
High-Density Lipoproteins and Mediterranean Diet: A Systematic Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Searching Strategy
2.2. Selection Criteria
2.3. Data Extraction and Reliability
3. Results
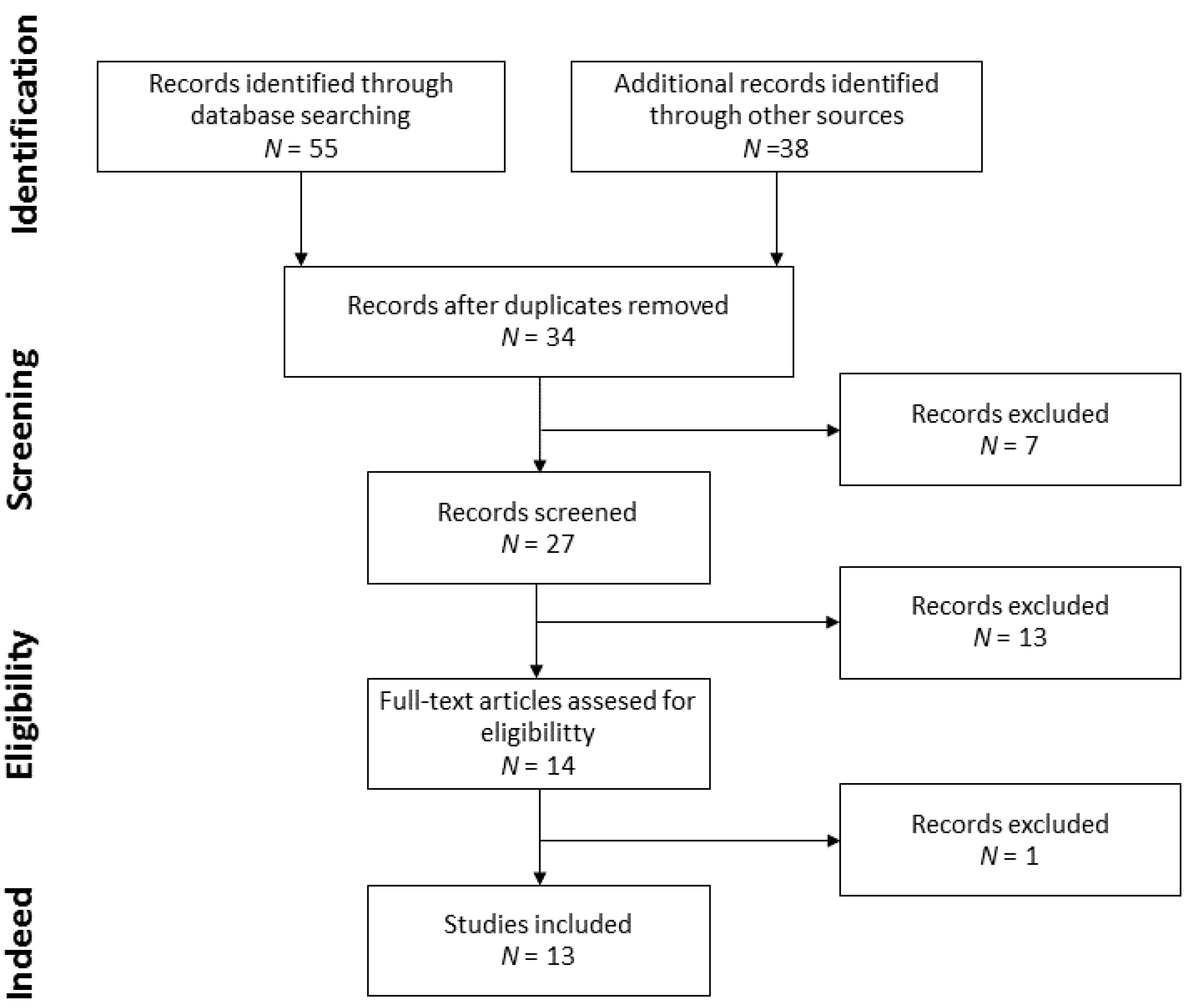
3.1. Search and Selection of Studies
3.2. Comparison between Studies
3.3. HDL Functionality Modulation
3.4. HDL Oxidation
3.5. HDL Monolayer Fluidity
3.6. HDL Composition
3.7. HDL Size
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kontush, A.; Lindahl, M.; Lhomme, M.; Calabresi, M.; Chapman, M.J.; Davidson, W. Structure of HDL: Particle subclases and molecular components. Handb. Exp. Pharmacol. 2015, 224, 3–51. [Google Scholar] [CrossRef] [Green Version]
- March, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascularrisk. Eur. Heart J. 2020, 41, 111–181. [Google Scholar] [CrossRef]
- Ronsein, G.E.; Heinecke, J.W. Time to ditch HDL-C as a measure of HDL function. Curr. Opin. Lipidol. 2017, 28, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.B. Dyslipidaemia: Effect of hypercholesterolaemia on HDL particle remodelling. Nat. Rev. Cardiol. 2017, 14, 505. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.Y.; Hafiane, A.; Schwertani, A.; Genest, J. High-Density Lipoproteins: Biology, Epidemiology, and Clinical Management. Can. J. Cardiol. 2017, 33, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Varela, L.M.; Mesenguer, E.; Apergue, B.; Couret, D.; Amarenco, P.; Meilhac, O. Changes in High-density Lipoproteins Related to Outcomes in Patients with Acute Stroke. J. Clin. Med. 2020, 9, 2269. [Google Scholar] [CrossRef] [PubMed]
- Sattler, K.; Lehmann, L.; Graler, M.; Brocker-Preuss, M.; Erbel, R.; Heusch, G.; Levkau, B. HDL-bound sphingosine 1-phosphate (S1P) predicts the severity of coronary artery atherosclerosis. Cell Physiol. Biochem. 2014, 34, 172–184. [Google Scholar] [CrossRef]
- Soria-Florido, M.T.; Castañer, O.; Lassale, C.; Estruch, R.; Salas-Salvado, J.; Martinez-Gonzalez, M.A.; Corella, D.; Ros, E.; Arós, F.; Elosua, R.; et al. Dysfunctional High-Density lipoproteins Are Associated With a Greater Incidence of Acute Coronary Syndrome in a Population at High Cardiovascular Risk. A Nested Case-Control Study. Circulation 2020, 141, 444–453. [Google Scholar] [CrossRef]
- Prats-Uribe, A.; Sayols-Baixeras, S.; Fernandez-Sanles, A.; Subirana, I.; Carreras-Torres, R.; Vilahur, G.; Civeira, F.; Marrugat, J.; Fitó, M.; Hernáez, Á.; et al. High-density lipoprotein characteristics and coronary artery disease: A Mendelian randomization study. Metabolism 2020, 112, 154351. [Google Scholar] [CrossRef]
- Hisham, M.D.B.; Aziz, Z.; Huin, W.K.; Teoh, C.H.; Jamil, A.H.A. The effects of palm oil on serum lipid profiles: A systematic review and meta-analysis. Asia Pac. J. Clin. Nutr. 2020, 28, 523–536. [Google Scholar] [CrossRef]
- Di Renzo, L.; Cinelli, G.; Dri, M.; Gualtieri, P.; Attina, A.; Leggeri, C.; Cenname, G.; Esposito, E.; Pujia, A.; Chiricolo, G.; et al. Mediterranean personalized diet combined with physical activity therapy for the prevention of cardiovascular diseases in Italian women. Nutrients 2020, 12, 3456. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses. The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernaez, A.; Sanllorente, A.; Castañer, O.; Martinez-Gonzalez, M.; Ros, E.; Pinto, X.; Estruch, R.; Salas-Salvado, J.; Corella, D.; Alonso-Gomez, A.M.; et al. Increased Consumption of Virgin Olive Oil, Nuts, Legumes, Whole Grains, and Fish Promotes HDL Functions in Humans. Mol. Nutr. Food Res. 2019, 63, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, A.; Castañer, O.; Elosua, R.; Pinto, X.; Estruch, R.; Salas-Salvado, J.; Corella, D.; Aros, F.; Serra-Majem, L.; Fiol, M.; et al. Mediterranean Diet Improves High-Density Lipoprotein Function in High-Cardiovascular-Risk Individuals. Circulation 2017, 135, 633–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernaez, A.; Fernandez-Castillejo, A.; Farras, M.; Catalan, U.; Subirana, I.; Montes, R.; Sola, R.; Muñoz-Aguayo, D.; Gelabert-Gorges, A.; Diaz-Gil, O.; et al. Olive oil polyphenols enhance high-density lipoprotein function in humans: A randomized controlled trial. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2115–2119. [Google Scholar] [CrossRef] [Green Version]
- McEneny, J.; Wade, L.; Young, I.S.; Masson, L.; Duthie, G.; McGinty, A.; Duthie, G.; McGinty, A.; McMaster, C.; Thies, F. Lycopene intervention reduces inflammation and improves HDL functionality in moderately overweight middle-aged individuals. J. Nutr. Biochem. 2013, 24, 163–168. [Google Scholar] [CrossRef]
- Zhu, C.; Sawrey-Kubicek, L.; Beals, E.; Hughes, R.L.; Rhodes, C.H.; Sacchi, R.; Zivkovic, A.M. The HDL lipidome is widely remodelled by fast food versus Mediterranean diet in 4 days. Metabolomics 2019, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helal, O.; Berrougui, H.; Loued, A.; Khalil, A. Extra-virgin olive oil consumption improves the capacity of HDL to mediate cholesterol efflux and increases ABCA1 and ABCG1 expression in human macrophages. Br. J. Nutr. 2013, 109, 1844–1855. [Google Scholar] [CrossRef] [Green Version]
- Sola, R.; la Ville, A.E.; Richard, J.L.; Motta, C.; Bargallo, M.T.; Girona, J.; Masana, L.; Bernard, J. Oleic acid rich diet protects against the oxidative modification of high density lipoprotein. Free Radic. Biol. Med. 1997, 22, 1037–1045. [Google Scholar] [CrossRef]
- Tanaka, N.; Ishida, T.; Nagao, M.; Mori, T.; Monguchi, T.; Sasaki, M.; Mori, K.; Kondo, K.; Nakajima, H.; Honjo, T.; et al. Administration of high dose eicosapentaenoic acid enhances anti-inflammatory properties of high-density lipoprotein in Japanese patients with dyslipidemia. Atherosclerosis 2014, 237, 577–583. [Google Scholar] [CrossRef]
- Sola, R.; Fito, M.; Estruch, R.; Salas-Salvado, J.; Corella, D.; de la Torre, R.; Muñoz, M.A.; Lopez-Sabater, M.C.; Martinez-Gonzalez, M.A.; Aros, F.; et al. Effect of a traditional Mediterranean diet on apolipoproteins B, A-I, and their ratio: A randomized controlled trial. Atherosclerosis 2011, 218, 174–180. [Google Scholar] [CrossRef]
- Farras, M.; Castañer, O.; Martin-Pelaez, S.; Hernaez, A.; Schroder, H.; Subirana, I.; Muñoz-Aguayo, D.; Gaixas, S.; de la Torre, R.; Farre, M.; et al. Complementary phenol-enriched olive oil improves HDL charasteristic in hypercholesterolemic subjects. A randomized, double-blind, crossover, controlled trial. The VOHF Study. Mol. Nutr. Food Res. 2015, 59, 1758–1770. [Google Scholar] [CrossRef]
- Fernandez-Castillejo, S.; Rubio, L.; Hernaez, A.; Catalan, U.; Pedret, A.; Valls, R.M.; Mosele, J.I.; Covas, M.I.; Remaley, A.T.; Castañer, O.; et al. Determinants of HDL Cholesterol Efflux Capacity after Virgin Olive Oil Ingestion: Interrelationships with Fluidity of HDL Monolayer. Mol. Nutr. Food Res. 2017, 61, 1–21. [Google Scholar] [CrossRef]
- Farras, M.; Fernandez-Castillejo, S.; Rubio, L.; Arranz, S.; Catalan, U.; Subirana, I.; Romero, M.P.; Castañer, O.; Pedret, A.; Blanchart, A.; et al. Phenol-enriched olive oils improve HDL antioxidant content in hypercholesterolemic subjects. A randomized double-blind, cross-over, controlled trial. J. Nutr. Biochem. 2018, 51, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Pedret, A.; Catalan, U.; Fernandez-Castillejo, S.; Farras, M.; Valls, R.M.; Rubio, L.; Canela, N.; de la Torre, R.; Covas, M.I.; Fito, M.; et al. Impact of virgin olive oil and phenol-enriched virgin olive oils on the HDL proteome in hypercholesterolemic subjects: A double blind, randomized, controlled, cross-over clinical trial (VOHF study). PLoS ONE 2015, 10, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimmino, G.; Ciccarelli, G.; Morello, A.N.; Ciccarelli, M.; Golino, P. High Density Lipoprotein Cholesterol Increasing Therapy: The Unmet Cardiovascular Need. Transl. Med. UniSa 2015, 12, 29–40. [Google Scholar] [PubMed]
- Morgantini, C.; Trifiro, S.; Trico, D.; Meriwether, D.; Baldi, S.; Mengozzi, A.; Reddy, S.T.; Natali, A. A short-term increase in dietary cholesterol and fat intake affects high-density lipoprotein composition in healthy subjects. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Andraski, A.B.; Singh, S.A.; Lee, H.L.; Higashi, H.; Smith, N.; Zhang, B.; Aikawa, M.; Sacks, F.M. Effects of Replacing Dietary Monounsaturated Fat with Carbohydrate on HDL (High-Density Lipoprotein) Protein Metabolism and Proteome Composition in Humans. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 2411–2430. [Google Scholar] [CrossRef]
- Kashyap, S.R.; Osme, A.; Ilchenko, S.; Golizeh, M.; Lee, K.; Wang, S.; BENA, J.; Previs, S.F.; Smith, J.D.; Kasumov, T. Glycation reduces the stability of apoai and increases HDL dysfunction in diet-controlled type 2 diabetes. J. Clin. Endocrinol Metab. 2018, 103, 388–396. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Criteria | Definition |
|---|---|
| Population | Human studies: adult men and women, including healthy participants, obese and dyslipidemic patients and not including individuals with genetic diseases |
| Interventions | MD or MD isolated food interventions |
| Comparator | Comparison against baseline or comparison against different interventions |
| Outcomes | HDL composition changes HDL functionality changes HDL components modifications |
| Study design | Human pilot studies and controlled trials |
| Authors and Publication Year | Study Characteristic | Intervention | ||||
|---|---|---|---|---|---|---|
| Sample | Age | Country | Duration | Design | ||
| A. Hernaez et al., 2019 [13] | 196 individuals from the PREDIMED study | 55–80 | Spain | 1 year | Randomized controlled trial | Traditional MD—VOO Traditional MD–nuts Traditional MD—fish Traditional MD—legumes Traditional MD—whole grains |
| A. Hernaez et al., 2017 [14] | 296 individuals from the PREDIMED study | 55–80 | Spain | 1 year | Randomized controlled trial | Traditional MD—nuts Traditional MD—VOO Low-fat diet |
| A. Hernaez et al., 2014 [15] | 47 individuals from the EUROLIVE study | 20–60 | Germany Spain Finland | 3 weeks | Randomized controlled trial | HPCOO LPCOO |
| N. Tanaka et al., 2014 [20] | 28 dyslipidemic individuals | 50–85 | Japan | 4 weeks | Randomized trial | Low-fat diet enriched with EPA |
| R. Sola et al., 2011 [21] | 772 individuals from the PREDIMED study | 55–80 | Spain | 3 months | Randomized controlled trial | Traditional MD—VOO Traditional MD—nuts Low-fat diet |
| J. McEneny et al., 2013 [16] | 54 overweight individuals | 45–55 | UK | 12 weeks | Randomized controlled trial | Lycopene rich diet Lycopene supplemented diet |
| C. Zhu et al., 2019 [17] | 10 healthy individuals | 18–25 | California | 4 days | Randomized crossover trial | Fast food diet MD |
| O. Helal et al., 2013 [18] | 26 healthy individuals | 18–75 | Canada | 12 weeks | Randomized trial | Extra VOO |
| M. Farras et al., 2015 [22] S. Fernandez-Castillejo et al., 2017 [23] M. Farras et al., 2018 [24] A. Pedret et al., 2015 [25] | 33 individuals of the VOHF study | 35–80 | Spain | 3 weeks | Randomized controlled trial | VOO FVOO FVOOT |
| R. Sola et al., 1997 [19] | 22 healthy individuals | 45–55 | 8 weeks | Randomized crossover trial | MD rich in oleic MD rich in linoleic | |
| Author(s) and Publication Year | Measurement | ||||
|---|---|---|---|---|---|
| CEC | CETP | PON1 | LCAT | ||
| A. Hernaez et al., 2019 [13] | Traditional MD—VOO | Increase | NS | NS | NM |
| Traditional MD—nuts | NS | NS | Increase | ||
| Traditional MD—legumes | NS | Decrease | Increase | ||
| Traditional MD—whole-grains | Increase | NS | NS | ||
| Traditional—fish | Decrease | Decrease | Increase | ||
| A. Hernaez et al., 2017 [14] | Traditional MD—VOO | Increase | Decrease | NS a | NM |
| Traditional MD—nuts | Increase | NS | NS | ||
| A. Hernaez et al., 2014 [15] | LPCOO | NS | NS | NM | NS |
| HPCOO | NS b | NS | NS | ||
| N. Tanaka et al., 2014 [20] | Low fat diet—EPA | Increase | NM | Increase | NM |
| R. Sola et al., 2011 [21] | NM | ||||
| J. McEneny et al., 2013 [16] | Lycopene rich diet | NM | NS | Increase | NS |
| Lycopene supplemented diet | NS | Increase | Increase | ||
| C. Zhu et al., 2019 [17] | NM | ||||
| O. Helal et al., 2013 [18] | Extra VOO | Increase | NM | NM | NM |
| M. Farras et al., 2015 [22] S. Fernandez-Castillejo et al., 2017 [23] M. Farras et al., 2018 [24] A. Pedret et al., 2015 [25] | VOO | NS | NM | NS | NS |
| FVOO | NS | NS | NS | ||
| FVOOT | Increase | Increase | NS c | ||
| R. Sola et al., 1997 [19] | Oleic acid vs. linoleic acid rich MD | NS | NM | NM | NM |
| Author(s) and Publication Year | HDL Oxidation Rate Variation | |
|---|---|---|
| A. Hernaez et al., 2017 [14] | Traditional MD—VOO | Decreased |
| Traditional MD—nuts | NS | |
| M. Farras et al., 2015 [22] S. Fernandez-Castillejo et al., 2017 [23] M. Farras et al., 2018 [24] A. Pedret et al., 2015 [25] | VOO | NS |
| FVOO | NS | |
| FVOOT | NS | |
| R. Sola et al., 1997 [19] | Oleic acid vs. linoleic acid | Decreased in oleic acid |
| Author(s) and Publication Year | HDL Monolayer Fluidity Variation | |
|---|---|---|
| A. Hernaez et al., 2014 [15] | LPCOO | NS |
| HPCOO | Increased | |
| O. Helal et al. 2013 [18] | Extra VOO | Increased |
| M. Farras et al., 2015 [22] S. Fernandez-Castillejo et al., 2017 [23] M. Farras et al., 2018 [24] A. Pedret et al., 2015 [25] | VOO + FVOO + FVOOT | NS |
| R. Sola et al., 1997 [19] | Oleic acid vs. linoleic acid | NS |
| Author(S) And Publication Year | HDL Size Modifications | |
|---|---|---|
| A. Hernaez et al., 2017 [14] | Traditional MD—VOO | Increased levels of large HDLs |
| Traditional MD—nuts | Increased levels of large HDLs | |
| A. Hernaez et al., 2014 [15] | LPCOO | NS |
| HPCOO a | Increased levels of large HDLs Decreased levels of small HDLs | |
| O. Helal et al. 2013 [18] | Extra VOO | NS |
| M. Farras et al., 2015 [22] S. Fernandez-Castillejo et al., 2017 [23] M. Farras et al., 2018 [24] A. Pedret et al., 2015 [25] | VOO | NS |
| FVOO | Increased levels of small HDLs | |
| FVOOT b | Decreased levels of large HDLs | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grao-Cruces, E.; Varela, L.M.; Martin, M.E.; Bermudez, B.; Montserrat-de la Paz, S. High-Density Lipoproteins and Mediterranean Diet: A Systematic Review. Nutrients 2021, 13, 955. https://doi.org/10.3390/nu13030955
Grao-Cruces E, Varela LM, Martin ME, Bermudez B, Montserrat-de la Paz S. High-Density Lipoproteins and Mediterranean Diet: A Systematic Review. Nutrients. 2021; 13(3):955. https://doi.org/10.3390/nu13030955
Chicago/Turabian StyleGrao-Cruces, Elena, Lourdes M. Varela, Maria E. Martin, Beatriz Bermudez, and Sergio Montserrat-de la Paz. 2021. "High-Density Lipoproteins and Mediterranean Diet: A Systematic Review" Nutrients 13, no. 3: 955. https://doi.org/10.3390/nu13030955
APA StyleGrao-Cruces, E., Varela, L. M., Martin, M. E., Bermudez, B., & Montserrat-de la Paz, S. (2021). High-Density Lipoproteins and Mediterranean Diet: A Systematic Review. Nutrients, 13(3), 955. https://doi.org/10.3390/nu13030955