
Exploring the Attitudes of Health Professionals Providing Care to Patients Undergoing Treatment for Upper Gastrointestinal Cancers to Different Models of Nutrition Care Delivery: A Qualitative Investigation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Procedures
2.3. Analysis
3. Results
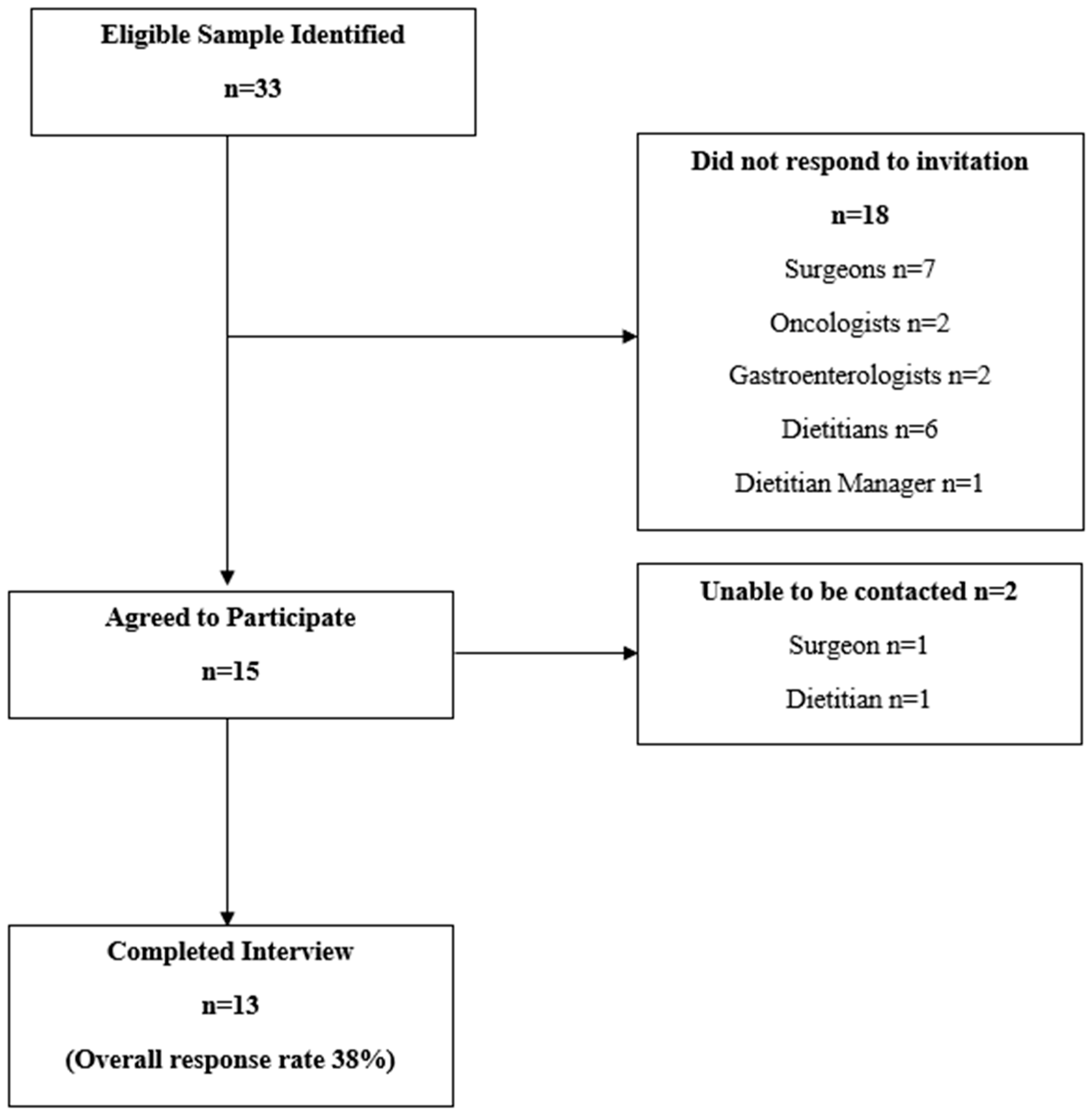
3.1. Participant Sample
3.2. Thematic Analysis
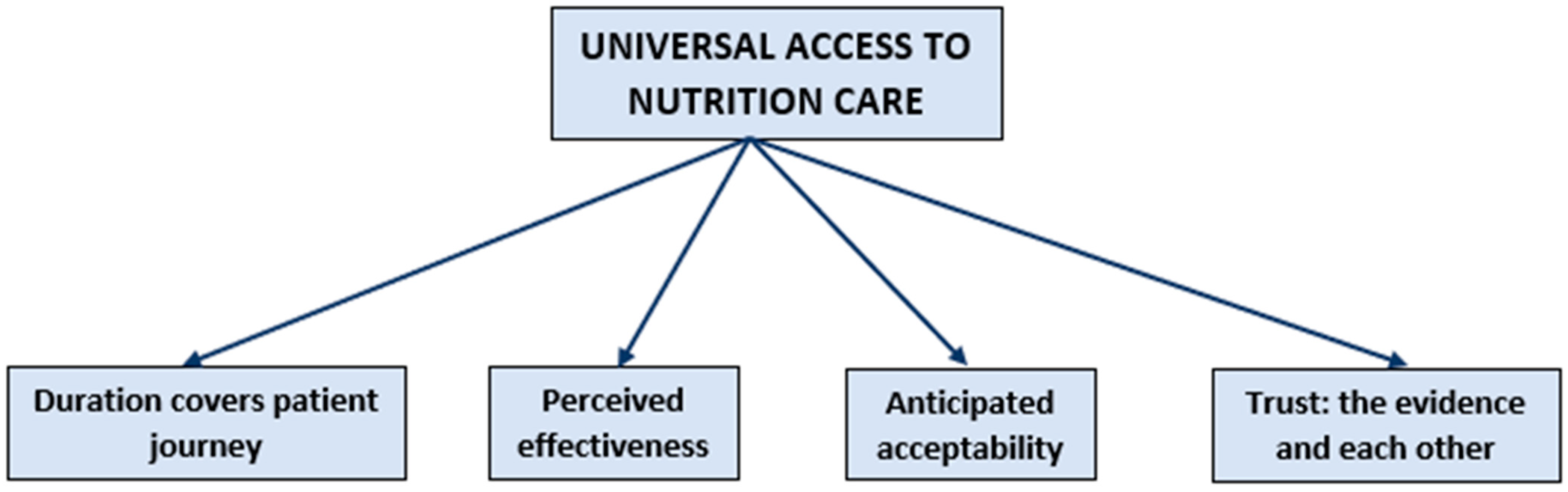
3.3. Universal Access to Nutrition Care for People with Upper Gastrointestinal Cancers
#12 “No, I think, no I think it’s never futile, I think that people should be nourished unless it’s truly end of life issues. Then I think there is a role for caring for nutrition”
3.4. The Duration of Nutrition Intervention Covers the Patient Journey
#11 “you know it should be 6 months or 3 months post completion of their treatment. I think that 18 weeks doesn’t actually cover a lot of our patients’ complete treatment”
3.5. Perceived Effectiveness and Trust: The Evidence
#9 “There is very good evidence that nutrition impacts on, directly on survival, impacts the ability to have treatment, improves quality of life. I think there’s very good evidence”
3.6. Anticipated Acceptability and Trust: The Team
#12 “Maybe there is a generational issue, maybe older patients would rather a face-to-face or telephone conversation than using a device or app”
#6 “So, better partnerships with our regional hospitals would be really important. It’s around resource and kind of service delivery, understanding our patient journey and where our patients are being seen, and going”
#1 “I suppose it’s about those relationships, it’s about the staff here, the premise is that the medical staff actually know the dietitian. I’m going to say respect but feel comfortable and confident in their clinical skills and the information they give”
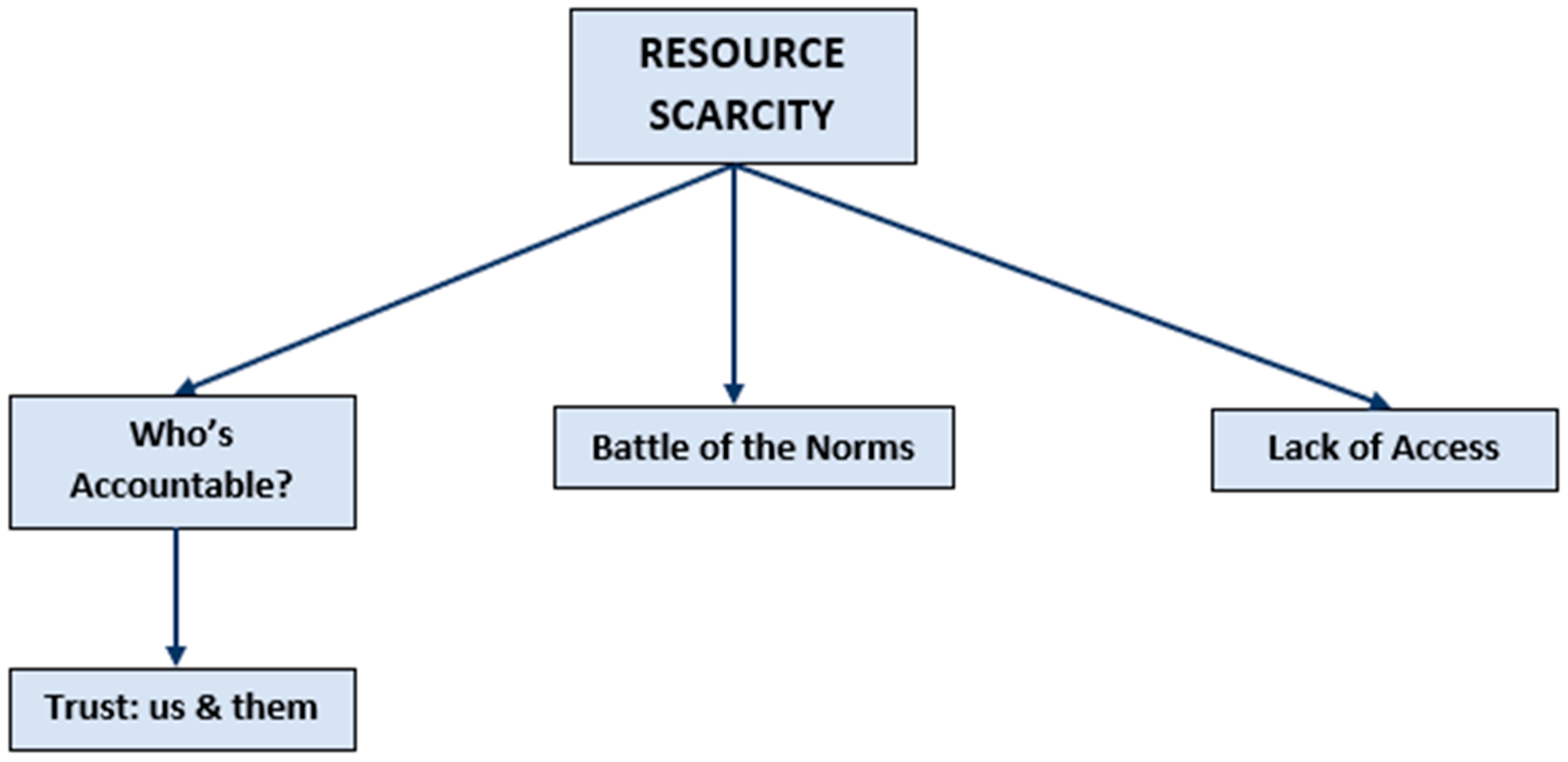
3.7. Resource Scarcity
#9 “Well I think that it’s well recognised that nutrition is incredibly important, however where the resources are so ahh poor, you know, both in umm medical and allied that we really don’t optimise nutrition and there is lots of data around malnutrition in patient populations obviously, so it’s a real issue for us”
3.8. Who Is Accountable?
#11 “It’s very, I think it’s very hard for one person to take ownership and claim ‘I need to be responsible for their weight loss’”
3.9. Trust: Us and Them
#1 “Their view (medical staff) is, they’re fine because they’re, you know they’ve got a BMI of 23 or whatever but in actual fact they may not be fine. We forget that in, they are living off soup in the short term, but they’re eating, so, it is about changing their minds as well”
#3 “I think you’ll find there is some traditionalists who ‘I’ve done this the same way always, my patients do very well, I fit within the ANZGOSA death and complications guidelines’”
3.10. Battle of the Norms
#6 “I think there is an apathy towards weight change in our oncology patients, especially in our UGI in that there is an acceptance by our medical teams and nursing staff that all patients will lose weight on their journey”
3.11. Lack of Access
#9 “So, we’ve now got a 6–8 week waiting time for a new patient and in that time, if you’ve got oesophageal cancer, you’re going to lose a lot of weight and even block your oesophagus off. Whereas if you started treatment earlier, so it’s not really acceptable but that’s what we’ve got”
#11 “It’s just that pre-treatment part, the from the point of diagnosis to treatment is the part where we have a big, big issue and a big downfall”
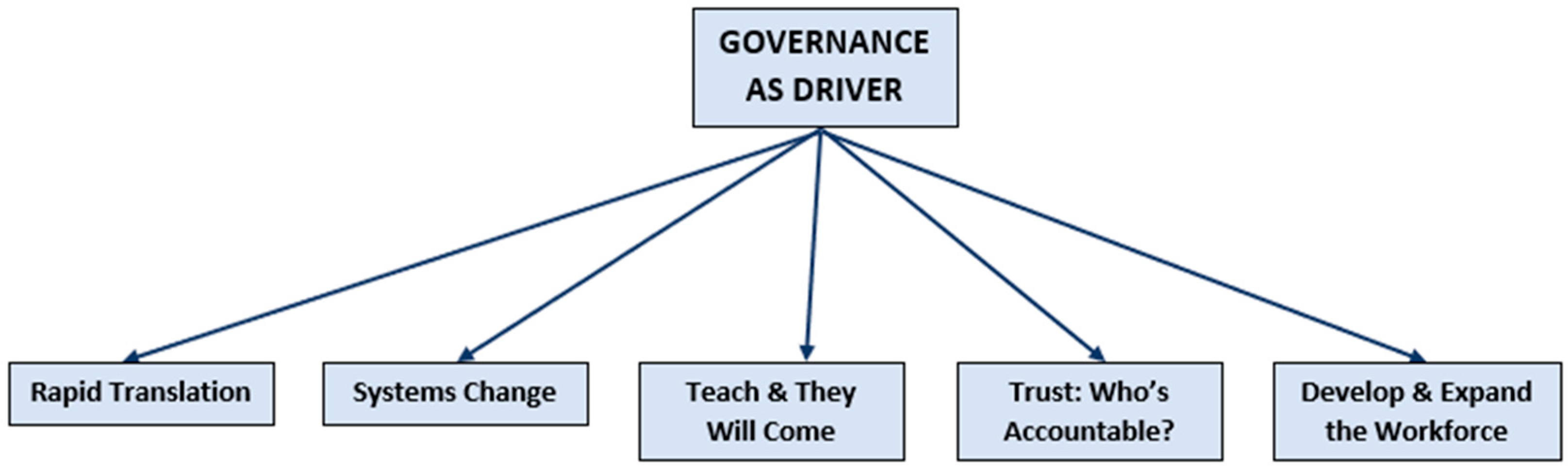
3.12. Governance as Driver
#3 “Once we’ve got the evidence and the information out there, that’s when a group, a governing body like ANZGOSA which is appointed by the College of Surgeons to run upper GI surgery in this country can send out a draft position paper to all upper GI surgeons in the country”
3.13. Trust: Who Is Accountable?
#6 “Well how do we get our medical buy in?’ because that’s more important I think”
3.14. Systems Change
#2 “If we could get a model and we are so far off this but would replicate something like what the breast patients get. And that’s the one stop shop. The come in and they see their surgeon, they see their oncologist, they see their dietitian, they see their nurse…”
3.15. Develop and Expand the Workforce
#9 “The other thing is sort of community based dietitians, but they would need a competency in this area. Umm, and I know for psychology umm, the MPCCC is doing a project looking at upskilling community based psychologists knowing that we’re never going to have enough in the hospital system, then if you had community based, there’s enough people with cancer in the community that you could have practices that, that you know, specialise in this”.
#6 “We need the right person to be delivering the right task at the right time and that doesn’t necessarily need to be a specialist. I think there is a care partnership that would be possible”
3.16. Teach and They Will Come
#6 “So I think that having nutrition taught in a medical degree is really important and should be one of the core subjects for them”
3.17. Rapid Translation
#3 “The upper GI/oncological/radiotherapy/surgical community, we present, we produce papers, present at meetings, present at our craft group conferences. The only way to get surgeons to change is to get up there and talk about it”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Health and Human Services. The Australian Charter of Healthcare Rights in Victoria; State Government of Victoria: Victoria, Australia, 2017.
- World Health Organization. Basic Documents: Forty-Ninth Edition (Including Amendments Adopted Up to 31 May 2019); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Department of Health and Human Services. Malnutrition in Victorian Cancer Services: Malnutrition Governance Toolkit; State Government of Victoria: Victoria, Australia, 2014.
- Australian Commision on Safety and Quality in Healthcare. The NSQHS Standards, Comprehensive Care Standard, Minimising Patient Harm. Action 5.27: Nutrition and Hydration; Australian Commision on Safety and Quality in Healthcare: Sydney, Australia, 2019.
- Andreyev, H.J.; Norman, A.R.; Oates, J.; Cunningham, D. Why do patients with weight loss have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur. J. Cancer 1998, 34, 503–509. [Google Scholar] [CrossRef]
- Choi, W.J.; Kim, J. Nutritional Care of Gastric Cancer Patients with Clinical Outcomes and Complications: A Review. Clin. Nutr. Res. 2016, 5, 65–78. [Google Scholar] [CrossRef] [Green Version]
- Garth, A.K.; Newsome, C.M.; Simmance, N.; Crowe, T.C. Nutritional status, nutrition practices and post-operative complications in patients with gastrointestinal cancer. J. Hum. Nutr. Diet. 2010, 23, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Odelli, C.; Burgess, D.; Bateman, L.; Hughes, A.; Ackland, S.; Gillies, J.; Collins, C.E. Nutrition support improves patient outcomes, treatment tolerance and admission characteristics in oesophageal cancer. Clin. Oncol. 2005, 17, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Arends, J. The causes and consequences of cancer-associated malnutrition. Eur. J. Oncol. Nurs. Off. J. Eur. Oncol. Nurs. Soc. 2005, 9 (Suppl. 2), S51–S63. [Google Scholar] [CrossRef]
- Sandrucci, S.; Beets, G.; Braga, M.; Dejong, K.; Demartines, N. Perioperative nutrition and enhanced recovery after surgery in gastrointestinal cancer patients. A position paper by the ESSO task force in collaboration with the ERAS society (ERAS coalition). Eur. J. Surg. Oncol. 2018, 44, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Isenring, E.A.; Capra, S.; Bauer, J.D. Nutrition intervention is beneficial in oncology outpatients receiving radiotherapy to the gastrointestinal or head and neck area. Br. J. Cancer 2004, 91, 447–452. [Google Scholar] [CrossRef]
- Silvers, M.A.; Savva, J.; Huggins, C.E.; Truby, H.; Haines, T. Potential benefits of early nutritional intervention in adults with upper gastrointestinal cancer: A pilot randomised trial. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2014, 22, 3035–3044. [Google Scholar] [CrossRef]
- Furness, K.; Silvers, M.A.; Savva, J.; Huggins, C.E.; Truby, H.; Haines, T. Long-term follow-up of the potential benefits of early nutritional intervention in adults with upper gastrointestinal cancer: A pilot randomised trial. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2017, 25, 3587–3593. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hutterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [Green Version]
- Isenring, E.; Zabel, R.; Bannister, M.; Brown, T.; Findlay, M.; Kiss, N.; Loeliger, J.; Johnstone, C.; Camilleri, B.; Davidson, W.; et al. Updated evidence-based practice guidelines for the nutritional management of patients receiving radiation therapy and/or chemotherapy. Nutr. Diet. 2013, 70, 312–324. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hubner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Carey, S.; He, L.; Ferrie, S. Nutritional management of patients undergoing major upper gastrointestinal surgery: A survey of current practice in Australia. Nutr. Diet. 2010, 67, 219–223. [Google Scholar] [CrossRef]
- Caccialanza, R.; Cereda, E.; Pinto, C.; Cotogni, P.; Farina, G.; Gavazzi, C.; Gandini, C.; Nardi, M.; Zagonel, V.; Pedrazzoli, P. Awareness and consideration of malnutrition among oncologists: Insights from an exploratory survey. Nutrition 2016, 32, 1028–1032. [Google Scholar] [CrossRef] [PubMed]
- Pirlich, M.; Schütz, T.; Norman, K.; Gastell, S.; Lübke, H.J.; Bischoff, S.C.; Bolder, U.; Frieling, T.; Güldenzoph, H.; Hahn, K.; et al. The German hospital malnutrition study. Clin. Nutr. 2006, 25, 563–572. [Google Scholar] [CrossRef]
- Cancer Council Australia. Optimal Care Pathway for People with Oesophagogastric Cancer 2016. Available online: https://www.cancer.org.au/content/ocp/health/optimal-care-pathway-for-people-with-oesophagogastric-cancer-june-2016.pdf#_ga=2.138999856.2055128893.1575446242-1356875617.1574729126 (accessed on 9 May 2020).
- Cancer Council Australia. Optimal Care Pathway for People with Pancreatic Cancer 2016. Available online: https://www.cancer.org.au/content/ocp/health/optimal-care-pathway-for-people-with-pancreatic-cancer-june-2016.pdf#_ga=2.210440982.2055128893.1575446242-1356875617.1574729126 (accessed on 9 May 2020).
- Low, D.E.; Allum, W.; De Manzoni, G.; Ferri, L.; Immanuel, A.; Kuppusamy, M.; Law, S.; Lindblad, M.; Maynard, N.; Neal, J.; et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery After Surgery (ERAS((R))) Society Recommendations. World J. Surg. 2019, 43, 299–330. [Google Scholar] [CrossRef]
- Lassen, K.; Coolsen, M.M.E.; Slim, K.; Carli, F.; de Aguilar-Nascimento, J.E.; Schäfer, M.; Parks, R.W.; Fearon, K.C.H.; Lobo, D.N.; Demartines, N.; et al. Guidelines for Perioperative Care for Pancreaticoduodenectomy: Enhanced Recovery After Surgery (ERAS®) Society Recommendations. World J. Surg. 2013, 37, 240–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortensen, K.; Nilsson, M.; Slim, K.; Schäfer, M.; Mariette, C.; Braga, M.; Carli, F.; Demartines, N.; Griffin, S.M.; Lassen, K.; et al. Consensus guidelines for enhanced recovery after gastrectomy. BJS 2014, 101, 1209–1229. [Google Scholar] [CrossRef]
- Osland, E.; Memon, M. Early Postoperative feeding in resectional gastrointestinal surgical cancer patients. World J. Gastrointest. Oncol. 2010, 2, 187. [Google Scholar] [CrossRef]
- Hanna, L.; Huggins, C.E.; Furness, K.; Silvers, M.A.; Savva, J.; Frawley, H.; Croagh, D.; Cashin, P.; Low, L.; Bauer, J.; et al. Effect of early and intensive nutrition care, delivered via telephone or mobile application, on quality of life in people with upper gastrointestinal cancer: Study protocol of a randomised controlled trial. BMC Cancer 2018, 18, 707. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. J. Assoc. Am. Med Coll. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int. J. Qual. Stud. Health Well-Being 2014, 9, 26152. [Google Scholar] [CrossRef] [Green Version]
- Castleberry, A.; Nolen, A. Thematic analysis of qualitative research data: Is it as easy as it sounds? Curr. Pharm. Teach. Learn. 2018, 10, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Marks, D.F.; Yardley, L. Content and Thematic Analysis in Research Methods for Clinical and Health Psychology; SAGE Publications, Ltd.: London, UK, 2004; pp. 56–68. Available online: https://methods.sagepub.com/book/research-methods-for-clinical-and-health-psychology (accessed on 9 May 2020).
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Parker, V.; Giles, M.; Boyle, B. The ABC of health care team dynamics: Understanding complex affective, behavioral, and cognitive dynamics in interprofessional teams. Health Care Manag. Rev. 2014, 39, 1–9. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, P.; Lee, S.H.; O’Sullivan, M.; Cullen, W.; Kennedy, C.; MacFarlane, A. Assessing the facilitators and barriers of interdisciplinary team working in primary care using normalisation process theory: An integrative review. PLoS ONE 2017, 12, e0177026. [Google Scholar] [CrossRef] [Green Version]
- Mulvale, G.; Embrett, M.; Razavi, S.D. ‘Gearing Up’ to improve interprofessional collaboration in primary care: A systematic review and conceptual framework. BMC Fam. Pract. 2016, 17, 83. [Google Scholar] [CrossRef] [Green Version]
- Wranik, W.D.; Price, S.; Haydt, S.M.; Edwards, J.; Hatfield, K.; Weir, J.; Doria, N. Implications of interprofessional primary care team characteristics for health services and patient health outcomes: A systematic review with narrative synthesis. Health Policy 2019, 123, 550–563. [Google Scholar] [CrossRef]
- Jehn, K.A. A multimethod examination of the benefits and detriments of intragroup conflict. Adm. Sci. Q. 1995, 40, 256–282. [Google Scholar] [CrossRef]
- Lingard, L.; Reznick, R.; DeVito, I.; Espin, S. Forming professional identities on the health care team: Discursive constructions of the ‘other’ in the operating room. Med. Educ. 2002, 36, 728–734. [Google Scholar] [CrossRef]
- Sifaki-Pistolla, D.; Melidoniotis, E.; Dey, N.; Chatzea, V.-E. How trust affects performance of interprofessional health-care teams. J. Interprof. Care 2020, 34, 218–224. [Google Scholar] [CrossRef]
- Macri, J. Australia’s Health System: Some Issues and Challenges. J. Health Med. Econ. 2016, 2. [Google Scholar] [CrossRef]
- Bagheri, A. Medical Futility: Is a Policy Needed? J. Clin. Res. Bioeth. 2014, 5. [Google Scholar] [CrossRef]
- Davidson, W.; Ash, S.; Capra, S.; Bauer, J. Weight stabilisation is associated with improved survival duration and quality of life in unresectable pancreatic cancer. Clin. Nutr. 2004, 23, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Marín Caro, M.M.; Laviano, A.; Pichard, C. Nutritional intervention and quality of life in adult oncology patients. Clin. Nutr. 2007, 26, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.J.; May, C.R. Promoting professional behaviour change in healthcare: What interventions work, and why? A theory-led overview of systematic reviews. Bmj Open 2015, 5, e008592. [Google Scholar] [CrossRef] [Green Version]
- Rogers, E.M. Diffusions of Innovation; Free Press of Glencoe: New York, NY, USA, 1962. [Google Scholar]
- Lane, H.; Sturgess, T.; Philip, K.; Markham, D.; Martin, J.; Walsh, J.; Hubbard, W.; Haines, T. What Factors Do Allied Health Take Into Account When Making Resource Allocation Decisions? Int. J. Health Policy Manag. 2018, 7, 412–420. [Google Scholar] [CrossRef] [Green Version]
- Harst, L.; Lantzsch, H.; Scheibe, M. Theories Predicting End-User Acceptance of Telemedicine Use: Systematic Review. J. Med. Internet Res. 2019, 21, e13117. [Google Scholar] [CrossRef] [Green Version]
- Awad, S.; Herrod, P.J.; Forbes, E.; Lobo, D.N. Knowledge and attitudes of surgical trainees towards nutritional support: Food for thought. Clin. Nutr. 2010, 29, 243–248. [Google Scholar] [CrossRef]
- Crowley, J.; Ball, L.; Laur, C.; Wall, C.; Arroll, B.; Poole, P.; Ray, S. Nutrition guidelines for undergraduate medical curricula: A six-country comparison. Adv. Med. Educ. Pract. 2015, 6, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deakin University School of Medicine and School of Exercise and Nutrition Sciences Faculty of Health. Extended Nutrition Competency Framework (NCF); Deakin University: Burwood, Australia, 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Question Logic |
|---|---|
| Describe to me your role in managing patients with upper GI cancer? | Elicits background information about the health professional role |
| Cancers of the upper GI tract are often associated with weight change. Tell me about your experiences as a practitioner and managing cancer treatment in patients who are experiencing weight change. | Explores the views, experiences and attitudes of health professionals managing weight change in their patients |
| Given that upper gastrointestinal cancers have very low survival rates, do you think that there is any benefit to providing nutrition interventions to these patients? | Explores the views of health professionals of the provision of nutrition interventions across the continuum of care |
| All of your patients who were diagnosed with gastric, oesophageal, or pancreatic cancers were eligible to access early and intensive nutrition support via a telephone or mobile app delivery method. Can you tell me what experience you have had with this research study? | Elicits information about health professional’s knowledge of the intervention study and what experiences they had with it directly |
| Did you experience any challenges with the study, if so, can you give some examples? | Ascertains any challenges they had with engaging with the intervention study |
| Tell me about your opinion of the two different delivery methods? | Explores the views of health professionals regarding external, centralised synchronous and asynchronous nutrition care delivery models |
| If you could design a service delivery model for your patients what would the features be? | Explores the ultimate nutrition care service delivery model |
| To access this nutrition service delivery model, describe the referral process that would work for you? | Ascertains information about the best nutrition referral method for health professionals |
| If you could have one thing at your disposal to address the nutrition concerns of your patients, what would it be? | Elicits information about the most important factor to implementing the best nutrition care model |
| Is there any final remarks or comments you would like to make? | Open commentary from health professionals |
| Demographics | ||
|---|---|---|
| Profession | Total | Percent |
| Surgeon | 5 | 38% |
| Oncologist | 1 | 9% |
| Nurse | 2 | 15% |
| Dietitians | 5 | 38% |
| Gender | ||
| Female | 9 | 69% |
| Male | 4 | 31% |
| Age | ||
| 30–40 | 3 | 23% |
| 40–50 | 6 | 46% |
| 50–60 | 4 | 31% |
| Health Service | ||
| Public | 7 | 54% |
| Private | 2 | 15% |
| Both | 4 | 31% |
| Experience (years) | ||
| 5–10 | 3 | 23% |
| 10–20 | 2 | 15% |
| 20–30 | 7 | 54% |
| 30+ | 1 | 8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furness, K.; Huggins, C.; Croagh, D.; Haines, T. Exploring the Attitudes of Health Professionals Providing Care to Patients Undergoing Treatment for Upper Gastrointestinal Cancers to Different Models of Nutrition Care Delivery: A Qualitative Investigation. Nutrients 2021, 13, 1020. https://doi.org/10.3390/nu13031020
Furness K, Huggins C, Croagh D, Haines T. Exploring the Attitudes of Health Professionals Providing Care to Patients Undergoing Treatment for Upper Gastrointestinal Cancers to Different Models of Nutrition Care Delivery: A Qualitative Investigation. Nutrients. 2021; 13(3):1020. https://doi.org/10.3390/nu13031020
Chicago/Turabian StyleFurness, Kate, Catherine Huggins, Daniel Croagh, and Terry Haines. 2021. "Exploring the Attitudes of Health Professionals Providing Care to Patients Undergoing Treatment for Upper Gastrointestinal Cancers to Different Models of Nutrition Care Delivery: A Qualitative Investigation" Nutrients 13, no. 3: 1020. https://doi.org/10.3390/nu13031020
APA StyleFurness, K., Huggins, C., Croagh, D., & Haines, T. (2021). Exploring the Attitudes of Health Professionals Providing Care to Patients Undergoing Treatment for Upper Gastrointestinal Cancers to Different Models of Nutrition Care Delivery: A Qualitative Investigation. Nutrients, 13(3), 1020. https://doi.org/10.3390/nu13031020