
Type 2 Diabetes Prevention Focused on Normalization of Glycemia: A Two-Year Pilot Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Intervention
2.3. Assessments
2.4. Statistical Methods
3. Results
3.1. Participant Characteristics, Retention, and Adherence
3.2. Incidence of Normoglycemia and Type 2 Diabetes
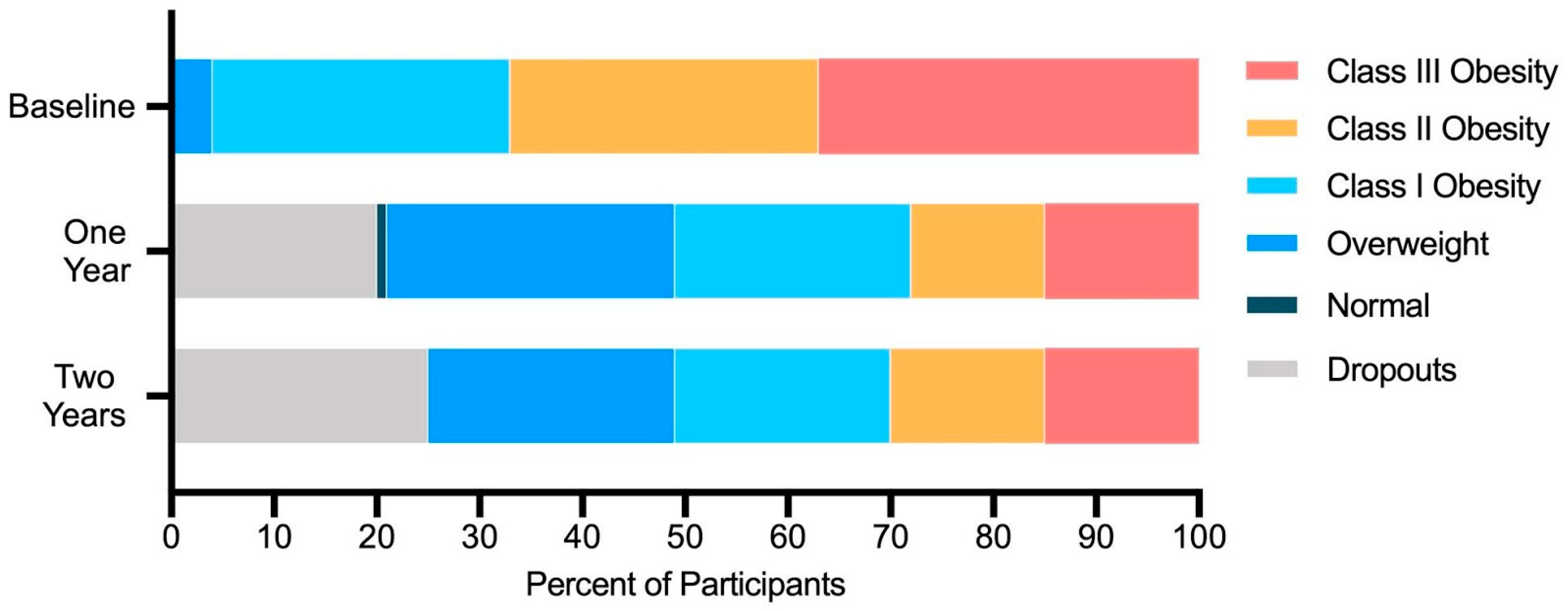
3.3. Change in Metabolic Condition Status
3.4. Change in Clinical Markers Associated with Metabolic Conditions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report 2020: Estimates of Diabetes and Its Burden in the United States; U.S. Department of Health and Human Services: Washington, DC, USA, 2020.
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A High-Risk State for Diabetes Development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- DeJesus, R.S.; Breitkopf, C.R.; Rutten, L.J.; Jacobson, D.J.; Wilson, P.M.; Sauver, J.S. Incidence Rate of Prediabetes Progression to Diabetes: Modeling an Optimum Target Group for Intervention. Popul. Health Manag. 2017, 20, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, C.; Okoloise, M.; Williams, K.; Stern, M.P.; Haffner, S.M. The Metabolic Syndrome as Predictor of Type 2 Diabetes. Diabetes Care 2003, 26, 3153–3159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perreault, L.; Pan, Q.; Aroda, V.R.; Barrett-Connor, E.; Dabelea, D.; Dagogo-Jack, S.; Hamman, R.F.; Kahn, S.E.; Mather, K.J.; Knowler, W.C.; et al. Exploring Residual Risk for Diabetes and Microvascular Disease in the Diabetes Prevention Program Outcomes Study (DPPOS). Diabetic Med. 2017, 34, 1747–1755. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Group, D. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Siu, A.L.; United States Preventive Services Task Force. Screening for Abnormal Blood Glucose and Type 2 Diabetes Mellitus: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2015, 163, 861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ackermann, R.T.; Finch, E.A.; Brizendine, E.; Zhou, H.; Marrero, D.G. Translating the Diabetes Prevention Program into the Community The DEPLOY Pilot Study. Am. J. Prev. Med. 2008, 35, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Department of Health and Human Services; Centers for Medicare and Medicaid Services. Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016. Fed. Regist. 2016, 220, 70886–71386. [Google Scholar]
- Centers for Disease Control and Prevention Diabetes Prevention Recognition Program. Available online: https://www.cdc.gov/diabetes/prevention/pdf/dprp-standards.pdf (accessed on 15 November 2020).
- Cannon, M.J.; Masalovich, S.; Ng, B.P.; Soler, R.E.; Jabrah, R.; Ely, E.K.; Smith, B.D. Retention Among Participants in the National Diabetes Prevention Program Lifestyle Change Program, 2012–2017. Diabetes Care 2020, 43, 2042–2049. [Google Scholar] [CrossRef]
- Ritchie, N.D. Solving the Puzzle to Lasting Impact of the National Diabetes Prevention Program. Diabetes Care 2020, 43, 1994–1996. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S1–S212. [Google Scholar] [CrossRef] [Green Version]
- McKenzie, A.L.; Hallberg, S.J.; Creighton, B.C.; Volk, B.M.; Link, T.M.; Abner, M.K.; Glon, R.M.; McCarter, J.P.; Volek, J.S.; Phinney, S.D. A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes. JMIR Diabetes 2017, 2, e5. [Google Scholar] [CrossRef]
- Hallberg, S.J.; McKenzie, A.L.; Williams, P.T.; Bhanpuri, N.H.; Peters, A.L.; Campbell, W.W.; Hazbun, T.L.; Volk, B.M.; McCarter, J.P.; Phinney, S.D.; et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Ther. 2018, 9, 583–612. [Google Scholar] [CrossRef] [Green Version]
- Athinarayanan, S.J.; Adams, R.N.; Hallberg, S.J.; McKenzie, A.L.; Bhanpuri, N.H.; Campbell, W.W.; Volek, J.S.; Phinney, S.D.; McCarter, J.P. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-Randomized Clinical Trial. Front. Endocrinol. 2019, 10, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, G.; Zimmet, P.; Shaw, J.; Grundy, S.M. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. Bruss. Int. Diabetes Fed. 2006, 23, 469–480. [Google Scholar]
- Alberti, K.G.M.; Zimmet, P.; Shaw, J. The Metabolic Syndrome—A New Worldwide Definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstråle, M.; Groop, L.; et al. Prediction of Non-Alcoholic Fatty Liver Disease and Liver Fat Using Metabolic and Genetic Factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef]
- Kline, R. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Rich, J.T.; Neely, J.G.; Paniello, R.C.; Voelker, C.C.J.; Nussenbaum, B.; Wang, E.W. A Practical Guide to Understanding Kaplan-Meier Curves. Otolaryngol.—Head Neck Surg. 2010, 143, 331–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, J.W.; Olchowski, A.E.; Gilreath, T.D. How Many Imputations Are Really Needed? Some Practical Clarifications of Multiple Imputation Theory. Prev. Sci. 2007, 8, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Ely, E.K.; Gruss, S.M.; Luman, E.T.; Gregg, E.W.; Ali, M.K.; Nhim, K.; Rolka, D.B.; Albright, A.L. A National Effort to Prevent Type 2 Diabetes: Participant-Level Evaluation of CDC’s National Diabetes Prevention Program. Diabetes Care 2017, 40, dc162099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katula, J.A.; Dressler, E.V.; Kittle, C.; Almeida, F.A.; Wilson, K.E.; Michaud, T.L.; Porter, G.C.; Brito, F.A.; Jasik, C.B.; Sweet, C.M.C.; et al. Effects of a Digital Diabetes Prevention Program on HbA1c and Body Weight in Prediabetes. Available online: https://tos.planion.com/Web.User/AbstractDet?ACCOUNT=TOS&ABSID=24380&CONF=OW2020&ssoOverride=OFF&CKEY= (accessed on 6 November 2020).
- Alexander, E.; Tseng, E.; Durkin, N.; Jerome, G.J.; Dalcin, A.; Appel, L.J.; Clark, J.M.; Gudzune, K.A. Long-term Retention in an Employer-based, Commercial Weight-loss Programme. Clin. Obes. 2019, 9, e12284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apolzan, J.W.; Venditti, E.M.; Edelstein, S.L.; Knowler, W.C.; Dabelea, D.; Boyko, E.J.; Pi-Sunyer, X.; Kalyani, R.R.; Franks, P.W.; Srikanthan, P.; et al. Long-Term Weight Loss With Metformin or Lifestyle Intervention in the Diabetes Prevention Program Outcomes Study. Ann. Intern. Med. 2019, 170, 682. [Google Scholar] [CrossRef] [PubMed]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of Weight Loss With Lifestyle Intervention on Risk of Diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [Green Version]
- Perreault, L.; Pan, Q.; Mather, K.J.; Watson, K.E.; Hamman, R.F.; Kahn, S.E.; Diabetes Prevention Program Research Group. Effect of Regression from Prediabetes to Normal Glucose Regulation on Long-Term Reduction in Diabetes Risk: Results from the Diabetes Prevention Program Outcomes Study. Lancet 2012, 379, 2243–2251. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Wu, S.; Song, Q.; Wang, X. Reversion from Pre–Diabetes Mellitus to Normoglycemia and Risk of Cardiovascular Disease and All-Cause Mortality in a Chinese Population: A Prospective Cohort Study. J. Am. Heart Assoc. 2021, e019045. [Google Scholar] [CrossRef]
- Perreault, L.; Pan, Q.; Schroeder, E.B.; Kalyani, R.R.; Bray, G.A.; Dagogo-Jack, S.; White, N.H.; Goldberg, R.B.; Kahn, S.E.; Knowler, W.C.; et al. Regression From Prediabetes to Normal Glucose Regulation and Prevalence of Microvascular Disease in the Diabetes Prevention Program Outcomes Study (DPPOS). Diabetes Care 2019, 42, 1809–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diabetes Prevention Program Research Group. Long-Term Effects of Lifestyle Intervention or Metformin on Diabetes Development and Microvascular Complications over 15-Year Follow-up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015, 3, 866–875. [Google Scholar] [CrossRef] [Green Version]
- Perreault, L.; Kahn, S.E.; Christophi, C.A.; Knowler, W.C.; Hamman, R.F. Regression From Pre-Diabetes to Normal Glucose Regulation in the Diabetes Prevention Program. Diabetes Care 2009, 32, 1583–1588. [Google Scholar] [CrossRef] [Green Version]
- Pories, W.J.; Swanson, M.S.; MacDonald, K.G.; Long, S.B.; Morris, P.G.; Brown, B.M.; Barakat, H.A.; deRamon, R.A.; Israel, G.; Dolezal, J.M.; et al. Who Would Have Thought It? An Operation Proves to Be the Most Effective Therapy for Adult-Onset Diabetes Mellitus. Ann. Surg. 1995, 222, 339–352. [Google Scholar] [CrossRef]
- Hyde, P.N.; Sapper, T.N.; Crabtree, C.D.; LaFountain, R.A.; Bowling, M.L.; Buga, A.; Fell, B.; McSwiney, F.T.; Dickerson, R.M.; Miller, V.J.; et al. Dietary Carbohydrate Restriction Improves Metabolic Syndrome Independent of Weight Loss. JCI Insight 2019, 4, e128308. [Google Scholar] [CrossRef] [Green Version]
- Orchard, T.J.; Temprosa, M.; Goldberg, R.; Haffner, S.; Ratner, R.; Marcovina, S.; Fowler, S.; Diabetes Prevention Program Research Group. The Effect of Metformin and Intensive Lifestyle Intervention on the Metabolic Syndrome: The Diabetes Prevention Program Randomized Trial. Ann. Intern. Med. 2005, 8, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Mardinoglu, A.; Wu, H.; Bjornson, E.; Zhang, C.; Hakkarainen, A.; Räsänen, S.M.; Lee, S.; Mancina, R.M.; Bergentall, M.; Pietiläinen, K.H.; et al. An Integrated Understanding of the Rapid Metabolic Benefits of a Carbohydrate-Restricted Diet on Hepatic Steatosis in Humans. Cell Metab. 2018, 27, 559–571.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Metabolic Condition | Baseline | 1 Year | 2 Years | |||||
|---|---|---|---|---|---|---|---|---|
| n | Mean ± SE | n | Mean ± SE | p | n | Mean ± SE | p | |
| Prediabetes (%) | 96 | 100.0 ± 0.0 | 70 | 54.0 ± 6.0 | <0.001 | 63 | 67.0 ± 5.9 | <0.001 |
| Normoglycemia (%) | 96 | 0.0 ± 0.0 | 70 | 46.0 ± 6.0 | <0.001 | 63 | 33.0 ± 5.9 | <0.001 |
| Type 2 Diabetes (%) | 96 | 0.0 ± 0.0 | 70 | 4.0 ± 2.7 | 0.04 | 63 | 5.0 ± 3.1 | 0.02 |
| Metabolic Syndrome (%) | 94 | 94.0 ± 2.5 | 65 | 30.0 ± 5.7 | <0.001 | 47 | 49.0 ± 7.1 | <0.001 |
| Obesity ≥ Class II (%) | 96 | 67.0 ± 4.8 | 77 | 38.0 ± 5.5 | <0.001 | 72 | 43.0 ± 5.6 | <0.001 |
| Suspected Steatosis (%) | 89 | 88.0 ± 3.5 | 58 | 41.0 ± 6.1 | <0.001 | 42 | 48.0 ± 6.5 | <0.001 |
| Baseline | 1 year | 2 years | ||||||
|---|---|---|---|---|---|---|---|---|
| n | EMM ± SE | n | EMM ± SE | p | n | EMM ± SE | p | |
| HbA1c (%) | 96 | 5.95 ± 0.02 | 70 | 5.63 ± 0.03 | <0.001 | 64 | 5.73 ± 0.04 | <0.001 |
| HbA1c (mmol/mol) | 96 | 41.5 ± 0.2 | 70 | 38.3 ± 0.3 | <0.001 | 64 | 39.3 ± 0.4 | <0.001 |
| Fasting Glucose (mmol/L) | 95 | 6.11 ± 0.08 | 69 | 5.61 ± 0.08 | <0.001 | 63 | 5.64 ± 0.08 | <0.001 |
| Fasting Insulin (pmol/L) | 90 | 164.80 ± 10.21 | 67 | 94.73 ± 6.53 | <0.001 | 58 | 104.59 ± 7.22 | <0.001 |
| SBP (mmHg) | 95 | 129.9 ± 1.4 | 62 | 123.1 ± 1.5 | <0.001 | 48 | 127.3 ± 1.8 | 0.18 |
| DBP (mmHg) | 95 | 82.5 ± 0.8 | 62 | 79.2 ± 1.0 | 0.01 | 48 | 80.5 ± 1.1 | 0.11 |
| Weight (kg) | 96 | 109.6 ± 2.2 | 77 | 95.7 ± 1.9 | <0.001 | 72 | 97.2 ± 1.9 | <0.001 |
| BMI (kg/m2) | 96 | 39.08 ± 0.72 | 77 | 34.11 ± 0.63 | <0.001 | 72 | 34.62 ± 0.62 | <0.001 |
| Waist Circumference (cm) | 74 | 118.9 ± 1.6 | 52 | 107.8 ± 1.7 | <0.001 | 42 | 110.9 ± 2.7 | 0.002 |
| HDL-cholesterol (mmol/L) | 90 | 1.28 ± 0.03 | 67 | 1.45 ± 0.04 | <0.001 | 58 | 1.46 ± 0.05 | <0.001 |
| Triglycerides (mmol/L) | 90 | 1.81 ± 0.09 | 67 | 1.38 ± 0.09 | <0.001 | 58 | 1.28 ± 0.08 | <0.001 |
| ALT (µkat/L) † | 95 | 0.46 ± 0.02 | 69 | 0.37 ± 0.02 | <0.001 | 63 | 0.37 ± 0.02 | <0.001 |
| AST (µkat/L) † | 95 | 0.37 ± 0.02 | 69 | 0.34 ± 0.02 | 0.03 | 63 | 0.33 ± 0.01 | 0.04 |
| NAFLD-Liver Fat Score | 89 | 1.84 ± 0.24 | 58 | −0.78 ± 0.20 | <0.001 | 42 | −0.35 ± 0.24 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKenzie, A.L.; Athinarayanan, S.J.; McCue, J.J.; Adams, R.N.; Keyes, M.; McCarter, J.P.; Volek, J.S.; Phinney, S.D.; Hallberg, S.J. Type 2 Diabetes Prevention Focused on Normalization of Glycemia: A Two-Year Pilot Study. Nutrients 2021, 13, 749. https://doi.org/10.3390/nu13030749
McKenzie AL, Athinarayanan SJ, McCue JJ, Adams RN, Keyes M, McCarter JP, Volek JS, Phinney SD, Hallberg SJ. Type 2 Diabetes Prevention Focused on Normalization of Glycemia: A Two-Year Pilot Study. Nutrients. 2021; 13(3):749. https://doi.org/10.3390/nu13030749
Chicago/Turabian StyleMcKenzie, Amy L, Shaminie J Athinarayanan, Jackson J McCue, Rebecca N Adams, Monica Keyes, James P McCarter, Jeff S Volek, Stephen D Phinney, and Sarah J Hallberg. 2021. "Type 2 Diabetes Prevention Focused on Normalization of Glycemia: A Two-Year Pilot Study" Nutrients 13, no. 3: 749. https://doi.org/10.3390/nu13030749
APA StyleMcKenzie, A. L., Athinarayanan, S. J., McCue, J. J., Adams, R. N., Keyes, M., McCarter, J. P., Volek, J. S., Phinney, S. D., & Hallberg, S. J. (2021). Type 2 Diabetes Prevention Focused on Normalization of Glycemia: A Two-Year Pilot Study. Nutrients, 13(3), 749. https://doi.org/10.3390/nu13030749