
Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome


{kind=link}
Abstract
:1. Introduction
2. Biomarkers of Creatine Metabolism in Post-Viral Fatigue Syndrome
3. Dietary Creatine and Alternatives in Syndromes with Prolonged Fatigue
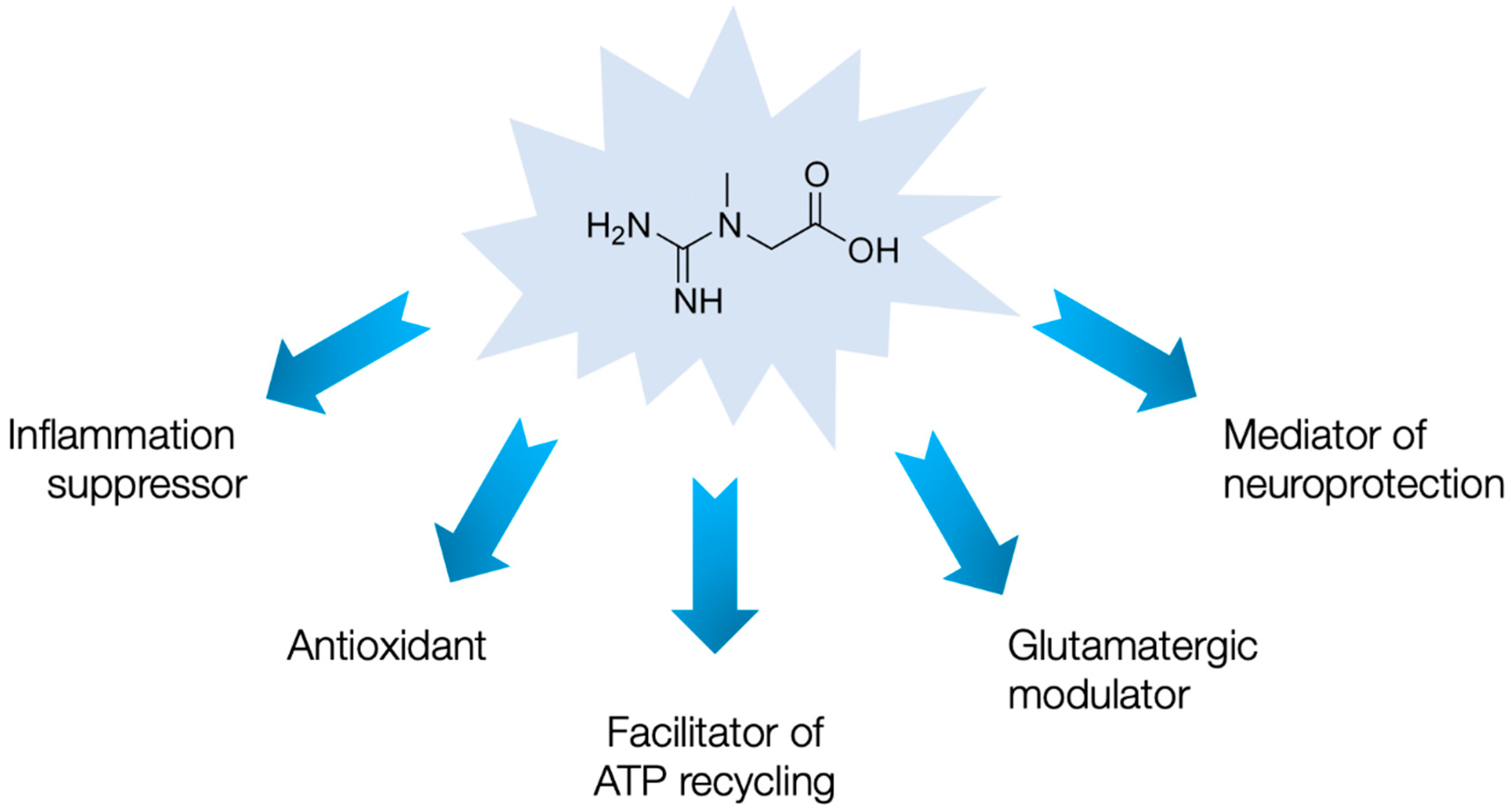
4. Alternative Mechanisms of Creatine Action
5. Open Questions and Creatine in the Post-COVID-19 World
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision). 2019. Available online: https://icd.who.int/browse11/l-m/en (accessed on 15 December 2020).
- Unger, E.R.; Lin, J.S.; Brimmer, D.J.; Lapp, C.W.; Komaroff, A.L.; Nath, A.; Laird, S.; Iskander, J. CDC grand rounds: Chronic fatigue syndrome-advancing research and clinical education. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 1434–1438. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.J.; Son, C.G. Review of case definitions for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2020, 18, 289. [Google Scholar] [CrossRef]
- Sandler, C.X.; Lloyd, A.R. Chronic fatigue syndrome: Progress and possibilities. Med. J. Aust. 2020, 212, 428–433. [Google Scholar] [CrossRef]
- Kim, D.Y.; Lee, J.S.; Park, S.Y.; Kim, S.J.; Son, C.G. Systematic review of randomized controlled trials for chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J. Transl. Med. 2020, 18, 7. [Google Scholar] [CrossRef] [Green Version]
- Morris, G.; Berk, M.; Walder, K.; Maes, M. The putative role of viruses, bacteria, and chronic fungal biotoxin exposure in the genesis of intractable fatigue accompanied by cognitive and physical disability. Mol. Neurobiol. 2016, 53, 2550–2571. [Google Scholar] [CrossRef]
- Afari, N.; Buchwald, D. Chronic fatigue syndrome: A review. Am. J. Psychiatry 2003, 160, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Ostojic, S.M. Postviral fatigue syndrome and creatine: A piece of the puzzle? Nutr. Neurosci 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Archard, L.C.; Bowles, N.E.; Behan, P.O.; Bell, E.J.; Doyle, D. Postviral fatigue syndrome: Persistence of enterovirus RNA in muscle and elevated creatine kinase. J. R. Soc. Med. 1988, 81, 326–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preedy, V.R.; Smith, D.G.; Salisbury, J.R.; Peters, T.J. Biochemical and muscle studies in patients with acute onset post-viral fatigue syndrome. J. Clin. Pathol. 1993, 46, 722–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.; Smith, D.G.; Doyle, D.; Fowler, C.J. Chronic fatigue: Electromyographic and neuropathological evaluation. J. Neurol. 1993, 240, 435–438. [Google Scholar] [CrossRef]
- Wassif, W.S.; Sherman, D.; Salisbury, J.R.; Peters, T.J. Use of dynamic tests of muscle function and histomorphometry of quadriceps muscle biopsies in the investigation of patients with chronic alcohol misuse and chronic fatigue syndrome. Ann. Clin. Biochem. 1994, 31, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Cannon, J.G.; Angel, J.B.; Abad, L.W.; O’Grady, J.; Lundgren, N.; Fagioli, L.; Komaroff, A.L. Hormonal influences on stress-induced neutrophil mobilization in health and chronic fatigue syndrome. J. Clin. Immunol. 1998, 18, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Lopaschuk, G.; Zhu, G.; Walker, D.; Catellier, D.; Burton, D.; Teo, K.; Collins-Nakai, R.; Montague, T. Skeletal muscle metabolism in the chronic fatigue syndrome. In vivo assessment by 31P nuclear magnetic resonance spectroscopy. Chest 1992, 102, 1716–1722. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.R.; Taylor, D.J.; Kemp, G.J.; Radda, G.K. Skeletal muscle bioenergetics in the chronic fatigue syndrome. J. Neurol. Neurosurg. Psychiatry 1993, 56, 679–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCully, K.K.; Natelson, B.H.; Iotti, S.; Sisto, S.; Leigh, J.S., Jr. Reduced oxidative muscle metabolism in chronic fatigue syndrome. Muscle Nerve 1996, 19, 621–625. [Google Scholar] [CrossRef]
- Block, W.; Träber, F.; Kuhl, C.K.; Keller, E.; Lamerichs, R.; Karitzky, J.; Rink, H.; Schild, H.H. 31P-MR- [31P-mr spectroscopy of peripheral skeletal musculature under load: Demonstration of normal energy metabolites compared with metabolic muscle diseases]. Rofo 1998, 168, 250–257. [Google Scholar] [CrossRef]
- McCully, K.K.; Smith, S.; Rajaei, S.; Leigh, J.S., Jr.; Natelson, B.H. Blood flow and muscle metabolism in chronic fatigue syndrome. Clin. Sci. 2003, 104, 641–647. [Google Scholar] [CrossRef] [Green Version]
- McCully, K.K.; Smith, S.; Rajaei, S.; Leigh, J.S., Jr.; Natelson, B.H. Muscle metabolism with blood flow restriction in chronic fatigue syndrome. J. Appl. Physiol. 2004, 96, 871–878. [Google Scholar] [CrossRef] [Green Version]
- Brooks, J.C.; Roberts, N.; Whitehouse, G.; Majeed, T. Proton magnetic resonance spectroscopy and morphometry of the hippocampus in chronic fatigue syndrome. Br. J. Radiol. 2000, 73, 1206–1208. [Google Scholar] [CrossRef]
- Tomoda, A.; Miike, T.; Yamada, E.; Honda, H.; Moroi, T.; Ogawa, M.; Ohtani, Y.; Morishita, S. Chronic fatigue syndrome in childhood. Brain Dev. 2000, 22, 60–64. [Google Scholar] [CrossRef]
- Forton, D.M.; Allsop, J.M.; Main, J.; Foster, G.R.; Thomas, H.C.; Taylor-Robinson, S.D. Evidence for a cerebral effect of the hepatitis C virus. Lancet 2001, 358, 38–39. [Google Scholar] [CrossRef]
- Puri, B.K.; Counsell, S.J.; Zaman, R.; Main, J.; Collins, A.G.; Hajnal, J.V.; Davey, N.J. Relative increase in choline in the occipital cortex in chronic fatigue syndrome. Acta Psychiatr. Scand. 2002, 106, 224–226. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.; Condon, B.R.; Gow, J.W.; Brennan, D.; Hadley, D.M. Proton magnetic resonance spectroscopy of basal ganglia in chronic fatigue syndrome. Neuroreport 2003, 14, 225–228. [Google Scholar] [CrossRef]
- Hollingsworth, K.G.; Jones, D.E.; Taylor, R.; Blamire, A.M.; Newton, J.L. Impaired cardiovascular response to standing in chronic fatigue syndrome. Eur. J. Clin. Investig. 2010, 40, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Van der Schaaf, M.E.; De Lange, F.P.; Schmits, I.C.; Geurts, D.E.M.; Roelofs, K.; van der Meer, J.W.M.; Toni, I.; Knoop, H. Prefrontal structure varies as a function of pain symptoms in chronic fatigue syndrome. Biol. Psychiatry 2017, 81, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Mueller, C.; Lin, J.C.; Sheriff, S.; Maudsley, A.A.; Younger, J.W. Evidence of widespread metabolite abnormalities in Myalgic encephalomyelitis/chronic fatigue syndrome: Assessment with whole-brain magnetic resonance spectroscopy. Brain Imaging Behav. 2020, 14, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Malatji, B.G.; Meyer, H.; Mason, S.; Engelke, U.F.H.; Wevers, R.A.; van Reenen, M.; Reinecke, C.J. A diagnostic biomarker profile for fibromyalgia syndrome based on an NMR metabolomics study of selected patients and controls. BMC Neurol. 2017, 17, 88. [Google Scholar] [CrossRef]
- Armstrong, C.W.; McGregor, N.R.; Lewis, D.P.; Butt, H.L.; Gooley, P.R. Metabolic profiling reveals anomalous energy metabolism and oxidative stress pathways in chronic fatigue syndrome patients. Metabolomics 2015, 11, 1626–1639. [Google Scholar] [CrossRef]
- Nacul, L.; de Barros, B.; Kingdon, C.C.; Cliff, J.M.; Clark, T.G.; Mudie, K.; Dockrell, H.M.; Lacerda, E.M. Evidence of clinical pathology abnormalities in people with myalgic encephalomyelitis/chronic fatigue syndrome (me/cfs) from an analytic cross-sectional study. Diagnostics 2019, 9, 41. [Google Scholar] [CrossRef] [Green Version]
- Almenar-Pérez, E.; Sarría, L.; Nathanson, L.; Oltra, E. Assessing diagnostic value of microRNAs from peripheral blood mononuclear cells and extracellular vesicles in myalgic encephalomyelitis/chronic fatigue syndrome. Sci. Rep. 2020, 10, 2064. [Google Scholar] [CrossRef] [Green Version]
- Germain, A.; Ruppert, D.; Levine, S.M.; Hanson, M.R. Metabolic profiling of a myalgic encephalomyelitis/chronic fatigue syndrome discovery cohort reveals disturbances in fatty acid and lipid metabolism. Mol. Biosyst. 2017, 13, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomas, C.; Brown, A.; Strassheim, V.; Elson, J.L.; Newton, J.; Manning, P. Cellular bioenergetics is impaired in patients with chronic fatigue syndrome. PLoS ONE 2017, 12, e0186802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwers, F.M.; Van Der Werf, S.; Bleijenberg, G.; Van Der Zee, L.; Van Der Meer, J.W. The effect of a polynutrient supplement on fatigue and physical activity of patients with chronic fatigue syndrome: A double-blind randomized controlled trial. QJM 2002, 95, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Alves, C.R.; Santiago, B.M.; Lima, F.R.; Otaduy, M.C.; Calich, A.L.; Tritto, A.C.; de Sá Pinto, A.L.; Roschel, H.; Leite, C.C.; Benatti, F.B.; et al. Creatine supplementation in fibromyalgia: A randomized, double-blind, placebo-controlled trial. Arthritis Care Res. 2013, 65, 1449–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostojic, S.M.; Stojanovic, M.; Drid, P.; Hoffman, J.R.; Sekulic, D.; Zenic, N. Supplementation with guanidinoacetic acid in women with chronic fatigue syndrome. Nutrients 2016, 8, 72. [Google Scholar] [CrossRef] [PubMed]
- Trabal, J.; Leyes, P.; Fernández-Solá, J.; Forga, M.; Fernández-Huerta, J. Patterns of food avoidance in chronic fatigue syndrome: Is there a case for dietary recommendations? Nutr. Hosp. 2012, 27, 659–662. [Google Scholar] [PubMed]
- Jenkins, M.; Rayman, M. Nutrient intake is unrelated to nutrient status in patients with chronic fatigue syndrome. J. Nutr. Environ. Med. 2005, 15, 177–189. [Google Scholar] [CrossRef]
- Riesberg, L.A.; Weed, S.A.; McDonald, T.L.; Eckerson, J.M.; Drescher, K.M. Beyond muscles: The untapped potential of creatine. Int. Immunopharmacol. 2016, 37, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Dolan, E.; Gualano, B.; Rawson, E.S. Beyond muscle: The effects of creatine supplementation on brain creatine, cognitive processing, and traumatic brain injury. Eur. J. Sport Sci. 2019, 19, 1–14. [Google Scholar] [CrossRef]
- Marques, E.P.; Wyse, A.T.S. Creatine as a neuroprotector: An actor that can play many parts. Neurotox. Res. 2019, 36, 411–423. [Google Scholar] [CrossRef]
- Balestrino, M.; Sarocchi, M.; Adriano, E.; Spallarossa, P. Potential of creatine or phosphocreatine supplementation in cerebrovascular disease and in ischemic heart disease. Amino Acids 2016, 48, 1955–1967. [Google Scholar] [CrossRef] [PubMed]
- Beal, M.F. Neuroprotective effects of creatine. Amino Acids 2011, 40, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.; Maes, M. Mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome explained by activated immuno-inflammatory, oxidative and nitrosative stress pathways. Metab. Brain Dis. 2014, 29, 19–36. [Google Scholar] [CrossRef] [PubMed]
- Leland, K.M.; McDonald, T.L.; Drescher, K.M. Effect of creatine, creatinine, and creatine ethyl ester on TLR expression in macrophages. Int. Immunopharmacol. 2011, 11, 1341–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambuzza, M.E.; Salmeri, F.M.; Soraci, L.; Soraci, G.; Sofo, V.; Marino, S.; Bramanti, P. The role of toll-like receptors in chronic fatigue syndrome/myalgic encephalomyelitis: A new promising therapeutic approach? CNS Neurol. Disord. Drug Targets 2015, 14, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Sestili, P.; Martinelli, C.; Colombo, E.; Barbieri, E.; Potenza, L.; Sartini, S.; Fimognari, C. Creatine as an antioxidant. Amino Acids 2011, 40, 1385–1396. [Google Scholar] [CrossRef]
- Guidi, C.; Potenza, L.; Sestili, P.; Martinelli, C.; Guescini, M.; Stocchi, L.; Zeppa, S.; Polidori, E.; Annibalini, G.; Stocchi, V. Differential effect of creatine on oxidatively-injured mitochondrial and nuclear DNA. Biochim. Biophys. Acta 2008, 1780, 16–26. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, H.G.; Lee, D.S.; Son, C.G. Oxidative stress is a convincing contributor to idiopathic chronic fatigue. Sci. Rep. 2018, 8, 12890. [Google Scholar] [CrossRef]
- Koga, Y.; Takahashi, H.; Oikawa, D.; Tachibana, T.; Denbow, D.M.; Furuse, M. Brain creatine functions to attenuate acute stress responses through GABAnergic system in chicks. Neuroscience 2005, 132, 65–71. [Google Scholar] [CrossRef]
- Royes, L.F.; Fighera, M.R.; Furian, A.F.; Oliveira, M.S.; Fiorenza, N.G.; Ferreira, J.; da Silva, A.C.; Priel, M.R.; Ueda, E.S.; Calixto, J.B.; et al. Neuromodulatory effect of creatine on extracellular action potentials in rat hippocampus: Role of NMDA receptors. Neurochem. Int. 2008, 53, 33–37. [Google Scholar] [CrossRef]
- Rönnbäck, L.; Hansson, E. On the potential role of glutamate transport in mental fatigue. J. Neuroinflamm. 2004, 1, 22. [Google Scholar] [CrossRef] [Green Version]
- Béard, E.; Braissant, O. Synthesis and transport of creatine in the CNS: Importance for cerebral functions. J. Neurochem. 2010, 115, 297–313. [Google Scholar]
- Ainsley Dean, P.J.; Arikan, G.; Opitz, B.; Sterr, A. Potential for use of creatine supplementation following mild traumatic brain injury. Concussion 2017, 2, CNC34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adriano, E.; Gulino, M.; Arkel, M.; Salis, A.; Damonte, G.; Liessi, N.; Millo, E.; Garbati, P.; Balestrino, M. Di-acetyl creatine ethyl ester, a new creatine derivative for the possible treatment of creatine transporter deficiency. Neurosci. Lett. 2018, 665, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.H.; Wing, Y.K.; Yu, M.W.; Leung, C.M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.; Lam, S.P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: Long-term follow-up. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Ostojic, S.M. Can creatine help in pulmonary rehabilitation after COVID-19? Ther. Adv. Respir. Dis. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Butters, D.; Whitehouse, M. COVID-19 and nutriceutical therapies, especially using zinc to supplement antimicrobials. Inflammopharmacology 2020, in press. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostojic, S.M. Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome. Nutrients 2021, 13, 503. https://doi.org/10.3390/nu13020503
Ostojic SM. Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome. Nutrients. 2021; 13(2):503. https://doi.org/10.3390/nu13020503
Chicago/Turabian StyleOstojic, Sergej M. 2021. "Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome" Nutrients 13, no. 2: 503. https://doi.org/10.3390/nu13020503
APA StyleOstojic, S. M. (2021). Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome. Nutrients, 13(2), 503. https://doi.org/10.3390/nu13020503