1. Introduction
Oral frailty (OF) has been defined as the accumulation of a slightly poor status in oral conditions and function that is considered a strong prediction of physical frailty [
1]. Tanaka et al. [
1] reported that OF was significantly associated with 2.4-, 2.2-, 2.3-, and 2.2-fold increased risk of physical frailty, sarcopenia, disability, and mortality, respectively. A previous study [
2] demonstrated that the risk of frailty was associated with lower occlusal force, masseter muscle thickness, and oral diadochokinetic rate. There have been several reports on the association between systemic frailty and mineral intake [
3,
4,
5]. A review by Morante et al. [
3] reported that dietary factors associated with frailty were calorie, protein, vitamin D, and calcium intake. Moreover, a cohort study [
4] demonstrated that low sodium intake (<2504 mg) was associated with frailty in the elderly. Furthermore, a cross-sectional study among middle- and older-aged groups suggested that dietary magnesium intake was also associated with the risk of frailty. However, few studies have evaluated the relationship between OF and mineral intake. A cross-sectional study that investigated the relationship between oral function and nutrient intake found that there was no relationship between oral health behavior (including twice a day tooth brushing or regular attendance of dental clinic) and macro- or micromineral intake [
6]. However, the study did not examine systemic factors such as osteoporosis. Due to the importance of systemic factors in bone mineral density, it is necessary to evaluate its influence in the relationship between OF and mineral intake.
With regard to the relationship between bone mineral density and oral cavity, it has been reported that there is a relationship between decreased bone mineral density and the progression of periodontal disease, especially alveolar bone resorption in postmenopausal women [
7,
8,
9]. Grocholewicza and Bohatyrewicz [
7] reported a negative correlation between the lumbar bone mineral density and the periodontal disease index and between the radius bone mineral density and the papillary bleeding index. Inagaki et al. [
9] also demonstrated that mineral bone density loss of metacarpal was associated with periodontitis and tooth loss in Japanese women. Therefore, osteoporosis has been considered to be a risk factor for periodontal disease. A systematic review by Gerritsen et al. [
10] has shown that tooth loss is associated with impairment of oral health-related quality of life. Although it has been reported that systemic frailty is associated with reduced bone mineral density [
11], it remains unclear whether OF is directly associated with these reductions.
On the basis of the association between OF, mineral intake, and bone mineral density, it is necessary to examine the interactions between these factors. Therefore, this study aimed to investigate the relationship between mineral intake and bone mineral density in middle-aged and older people with oral dysfunction, including pre-OF.
2. Materials and Methods
2.1. Study Design and Site
This was a cross-sectional study conducted among residents of Shika Town, Ishikawa Prefecture, Japan, termed the Shika study. As of November 2017, there were 21,007 residents in Shika Town, and 13,713 were older than 40 years [
12]. The Shika study epidemiologically investigated the causes of lifestyle-related diseases through interviews, self-administered questionnaires, and comprehensive medical examinations [
13,
14,
15].
2.2. Participants
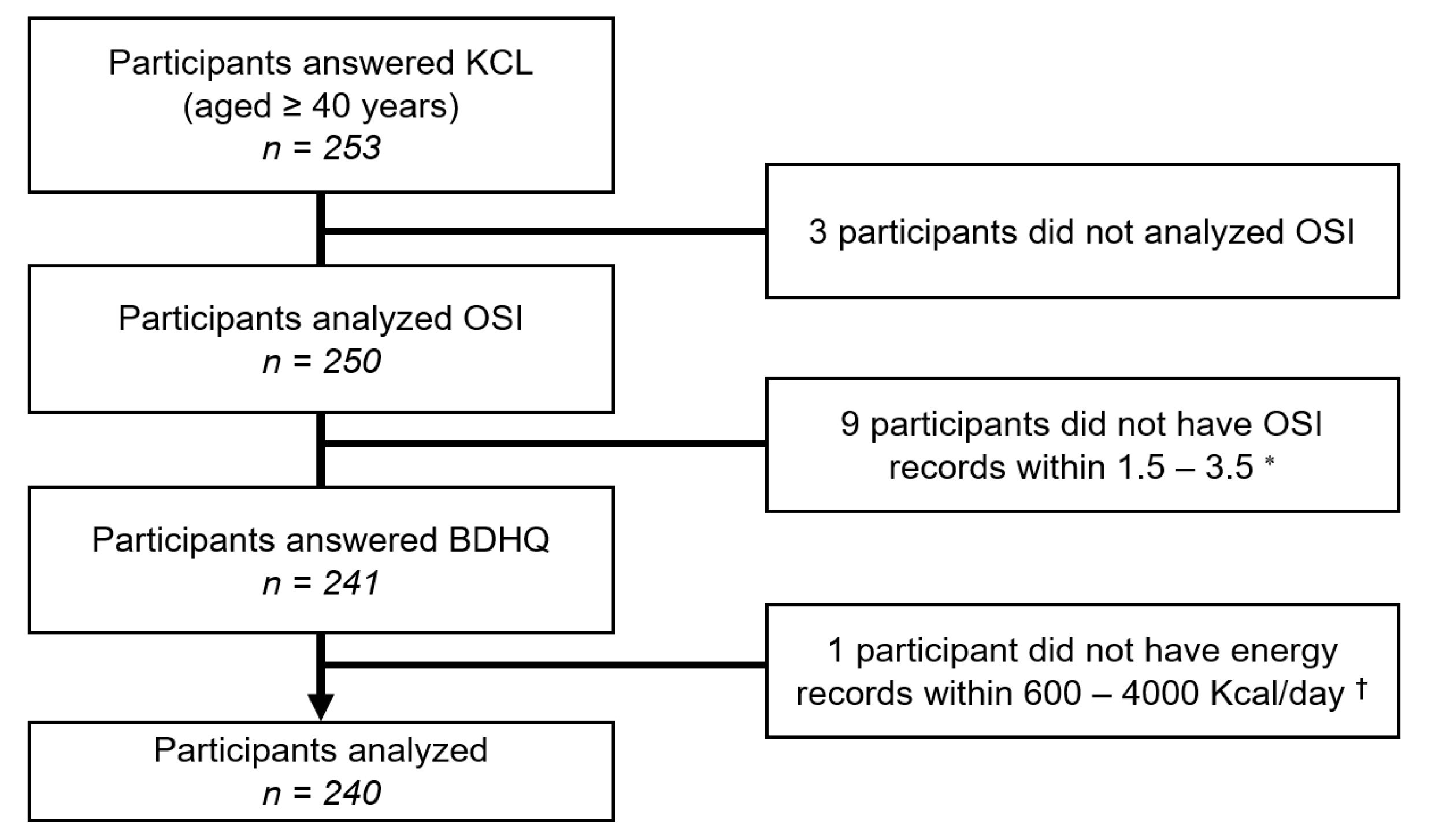
A total of 253 people aged 40 years and older who live in four model districts (Horimatsu, Tsuchida, Higashi Matsudo, and Togi) of Shika Town provided their consent to participate in this study. Of these individuals, 13 were excluded because they did not evaluate osteo-sono assessment index (OSI) or did not have energy records within 600–4000 Kcal on the brief-type self-administered diet history questionnaire (BDHQ)).
Figure 1 shows the inclusion criteria. A total of 240 participants who answered all relevant questions in the questionnaires and did not withdraw their consent were included in the analysis.
2.3. Questionnaire and Measurements
Comprehensive health survey data were collected from the residents of Shika Town, Ishikawa Prefecture, Japan, between November 2017 and February 2018. The participants completed a self-administered questionnaire on lifestyle and underlying diseases. Lifestyle items included current smokers (1. no, 2. yes) and/or current drinkers (1. no, 2. yes) and education (1. junior high school, 2. high school 3. junior college, 4. university or higher). Underlying disease items included hypertension (1. no, 2. yes), diabetes (1. no, 2. yes), and osteoporosis (1. no, 2. yes). Body mass index (BMI) was measured using health survey data from the Shika study.
The Kihon Checklist (KCL) was used to evaluate OF. KCL is a self-reported comprehensive health checklist designed by a study group from the Ministry of Health, Labour, and Welfare as a screening tool to identify community-dwelling older adults who are vulnerable to frailty and have a higher risk of becoming dependent [
16,
17]. The validity of the KCL has been demonstrated in previous studies [
18,
19]. The three oral questions in the KCL were used as components of OF in this study. Specifically, difficulties eating tough foods from half a year ago, difficulties in swallowing tea or soup, and experience of having a dry mouth were defined as the eating, the swallowing, and the oral dryness domain, respectively. For each question, “yes” was converted to 1 point, and the total point was defined as the OF score. Furthermore, as an evaluation of oral function, we asked whether they brushed their teeth at least twice a day and recorded the current number of teeth.
Nutrient intake was assessed using the BDHQ [
20,
21]. The BDHQ is a four-page structured questionnaire that assesses the consumption frequency of 58 foods and beverages commonly consumed by the general Japanese population. The BDHQ estimates dietary intake in the last month using an ad hoc computer algorithm. The validity of the BDHQ has been demonstrated in previous studies [
20,
21]. To analyze nutrient data, the density method was used to estimate intake per 1000 Kcal.
Using a quantitative ultrasonic device (AOS-100NW-B, Hitachi Aloka Medical, Tokyo, Japan), the OSI of the right calcaneus was measured as an indicator of bone strength. OSI correlates closely with bone mineral density measured by dual-energy X-ray absorptiometry [
22]. OSI was calculated using the following formula:
2.4. Statistical Analysis
The participants were classified into two OF groups: the non-OF group, which had a score of 0, and the OF group, which had a score of 1 or higher. The two OSI groups were classified into the low-OSI and high-OSI group based on the median of the participants in this study. IBM SPSS Statistics version 25 for Windows (IBM, Armonk, NY, USA) was used for the statistical analysis. Student’s t-test was used to determine the association between continuous variables, while the Chi-square test was performed to investigate the association between categorical variables. A two-way analysis of covariance (ANCOVA) was used to examine the effects of the interaction between OF and OSI on mineral and food intake. The following confounding factors were adjusted for age, sex, BMI, current smoker, and current drinker. A multiple logistic regression analysis was conducted to examine the effects of OF and mineral and food intake on bone density, using the OSI as the dependent variable. In addition, the analyses were stratified by OF. Pearson’s correlation coefficient was used to confirm multicollinearity. Specifically, there was no value of |r| > 0.9 in the correlation matrix table between independent variables. The forced input method was used for variable selection. The significance level was set at 5%.
2.5. Ethics Statement
This study was conducted with the approval of the Ethics Committee of Kanazawa University (No. 1491). Written informed consent was obtained from all participants prior to participation.
4. Discussion
Since oral frailty is a relatively new concept, its evaluation method is not well established. In the long-term care insurance system for the elderly in Japan, three domains related to the oral cavity of the KCL are used for the evaluation items of oral dysfunction [
18,
19]. In addition to these three domains, the current number of teeth [
1,
23], masticatory ability [
1], tooth brushing twice daily [
6], regular dental visits [
6], denture use [
24], occlusal force [
2], tongue–lip function [
2], and eating alone [
25] were used to evaluate OF. Furthermore, since the evaluation method of pre-OF has not been fully discussed, there have been some reports [
25,
26] that the survey items of OF with few applicable items are regarded as pre-OF. In this study, we decided to use three domains related to the oral cavity in the KCL to evaluate the oral dysfunction from an early stage, including pre-OF, as a population approach.
The main result of this study was that when OSI was stratified into two groups with OF as the dependent variable in multiple logistic regression analysis, minerals, potassium, calcium, magnesium, phosphorus, carrots/pumpkins, citrus, and salt intake were found to be significant independent variables in the low-OSI group.
According to ANCOVA results, the main effects were observed in potassium, magnesium, phosphorus, green leafy vegetables, citrus, and salt intake even after adjusting for confounding factors in the OF group. This contrasted the study by Nomura et al. [
6], who investigated the relationship between OF and nutrient intake and found no association between OF and mineral intake. They evaluated factors related to oral health behavior and macronutrients using structural equation modeling. It seems that the reason why our results differed from theirs was that they did not analyze the involvement of chewing and swallowing functions in the assessment of food choice and oral dysfunction. Alternatively, Zhe et al. [
23] reported that protein, vitamins, and mineral intake is positively associated with the total number of natural teeth. This study was thought to have elucidated the non-oral frailty and high-OSI group had 20 or more current teeth, while the other groups had less than 20 current teeth, indicating an interaction. In other words, it indicates that there is a relationship between the decline in oral function and food choice.
It has also been noted that not nutrients or foods, but HbA1c, diabetes, and currently drunk showed a main effect on the OSI even after adjusting the covariates. A meta-analysis by Ma et al. [
27] and a review by Piepkorn et al. [
28] reported that patients with type 2 diabetes have higher bone mineral density than non-diabetic patients. Our results that showed that the proportion of patients with diabetes was higher in the high-OSI group support this finding. A prospective study by Holbrook and Barrett-Connor [
29] also reported that drinking increased bone mineral density. Our findings that the proportion of current drinkers was higher in the high-OSI group might also support the report.
Potassium, magnesium, phosphorus, carrots/pumpkins, citrus, and salt intake were observed to have the main effect on the two OF groups or the interaction among the four OF and OSI groups. These minerals and foods were also significant independent variables when stratified by OSI in multiple logistic regression analysis with OF as the dependent variable. In line with our finding, previous studies investigating the relationship between mineral intake and bone mineral density reported that potassium and magnesium intake was associated with increased bone mineral density in the elderly [
30]; that dietary protein, phosphorus, and potassium were beneficial to bone mineral density in adult men consuming adequate dietary calcium [
31]; and that magnesium intake was associated with bone mineral density [
5,
32]. With regard to the relationship between food intake and bone mineral density, Kim et al. [
33] reported that intake of anchovies, radishes, carrots, zucchinis, and tomatoes were significant important factors in minimizing bone density risk. Our results support the above findings because we found a similar relationship between the minerals or mineral-containing food intake and OSI. Our study showed that the mean current number of teeth was 20 or more only in the non-OF and high-OSI group. Poor chewing and swallowing function due to OF and having less than 20 current teeth are presumed to reduce the variety of chewable foods. It suggests that the decrease in mineral intake due to the change in the food choice by OF is associated with the decrease in bone mineral density.
Since this study was a cross-sectional study, the causal relationship between OF, mineral intake, and bone mineral density could not be ascertained. Moreover, OSI does not directly evaluate bone mineral density. Finally, self-administration of BDHQ may lack objectivity.


 ,
, 


{kind=link}