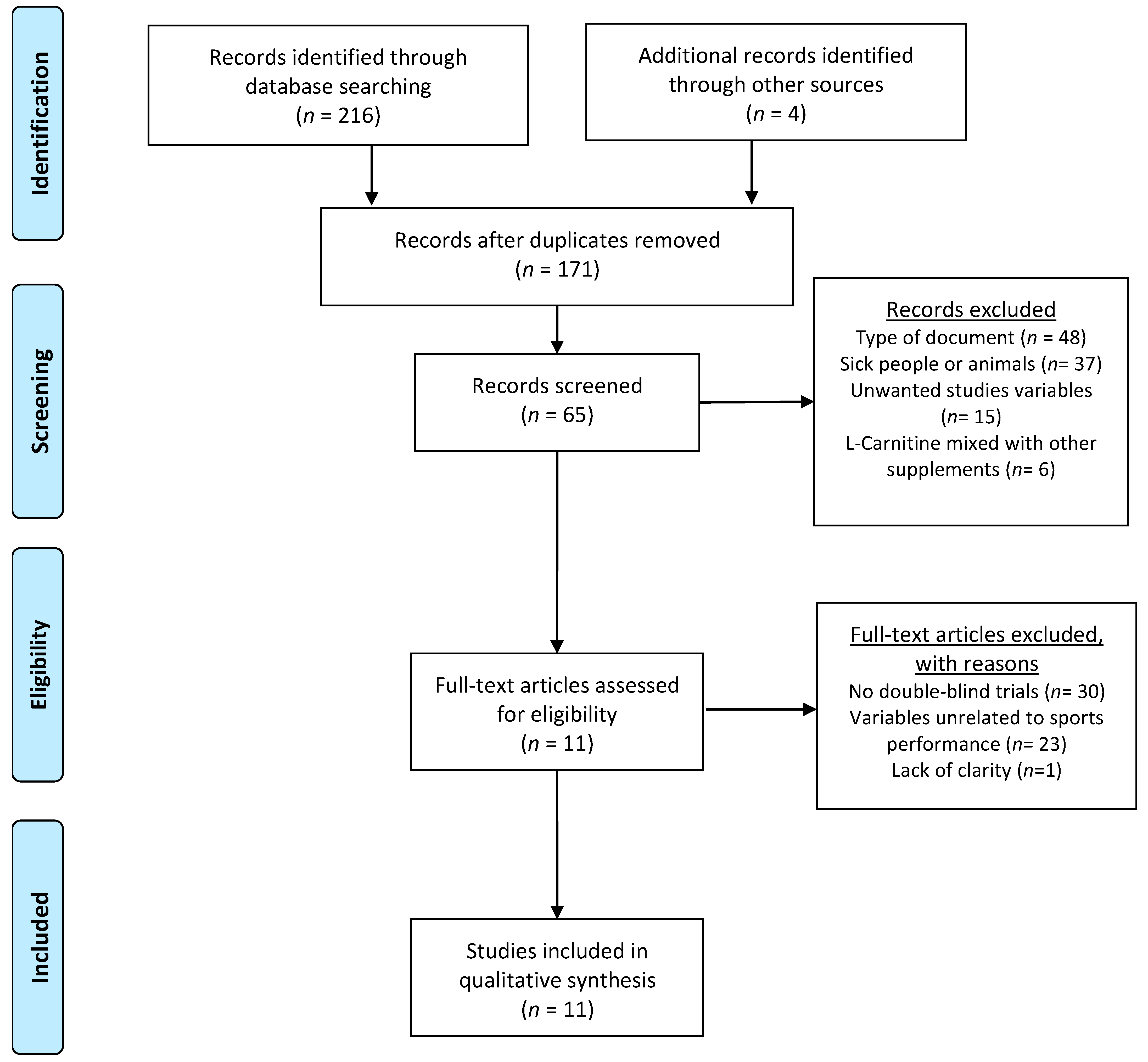
3.1. Main Search
3.2. Carnitine Supplementation
3.3. High-Intensity and Moderate-Intensity Exercise Performance Outcomes Analyzed
3.3.1. Effect of l-Carnitine Supplementation on High-Intensity Exercise Performance (≥80% O2 max)
3.3.2. Effect of l-Carnitine Supplementation on Moderate-Intensity (50–79% O2 max) Exercise Performance
4. Discussion
4.1. Effects of l-C Supplementation on High-Intensity Exercise Performance (≥80% O2 max)
4.1.1. Chronic l-C Supplementation Protocol for High-Intensity Exercise Performance (≥80% O2 max)
4.1.2. Acute l-C Supplementation Protocol for High-Intensity Exercise Performance (≥80% O2 max)
4.2. Effects of l-C Supplementation on Moderate-Intensity Exercise Performance (50–79% O2 max)
4.2.1. Chronic l-C Supplementation Protocol for Moderate-Intensity Exercise Performance (50–79% O2 max)
4.2.2. Acute Supplementation Protocol for Moderate-Intensity Exercise Performance (50–79% O2 max)
4.3. Limitations, Strengths, and Future Lines of Investigation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Garthe, I.; Maughan, R.J. Athletes and supplements: Prevalence and perspectives. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 126–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlic, H.; Lohninger, A. Supplementation of L-carnitine in athletes: Does it make sense? Nutrition 2004, 20, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Longo, N.; Frigeni, M.; Pasquali, M. Carnitine transport and fatty acid oxidation. Biochim. Biophys. Acta 2016, 1863, 2422. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Volek, J.S.; Dunn-Lewis, C. L-carnitine supplementation: Influence upon physiological function. Curr. Sports Med. Rep. 2008, 7, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Pekala, J.; Patkowska-Sokola, B.; Bodkowski, R.; Jamroz, D.; Nowakowski, P.; Lochynski, S.; Librowski, T. l-Carnitine—Metabolic Functions and Meaning in Humans Life. Curr. Drug Metab. 2011, 12, 667–678. [Google Scholar] [CrossRef]
- Fielding, R.; Riede, L.; Lugo, J.P.; Bellamine, A. l-Carnitine Supplementation in Recovery after Exercise. Nutrients 2018, 10, 349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, H.; Djalali, M.; Daneshpazhooh, M.; Honarvar, N.M.; Chams-Davatchi, C.; Sepandar, F.; Fakhri, Z.; Yaghubi, E.; Zarei, M.; Javanbakht, M.H. Effects of L-carnitine supplementation on biomarkers of oxidative stress, antioxidant capacity and lipid profile, in patients with pemphigus vulgaris: A randomized, double-blind, placebo-controlled trial. Eur. J. Clin. Nutr. 2018, 72, 99–104. [Google Scholar] [CrossRef]
- Gnoni, A.; Longo, S.; Gnoni, G.V.; Giudetti, A.M. Carnitine in human muscle bioenergetics: Can carnitine supplementation improve physical exercise? Molecules 2020, 25, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, F.B.; Evans, C.E.; Constantin-Teodosiu, D.; Greenhaff, P.L. Carbohydrate ingestion augments L-carnitine retention in humans. J. Appl. Physiol. 2007, 102, 1065–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, F.B.; Wall, B.T.; Marimuthu, K.; Shannon, C.E.; Constantin-Teodosiu, D.; Macdonald, I.A.; Greenhaff, P.L. Skeletal muscle carnitine loading increases energy expenditure, modulates fuel metabolism gene networks and prevents body fat accumulation in humans. J. Physiol. 2013, 591, 4655–4666. [Google Scholar] [CrossRef]
- Oliveira, C.; Sousa, M. The effects of L-carnitine supplementation in athletic performance. Sci. Sport. 2019, 34, 63–72. [Google Scholar] [CrossRef]
- Trinity, J.D.; Lee, J.F.; Pahnke, M.D.; Beck, K.C.; Coyle, E.F. Attenuated relationship between cardiac output and oxygen uptake during high-intensity exercise. Acta Physiol. 2012, 204, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Stephens, F.B.; Constantin-teodosiu, D.; Greenhaff, P.L. New insights concerning the role of carnitine in the regulation of fuel metabolism in skeletal muscle. J. Physiol. 2007, 581, 431–444. [Google Scholar] [CrossRef]
- Trappe, S.W.; Costill, D.L.; Goodpaste, B.; Vukovich, M.D.; Fink, W.J. The effects of L-carnitine supplementation on performance during interval swimming. Int. J. Sports Med. 1994, 15, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Shannon, C.E.; Ghasemi, R.; Greenhaff, P.L.; Stephens, F.B. Increasing skeletal muscle carnitine availability does not alter the adaptations to high-intensity interval training. Scand. J. Med. Sci. Sport. 2018, 28, 107–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orer, G.E.; Guzel, N.A. The effects of acute l-carnitine supplementation on endurance performance of athletes. J. Strength Cond. Res. 2014, 28, 514–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greig, C.; Finch, K.M.; Jones, D.A.; Cooper, M.; Sargeant, A.J.; Forte, C.A. The effect of oral supplementation with l-carnitine on maximum and submaximum exercise capacity. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Soop, M.; Bjorkman, O.; Cederblad, G.; Hagenfeldt, L.; Wahren, J. Influence of carnitine supplementation on muscle substrate and carnitine metabolism during exercise. J. Appl. Physiol. 1988, 64, 2394–2399. [Google Scholar] [CrossRef]
- Marconi, C.; Sassi, G.; Carpinelli, A.; Cerretelli, P. Effects of l-carnitine loading on the aerobic and anaerobic performance of endurance athletes. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Colombani, P. Effects of L-carnitine supplementation on physical performance and energy metabolism of endurance-trained athletes: A double-blind crossover field study. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 73, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Stephens, F.B.; Constantin-Teodosiu, D.; Laithwaite, D.; Simpson, E.J.; Greenhaff, P.L. Insulin stimulates L-carnitine accumulation in human skeletal muscle. FASEB J. 2005, 20, 377–379. [Google Scholar] [CrossRef]
- Stephens, F.B.; Constantin-Teodosiu, D.; Laithwaite, D.; Simpson, E.J.; Greenhaff, P.L. An acute increase in skeletal muscle carnitine content alters fuel metabolism in resting human skeletal muscle. J. Clin. Endocrinol. Metab. 2006, 91, 5013–5018. [Google Scholar] [CrossRef] [Green Version]
- Wall, B.T.; Stephens, F.B.; Constantin-Teodosiu, D.; Marimuthu, K.; Macdonald, I.A.; Greenhaff, P.L. Chronic oral ingestion of l-carnitine and carbohydrate increases muscle carnitine content and alters muscle fuel metabolism during exercise in humans. J. Physiol. 2011, 589, 963–973. [Google Scholar] [CrossRef] [PubMed]
- Burrus, B.M.; Moscicki, B.M.; Matthews, T.D.; Paolone, V.J. The Effect of Acute L-carnitine and Carbohydrate Intake on Cycling Performance. Int. J. Exerc. Sci. 2018, 11, 404–416. [Google Scholar] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65–W-94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm. Policy Ment. Health 2015, 42, 533. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, D.A.; Green, S.E.; Higgins, J.P.T. Defining the review question and developing criteria for including studies. In Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; John Wiley & Sons: Chichester, UK, 2008; pp. 83–94. [Google Scholar]
- Law, M.; Stewart, D.; Letts, L.; Pollock, N.; Bosch, J.; Westmorland, M. Guidelines for Critical Review Form—Quantitative Studies 1998; McMaster University: Hamilton, ON, Canada, 2008. [Google Scholar]
- Broad, E.M.; Maughan, R.J.; Galloway, S.D.R. Effects of four weeks l-Carnitine L-tartrate ingestion on substrate utilization during prolonged exercise. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 665–679. [Google Scholar] [CrossRef]
- Arazi, H.; Mehrtash, M. Effect of Acute l-Carnitine Supplementation on Blood Lactate, Glucose, Aerobic and Anaerobic Performance in Elite Male Artistic Gymnasts. Balt. J. Sport Health Sci. 2017, 1, 2–7. [Google Scholar] [CrossRef]
- Jacobs, P.L.; Goldstein, E.R.; Blackburn, W.; Orem, I.; Hughes, J.J. Glycine propionyl-L-carnitine produces enhanced anaerobic work capacity with reduced lactate accumulation in resistance trained males. J. Int. Soc. Sports Nutr. 2009, 6, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koozehchian, M.S.; Daneshfar, A.; Fallah, E.; Agha-Alinejad, H.; Samadi, M.; Kaviani, M.; Kaveh, B.M.; Jung, Y.P.; Sablouei, M.H. Effects of nine weeks l-Carnitine supplementation on exercise performance, anaerobic power, and exercise-induced oxidative stress in resistance-trained males. J. Exerc. Nutr. Biochem. 2018, 22, 7–19. [Google Scholar] [CrossRef]
- Smith, W.A.; Fry, A.C.; Tschume, L.C.; Bloomer, R.J. Effect of glycine propionyl-L-carnitine on aerobic and anaerobic exercise performance. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 19–36. [Google Scholar] [CrossRef] [PubMed]
- Barnett, C.; Costill, D.L.; Vukovich, M.D.; Cole, K.J.; Goodpaster, B.H.; Trappe, S.W.; Fink, W.J. Effect of l-carnitine supplementation on muscle and blood carnitine content and lactate accumulation during high-intensity sprint cycling. Int. J. Sport Nutr. 1994, 4, 280–288. [Google Scholar] [CrossRef]
- Reuter, S.; Evans, A. Carnitine and acylcarnitines: Pharmacokinetic, pharmacological and clinical aspects. Clin. Pharmacokinet. 2012, 51, 553–572. [Google Scholar] [CrossRef]
- Westerblad, H.; Bruton, J.; Katz, A. Skeletal muscle: Energy metabolism, fiber types, fatigue and adaptability. Exp. Cell Res. 2010, 316, 3093–3099. [Google Scholar] [CrossRef]
- Harris, R.C.; Foster, C.V.L.; Hultman, E. Acetylcarnitine formation during intense muscular contraction in humans. J. Appl. Physiol. 1987, 63, 440–442. [Google Scholar] [CrossRef]
- Van Loon, L.J.C.; Greenhaff, P.L.; Constantin-Teodosiu, D.; Saris, W.H.M.; Wagenmakers, A.J.M. The effects of increasing exercise intensity on muscle fuel utilisation in humans. J. Physiol. 2001, 536, 295. [Google Scholar] [CrossRef] [PubMed]
- Kasper, J.D.; Meyer, R.A.; Beard, D.A.; Wiseman, R.W. Effects of altered pyruvate dehydrogenase activity on contracting skeletal muscle bioenergetics. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 316, R76–R86. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.J.; Qin, Z.; Wang, P.Y.; Sun, Y.; Liu, X. Muscle fatigue: General understanding and treatment. Exp. Mol. Med. 2017, 49, e384. [Google Scholar] [CrossRef]
- Drăgan, G.I.; Vasiliu, A.; Georgescu, E.; Dumas, I. Studies concerning chronic and acute effects of L-carnitine on some biological parameters in elite athletes. Physiologie 1987, 24, 23–28. [Google Scholar] [PubMed]
- Torma, F.; Gombos, Z.; Jokai, M.; Takeda, M.; Mimura, T.; Radak, Z. High intensity interval training and molecular adaptive response of skeletal muscle. Sport. Med. Health Sci. 2019, 1, 24–32. [Google Scholar] [CrossRef]
- Ross, A.; Leveritt, M. Long-Term Metabolic and Skeletal Muscle Adaptations to Short-Sprint Training and Tapering. Sport. Med. 2001, 31, 1063–1082. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, R.J.; Smith, W.A.; Fisher-Wellman, K.H. Glycine propionyl-L-carnitine increases plasma nitrate/nitrite in resistance trained men. J. Int. Soc. Sports Nutr. 2007, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Siliprandi, N.; Di Lisa, F.; Pieralisi, G.; Ripari, P.; Maccari, F.; Menabo, R.; Giamberardino, M.A.; Vecchiat, L. Metabolic changes induced by maximal exercise in human subjects following L-carnitine administration. BBA Gen. Subj. 1990, 1034, 17–21. [Google Scholar] [CrossRef]
- Vecchiet, L.; Di Lisa, F.; Pieralisi, G.; Ripari, P.; Menab, R.; Giamberardino, M.A.; Siliprandi, N. Influence of L-carnitine administration on maximal physical exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 61, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Coyle, E.F. Endurance exercise performance: The physiology of champions. J. Physiol. 2008, 586, 35–44. [Google Scholar] [CrossRef]
- San-Millán, I.; Brooks, G.A. Assessment of Metabolic Flexibility by Means of Measuring Blood Lactate, Fat, and Carbohydrate Oxidation Responses to Exercise in Professional Endurance Athletes and Less-Fit Individuals. Sport. Med. 2018, 48, 467–479. [Google Scholar] [CrossRef] [Green Version]
- Moran, C.N.; Pitsiladis, Y.P. Tour de France Champions born or made: Where do we take the genetics of performance? J. Sports Sci. 2017, 35, 1411–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gormley, S.; Swain, D.; High, R.; Spina, R.; Dowling, E.; Kotipalli, U.; Gandrakota, R. Effect of intensity of aerobic training on VO2max. Med. Sci. Sports Exerc. 2008, 40, 1336–1343. [Google Scholar] [CrossRef]
- Duran, M.; Loof, N.; Ketting, D.; Dorland, L. Secondary carnitine deficiency. J. Clin. Chem. Clin. Biochem. 1990, 28, 359–363. [Google Scholar]
- Fritz, I.B.; Yue, K.T. Long-chain carnitine acyltransferase and the role of acylcarnitine derivatives in the catalytic increase of fatty acid oxidation induced by carnitine. J. Lipid Res. 1963, 4, 279–288. [Google Scholar] [CrossRef]
- Arenas, J.; Huertas, R.; Campos, Y.; Díaz, A.E.; Villalón, J.M.; Vilas, E. Effects of l-carnitine on the pyruvate dehydrogenase complex and carnitine palmitoyl transferase activities in muscle of endurance athletes. FEBS Lett. 1994, 341, 91–93. [Google Scholar] [CrossRef] [Green Version]
- Gorostiaga, E.M.; Maurer, A.C.; Eclache, J.P. Decrease in respiratory quotient during exercise following L-carnitine supplementation. Int. J. Sports Med. 1989, 10, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Abramowicz, W.N.; Galloway, S.D.R. Effects of acute versus chronic l-Carnitine L-tartrate supplementation on metabolic responses to steady state exercise in males and females. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 386–400. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Studies Included | ITEMS | T | % | MQ | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | ||||
| Trappe et al., 1994 [14] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 9 | 60.00 | A |
| Colombani et al., (1996) [20] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 9 | 60.00 | A |
| Broad et al., (2005) [30] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 12 | 75.00 | G |
| Smith et al., (2008) [34] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 13 | 86.66 | VG |
| Jacobs et al., (2009) [32] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 14 | 93.33 | VG |
| Wall et al., (2011) [23] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 13 | 81.25 | VG |
| Orer et al., (2014) [16] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 14 | 87.50 | VG |
| Arazi & Mehrtash (2017) [31] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 11 | 68.75 | G |
| Koozehchian et al., (2018) [33] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 14 | 87.50 | VG |
| Burrus et al., (2018) [24] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 13 | 81.25 | VG |
| Shannon et al. (2018) [15] | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 10 | 62.50 | A |
| Level of participants | Professional | 2 studies [16,31] | |
| Amateur | 7 studies [14,20,23,24,30,32,33] | ||
| Untrained | 2 studies [15,34] | ||
| Type of l-Carnitine | l-Carnitine | 6 studies [14,16,20,24,31,33] | |
| l-Carnitine L-Tartrate | 3 studies [15,23,30] | ||
| Glycine-Propionyl l-Carnitine | 2 studies [32,34] | ||
| Time of administration | Chronic | 4 weeks | 1 study [30] |
| 8 weeks | 1 study [34] | ||
| 9 weeks | 1 study [33] | ||
| 24 weeks | 2 studies [15,23] | ||
| Acute | 7 days | 1 study [14] | |
| Before/during | 5 studies [16,20,24,31,32] | ||
| Doses used | Chronic | 1 g/day (Propionyl l-Carnitine) | 1 study [34] |
| 2 g/day | 2 studies [30,33] | ||
| 2,72 g/day | 1 study [23] | ||
| 3 g/day (Propionyl l-Carnitine or l-Carnitine) | 2 studies [15,34] | ||
| Acute | 3 g (l-Carnitine) 3 g (Propionyl l-Carnitine) | 3 studies [16,24,31] 1 study [32] | |
| 4 g (l-Carnitine) | 3 studies [14,16,20] | ||
| Author/s | Population | Intervention | Outcomes Analyzed | Main Results | |
|---|---|---|---|---|---|
| Chronic l-C supplementation | |||||
| Smith et al., 2008 [34] | 32 untrained participants (9 men and 23 women aged between 18 and 44 years) | 1 g/day of PL-C n = 11 3 g/day of PL-C n = 12 Duration: 8 weeks | Test of anaerobic power (30 s on cycle ergometer): | GPL-C-1 | GPL-C-3 |
| ↔ | ↔ | |||
| ↔ | ↔ | |||
| ↔ | ↔ | |||
| ↔ | ↔ | |||
| Wall et al., 2011 [23] | 14 moderately trained recreational athletes (25.9 ± 2.1 years) | 4 g/day l-CLT (2,72 g/day l-C) with 160 g of CHO distributed 2 times per day (1 at breakfast and 4 h later) Duration: 24 weeks | 30 min at 80% O2 max on cycle ergometer: | Week12 | Week24 |
| ↔ | ↑ | |||
| 30 min “all out” on cycle ergometer: | |||||
| ↔ | ↑ | |||
| Shannon et al., 2018 [15] | 14 untrained men (23 ± 2 years) | 4.50 g/day of l-CLT (3 g/day l-C) with 160 g of CHO distributed 2 times per day (1 at breakfast and 4 h later) Duration: 24 weeks | HIIT on cycle ergometer (100% O2 max): | ||
| ↔ | ||||
| ↔ | ||||
| ↔ | ||||
| Koozehchian et al., 2018 [33] | 23 endurance-trained males (25 ± 2 years) | 2 g/day of l-C caps of 1 g (one at breakfast and the other at lunch) Duration: 9 weeks | Performance on bench press: | ||
| ↔ | ||||
| ↔ | ||||
| Performance on leg press: | |||||
| ↑ | ||||
| ↑ | ||||
| Anaerobic performance (30 s Wingate test): | |||||
| ↔ | ||||
| ↑ | ||||
| Acute l-C supplementation | |||||
| Trappe et al., 1994 [14] | 20 trained collegiate male swimmers (20.1 ± 0.6 years) | 4 g/day of l-C in a citrus drink twice daily for 7 days | Five 91.4 m (100 yd) repeated swims at a supramaximal intensity with 2 min rest between each | ||
| ↔ | ||||
| Jacobs et al., 2009 [32] | 24 resistance-trained men (25.2 ± 3.6 years) | 4,5 g GPL-C (3 g PL-C) with 8 oz of water 90 min before the test | Wingate test (5 sprints of 10 s on cycle ergometer) | ||
| ↑ | ||||
| ↑ | ||||
| ↔ | ||||
| Orer & Guzel, 2014 [16] | 26 male professional soccer players (18.42 ± 0.50) | 3 g of l-C with a glass of juice (n = 12) LK3 4 g of l-C with a glass of juice (n = 14) LK4 1 h before the test | Graded exercise test on the treadmill until exhaustion: | LK3 | LK4 |
| Speed at: | |||||
| ↑ | ↔ | |||
| ↑ | ↑ | |||
| ↑ | ↑ | |||
| Borg Scale at: | |||||
| ↑ | ↔ | |||
| ↑ | ↑ | |||
| ↔ | ↑ | |||
| Arazi and Mehrtash (2017) [31] | 18 male artistic gymnasts (21 ± 2.12 years) | 3 g of l-C 90 min before the test | Anaerobic sprint test (RAST) | ||
| ↑ | ||||
| ↔ | ||||
| 20 m shuttle run | |||||
| ↑ | ||||
| Burrus et al., 2018 [24] | 10 moderately active men (27 ± 4 years) | 3 g l-C in 200 mL of H2O 3 h before the exercise 94 g of CHO in 500 mL H2O 2 h before the exercise 94 g of CHO in 500 mL H2O 30 min before the exercise | Exercise on cycle ergometer at 85% O2 Peak: | ||
| ↔ | ||||
| ↔ | ||||
| Author/s | Population | Intervention | Outcomes Analyzed | Main Results | |
|---|---|---|---|---|---|
| Chronic l-C supplementation | |||||
| Broad et al., 2005 [30] | 15 endurance-trained men (20 to 46 years) | 3 g of l-CLT (2 g l-C) Duration: 4 weeks and 2 weeks washout period between them | 90 min at 65% O2 max on cycle ergometer: | ||
| ↔ | ||||
| ↔ | ||||
| 20 km time trial duration: Total time trial | |||||
| ↔ | ||||
| Smith et al., 2008 [34] | 32 untrained participants (9 men and 23 women (18 to 44 years) | 1 g/day of PL-C n = 11 3 g/day of PL-C n= 12 Duration: 8 weeks | Aerobic exercise test on the treadmill: | GPL-C-1 | GPL-C-3 |
| ↔ | ↔ | |||
| ↔ | ↔ | |||
| ↔ | ↔ | |||
| Wall et al., 2011 [23] | 14 Moderately trained recreational athletes (25.9 ± 2.1 years) | 4 g of l-CLT (2,72 l-C) with 160 g of CHO distributed 2 times per day (1 at breakfast and 4 h later Duration: 24 weeks | Test on cycle ergometer at 50% O2 max: | week 12 | week 24 |
| ↔ | ↔ | |||
| Acute l-C supplementation | |||||
| Colombani et al., 1996 [20] | 7 endurance-trained men (36 ± 3 years) | 2 g of l-C 2 h before the marathon and 2 g of l-C after 20 km 125 mL of sugar tea every 5 km and 500 mL during the next hour after the marathon | Marathon: | ||
| ↔ | ||||
| Burrus et al., 2018 [24] | 10 moderately active men (27 ± 4 years) | 3 g of l-C + 200 mL of H2O 3 h before the exercise 94 g of CHO in 500 mL of H2O 2 h before the exercise 94 g of CHO in 500 mL of H2O 30 min before the exercise | Test on cycle ergometer at 65% O2 peak: | ||
| ↔ | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mielgo-Ayuso, J.; Pietrantonio, L.; Viribay, A.; Calleja-González, J.; González-Bernal, J.; Fernández-Lázaro, D. Effect of Acute and Chronic Oral l-Carnitine Supplementation on Exercise Performance Based on the Exercise Intensity: A Systematic Review. Nutrients 2021, 13, 4359. https://doi.org/10.3390/nu13124359
Mielgo-Ayuso J, Pietrantonio L, Viribay A, Calleja-González J, González-Bernal J, Fernández-Lázaro D. Effect of Acute and Chronic Oral l-Carnitine Supplementation on Exercise Performance Based on the Exercise Intensity: A Systematic Review. Nutrients. 2021; 13(12):4359. https://doi.org/10.3390/nu13124359
Chicago/Turabian StyleMielgo-Ayuso, Juan, Laura Pietrantonio, Aitor Viribay, Julio Calleja-González, Jerónimo González-Bernal, and Diego Fernández-Lázaro. 2021. "Effect of Acute and Chronic Oral l-Carnitine Supplementation on Exercise Performance Based on the Exercise Intensity: A Systematic Review" Nutrients 13, no. 12: 4359. https://doi.org/10.3390/nu13124359
APA StyleMielgo-Ayuso, J., Pietrantonio, L., Viribay, A., Calleja-González, J., González-Bernal, J., & Fernández-Lázaro, D. (2021). Effect of Acute and Chronic Oral l-Carnitine Supplementation on Exercise Performance Based on the Exercise Intensity: A Systematic Review. Nutrients, 13(12), 4359. https://doi.org/10.3390/nu13124359