
Maternal Dietary Selenium Intake during Pregnancy and Neonatal Outcomes in the Norwegian Mother, Father, and Child Cohort Study


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Study Population
2.3. Maternal Selenium Intake from Food and Dietary Supplements
2.4. Selenium Status
2.5. Neonatal Outcomes
2.6. Statistical Analyses
3. Results
3.1. Study Population
3.2. Selenium Intake
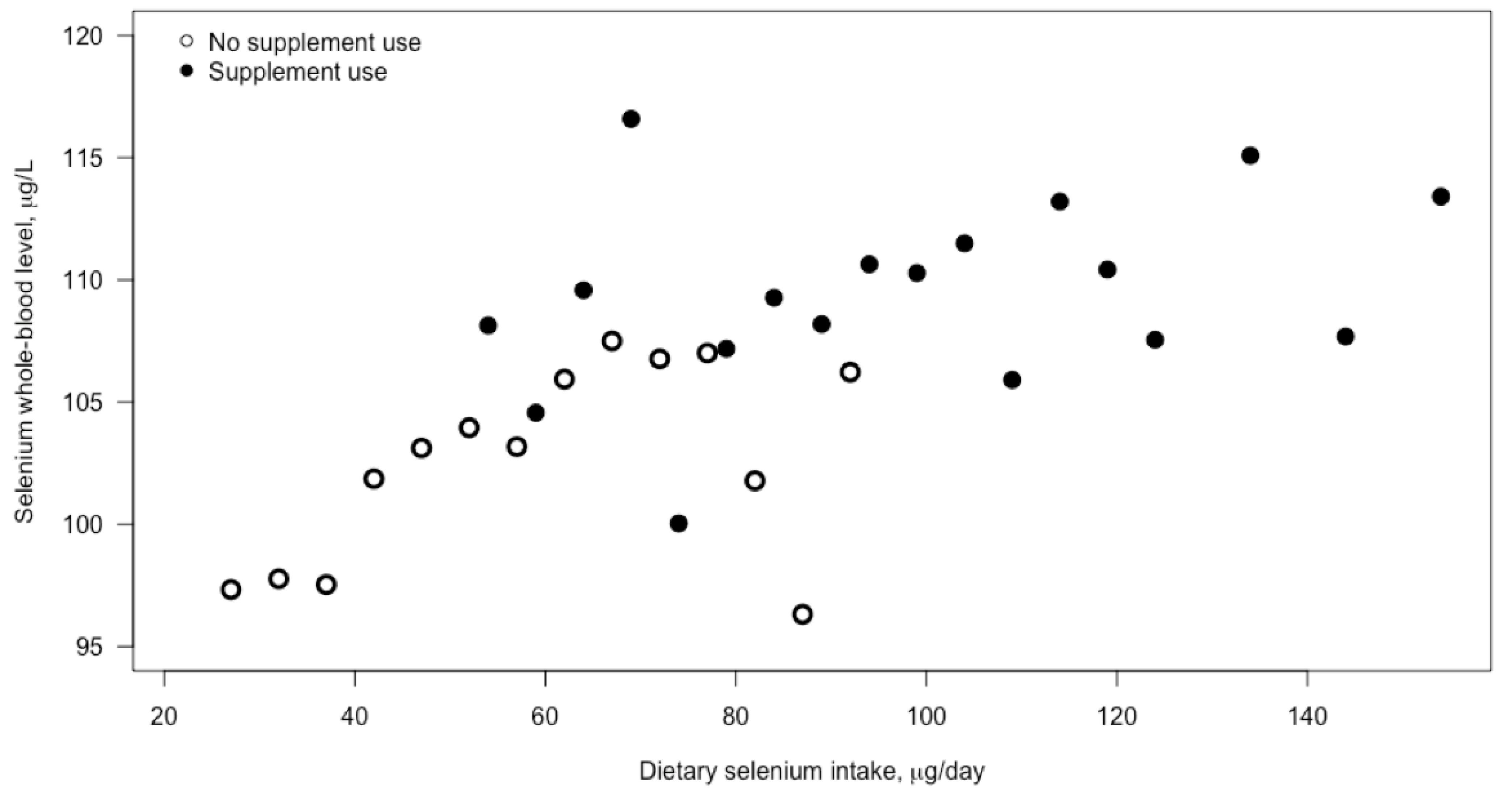
3.3. Blood Selenium Concentration
3.4. Neonatal Outcomes
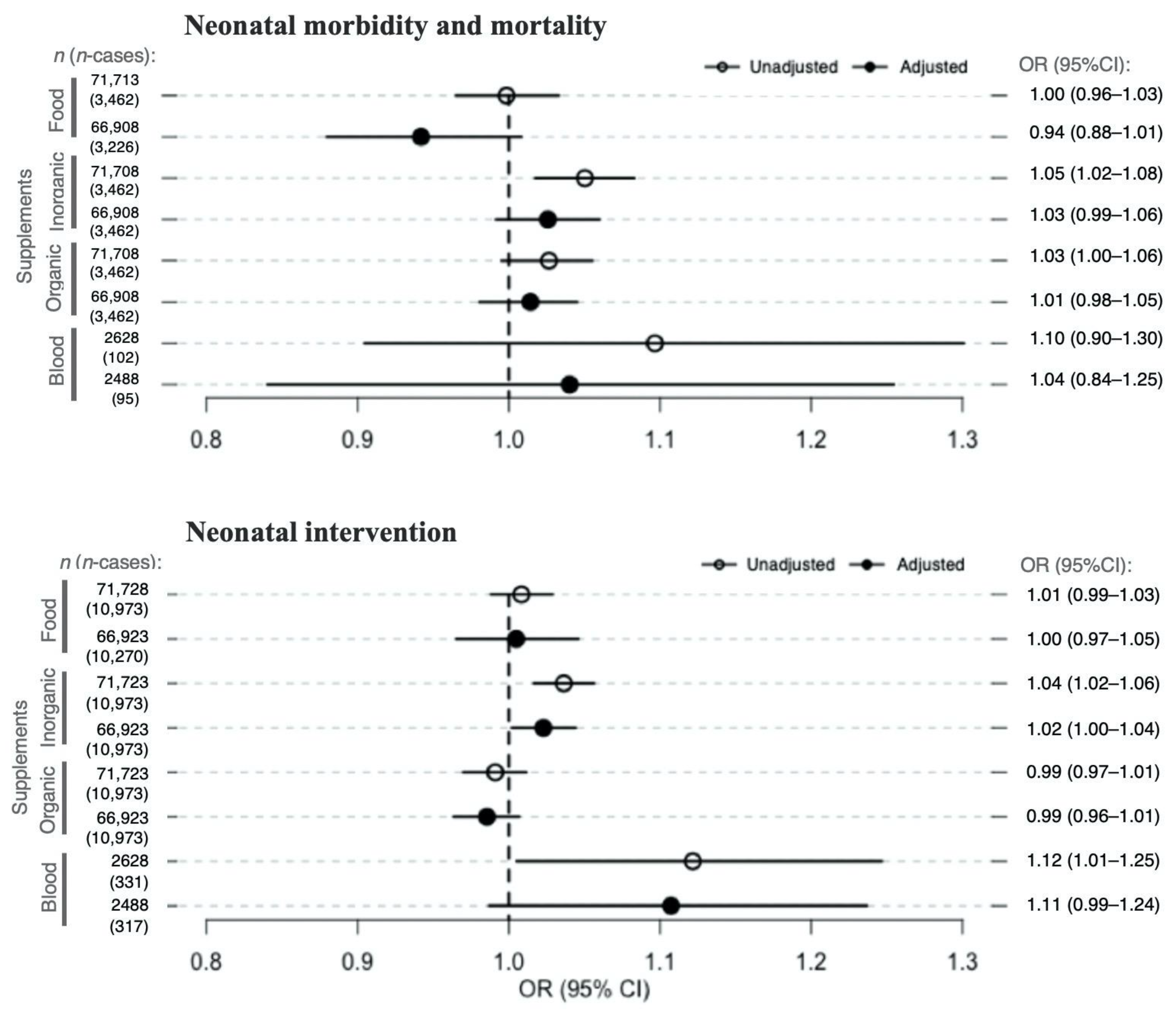
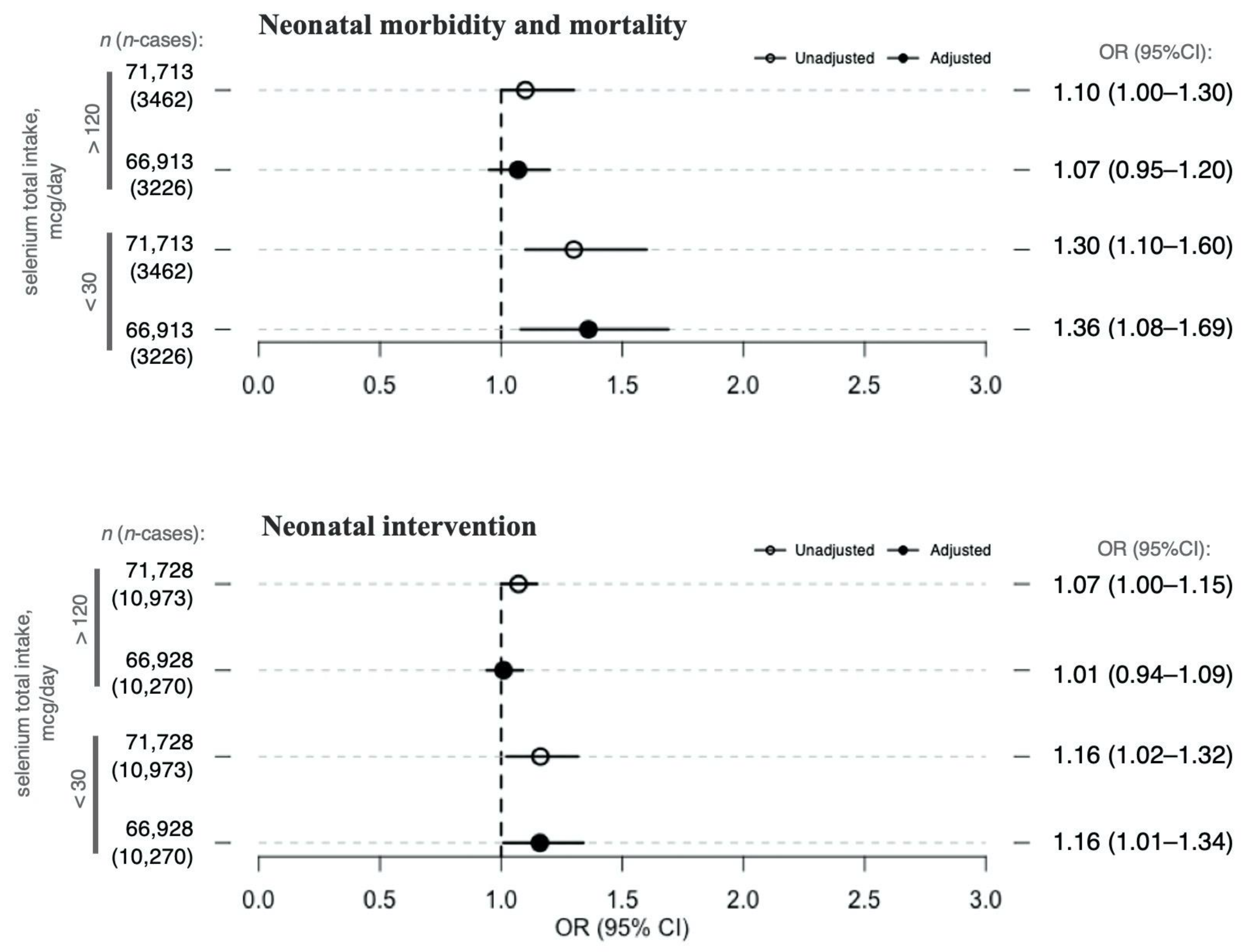
3.5. Selenium Exposure and Neonatal Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hovdenak, N.; Haram, K. Influence of Mineral and Vitamin Supplements on Pregnancy Outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 164, 127–132. [Google Scholar] [CrossRef]
- Christian, P.; Mullany, L.C.; Hurley, K.M.; Katz, J.; Black, R.E. Nutrition and Maternal, Neonatal, and Child Health. Semin. Perinatol. 2015, 39, 361–372. [Google Scholar] [CrossRef]
- Hofstee, P.; McKeating, D.R.; Perkins, A.V.; Cuffe, J.S. Placental Adaptations to Micronutrient Dysregulation in the Programming of Chronic Disease. Clin. Exp. Pharmacol. Physiol. 2018, 45, 871–884. [Google Scholar] [CrossRef]
- Farias, P.M.; Marcelino, G.; Santana, L.F.; de Almeida, E.B.; Guimarães, R.d.C.A.; Pott, A.; Hiane, P.A.; Freitas, K.d.C. Minerals in Pregnancy and Their Impact on Child Growth and Development. Molecules 2020, 25, 5630. [Google Scholar] [CrossRef] [PubMed]
- Abu-Saad, K.; Fraser, D. Maternal Nutrition and Birth Outcomes. Epidemiol. Rev. 2010, 32, 5–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinggi, U. Selenium: Its Role as Antioxidant in Human Health. Environ. Health Prev. Med. 2008, 13, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duhig, K.; Chappell, L.C.; Shennan, A.H. Oxidative Stress in Pregnancy and Reproduction. Obstet. Med. 2016, 9, 113–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanagal, D.V.; Rajesh, A.; Rao, K.; Shetty, H.; Shetty, P.K.; Ullal, H. Zinc and Copper Levels in Preeclampsia: A Study from Coastal South India. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 3, 370–373. [Google Scholar] [CrossRef]
- Redman, C.W.; Sargent, I.L. Latest Advances in Understanding Preeclampsia. Science 2005, 308, 1592–1594. [Google Scholar] [CrossRef]
- Weber, D.; Stuetz, W.; Bernhard, W.; Franz, A.; Raith, M.; Grune, T.; Breusing, N. Oxidative Stress Markers and Micronutrients in Maternal and Cord Blood in Relation to Neonatal Outcome. Eur. J. Clin. Nutr. 2014, 68, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, K.K.; McElrath, T.F.; Chen, Y.-H.; Loch-Caruso, R.; Mukherjee, B.; Meeker, J.D. Repeated Measures of Urinary Oxidative Stress Biomarkers during Pregnancy and Preterm Birth. Am. J. Obstet. Gynecol. 2015, 212, 208.e1–208.e8. [Google Scholar] [CrossRef] [Green Version]
- El-Mazary, A.-A.M.; Abdel-Aziz, R.A.; Mahmoud, R.A.; El-Said, M.A.; Mohammed, N.R. Correlations between Maternal and Neonatal Serum Selenium Levels in Full Term Neonates with Hypoxic Ischemic Encephalopathy. Ital. J. Pediatr. 2015, 41, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.; Feenstra, B.; Bacelis, J.; Liu, X.; Muglia, L.M.; Juodakis, J.; Miller, D.E.; Litterman, N.; Jiang, P.-P.; Russell, L.; et al. Genetic Associations with Gestational Duration and Spontaneous Preterm Birth. N. Engl. J. Med. 2017, 377, 1156–1167. [Google Scholar] [CrossRef] [PubMed]
- Barman, M.; Brantsæter, A.L.; Nilsson, S.; Haugen, M.; Lundh, T.; Combs, G.F.; Zhang, G.; Muglia, L.J.; Meltzer, H.M.; Jacobsson, B.; et al. Maternal Dietary Selenium Intake Is Associated with Increased Gestational Length and Decreased Risk of Preterm Delivery. Br. J. Nutr. 2020, 123, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solé-Navais, P.; Brantsæter, A.L.; Caspersen, I.H.; Lundh, T.; Muglia, L.J.; Meltzer, H.M.; Zhang, G.; Jacobsson, B.; Sengpiel, V.; Barman, M. Maternal Dietary Selenium Intake during Pregnancy Is Associated with Higher Birth Weight and Lower Risk of Small for Gestational Age Births in the Norwegian Mother, Father and Child Cohort Study. Nutrients 2020, 13, 23. [Google Scholar] [CrossRef]
- Kramer, M.S. Born Too Small or Too Soon. Lancet Glob. Health 2013, 1, e7–e8. [Google Scholar] [CrossRef] [Green Version]
- Irgens, L.M. The Medical Birth Registry of Norway. Epidemiological Research and Surveillance throughout 30 Years. Acta Obstet. Gynecol. Scand. 2000, 79, 435–439. [Google Scholar]
- Magnus, P.; Birke, C.; Vejrup, K.; Haugan, A.; Alsaker, E.; Daltveit, A.K.; Handal, M.; Haugen, M.; Høiseth, G.; Knudsen, G.P.; et al. Cohort Profile Update: The Norwegian Mother and Child Cohort Study (MoBa). Int. J. Epidemiol. 2016, 45, 382–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meltzer, H.M.; Brantsaeter, A.L.; Ydersbond, T.A.; Alexander, J.; Haugen, M. Methodological Challenges When Monitoring the Diet of Pregnant Women in a Large Study: Experiences from the Norwegian Mother and Child Cohort Study (MoBa). Matern. Child. Nutr. 2008, 4, 14–27. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Haugen, M.; Alexander, J.; Meltzer, H.M. Validity of a New Food Frequency Questionnaire for Pregnant Women in the Norwegian Mother and Child Cohort Study (MoBa). Matern. Child. Nutr 2008, 4, 28–43. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Haugen, M.; Hagve, T.-A.; Aksnes, L.; Rasmussen, S.E.; Julshamn, K.; Alexander, J.; Meltzer, H.M. Self-Reported Dietary Supplement Use Is Confirmed by Biological Markers in the Norwegian Mother and Child Cohort Study (MoBa). Ann. Nutr. Metab. 2007, 51, 146–154. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Haugen, M.; Thomassen, Y.; Ellingsen, D.G.; Ydersbond, T.A.; Hagve, T.-A.; Alexander, J.; Meltzer, H.M. Exploration of Biomarkers for Total Fish Intake in Pregnant Norwegian Women. Public Health Nutr. 2010, 13, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Lauritsen, J. FoodCalc v.1.3: Diet, Cancer and Health Project; Danish Cancer Society: Copenhagen, Denmark, 1998. [Google Scholar]
- Rimestad, A.H.; Borgejordet, Å.; Vesterhus, K.N.; Sygnestveit, K.; Løken, E.B.; Trygg, K.; Pollestad, M.L.; Lund-Larsen, K.; Omholt-Jensen, G.; Nordbotten, A. Den Store Matvaretabellen [The Norwegian Food Table]; Statens Råd for Ernæring Og Fysisk Aktivitet, Statens Næringsmiddeltilsyn, Universitetet i Oslo—Institutt for Ernæringsforskning: Oslo, Norway, 2005. [Google Scholar]
- Haugen, M.; Brantsaeter, A.L.; Alexander, J.; Meltzer, H.M. Dietary Supplements Contribute Substantially to the Total Nutrient Intake in Pregnant Norwegian Women. Ann. Nutr. Metab. 2008, 52, 272–280. [Google Scholar] [CrossRef] [Green Version]
- Paltiel, L.; Anita, H.; Skjerden, T.; Harbak, K.; Bækken, S.; Kristin, S.N.; Knudsen, G.P.; Magnus, P. The Biobank of the Norwegian Mother and Child Cohort Study—Present Status. Nor. J. Epidemiol. 2014, 24. [Google Scholar] [CrossRef]
- Caspersen, I.H.; Thomsen, C.; Haug, L.S.; Knutsen, H.K.; Brantsæter, A.L.; Papadopoulou, E.; Erlund, I.; Lundh, T.; Alexander, J.; Meltzer, H.M. Patterns and Dietary Determinants of Essential and Toxic Elements in Blood Measured in Mid-Pregnancy: The Norwegian Environmental Biobank. Sci. Total Environ. 2019, 671, 299–308. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision; World Health Organization: Geneva, Switzerland, 2004; ISBN 978-92-4-154649-2. [Google Scholar]
- Skjærven, R.; Gjessing, H.K.; Bakketeig, L.S. Birthweight by Gestational Age in Norway. Acta Obstet. Gynecol. Scand. 2000, 79, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Kipp, A.P.; Strohm, D.; Brigelius-Flohé, R.; Schomburg, L.; Bechthold, A.; Leschik-Bonnet, E.; Heseker, H. Revised Reference Values for Selenium Intake. J. Trace Elem. Med. Biol. 2015, 32, 195–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, H.-C. Impact of Maternal Selenium Supplementation on Neonates. Pediatrics Neonatol. 2012, 53, 327–328. [Google Scholar] [CrossRef] [Green Version]
- Mostafa Gharehbaghi, M.; Gharabaghi, P.; Ghanbari, F.; Abdolmohammad-Zadeh, H.; Sadeghi, G.; Jouyban, A.G. Determination of Se in Serum Samples of Preterm Newborn Infants with Bronchopulmonary Dysplasia Using a Validated Hydride Generation System. Biol. Trace Elem. Res. 2011, 147, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Modzelewska, D.; Bellocco, R.; Elfvin, A.; Brantsæter, A.L.; Meltzer, H.M.; Jacobsson, B.; Sengpiel, V. Caffeine Exposure during Pregnancy, Small for Gestational Age Birth and Neonatal Outcome—Results from the Norwegian Mother and Child Cohort Study. BMC Pregnancy Childbirth 2019, 19, 80. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.P.; Chawanpaiboon, S.; Moller, A.-B.; Watananirun, K.; Bonet, M.; Lumbiganon, P. The Global Epidemiology of Preterm Birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Díaz, S.; Schisterman, E.F.; Hernán, M.A. The Birth Weight “Paradox” Uncovered? Am. J. Epidemiol. 2006, 164, 1115–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NNR Project Group. Selenium. In Nordic Nutrition Recommendations 2012, Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014; pp. 591–600. Available online: http://norden.diva-portal.org/smash/get/diva2:704251/FULLTEXT01.pdf (accessed on 2 February 2021).
- Nilsen, R.M.; Vollset, S.E.; Gjessing, H.K.; Skjaerven, R.; Melve, K.K.; Schreuder, P.; Alsaker, E.R.; Haug, K.; Daltveit, A.K.; Magnus, P. Self-Selection and Bias in a Large Prospective Pregnancy Cohort in Norway. Paediatr. Perinat. Epidemiol. 2009, 23, 597–608. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dietary Selenium Intake, μg/day | Total Selenium Intake, μg/L | ||||||
|---|---|---|---|---|---|---|---|
| Characteristics | n | % | Median | 25th–75th Percentile | Median | 25th–75th Percentile | |
| Total population | 71,728 | 100 | 53 | 44–62 | 102 | 83–123 | |
| Maternal age, years | <25 | 8239 | 11 | 50 | 41–61 | 101 | 83–125 |
| 25–29 | 24,313 | 34 | 52 | 43–62 | 101 | 83–122 | |
| 30–34 | 30,410 | 42 | 53 | 45–63 | 102 | 84–123 | |
| >34 | 8766 | 12 | 54 | 46–64 | 104 | 85–125 | |
| Maternal education, years | <12 | 22,286 | 31 | 51 | 42–62 | 102 | 84–125 |
| 12–16 | 29,757 | 41 | 53 | 44–62 | 101 | 83–123 | |
| >16 | 18,150 | 25 | 54 | 46–64 | 102 | 83–122 | |
| Missing | 1535 | 2 | 51 | 42–62 | 99 | 82–122 | |
| Pre-pregnancy BMI, kg/m2 | <18.5 | 2130 | 3 | 53 | 44–64 | 103 | 83–126 |
| 18.5–24.9 | 45,976 | 64 | 53 | 45–63 | 102 | 83–123 | |
| 25–29.9 | 15,134 | 21 | 52 | 43–61 | 101 | 84–123 | |
| >30 | 6633 | 9 | 51 | 42–61 | 102 | 84–122 | |
| Missing | 1855 | 3 | 52 | 44–62 | 99 | 81–121 | |
| Parity | 0 * | 38,169 | 53 | 52 | 43–62 | 102 | 84–123 |
| 1 | 21,557 | 30 | 53 | 44–62 | 101 | 83–122 | |
| 2 | 9652 | 13 | 54 | 45–63 | 101 | 83–121 | |
| ≥3 | 2293 | 3 | 54 | 45–64 | 104 | 82–128 | |
| Missing | 57 | 1 | 56 | 45–63 | 102 | 83–115 | |
| Smoking during pregnancy | Never | 65,504 | 91 | 51 | 42–62 | 105 | 83–127 |
| Occasionally | 3876 | 5 | 53 | 44–62 | 102 | 83–123 | |
| Daily | 1943 | 3 | 52 | 43–63 | 102 | 84–123 | |
| Missing | 405 | 1 | 52 | 43–62 | 99 | 79–121 | |
| Passive smoking | No | 62,767 | 88 | 53 | 44–62 | 102 | 83–123 |
| Yes | 7580 | 11 | 52 | 43–63 | 103 | 83–126 | |
| Missing | 1381 | 2 | 51 | 43–63 | 102 | 83–126 | |
| Alcohol consumption | No | 63,806 | 89 | 53 | 44–62 | 102 | 84–123 |
| Yes | 7922 | 11 | 54 | 46–63 | 101 | 82–122 | |
| Nausea during the second trimester | No | 63,504 | 89 | 53 | 44–62 | 102 | 84–123 |
| Yes | 8224 | 11 | 52 | 42–62 | 100 | 81–122 | |
| Iodine intake, μg/day | <89 | 17,637 | 25 | 43 | 36–50 | 91 | 74–112 |
| 89–121 | 17,564 | 24 | 50 | 43–58 | 98 | 81–118 | |
| 121–162 | 18,354 | 26 | 55 | 48–63 | 104 | 87–124 | |
| > 162 | 18,094 | 25 | 63 | 55–73 | 114 | 95–135 | |
| Protein intake, g/day | <76 | 23,952 | 33 | 42 | 36–48 | 89 | 72–108 |
| 76–93 | 23,826 | 33 | 65 | 58–74 | 114 | 97–136 | |
| >93 | 23,950 | 33 | 53 | 47–59 | 101 | 85–121 | |
| Total energy intake, kJ/day | <8392 | 23,950 | 33 | 44 | 37–50 | 91 | 75–112 |
| 8392–10,460 | 23,832 | 33 | 63 | 55–73 | 112 | 94–134 | |
| >10,460 | 23,946 | 33 | 53 | 46–60 | 102 | 85–121 | |
| Gestational age at birth, weeks + days | ≤27 + 6 | 126 | 0 | 53 | 47–62 | 114 | 83–133 |
| 28 + 0 to 31 + 6 | 306 | 0 | 50 | 41–60 | 98 | 85–114 | |
| 32 + 0 to 36 + 6 | 2836 | 4 | 53 | 44–62 | 103 | 86–123 | |
| ≥37 + 0 | 67,827 | 95 | 53 | 44–62 | 102 | 83–123 | |
| Missing | 594 | 1 | 53 | 44–62 | 100 | 81–120 | |
| Birth weight, g | <1500 | 398 | 1 | 52 | 44–62 | 101 | 82–121 |
| 1500–2500 | 1751 | 2 | 52 | 43–61 | 102 | 86–122 | |
| >2500 | 69551 | 97 | 53 | 44–62 | 102 | 83–123 | |
| Missing | 31 | 0 | 52 | 47–58 | 107 | 88–134 | |
| Morbidity (ICD-10) | Number of Children | Percentage | |
|---|---|---|---|
| Total | 71,728 | 100 | |
| Neonatal mortality and morbidity | Apgar score < 4 at 5 min | 137 | 0.19 |
| Birth asphyxia (P21) | 2416 | 3.3 | |
| Other disturbances in the cerebral status of the newborn (P910–916) | 30 | 0.04 | |
| Intracranial (non-traumatic) hemorrhage of the fetus and newborn | 154 | 0.21 | |
| Retinopathy of prematurity (H351) | 22 | 0.03 | |
| Meconium ileus/necrotizing enterocolitis (P75, P76, P77, P780, P781) | 31 | 0.04 | |
| Chronic respiratory disease originating in the perinatal period (P27) | 77 | 0.11 | |
| Bacterial sepsis in the newborn (P36) | 906 | 1.3 | |
| Other infections specific to the perinatal period (P39) | 252 | 0.35 | |
| Neonatal death | 629 | 0.88 | |
| Total neonatal mortality and morbidity | 3462 | 4.83 | |
| Neonatal intervention | Systemic antibiotics | 1976 | 2.8 |
| Ventilator | 363 | 0.51 | |
| CPAP | 935 | 1.30 | |
| NICU admission | 10,942 | 15.25 | |
| Total neonatal intervention | 10,973 | 15.30 | |
| Total, n = 71,728 | Neonatal Mortality/Morbidity | Neonatal Intervention | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | ||||||||
| Median 25th–75th Percentile | Median 25th–75th Percentile | Median 25th–75th Percentile | Median 25th–75th Percentile | Median 25th–75th Percentile | |||||||
| Dietary selenium intake, μg/day | 53 | 44–62 | 53 | 44–62 | 53 | 44–62 | 53 | 44–62 | 53 | 44–62 | |
| Inorganic selenium supplements, μg/day | 50 | 35–75 | 50 | 35–75 | 50 | 36–75 | 50 | 35–75 | 50 | 36–75 | |
| Organic selenium supplements, μg/day | 30 | 21–43 | 30 | 21–43 | 30 | 25–50 | 30 | 21–43 | 30 | 21–36 | |
| Selenium blood concentration, μg/L | 102 | 89–117 | 102 | 89–117 | 106 | 89–121 | 102 | 89–117 | 105 | 92–119 | |
| n | % | n | % | n | % | n | % | n | % | ||
| Total selenium (diet and supplements), μg/day | <30 | 1180 | 2 | 1101 | 2 | 79 | 2 | 976 | 2 | 204 | 2 |
| 30–120 | 64,114 | 89 | 61,064 | 89 | 3036 | 88 | 54,383 | 90 | 9731 | 89 | |
| >120 | 6434 | 9 | 6086 | 9 | 347 | 10 | 5396 | 8 | 1038 | 9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modzelewska, D.; Solé-Navais, P.; Brantsæter, A.L.; Flatley, C.; Elfvin, A.; Meltzer, H.M.; Sengpiel, V.; Barman, M.; Jacobsson, B. Maternal Dietary Selenium Intake during Pregnancy and Neonatal Outcomes in the Norwegian Mother, Father, and Child Cohort Study. Nutrients 2021, 13, 1239. https://doi.org/10.3390/nu13041239
Modzelewska D, Solé-Navais P, Brantsæter AL, Flatley C, Elfvin A, Meltzer HM, Sengpiel V, Barman M, Jacobsson B. Maternal Dietary Selenium Intake during Pregnancy and Neonatal Outcomes in the Norwegian Mother, Father, and Child Cohort Study. Nutrients. 2021; 13(4):1239. https://doi.org/10.3390/nu13041239
Chicago/Turabian StyleModzelewska, Dominika, Pol Solé-Navais, Anne Lise Brantsæter, Christopher Flatley, Anders Elfvin, Helle Margrete Meltzer, Verena Sengpiel, Malin Barman, and Bo Jacobsson. 2021. "Maternal Dietary Selenium Intake during Pregnancy and Neonatal Outcomes in the Norwegian Mother, Father, and Child Cohort Study" Nutrients 13, no. 4: 1239. https://doi.org/10.3390/nu13041239
APA StyleModzelewska, D., Solé-Navais, P., Brantsæter, A. L., Flatley, C., Elfvin, A., Meltzer, H. M., Sengpiel, V., Barman, M., & Jacobsson, B. (2021). Maternal Dietary Selenium Intake during Pregnancy and Neonatal Outcomes in the Norwegian Mother, Father, and Child Cohort Study. Nutrients, 13(4), 1239. https://doi.org/10.3390/nu13041239